
Abstract
Purpose
The purpose of this study was to compare the technical success rate, the selectivity of transarterial chemoembolization (TACE), the complication rate, the radiation dose given to the patients and the hospitalization stay between TACE performed using femoral artery approach (FAA) and TACE performed using radial artery approach (RAA) in patients with hepatocellular carcinoma (HCC).
Methods
Between June 2020 and April 2022, 49 patients with HCC who underwent 116 TACEs (75 using FAA and 41 using RAA) were included. Differences in technical success rate, selectivity of micro-catheterization, radiation dose given to the patients, fluoroscopy time, hospitalization stay duration, and complication rate were compared between FAA and RAA using Fisher exact or Student t tests.
Results
No differences in technical success rates were found between RAA (93%; 39/41 TACEs) and FAA (100%; 75/75 TACEs) (P = .12). There were no differences between the two groups in terms of selectivity of catheterization, radiation dose, fluoroscopy time and hospitalization stay duration. Five patients had Grade 2 complications (hematoma) after FAA vs. one patient with one Grade 1 complication (radial artery occlusion) after RAA (5/75 [7%] vs. 1/41 [2%], respectively; P = .42). No major arterial access site complications occurred with FAA or RAA.
Conclusions
This study confirms that RAA is a safe approach that does not compromise the technical efficacy and the selectivity of TACE compared to FAA in patients with HCC.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary cancer of the liver and the fifth most common cancer in men and the seventh in women. 1 While only 30% of the patients with HCC are amenable to curative treatment, trans-arterial chemoembolization (TACE) is an option for those with intermediate stage HCC (i.e., those with Barcelona Clinic for Liver Cancer [BCLC] stage B) who have unresectable HCC, pending satisfactory liver function.2,3
TACE is usually performed using a femoral artery approach (FAA), but this can result in an increased risk of bleeding, particularly in patients with HCC who often have chronic underlying hepatic disease and impaired coagulation status. 4 In this regard, one study reported minor complications related to FAA in 5.5% of TACEs (9/163) and major bleeding in 1.8% of TACEs (3/163) including access site bleeding in two and pseudo-aneurysm in one out of 163 TACEs. 5 Accordingly, the use of a radial artery approach (RAA) may appear as a valuable alternate option because the radial artery is more superficial and can be easily compressed at the end of TACE. In this regard, researchers found that RAA conveys a lower incidence of bleeding complications. 6
The use of RAA has been extensively reported in cardiologic interventions and studies have showed lower mortality rate, 7 lower incidence of major bleeding, 7 improved patients’ comfort 8 and reduced costs 9 compared to FAA. Other studies reported the use of RAA in a variety of intra-arterial procedures with results not different from those obtained with FAA in terms of safety and radiation dose.10–13 RAA is suggested to be the first-line approach for some abdominal procedures such as partial splenic embolization in patients with hypersplenism.14,15 However, to date, FAA remains the most commonly used approach for most embolization procedures in the interventional radiology community, with a FAA: RAA ratio at the advantage of FAA.16–18
In the elective field of TACE, RAA improves patients’ satisfaction and quality of life without compromising procedural variables and safety of TACE.19,20 The technical feasibility of RAA-TACE in HCC is well established5,19,20 However, it is not clear whether the same technical results can be obtained in terms of selectivity of micro-catheterization with RAA-TACE and FAA-TACE. In addition, the incidence of complications with both procedures remains unclear. One study reported a greater incidence of access-site complication with RAA with a rate of radial artery occlusion (RAO) up to 33% (11 out of 33 TACEs) 21 whereas other studies reported lower rates of access site complication with RAA.5,22
The purpose of this study was to compare the technical success rate, the selectivity of TACE, the complication rate, the radiation dose given to the patients and the hospitalization stay between TACE performed using FAA and TACE performed using RAA in patients with HCC.
Material and Methods
Study Population
Our institutional review board approved the retrospective data analysis (AAA-2022-09-021) and waived the need for written consent of the participants due to the retrospective design of the study. The database of our institution was queried to identify all patients with HCC who underwent TACE between June 2020 and April 2022 inclusively. Patients were further excluded when: (i), data regarding the procedure were missing; and (ii), an arterial access other than radial or femoral was used.
TACE Procedure
For all patients, TACE was decided during multidisciplinary tumour board meetings and based on BCLC recommendations (i.e., intermediate BCLC stage (B) and Child-Pugh A or B cirrhosis) in the absence of portal thrombosis and encephalopathy. For each TACE, the selection of RAA or FAA was decided by the radiologists who performed the TACE. All TACEs were performed in an angiography suite equipped with a C-arm fluoroscopic unit (Allura Xper FD20, Philips Health care, Amsterdam, The Netherlands) by a panel of five interventional radiologist with four or more years of experience in TACE, under fluoroscopic guidance and under strict aseptic conditions.
For RAA-TACEs, left radial artery puncture was performed using the Seldinger technique after local anesthesia under ultrasound guidance and a 4-F or 5-F Glidesheath Slender arterial sheath (Terumo, Tokyo, Japan) was introduced. RAA was undertaken after exclusion of patients with abnormal Allen test, radial artery smaller than 3 mm in diameter at ultrasound, non-patent radial artery at Doppler ultrasound and marked arterial tortuosity on pre-TACE computed tomography (CT) examination. Radial cocktail (i.e., unfractionated heparin, 50 units per kilogram; isosorbide dinitrate, 1 mg; verapamil, 2.5 mg) was injected through the arterial sheath. Catheterization of the celiac trunk, superior mesenteric artery or other arteries when needed, was performed using a 4-F or 5-F catheter (Radifocus™ Glidecath™ catheter, Terumo, Tokyo, Japan of 120-cm long; Impress™ of 125-cm long, Merit Medical) and then a 2- to 2.7-F microcatheter (Progreat™ 2.7, Terumo; Maestro™ 2.4, Merit Medical, South Jordan, UT, USA; Pursue™ 2.0, Merit Medical; Occlusafe™, Terumo) was coaxially introduced into the artery(ies) feeding the tumour with a .014- or .016-inch guidewire.
For FAA-TACEs, femoral artery puncture was performed using the Seldinger technique after local anesthesia under ultrasound and fluoroscopy guidance and a 5-F Glidesheath Slender arterial sheath (Terumor) was introduced. Catheterization of the celiac trunk, superior mesenteric artery or other arteries when needed, was performed using a 5-F shaped catheter (Cobra, Terumo; Simmons, Terumo). Then a 2- to 2.7-F microcatheter (Progreat™ 2.7, Terumo; Maestro™ 2.4, Merit Medical; Pursue™ 2.0 Merit Medical; Occlusafe™, Terumo) was placed as distally as possible using a .014- or .016-inch guidewire.
For all RAA- and FAA-TACES, artery(ies) feeding the tumour were selectively catheterized. Two-dimensional angiograms and three-dimensional angiograms using cone-beam CT were obtained to ensure complete tumour coverage. Chemoembolization was performed using conventional TACE or drug-eluting bead-TACE. Conventional TACE was made using 50 mg of doxorubicin and 10 mg of mitomycin C mixed with ethiodized oil (Lipidol®, Guerbet, Aulnay sous Bois, France) with a 1:2 ratio. Particle embolization was made using 100-300 μm Embosphere® (Merit Medical), until complete stasis. Drug-eluting bead-TACE was made using 50 mg of doxorubicin and two vials of beads (DC Bead™, Boston Scientific, Marlborough, MA, USA) diluted with 10 mL of normal saline and 10 mL of iodinated contrast material. The mixture was delivered until complete stasis was achieved.
After TACE, the arterial sheath was removed immediately. Manual compression was used for hemostasis after RAA-TACE whereas after FAA-TACE, the use of closure device or manual compression was left at the operator preference. When a vascular closure device was used (FemoSeal™ 7-F, Terumo), patients were assigned to remain in bed for 6 hours. When used, manual compression lasted 10 minutes and was followed by a compression bandage, and patients were asked to remain in bed for at least 8 hours. Bed restrictions were not recommended after RAA but patients were asked to limit wrist joint movement. Patients were discharged 24 hours after TACE.
Data Collection, Definitions, and Outcome
The study coordinator (M. H.) retrospectively evaluated the selectivity of the catheterization during TACE procedure by assessing how distally the catheter or the micro-catheter was placed before embolization using the radiology reports and by viewing the images and the cine loops of all TACEs using the picture archiving and communication system of our institution. Selectivity was classified into three categories as hemihepatic, sectorial or segmental depending on the location of the distal tip of the catheter/microcatheter during chemoembolization (i.e., in the first division of the hepatic artery, in a sectorial arterial or in a segmental artery, respectively). Radiology reports were also analyzed with respect to technical failure (defined as the inability to perform the chemoembolization and the need to either postpone the intervention or use FAA [i.e., crossover]), early or late access sites complication such as arterial occlusion, hematoma at the puncture site or pseudoaneurysm, radiation exposure with dose area product (DAP) and fluoroscopy time. The study coordinator also reviewed hospitalization charts of all patients to determine the hospitalization duration. Finally, the study coordinator reviewed the consultation charts of the patients obtained during a follow-up evaluation at 30 days after TACE for the presence of delayed complications such as arterial access thrombosis or pseudoaneurysm. For all complications, the CIRSE classification system for complications was used. 23
Statistical Analysis
Statistical analyses were performed with MedCalc 13 (MedCalc, Ostend, Belgium). Categorical variables were expressed as raw numbers, proportions and percentages and compared using Fisher exact tests. Continuous variables were expressed as means ± standard deviations (SD) and ranges or medians, interquartile ranges (Q1, Q3) depending on the normality of the distribution and compared using Student t test 24 All tests were two-sided and a P value <.05 was considered to indicate statistically significant difference.
Results
Study Cohort
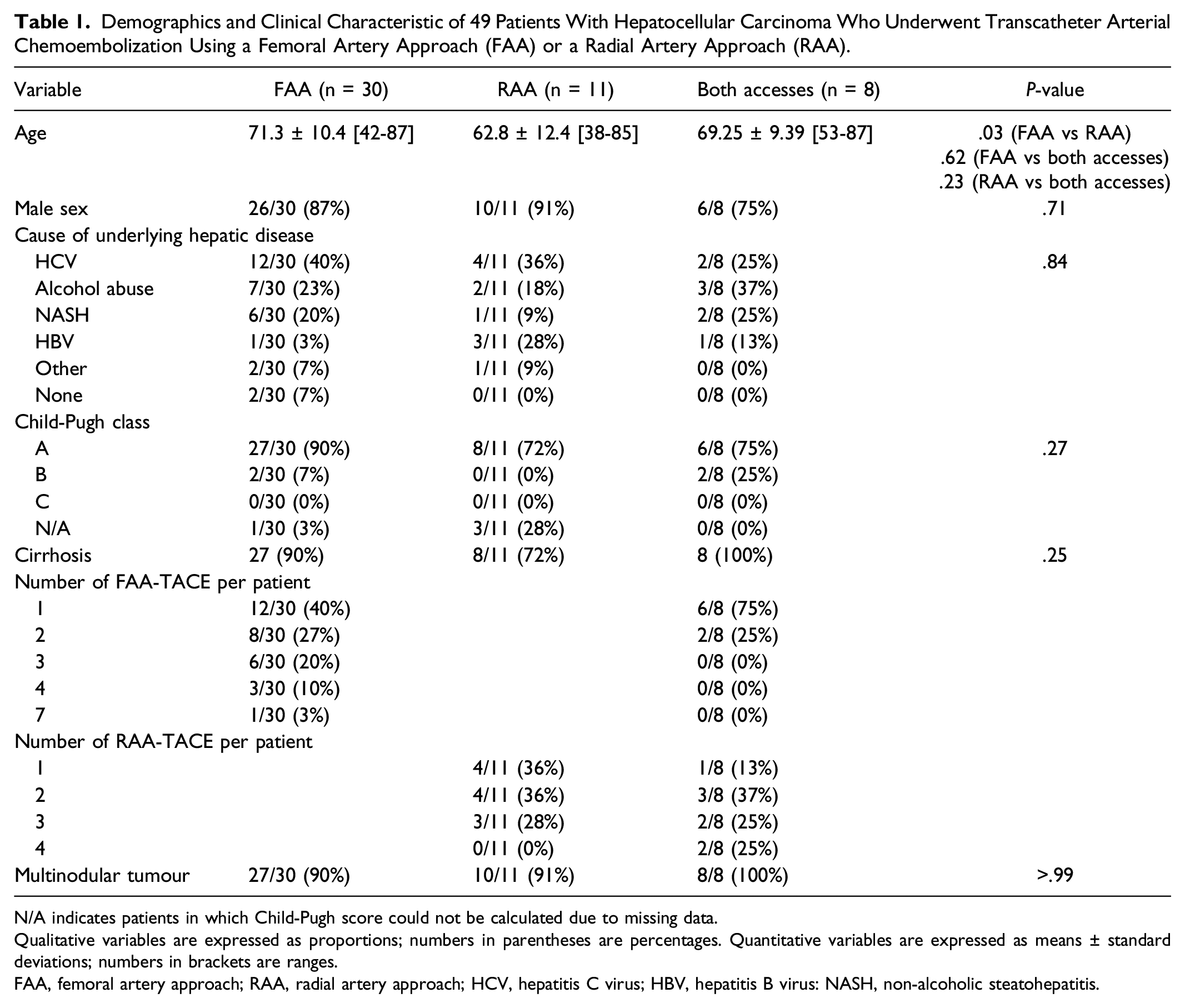
A total of 53 patients who underwent 120 TACEs were initially retrieved. Of these, 4 patients with 4 TACEs were excluded due to missing data (n = 2) or because of the use of a humeral artery access (n = 2). The final study population included 49 patients who underwent 116 TACEs. The flow chart of the study is showed on Figure 1. No patients has FAA due to abnormal Allen test, radial artery < 3 mm, non-patent radial artery or marked arterial tortuosity on pre-TACE CT. The demographics and clinical characteristics of the 49 patients are reported in Tables 1 and 2. Thirty patients had FAA only, representing a total of 65 (65/116; 56%) TACEs; of these 12 patients had only one TACE and 18 had multiple TACEs (8 had 2 TACEs, 6 had 3 TACEs, 3 had 4 TACEs and 1 has 7 TACEs). Eleven patients had RAA only, representing a total of 28 (28/116; 24%) TACEs; of these, 4 patients had only 1 TACE and 7 had multiple TACEs (1 had 2 TACEs, 2 had 3 TACEs and 4 had 4 TACEs). Eight patients had both FAA and RAA, representing a total of 23 TACEs (10 with FAA and 13 with RAA). Study flow chart. HCC indicates hepatocellular carcinoma; TACE indicates transarterial chemoembolization. Demographics and Clinical Characteristic of 49 Patients With Hepatocellular Carcinoma Who Underwent Transcatheter Arterial Chemoembolization Using a Femoral Artery Approach (FAA) or a Radial Artery Approach (RAA). N/A indicates patients in which Child-Pugh score could not be calculated due to missing data. Qualitative variables are expressed as proportions; numbers in parentheses are percentages. Quantitative variables are expressed as means ± standard deviations; numbers in brackets are ranges. FAA, femoral artery approach; RAA, radial artery approach; HCV, hepatitis C virus; HBV, hepatitis B virus: NASH, non-alcoholic steatohepatitis. Demographics and Clinical Characteristics of 116 TACEs for Hepatocellular Carcinoma. N/A indicates patients in which Child-Pugh score could not be calculated due to missing data. Qualitative variables are expressed as proportions; numbers in parentheses are percentages. Quantitative variables are expressed as means ± standard deviations; numbers in brackets are ranges. FAA, femoral artery approach; RAA, radial artery approach; HCV, hepatitis C virus; HBV, hepatitis B virus: NASH, non-alcoholic steatohepatitis.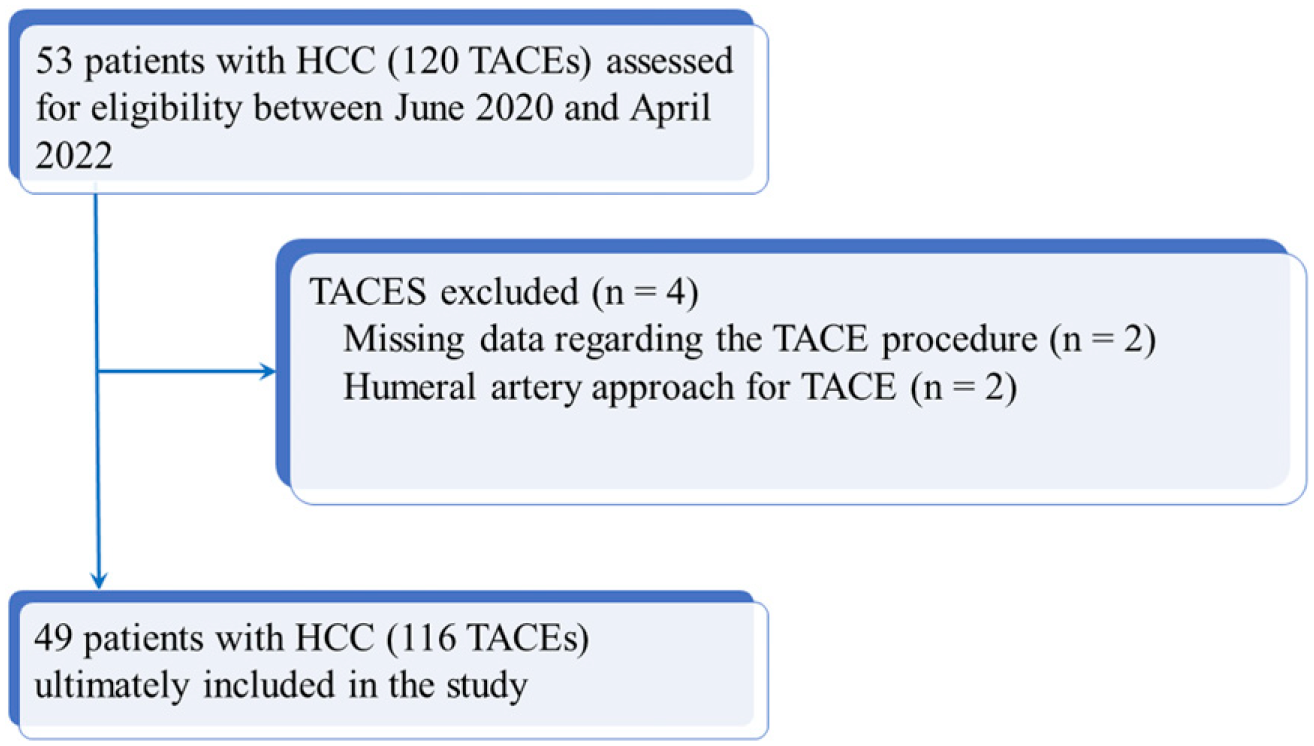
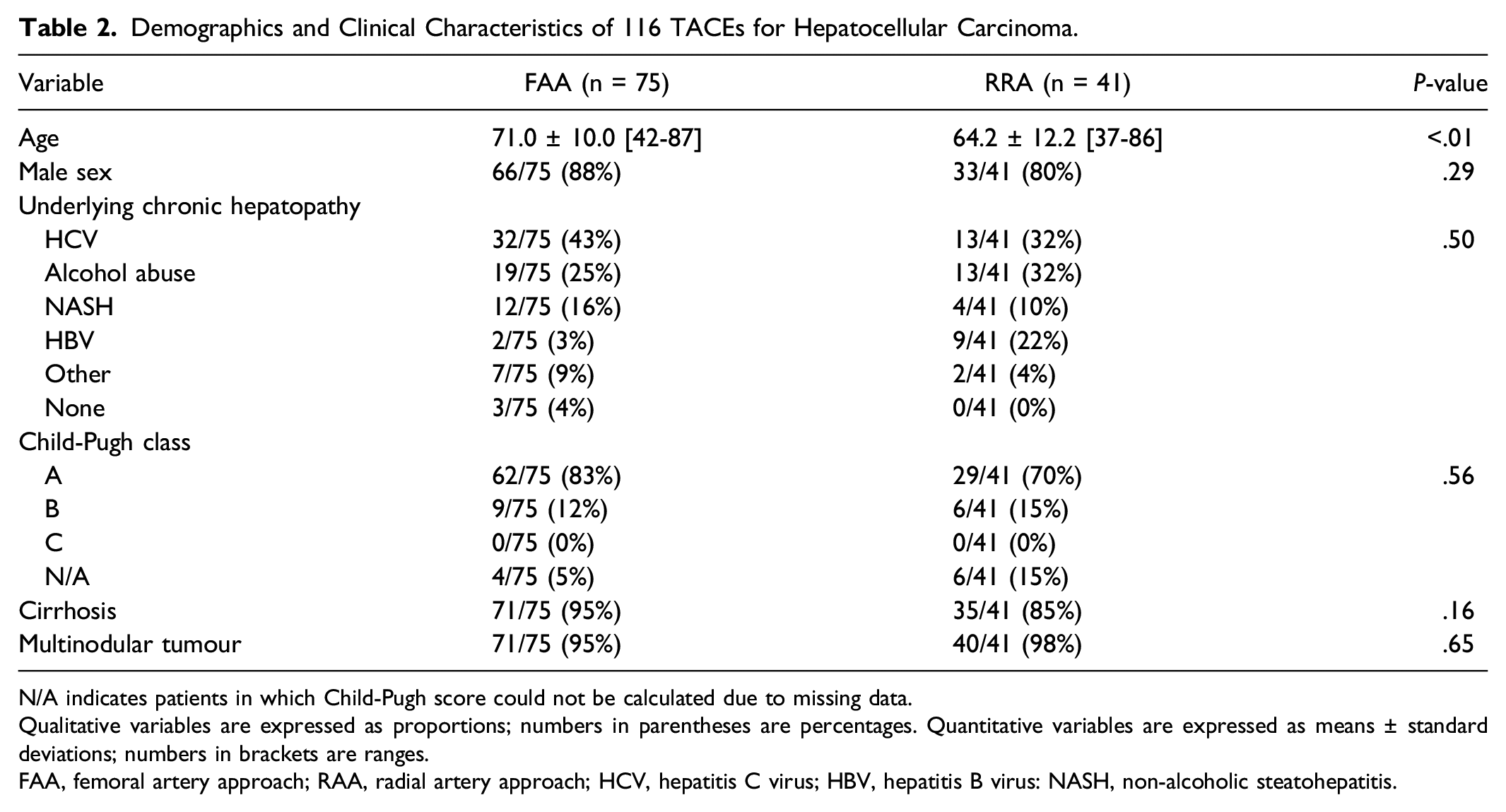
Baseline characteristics of the population were not different except for age, which was significantly lower in the RAA group (64.2 ± 12.2 [SD] years) than in the FAA group (71.0 ± 10.0 [SD] years) (P < .01) (Table 2).
Technical Success and Complications
Technical success was achieved in 39/41 (95%) TACEs with RAA and in 75/75 (100%) TACEs with FAA (P = .12). Reasons for technical failure with RAA were inability to catheterize the celiac trunk (n = 1) and radial artery spasm during TACE (n = 1) in 2 different patients. For these 2 patients, TACE was performed with FAA, resulting in 2 occurrences of crossovers with RAA.
Clinical Data and Outcomes of 116 TACE Procedures in 49 Patients With 164 Hepatocellular Carcinoma Nodules.
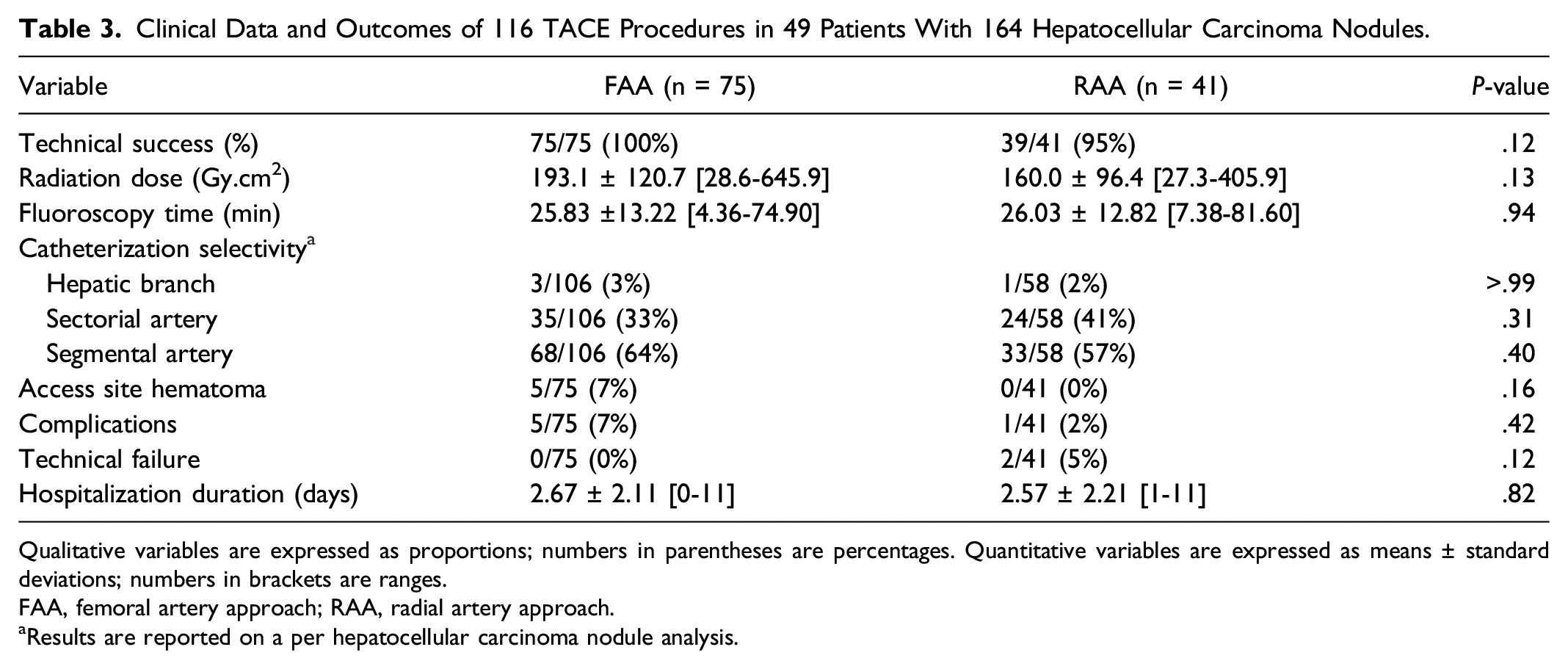
Qualitative variables are expressed as proportions; numbers in parentheses are percentages. Quantitative variables are expressed as means ± standard deviations; numbers in brackets are ranges.
FAA, femoral artery approach; RAA, radial artery approach.
aResults are reported on a per hepatocellular carcinoma nodule analysis.
In term of access site complication, 5 post TACE hematomas (Grade 2 of the CIRSE classification system for complication) were reported with FAA (5/75; 7%) vs. none with RAA (0/41; 0%) (P = .16). All 5 hematomas were self-limited and were treated with manual compression only. One occurrence of RAO classified as Grade 1 complication, was reported after RAA in 1 patient (1/41; 2%) whereas no femoral artery occlusion was reported (0/75; 0%) (P > .99). RAO was asymptomatic and incidentally found during the next TACE session. When considering the total of complications, no differences were observed between FAA (5/75; 7%) and RAA (1/41; 2%) (P = .42).
Radiation Exposure and Hospitalization Duration
In terms of radiation exposure, no differences were found in mean DAP between RAA (194.8 ± 124.5 [SD] Gycm2) and FAA (194.8 ± 124.5 [SD] Gycm2) (P = .24). No differences in fluoroscopy time were found between RAA group (26.03 ± 12.82 [SD] min) and FAA group (25.83 ± 13.22 [SD] min) (P = .94).
No differences in hospitalization stay duration were found between FAA (2.67 ± 2.11 [SD] days) and RAA (2.57 ± 2.21 [SD] days) (P = .82).
Discussion
In this study, we observed no differences in technical success rates between RAA (93%; 39/41 patients) and FAA (100%; 75/75 patients) (P = .12). In addition, no differences in terms of selectivity of catheterization, complication rate, radiation dose, fluoroscopy time and hospitalization stay were found between RAA and FAA. All these results support the use of RAA for TACE, considering the specific advantages of RAA compared to FAA in terms of patients’ satisfaction.8,19
In our study, we achieved a technical success rate of 95% (39/41) in the RAA group, which is similar to the results of Du et al. who reported a technical success rate of 95% (152/160) in the RAA group and 98.8% (161/163) in the FAA group, with no differences between the two approaches (P = .102). 5 Similarly, Ghosh et al. reported a 100% technical success rate between RAA (90/90) and FAA (56/56). 25 In another study, Wan et al. reported 92.3% (24/26) technical success rate for hepatic arterial infusion chemotherapy using RAA and 100% (43/43) technical success rate using FAA in their retrospective cohort (P = .139) and 100% technical success rate using RAA or FAA in their prospective cohort. 21 The same results were reported by Iezzi et al. who found 100% technical success rates for TACE using either RAA or FAA. 20 Our results provide further evidence on the technical efficacy of RAA for TACE in patients with HCC.
Regarding selectivity of TACE, we found no differences between RAA and FAA. RAA requires the use of longer catheters and microcatheters than FAA, which provide less support for the procedure and may be more vulnerable to respiratory motions. 26 Moreover, selectivity of TACE may be affected by patient anatomy. In this regard, RAA-TACE may be made more difficult with tall patients or with those with tortuous aorta or an ascending celiac trunk. With these concerns, we compared the selectivity of the micro-catheterization in both groups but found no differences in terms of selectivity of TACE. However, one study reported an improved efficacy of TACE in patients with HCC with a better tumour response rate using RAA (30.5%) compared to FAA (18.6%) (P = .024), assumably because of a lower rate of arterial spasm using RAA and a better access of chemotherapy to the target tumour. 22
In our study, six patients had minor access site complications (Grade 1 or Grade 2 complications) in the form of hematoma after FAA vs. one in the form of RAO after RAA, although the difference was not significant (P = .42). This result is consistent with those of previous studies.5,22 Du et al. reported lower rates of complication with RAA (3 out of 112 patients; 2.7%). 5 You et al. reported two puncture site hematomas (1.4%; 2/143) using FAA compared to zero (0%; 0/131) using RAA, although the difference was not significant (P = .499). 22 Although major hemorrhagic events are rare, they can be life-threatening and are more frequent using FAA. de Fina et al. reported seven puncture-site complications in 253 patients with HCC who underwent a total of 449 TACE using FAA 27 ; of these, there were two hematomas (.44%), two pseudoaneurysms (.44%), two limb ischemias (.44%) and one femoral artery dissection (.22%). 27 Of interest, no post procedure stroke was observed in our study. Due to this theoretical risk, all RAA TACE were performed with a left artery access, when possible.
Regarding artery occlusion at the puncture site, we observed only one occurrence of RAO in one patient (2%) who underwent RAA-TACE. This is consistent with the results of Du et al., who reported a rate of asymptomatic RAO of 2.7%, with RAO occurring in three patients out of 113 patients who underwent RAA-TACE, 5 or with the results of Restrepo et al., who reported one occurrence of RAO in 120 diverse intra-abdominal procedures. 28 RAO is a common complication of RAA (incidence of 7.7% at one month) 29 that might be underestimated in most studies due to the lack of systematic control of the radial artery by ultrasound at one month.
In our study, we found no differences in radiation dose given to the patient and fluoroscopy time between RAA and FAA. This is consistent with the results of Ghosh et al. who found no differences in terms of radiation dose between RAA (mean, 1578.9 mGy) and FAA (mean, 1383.0 mGy) (P = .08) and in terms of fluoroscopy time (26.8 min vs. 24.8 min, respectively (P = .23). 25 Similarly, Yamada et al. reported no differences in median radiation dose given to the patient between RAA (811 mGy) and FAA (1200.5 mGy) (P = .229) in 36 patients with HCC who underwent either transarterial bland embolization or TACE. 30 In a study involving 42 patients undergoing TACE with successive RAA and FAA, Iezzi et al. found no significant differences in term of fluoroscopy time between RAA (399.6 ± 85.8 [SD] s) and FAA (356 ± 26 [SD] s) (P = .071). 20 In the more general field of hepatic interventions, a systematic review based on 1096 procedures including TACEs, transcatheter arterial radioembolizations and hepatic arterial infusion chemotherapies, reported no differences in radiation dose (weighted mean difference, −13.11; P = .94) and fluoroscopy time (weighted mean difference, .85; P = .52) between RAA and FAA. 31 Other authors reported no significant differences in dose area products and fluoroscopy time between RAA and FAA in other intra-arterial procedures such as splenic or renal embolizations.12,13
In our study, no differences in hospitalization duration were found between RAA and FAA (P = .99). One reason may be the fact that most of the patients were not hospitalized only for TACE but also for the care of their underlying hepatopathy. This is in contrast with the results of You et al. who found significantly longer hospitalization stay in the FAA group (9.63 ± .35 [SD] days) by comparison with the RAA group (8.42 ± .36 [SD] days) (P = .01). However, this may be due to local policy of adverse events management at the authors’ institution. 22
Beyond the variables evaluated in our study, studies showed that RAA improves patients’ satisfaction compared to FAA.8,19,32 In a randomized controlled trial, Zhang et al. compared RAA to FAA in 130 patients with HCC who underwent TACE. 19 They found that significantly more patients preferred RAA for a next procedure compared to those who had FAA. Another study by Liu et al. on the topic of radioembolization compared 30 patients who underwent transarterial radioembolization using both RAA and FAA. 32 These researchers reported lower post procedure pain scores (2.0 vs. 2.9, P = .0046; 2.0 vs. 3.0, P = .0004; 2.1 vs. 2.9, P = .0357). In this study, 22 patients (73.3%) preferred the RAA, 4 patients preferred the FAA and 4 patients had no preference. 32 A study of 42 patients undergoing TACE with successive RAA and FAA showed improved comfort after the procedure particularly less discomfort at access route after procedure (P < .001) and less patient dependence after procedure (P < .001). 20 One of the main explanations was the fact that RAA enables early ambulation.
Our study has several limitations. First, it is an observational, retrospective, single center study, which may lead to selection bias. In this regard, patients who underwent RAA-TACE where those with anatomic characteristics favorable for RAA. Moreover, patients who underwent RAA were older than those who underwent FAA. It may be thus argued that age might be a confounding factor because older patients were more prone to complications and technical failure. In addition, due to the relatively small sample size and limited study power, small differences in technical success or complication rates between the two approaches might have been overlooked. Second, the cost-efficiency of RAA compared to that of FAA for TACE was not evaluated. However, several studies reported no differences in hospitalization expenses between the two approaches.22,25 Third, the choice between RAA and FAA was left to the operator preference, which might have introduced bias due to selection of one approach over the other in light of patients’ specificities, and limited the generalizability of our results. 33 Finally, we did not assess the differences in local pain at the puncture site between the two approaches. 34
In conclusion, the results of this study suggest that for patients with HCC, RAA is a safe approach that does not compromise the technical efficacy of TACE compared with FAA, in particular regarding the selectivity of the embolization. Considering the benefit of RAA in terms of patient satisfaction, this approach should be encouraged for TACE in patients with HCC.
Footnotes
Author Contributions
All authors attest that they meet the current International Committee of Medical Journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Attestation Statement
Data regarding any of the subjects in the study have not been previously published.
Data Availability Statement
Data will be available upon reasonable request.