
Abstract

Introduction
CT-fluoroscopy allows for real-time needle visualization with potential synchronization to the patient’s movements or changes in position of the intended biopsy target. 1 The rapidly beating heart is indisputably one of the most challenging biopsy targets due to the constant motion and the vulnerable anatomical structures. In addition, minor procedural complications may inadvertently lead to detrimental outcomes.
Materials and Methods
Patient Cohort
Twenty patients presenting with cardio-pericardial masses, referred for tissue sampling to our center between August 2018 and April 2023, were included in this study. The Institutional Ethics Board waived the need for retrospective patient consent.
Procedure
All procedures were performed on a Cardiac CT scanner (Canon Aquilion One Vision, Otawara, Japan). Intravenous sedation (50 micrograms of Fentanyl and 1 mg of Midazolam) and nasal oxygen were provided; EKG electrodes were connected to an in-room EKG monitor.
The best possible access route was determined with the following guiding principles: prefer the shortest access route, protect internal mammary and coronary vessels, and avoid penetrating ventilated lung tissue and myocardium if possible. For needle navigation, intermittent CT-fluoroscopy was either initiated by the foot pedal synchronous to the EKG monitor beeps or automatically synchronized to the EKG at end-systole to ensure the best possible reproducibility of the cardiac cycle.
Patients were monitored post-biopsy for 2 hours. Two posteroanterior chest radiographs were obtained at 1 and 2 hours post-procedure before patients were discharged home. The total procedure in-room time was taken from the Radiology Information System (RIS).
Results
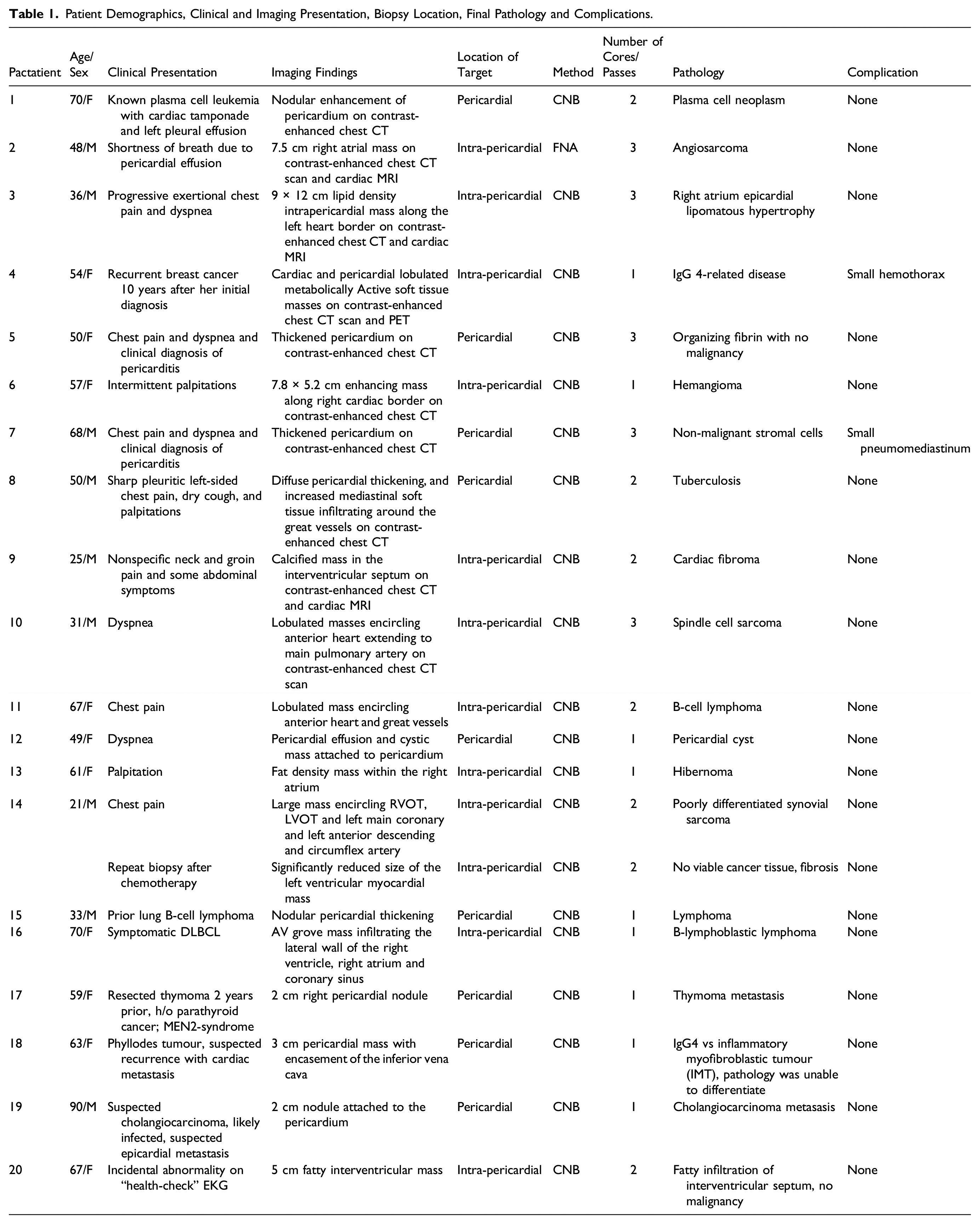
Patient Demographics, Clinical and Imaging Presentation, Biopsy Location, Final Pathology and Complications.
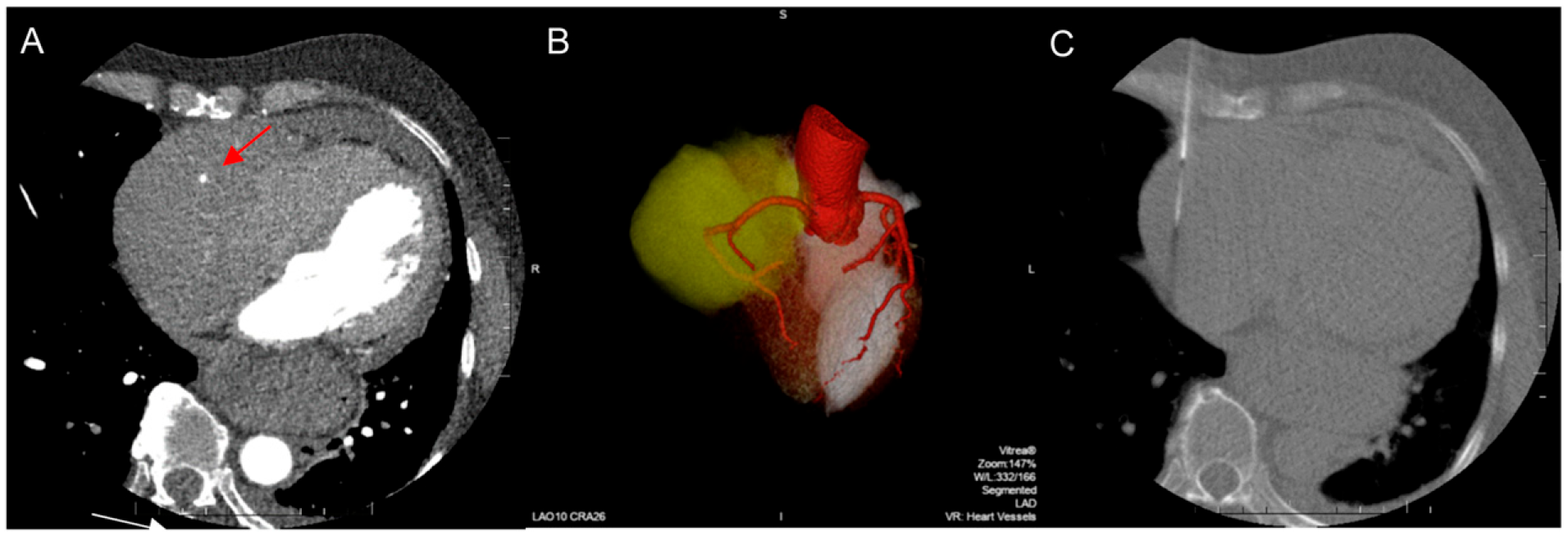
A seventy-year-old woman was found to have a soft tissue mass in the right AV grove infiltrating the lateral wall of the right ventricle, right atrium and coronary sinus. Mapping of the coronary arteries visualizes the course of the RCA (A, arrow; B, three-dimensional reconstruction, the mass is coloured in yellow). The needle was navigated using EKG-gated CT- fluoroscopy into the mass right lateral to the RCA (C). Histology identified the manifestation of a B-lymphoblastic lymphoma.
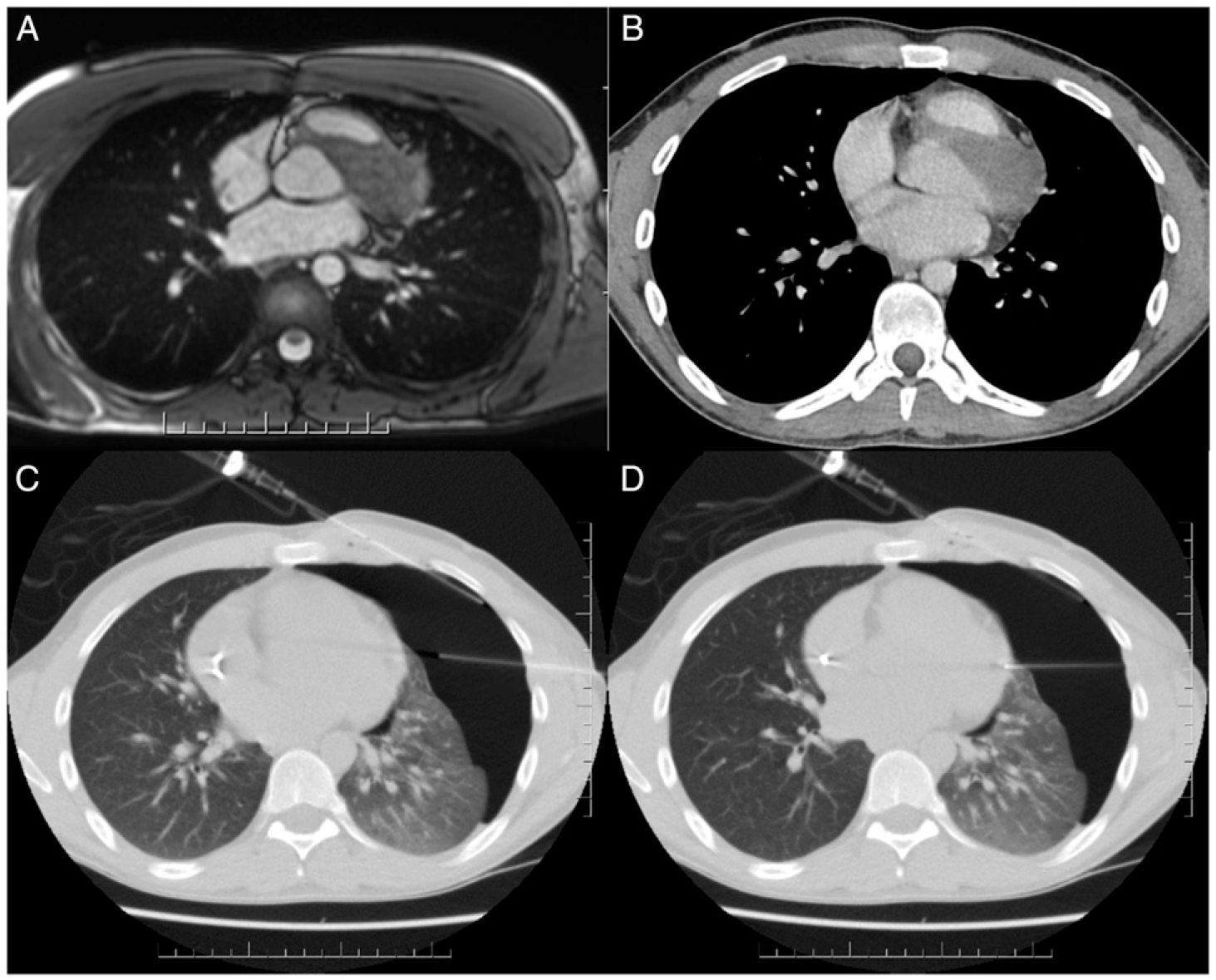
Twenty-one-year-old man with synovial sarcoma, second biopsy after chemotherapy. The T2-weighted free-breathing MRI (A) and contrast-enhanced CT (B) show the previously biopsied synovial sarcoma. The biopsy was indicated to assess treatment response and to evaluate subsequent surgical resection. A capnothorax was introduced to gain access from left lateral (C) without traversing ventilated lung (D). Histology confirmed treatment success, only showing fibrotic tissue without viable tumour cells.
With the exception of 1 case, an 18 gauge full-core biopsy gun was used to harvest 1-3 cores from the target lesion. A fine-needle aspiration biopsy was performed in 1 patient (patient 2).
All biopsies resulted in a definitive final diagnosis. The duration of the biopsy procedure ranged from 30-50 minutes (total in-room time). One patient developed a small hemothorax immediately detected after needle retraction and was admitted overnight as a precautionary measure. A trace of mediastinal air was detected in a single patient immediately after pericardial biopsy, likely introduced through the biopsy needle.
Discussion
All cardiac biopsies were successful, yielding definitive diagnoses with important bearings on further management, and performed under local anesthesia and intravenous sedation, obviating the need for general anesthesia. We did not experience relevant complications (extended hemorrhage, pericardial tamponade, arrhythmia, embolization), which compares favourably with individual case reports (supplemental submission).
Endoluminal access routes are often preferred to avoid excisional biopsy via mediastinoscopy or cardiac surgery;3,4 however, physical constraints limit the ability to sample deep myocardial or pericardial masses. Several techniques have been developed to allow for more forceful transcatheter “push” to avoid superficial sampling.5,6
Limitations of this study include its retrospective nature and the single-center experience with no alternative sampling methods tested in comparison. Also, all biopsies were performed by the same operator in collaboration with a clinical care team and highly skilled technologists and nurses, limiting the generalizability of the results.
In conclusion, this first case series highlights that CT-fluoroscopy guided cardiac biopsies are safe to perform, leading to definitive diagnoses in our study population; judicious use of this procedure in carefully selected patients appears paramount.
Supplemental Material
Supplemental Material - CT-Fluoroscopy Guided Percutaneous Biopsy of Cardio-Pericardial Masses
Supplemental Material for CT-Fluoroscopy Guided Percutaneous Biopsy of Cardio-Pericardial Masses by Patrik Rogalla, Ciara O’Brien, Mini Pakkal, Sonja Kandel, Nikta Sarie, Robert James Cusimano and Marina Pourafkari in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.