
Abstract
Abdominal emergencies in cancer patients encompass a wide spectrum of oncologic conditions caused directly by malignancies, paraneoplastic syndromes, reactions to the chemotherapy or often represent the first clinical manifestation of an unknown malignancy. Not rarely, clinical symptoms are the tip of an iceberg. In this scenario, the radiologist is asked to exclude the cause responsible for the patient’s symptoms, to suggest the best way to manage and to rule out the underlying malignancy. In this article, we discuss some of the most common abdominal oncological emergencies that may be encountered in an emergency department.
Introduction
Due to the rapidly increasing elderly population, there has been an increase in the diagnosis of cancer and a rise in oncological emergencies. Oncologic emergencies can result from local effects of the primary tumour, its metastases, paraneoplastic syndromes, or reaction to the chemotherapeutic agents.
1
–11
Many oncological emergencies are signs of advanced, stage IV disease, but occasionally patients present to the emergency department (ED) with a previously unknown primary tumour responsible for acute clinical symptoms. Imaging plays a crucial role in both the initial diagnosis and therapeutic decision process. Depending on the severity, type and localization of the clinical symptoms, the initial imaging evaluation in the ED traditionally begins with a chest radiograph, abdominal radiograph, or abdominal ultrasound (US) because of their wide availability, low cost, and minimal or no exposure to radiation.
12
However, contrast-enhanced computed tomography (CT) scan is the imaging modality of choice in the evaluation of oncological patient presenting to the ED with an acute abdomen
12
–14
Figure 1. 56 year old woman who presents with shortness of breath, abdominal discomfort, and back pain. On examination, she has frank ascites. (A, B, C) Axial contrast-enhanced MDCT scans show a large heterogenous mass of ovarian origin in the right iliac fossa, with evidence of the right ovarian vein seen entering the mass (B), moderate volume of ascites with large volume omental caking (C) and a serosal deposit on the surface of the liver (D, arrow).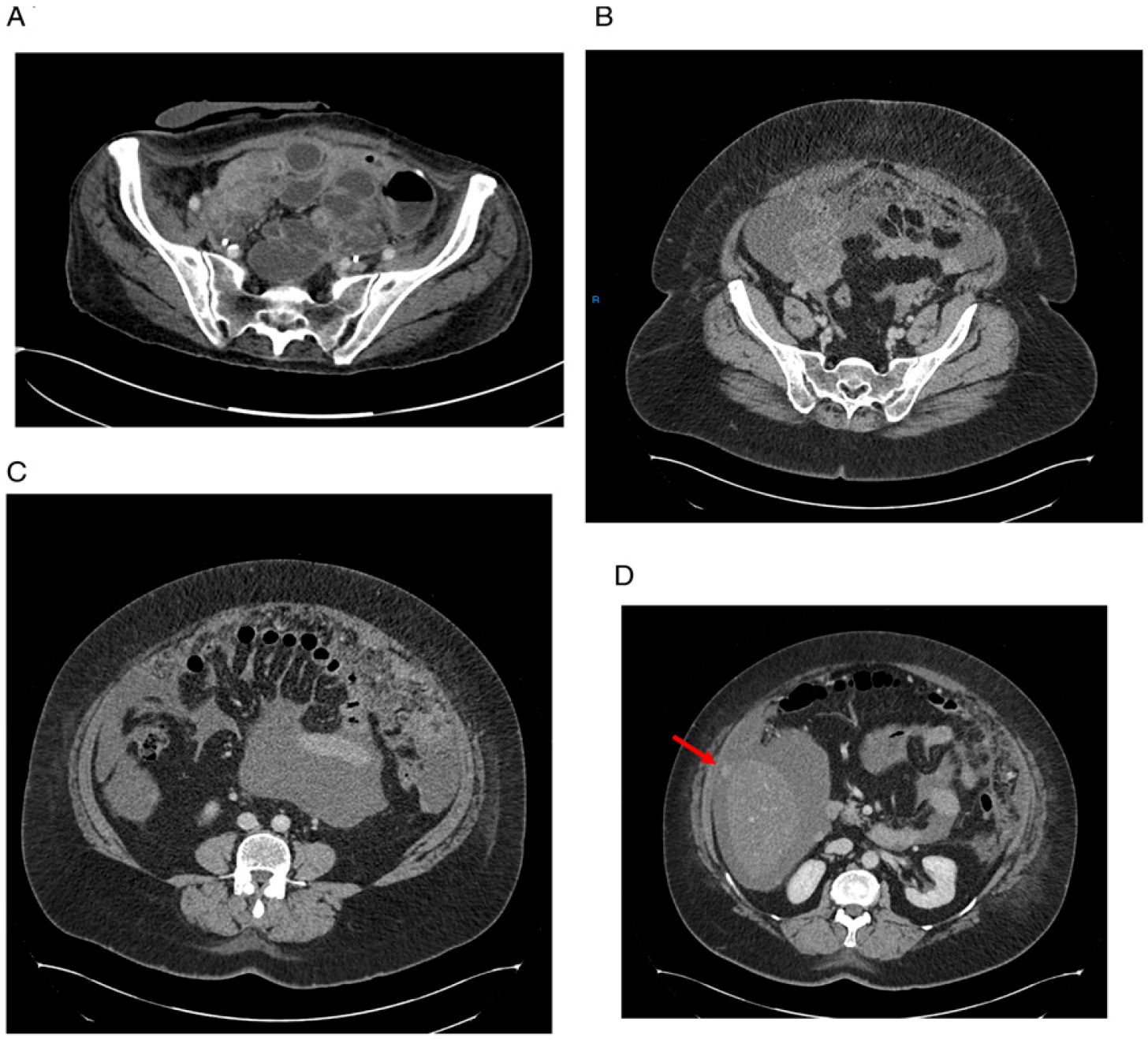
Abdominal pain and acute abdomen are common presentations of several intraabdominal oncological-related conditions and may constitute the first presentation of cancer or may be due to disease complication. 10 The signs and symptoms include fever, elevated white blood cell count, intestinal obstruction, peritonitis, anemia, elevated liver enzymes, jaundice, renal failure, hematuria, and intestinal obstruction. 15
In this article, we will review the common abdominal oncological emergencies which are encountered frequently in the ED and the role of radiologists in the emergency setting.
Obstruction
Cancer patients can experience symptoms of obstruction of different structures due to various causes. 9 A substantial number of obstructions is benign in nature and not caused by tumour mass. 16 –21
Obstruction of the Gastrointestinal Tract
Obstruction can occur anywhere along the gastrointestinal tract. In some cases, this represents the initial symptom of a neoplasm, whereas in others it develops during the course of disease. A malignant bowel obstruction (MBO) can be defined as 1 of the following: clinical evidence of bowel obstruction (by history, physical, and/or x-ray examination); bowel obstruction beyond the ligament of Treitz in the setting of a diagnosis of intra-abdominal neoplasm; or a diagnosis of extra-abdominal primary cancer with clear intraperitoneal disease. 14 As a result, many therapeutic options can be offered for these patients, and because MBOs rarely need to be managed urgently, the whole clinical team, patient, and family have time to consider these options in the perspective of the patient’s goals of care and underlying load of disease. 15 –20
Obstructions can be classified as either partial or complete. In partial obstruction, gas or liquid stool can pass through the point of intestinal narrowing. With complete obstruction, no content can pass. Such obstructions can be secondary to mechanical or functional disease. Mechanical obstructions can be classified as intraluminal (enlarging primary or secondary tumour), intramural (infiltration of the bowel wall), or extramural (extrinsic compression from masses, nodes, or adhesions). 1 Functional obstruction is characterized by an ileus (ie, spastic, hypotonic or paralytic ileus). 19 This can result from tumour infiltration of the mesentery that affects the bowel wall muscle and nerves, or it can be induced by the many pain medications used by this population. Ileus may also result from a paraneoplastic neuropathy, particularly in patients with lung cancer. 1 In the context of a mechanical obstruction, distinction should be made between simple and closed-loop obstruction. 21 –27 This is not just a theoretical distinction, because it has critical implications on management and patient’ outcome. Simple obstruction occurs when the intestinal lumen is partially or completely occluded at 1 or more points, thus resulting in a proximal dilatation and distal collapse of the bowel. In contrast, closed-loop obstruction occurs from 2 sequential occlusions at 2 adjacent points.
Small-bowel obstruction is 1 of the more frequent causes of acute abdomen, representing 20% of all surgical admissions for acute abdominal pain. 19 The incidence of intestinal obstruction due to neoplasm accounts for approximately 5%-15%. 26,27 Small bowel obstruction is more common than large bowel obstruction. 21 Small-bowel neoplasms are quite unusual. This may represent a diagnostic challenge since they usually present with nonspecific symptoms resulting in diagnostic delay with development of carcinomatosis, advanced stage IV disease, direct invasion or lymphatic system and hematogenous metastases. 2
Abdominal plain radiography should be performed as initial radiologic screening for suspected bowel obstruction as it has 60%-93% sensitivity in the diagnosis.
US is usually performed as first-line examination, as it is non-invasive, promptly available, and easily performed. US is a valid adjunct to plain film to define the presence of free fluid and to distinguish between functional (spastic, hypotonic and paralytic ileus) from mechanical obstruction looking at peristalsis and intestinal wall thickness. 19 This is important to establish if surgery is needed and the timing of intervention. 22,23
Contrast-enhanced CT is indicated for as overall assessment of the neoplastic obstruction and its complications. 22 –26 The contrast-enhanced CT allows rapid assessment of the features of bowel obstructions including variation of wall enhancement which can show increased of decreased attenuation compared to the loops not involved in the obstructing process, determining the need for a prompt surgical approach. 24,25
The most common protocol in our centers include portal venous phase scan with injection of 80-120 mL nonionized iodinated IV contrast agent followed by 20 mL of saline solution, at 3-5 mL/s with scanning from the diaphragm to the symphysis pubis.
Intravenous contrast medium administration is essential for assessing intestinal loop enhancement and mesenteric vascular supply. 2,25,26
The axial slice is typically thin (1.5 mm) for all pre- and post-contrast acquisitions, but further thick-slice 3.75 mm axial and other 3 to 5 mm coronal and sagittal planes (MPR and MIP) are obtained in order to get the transition zone localizatio), and then possible identify the obstruction cause, visualizing the “bowel and mesenteric complex”. The use of oral contrast material is controversial and usually not administrated in the first assessment of a SBO. 28
Multi-detector computed tomography (MDCT) has a high accuracy for the diagnosis of severe SBO (almost 95%) but it is less sensitive and specific in case of partial obstruction (with a variable range of 83-100% in sensitivity and 61-93% in specificity). 2,24 –27,29
Because of the multitude of differential diagnoses (ranging from bleeding hypervascular metastases to carcinomatosis), more recent publications have investigate the role of biphasic CT protocol in suspected small bowel obstruction at the emergency department. The positive predictive value of biphasic MDCT accounts for 92.9% for AMI, indicating the possibility to reduce patient radiation dose, numbers of images to review and unnecessary delays in patient work-up. 25
Large bowel obstruction (LBO) is much less common than SBO and frequently caused by an underlying malignancy. Other etiologies include diverticulitis and volvulus of the sigmoid colon or cecum. In the setting of a malignant LBO, the cause is frequently an intraluminal tumour growth, but it can also be the result of intussusception from a neoplastic leading point. Up to 20% of patients with colorectal cancer develop a LBO, which can have a substantial morbidity and mortality. Postoperatively, up to 25% of patients with a colorectal cancer resection develop a LBO.
2,30
Similar to SBO, mechanical obstruction of the large bowel causes bowel dilatation above the site of obstruction but it usually takes longer time for patient to present with symptoms of obstruction. Therefore, it rarely is an emergency until in the latest stages (for example, a stenosing cancer causing caecal dilatation over 8 cm) (Figure 2).
2
Furthermore, it is crucial for the team to distinguish between LBO and non-obstructive causes of large bowel dilation, such as a toxic megacolon. In this context, serial plain films play a crucial role to monitor evolution of disease.
30
69 year old man presenting with fecaloid vomiting, abdominal distention and bloody stools. (A) Axial contrast-enhanced CT scan shows a large solid mass in the descending colon (circle) obstructing the upstream large bowel. Note the large dilatation of the ascending colon exceeding 8 cm which indicates the need for an emergency laparotomy. (B) Sagittal MPR reconstruction offers a different spatial perspective of the colonic lesion (circle) and the obstructed large and small bowel loops.
The latter refers to dilation of the colon associated with acute colitis, either segmental or diffuse, without associated mechanical obstruction. A wide range of etiologies can result in acute colitis including inflammation, ischemia, infection or radiation. Symptoms of LBO may develop over several days.
Depending on the patency of the ileocecal valve, these symptoms can eventually progress to nausea and vomiting. Contrast-enhanced CT is the gold standard in the emergency setting to detect the site of obstruction, the extent of the primary malignancy or distant metastases which affect the subsequent procedural planning. 30
Bowel Perforations
Bowel perforations is 1 of the most serious complication of gastrointestinal tumour. It requires prompt diagnosis and surgical treatment as it is frequently associated with sepsis. 3 –5
Clinical presentation is variable, especially if the patients are old or severely ill, but it usually presents as an “acute abdomen.” In oncologic patient, perforation may be due to the necrosis of the neoplastic bowel wall that is caused by a rapid growth and lack of blood supply, or secondary to chemotherapeutic agents. 31 Gastrointestinal tumour perforation causes severe septic status but also spread of cancer cells in the peritoneal cavity with poor prognosis.
Chest and abdominal radiographs are the most frequently requested imaging modality even if their role is limited. 28 In the context of peritonitis, the detection of free intraperitoneal air on the radiograph is usually related to bowel perforation. 29 However, it should be remembered that abdominal free gas and bowel perforation are not always connected and free air can be related to thoracic, mediastinal and/or retroperitoneal issues. The specificity of radiograph for pneumoperitoneum is 50%-89.2%, but the site of perforation is almost never identified. 19 Contrast-enhanced CT is the imaging modality of choice for identifying the presence, location, and cause of bowel perforation. 29 The CT diagnosis of bowel perforation is based on direct CT findings, such as discontinuity of the bowel wall (a rare finding) and the presence of extraluminal air as well as indirect CT findings, such as bowel wall thickening, abnormal bowel wall enhancement, abscess, and inflammatory mass adjacent to the bowel or an ileus. Scrutinizing and comparing the axial scans and MPRs to look for the site of perforation is essential. Of note that in many cases the site of bowel perforation remain unknown even at CT. 21 Nevertheless, it should be emphasized that in many cases abdominal plain radiographs and/or even initial CT may show no gas or fluid in the peritoneal cavity at all but just an ileus.
Intestinal Infarctions
Mesenteric ischemia in oncologic patients may develop due to the direct involvement of vascular structures by the neoplasm, paraneoplastic syndrome causing hypercoagulability and consequent embolism or thrombosis of the mesenteric vessels, or secondary vascular involvement in malignant bowel obstruction. 2 Mesenteric ischemia includes acute arterial mesenteric ischemia, acute venous mesenteric ischemia, non-occlusive mesenteric ischemia, ischemia or reperfusion injury and ischemic colitis. Symptoms may be subtle and difficult to recognize since they are unspecific and may mimic other pathological conditions. 32 –37 Early diagnosis is important to improve survival rates. In most cases of late or missed diagnosis, the mortality rate from intestinal infarction is very high, with a reported value ranging from 60% to 90%. 31,36,37 MDCT is a crucial examination that should be immediately done in all patients with a suspicious ischemic bowel. 38 –40 Its diagnostic yield is much improved compared to the past and currently it is superior to that of any other noninvasive technique. 39,40 Contrast-enhanced CT can differentiate occlusive mesenteric ischemia vs non-occlusive mesenteric ischemia, which may have different therapeutic implications and options. Furthermore, contrast-enhanced CT is absolutely crucial to make any alternative diagnosis requiring a prompt surgical assessment, which is particularly useful in the cancer and elderly population. 31 –42
Abdominal Bleeding
Bleeding complications in cancer patients may be secondary to coagulation disorders, tumour rupture, or vascular involvement from neoplasm. Abdominal bleeding is a rare complication that may be fatal, so prompt diagnosis and treatment are required.
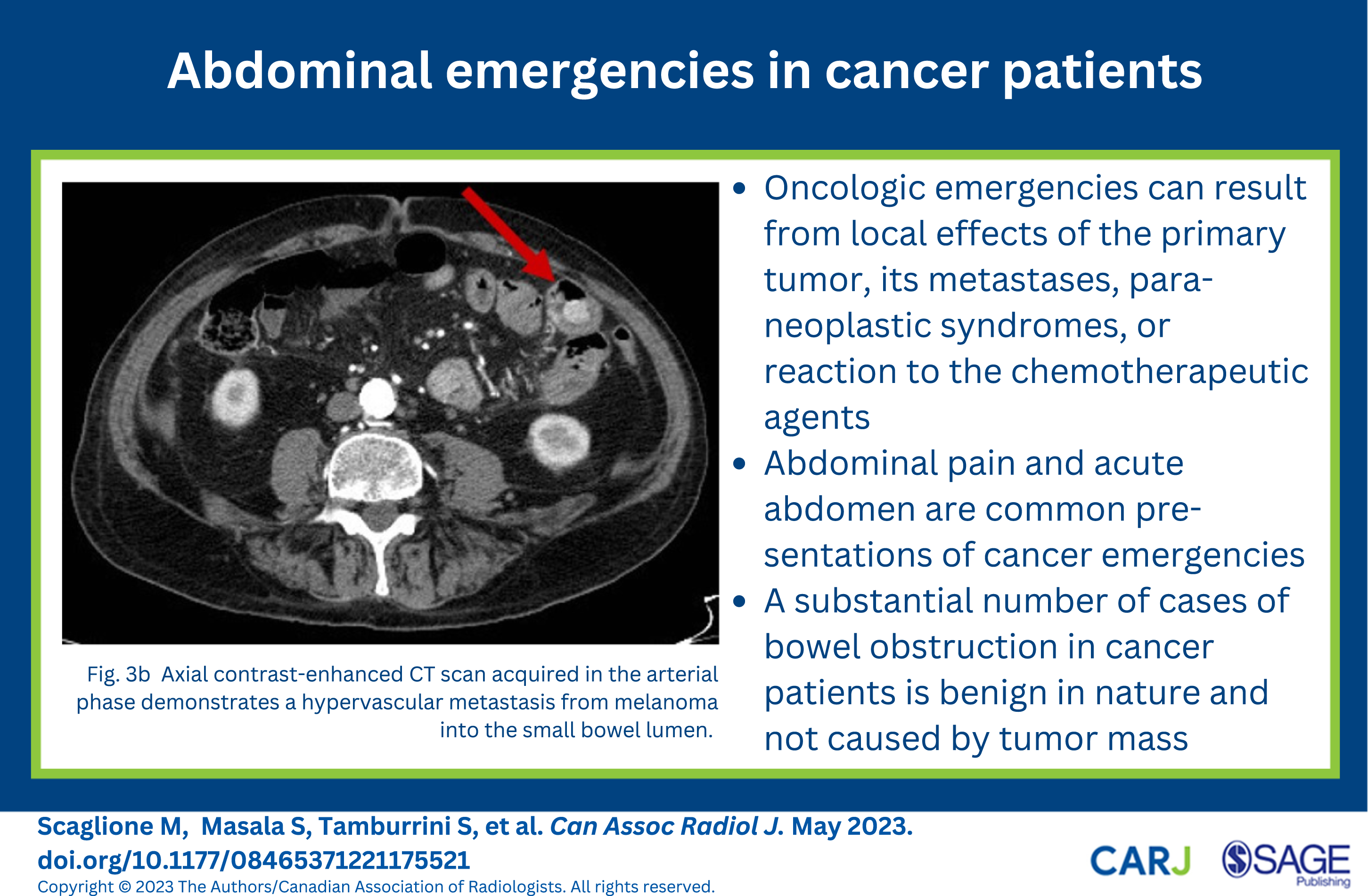
Spontaneous bleeding can occur mainly in hypervascular tumours, primarily localized peripherally and/or in subcapsular parenchymal spaces, such as hepatocellular carcinoma, renal cell carcinoma, and metastasis from melanoma.
43
–45
Figure 3. Furthermore, patients with hematologic malignancies may present with spontaneous hepatic or splenic rupture. Hepatocellular carcinoma is complicated by rupture with intraperitoneal hemorrhage in 3%-15% cases resulting in about 70% mortality, and renal cell carcinoma, most commonly the clear cell variant, is similarly complicated in .3%-1.4% of cases.
2
Figure 4. If abdominal haemorrhage is suspected, contrast-enhanced CT is the examination of choice allowing to detect the site of bleeding, its severity, and whether it is arterial or venous.
43
If it is arterial, digital angiography of the visceral arteries may confirm the source and allow the embolization of the bleeding vessel. However, when choosing the CT protocol (monophasic vs biphasic protocol), it should be desirable to know the histological type of cancer.
44
In cases of melanoma, breast cancer, papillary thyroid carcinoma, lung cancer, HCC, GIST, or RCC, it is essential to adopt a biphasic protocol (with an arterial phase) to avoid missing or confusing hypervascular metastasis.
2,45
80 year old man admitted with abdominal pain, sweats and dropping haemoglobin. The patient had an excised melanoma in the right goin 15 years earlier. (A, B, C). Axial contrast-enhanced CT scans acquired in the arterial phase demonstrates hypervascular lesions within the lumen of the gallbladder (A, arrow) and the small bowel. Note that in the portal phase these lesions appear hysodense and could be easily misinterpreted as fecal matter. 65 year old man presenting with abdominal pain and shock. No hepatic cirrhosis or any other disease in his previous medical history. (A) Contrast-enhanced MDCT shows a large hypervascular solid lesion at the segment IV of the liver and a further relatively small lesion at segment I (B, arrows) consistent with multifocal HCC associated with a jet of active bleeding and a large volume of mixed density ascites with clotted blood (B, C) in the peritoneal cavity.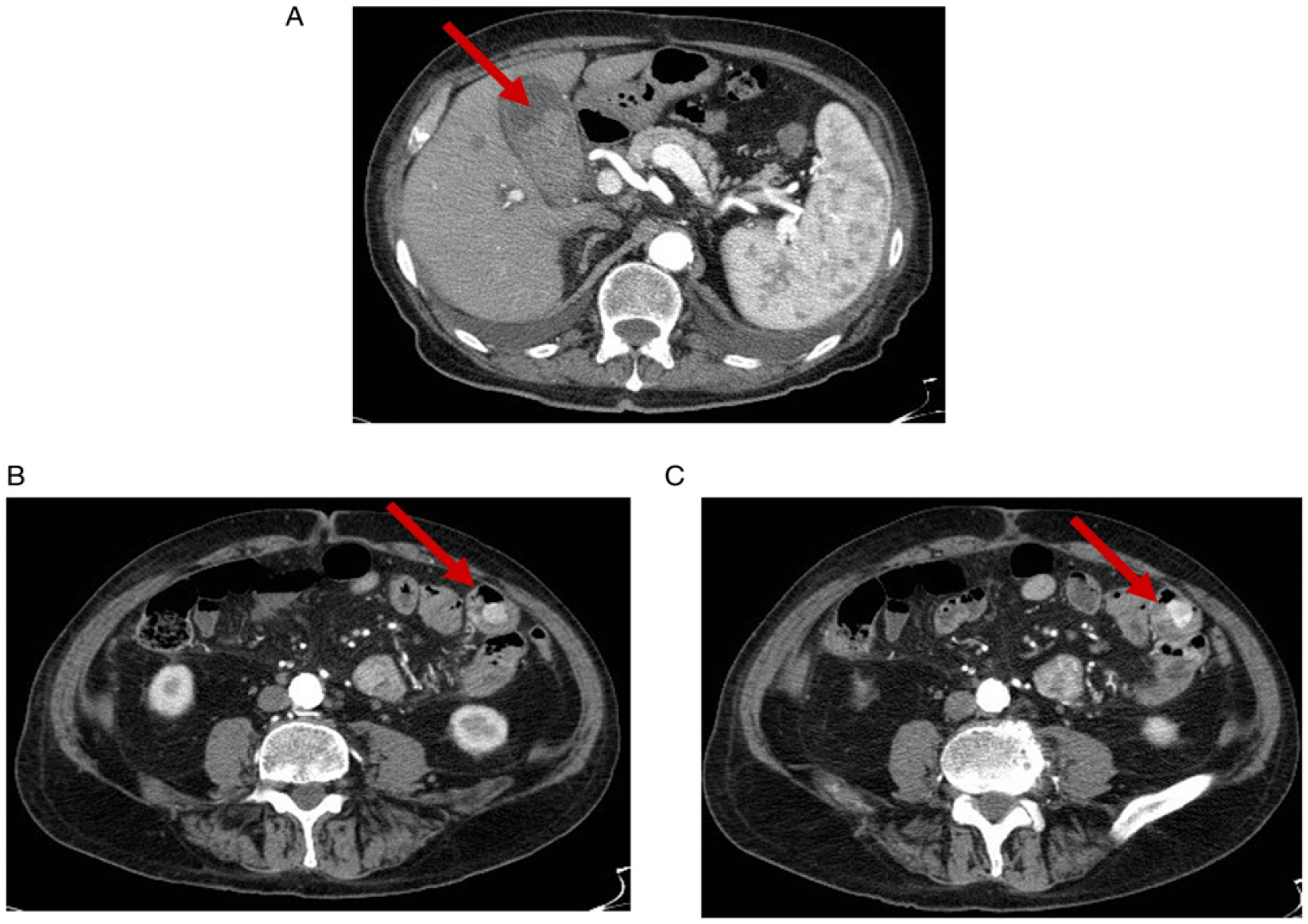
Urinary Obstruction
Urinary obstruction in oncologic patients can occur from primary urothelial and renal cancer, extensive disease of pelvic or retroperitoneal organs or inflammatory or fibrotic involvement of the ureters after chemo- or radiotherapy. 46
Ureteral obstruction may arise from direct infiltration or compression or adhesion, and can be unilateral or bilateral depending on the location of the obstruction.
Usually the obstruction develops slowly, therefore symptoms are nonspecific including abdominal pain localized to the right or left abdomen, with progressive dilation of the ureters, leading to eventual kidney failure. Depending on the nature, duration and location of the obstruction, anuria or hematuria can occur. 47
Imaging evaluation includes assessment of the thickness of the renal cortex (ie, cortical renal thinning is related to a degree of renal failure), the severity of hydronephrosis, the level and cause of ureteral obstruction, and degree of obstruction to consider the best treatment options.
46
In most cases, US is the first imaging modality.
47
Key points in US evaluation include establishing the obstruction level, assessing soft-tissue neoplasm, calculi or sludge and assessing whether the obstruction is partial or complete. US is very good tool at estimating the grade of hydronephrosis, detecting stones or sludge, even if sometimes it may not be able to determine whether stones are in in the middle third of the ureter.
47
It can be challenging to correctly assess soft-tissue mass with gray scale US, so color-Doppler may be helpful.
47,48
CT urogram is the examination of choice, providing valuable information on the type and level of obstruction, its extension, complications and is a valuable technique for a tailored management approach and staging. (Figure 5).
46,47,49
72 year old man presenting with hematuria, discomfort and pelvic pain. (A) CT urography shows right hydronephrosis caused by a soft tissue lesion within the right pelvic ureter with adjacent periureteral fat stranding (B). Coronal and sagittal MPR images give the overall spatial assessment of the full extent of the mass and upstream ureteral dilatation (C, D).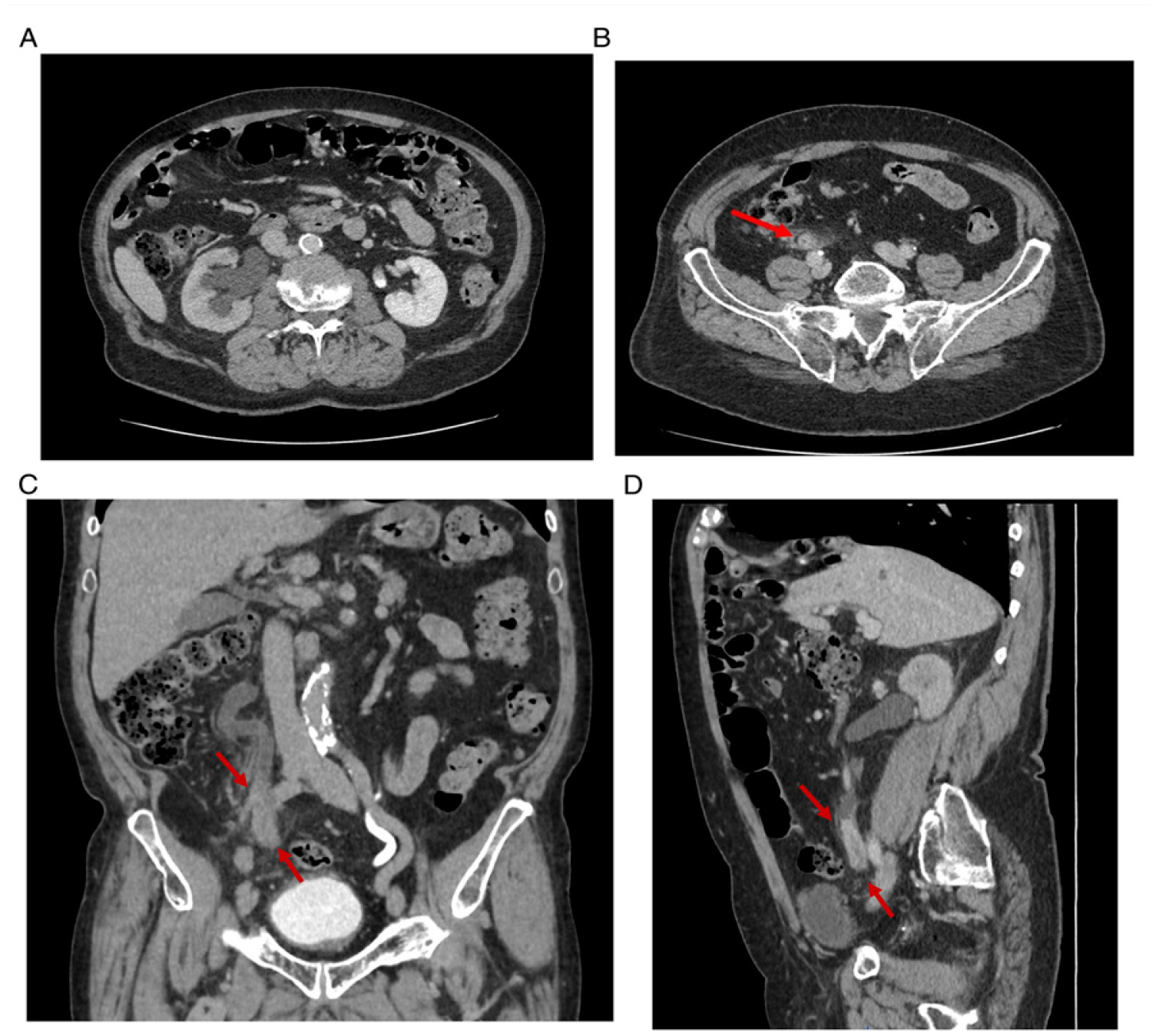
Biliary Obstruction
Patients with malignant biliary obstruction usually have a bad prognosis. Biliary obstruction in oncological patients is often caused by pancreatic adenocarcinoma, cholangiocarcinoma, peri-ampullary neoplasms, or metastatic lymphadenopathyat the porta hepatis. Biliary obstruction may also result from postoperative complication of biliary stent obstruction, migration or due to stenosis of biliary anastomosis. 4
US is usually the first imaging modality in the clinical algorithm in patients with right upper abdominal pain, and the clinical suspicion for biliary obstruction.
Occasionally, the patient presents at ED with a previously unknown malignancy which is causing biliary obstruction and the diagnosis is initially made by a first line US. US can identify the degree of biliary dilation, level of obstruction, and cause of the obstruction.
The dilation of intrahepatic or extrahepatic ducts or the involvement of pancreatic duct can be assessed to determine the level of obstruction and identify treatment options.
CT shows and characterizes the underlying cause and complications, guiding towards the appropriate management. CT should be performed with intravenous contrast to evaluate the full extension of a neoplasm, its surgical resectability and staging (Figure 6). MR is a valuable tool to evaluate the biliary tract, as it helps in identifying the cause of biliary obstruction, but its role in emergency context appears quite limited.
12
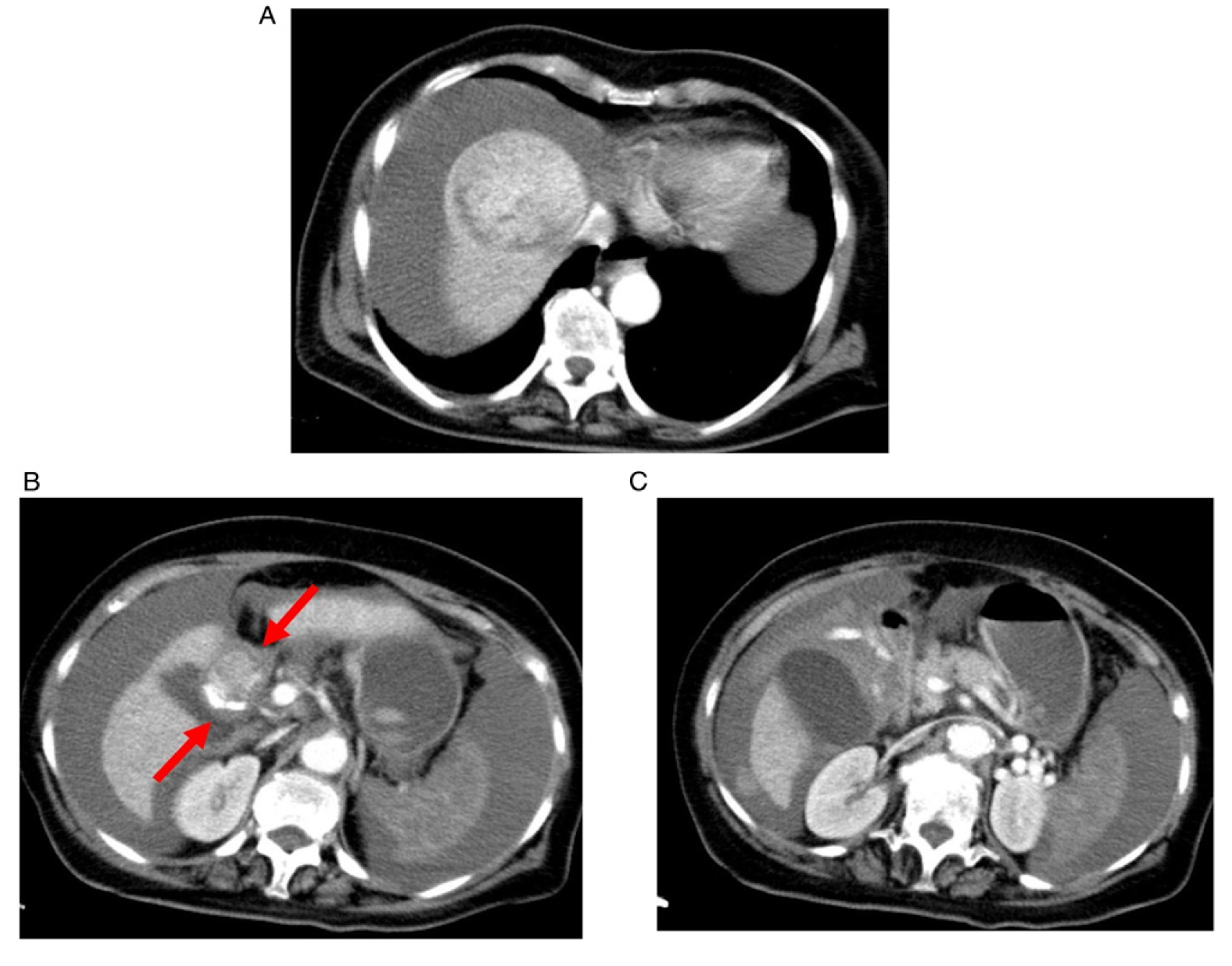
52 year old lady presenting with jaundice and itching (A) Axial contrast-enhanced MDCT and coronal MPR image (B) show intra-/extrahepatic biliary tree and gallbladder dilatation caused by a large pancreatic head necrotic mass in keeping with a pancreatic carcinoma. The lesion was considered surgically unresectable due to direct vessel involvement, therefore a biliary stent was placed. After a 3 days, the patient developed sudden abdominal pain and, therefore, a follow-up CT scan was performed. (C) Axial CT scan demonstrates an appropriate placement of the biliary stent and decompression of the biliary tree, but a pancreatitis at the tail (arrows) with small amount of fluid in the left pararenal space.
If cholangitis is associated with biliary dilation, drainage should be made immediately. Drainage can be done percutaneously or endoscopically. Percutaneous biliary drainage can be performed for any case of biliary obstruction. Endoscopic drainage with stent insertion alleviates obstruction in patients with pancreatic head malignancy 48,50 (Figure 6).
Radiation Enteritis
Radiation enteritis occurs in patients receiving a radio-therapeutic treatment of the abdomen and/or pelvis during the course of their planned cancer treatment. 51 –60 This entity is characterized by diffuse collagen infiltration and microvascular changes that results in a local narrowing of the intestinal lumen. 48,50 –54
There is a bowel dilation proximal to affected segments and progressive mucosal damage resulting in a bowel ulceration, perforation, and massive gastrointestinal bleeding. Pelvic irradiation, where the greatest volume of bowel is affected, is predominantly used in the treatment of gynecologic and urologic cancers. 48 –57 A recent study showed 50% incidence of radiation bowel damage among their cohort of 12,000 patients with pelvic cancer. 57
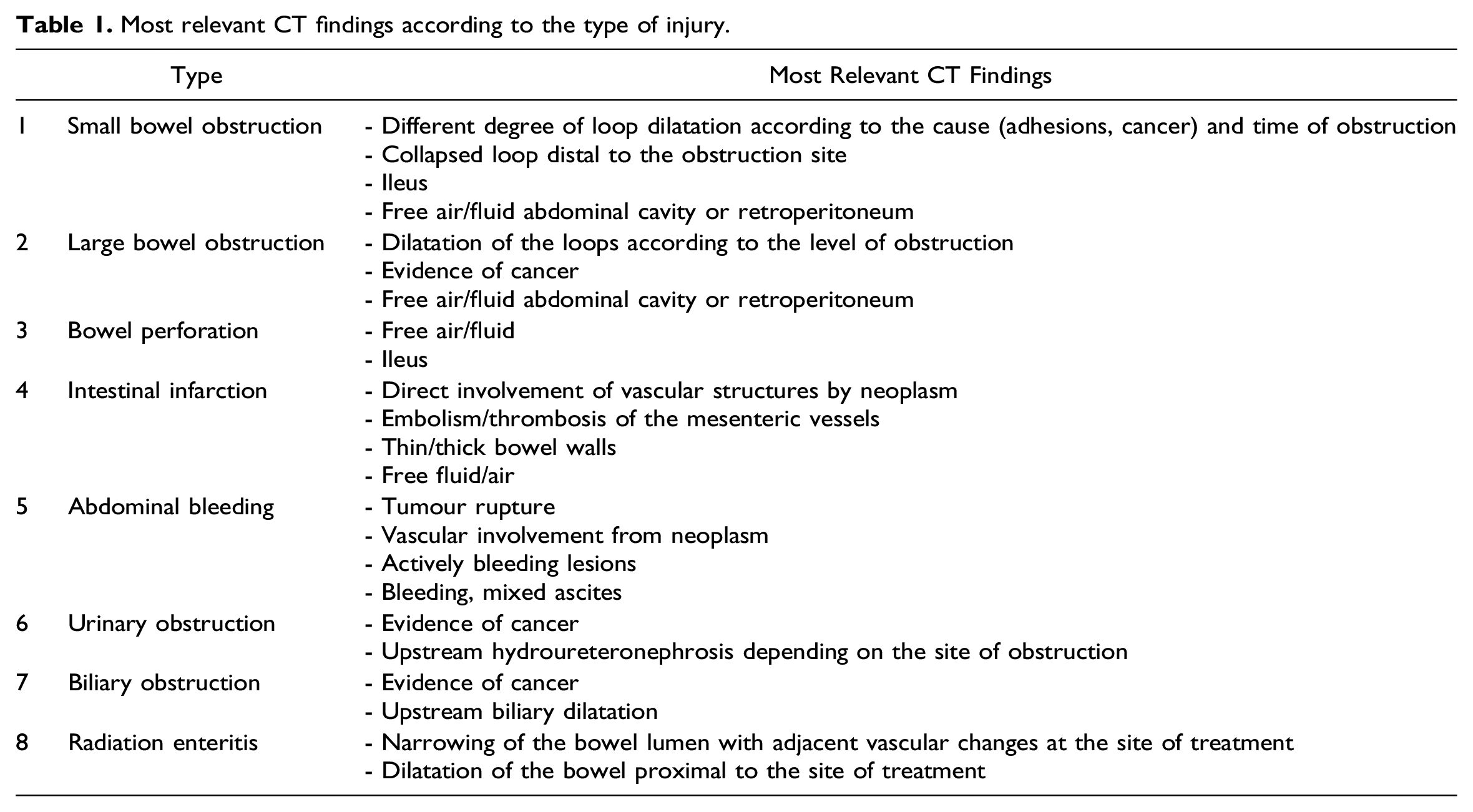
Most relevant CT findings according to the type of injury.
In conclusion, emergency radiologist may encounter numerous abdominal emergencies in cancer patients and should be cognizant of their unique presentations and available management options. 61
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.