
Abstract
Introduction
COVID-19 pandemic precautions required social distancing to minimise potential viral transmission. In many busy CT patient waiting rooms, adequate social distancing could not be achieved without decreasing the number of patients in the waiting room at any given time. This necessitated reduction in patient waiting room times to maintain workflow. The rate-limiting step in some practices is the administration of oral enteric contrast for abdominal CT. Oral contrast administration is a time-consuming process, requiring time for preparation, consumption and adequate gastrointestinal transit, which increases the duration the patient spends in the department. Traditionally, positive oral contrast has been routinely administered to delineate the bowel from other structures and assess its integrity. 1 There is a global variation in its use and practice patterns are heterogeneous.2-4 Many studies show that routine use of oral contrast may not be routinely necessary and that abdominal CT without oral contrast is accurate to demonstrate a variety of pathology in multiple clinical settings,5-13 and many international guidelines support a reduction in oral contrast use.14-16 In addition to prolonged wait times, oral contrast administration may be associated with an unpleasant taste and potential side effects, including a risk of aspiration especially in critically ill patients. 13 Oral contrast may increase radiation dose due to automatic exposure control feedback mechanisms, with reported increases of 11% in the CT dose index volume with positive oral contrast, which is a considerable increase, especially in young patients requiring repeated surveillance imaging. 17 Omission of oral contrast may reduce artefacts associated with beam-hardening from the dense intraluminal contrast and can also improve the sensitivity in the diagnosis of some entities including, mesenteric ischaemia, enteric mucosal disease, and gastrointestinal haemorrhage.1,18,19 However, presence of oral contrast remains crucial for some indications such as anastomotic leak and peritoneal carcinomatosis.2,20 Different types of positive oral contrast are available, with differing characteristics including transit time, homogeneity and attenuation. 21 Barium-based oral contrast agents are known to have a slower intestinal transit compared to water-soluble iodine-based agents. 22 Further, palatability of different agents also impact the duration of time needed to complete drinking the oral contrast solution/suspension. 23 As part of our Radiology department pandemic response initiative, we aimed to reduce the CT waiting room bottleneck created by oral contrast administration to prevent unnecessary overcrowding. To achieve this, a multidisciplinary stakeholder collaboration was utilised to adjust the oral contrast service by: (1) creating a new protocol guideline to limit the use of oral contrast when oral contrast was not necessary, and (2) introducing a new oral contrast regime to shorten the duration of oral contrast administration when oral contrast was felt to be necessary at our institution. In this study, we aim to assess the impact of this initiative.
Methods
We received approval from our institutional research and ethics board and the requirement for informed patient consent was waived.
In our academic centre with three hospitals, leveraging a multidisciplinary stakeholder collaboration, including technicians, managers and administrative staff, we updated the abdominopelvic CT oral contrast service by implementing two interventions which were then evaluated restrospectively for efficacy as part of our quality initiative:
Intervention 1: Judicious Use of Oral Contrast
We created a working group of radiologists to review current literature on optimal use of oral contrast. The working group developed a new ‘oral contrast policy’ document. The new oral contrast policy emphasised judicious use of oral contrast, limited to anastomotic leak, enteric fistula and suspected or confirmed peritoneal carcinomatosis. Prior to our intervention, there were a number of CT protocols already which did not require oral contrast, including various hepatobiliary protocols, renal colic studies, and CT urography. Additional protocols and indications were chosen to stop using routine oral contrast use. After discussion at our monthly divisional meeting, and follow-up for any questions, this quality initiative received support of the abdominal imaging division, which included 34 abdominal subspecialized radiologists. The institutional standardised CT protocols were modified to reflect this change in oral contrast use. The technologist and patient-flow teams were involved as stakeholders, to optimise workflow. The oral contrast policy was disseminated to radiologists, radiology learners, technologists, administrators and our radiology booking team via internal communications to the in order to ensure smooth implementation into practice.
Intervention 2: Creation of a New Shorter Oral Contrast Regime
The previously used barium-based oral contrast (E-Z-CAT 4.9% w/v oral suspension) was replaced with a water-soluble iodine-based oral contrast (Telebrix®–Meglumine ioxitalamate). Anticipating faster intestinal transit with Telebrix, we reduced the consumption to scan time, from 60 minutes previously to 30 minutes. The standardised patient check-in instructions (automated voice messaging, booking office patient call-in scripts, mail and email scripts, Website information, patient online portal information, information booklets) were updated accordingly. The patients receiving oral contrast were informed of the change and if they still required oral contrast, they were advised the appropriate time to attend for their scan based on the new shorter oral contrast regime timings.
We implemented these interventions into the CT service pathway and the final process map is shown in Figure 1. Process map for CT service pathway.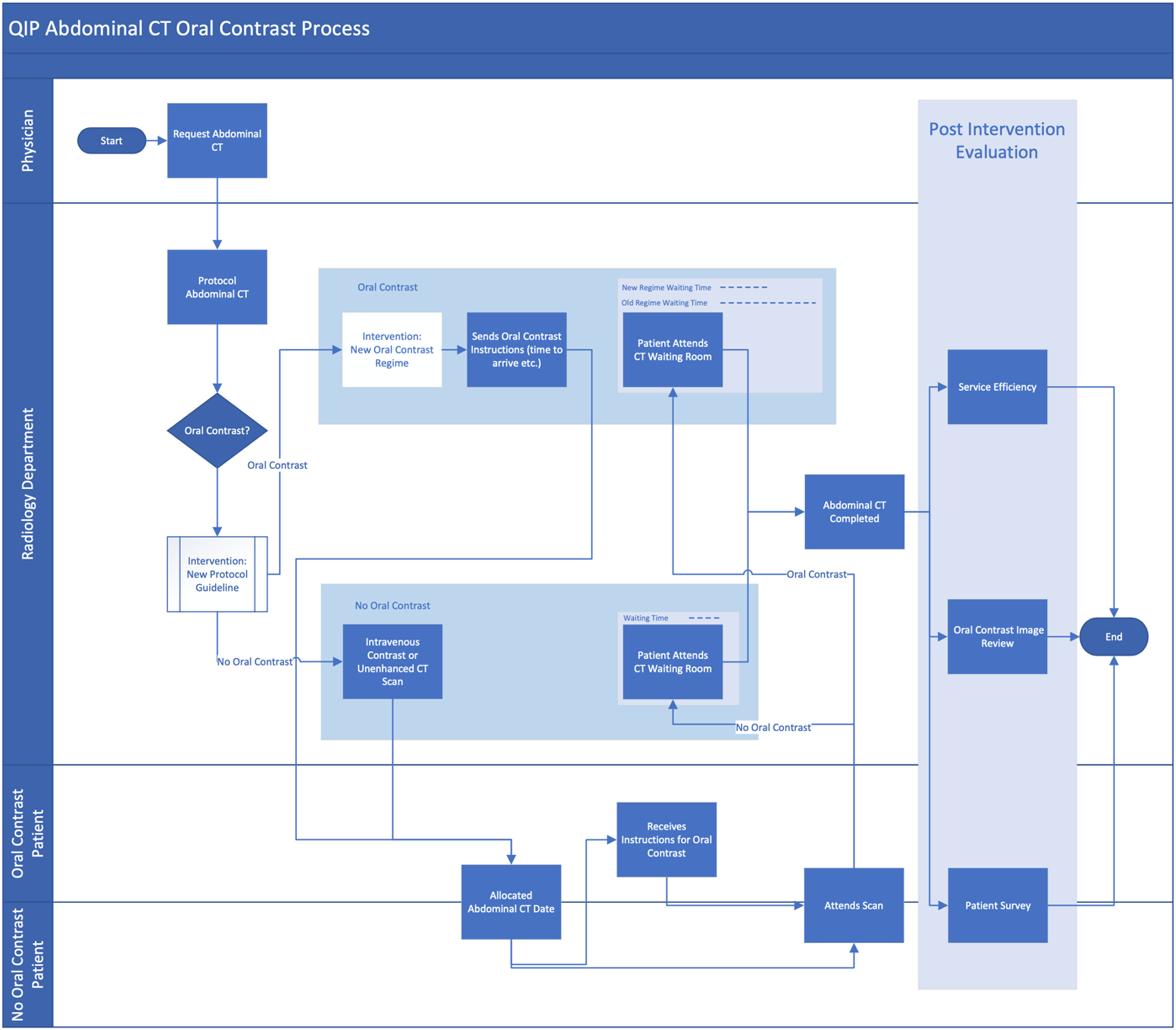
We measured the differences in oral contrast use before and after the intervention, as part of a Plan, Do, Study, Act. (PDSA) quality initiative, with a second review of level of sustained reduction in oral contrast administration for abdominal CT scans, 9 months after implementing these changes.
Analysis
We conducted a retrospective service evaluation of our outpatient (OP) abdominopelvic CT service at three time points: baseline-pre-pandemic (pp), baseline-pandemic (p) and post-intervention. This review was conducted at three hospitals within a single institution. We included two baseline groups (prior to (pp) and during the pandemic (p)) to account for any pandemic-related variables in patient processing times. Each group was over a 1-month period: baseline (pp) November 2019, baseline (p) September 2020 and post-intervention November 2020 and included all abdominal and abdominopelvic CT scans in each of these 1-month period. The following data and outcome measures were recorded:
Oral contrast use (Intervention 1)
We collected patient demographics, CT scan details including if oral contrast was administered and, where applicable the type of oral contrast. Oral contrast use was calculated as the percentage of abdominal CT scans performed with oral contrast. As part of a plan-do-study-act (PDSA) framework approach, we collected data on the use on oral contrast 9 months following intervention to assess whether the impact was sustained or reverted back to the mean.
Time efficiency (Intervention 1 and 2)
Patient waiting room time was defined as the time between patient check-in to CT scan start time. We assessed if the waiting room time was different between the baseline and post-intervention groups and the time saved (in min).
Cost-savings (Intervention 1 and 2)
A per-patient oral contrast cost-savings was determined based on the unit price of previously used and newly implemented oral contrast medium, in Canadian dollars.
Patient experience (Intervention 1 and 2)
Patient experience was evaluated with a voluntary paper-based patient questionnaire survey during the post-intervention period in the outpatient department (Figure 2). Voluntary patient survey questionnaire.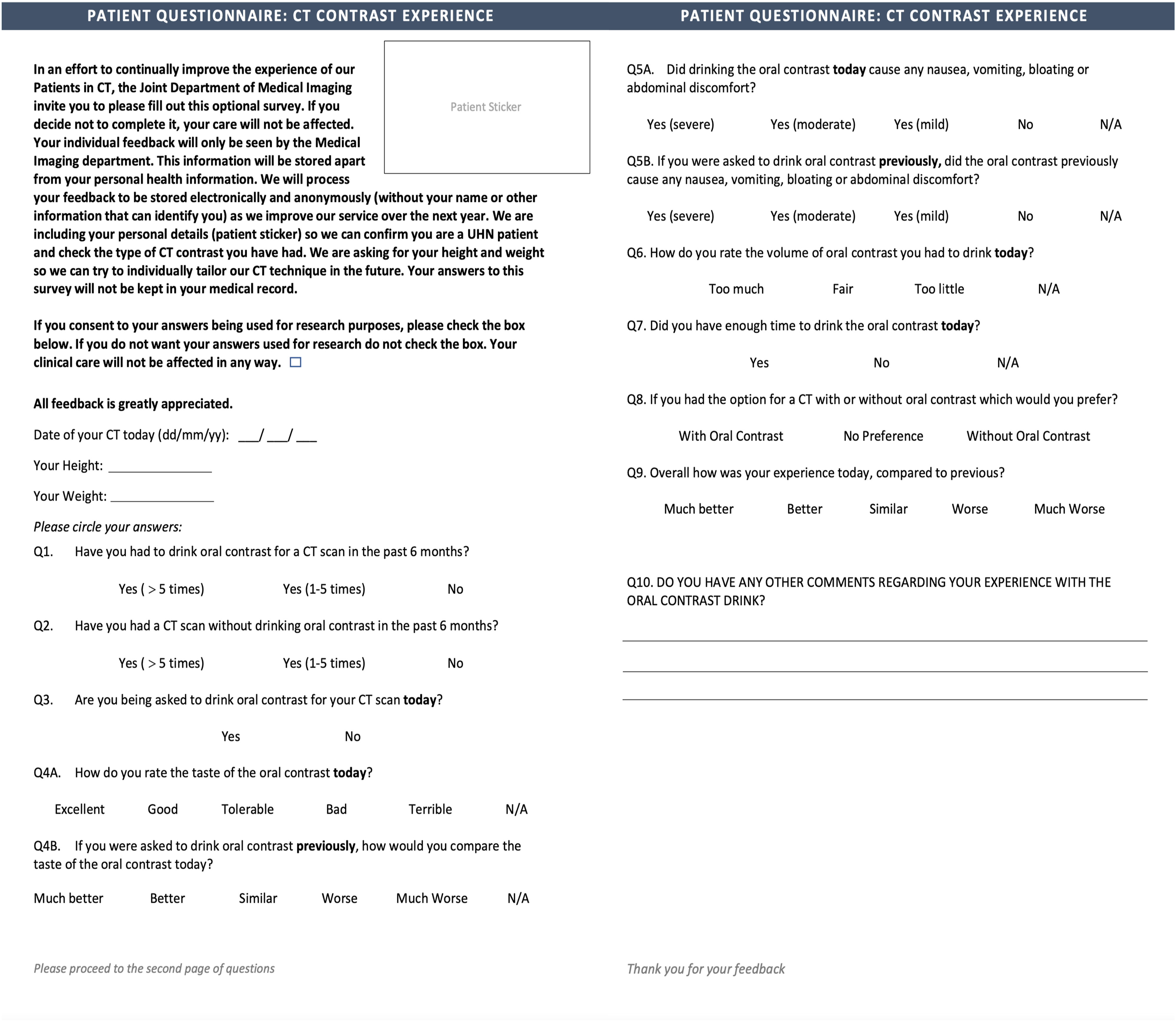
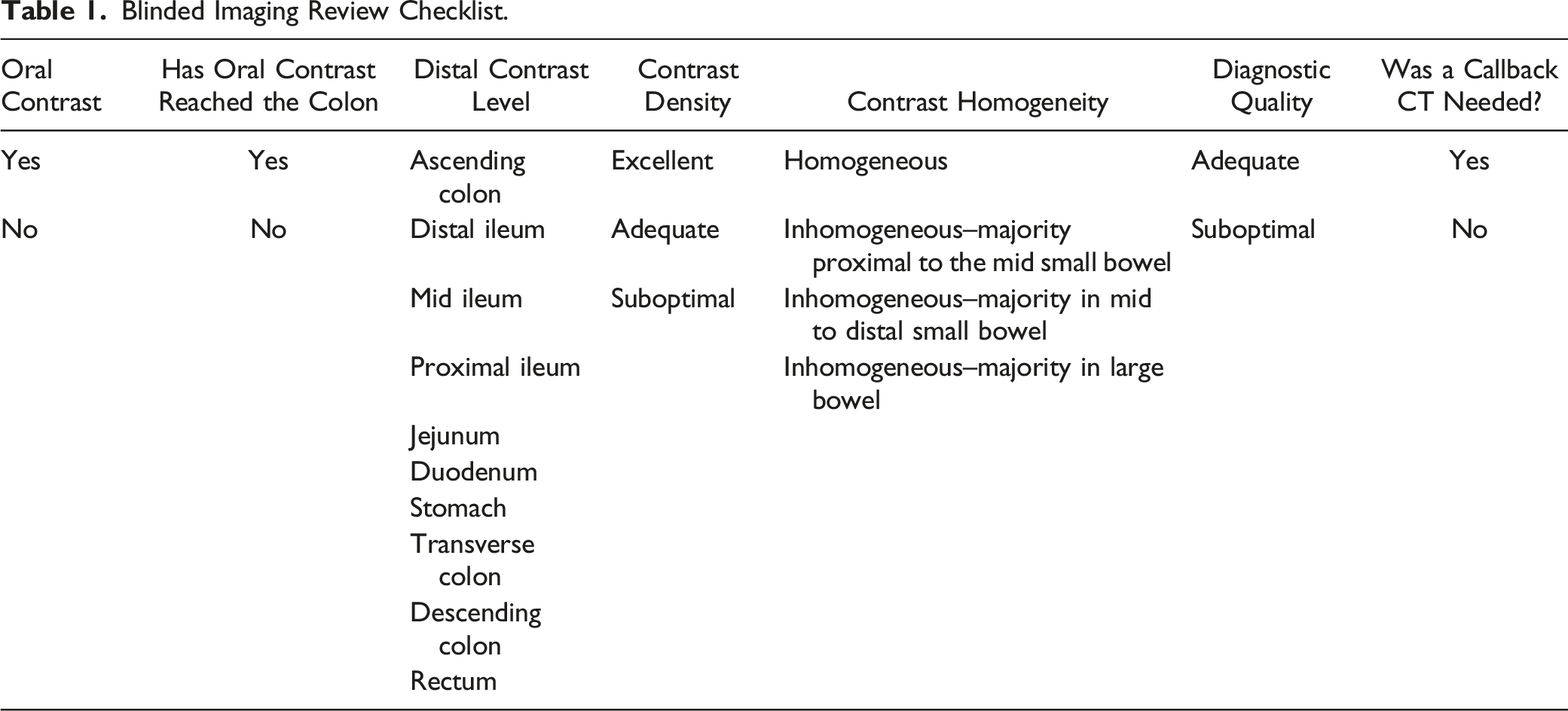
Blinded-image evaluation (Intervention 2)
Blinded Imaging Review Checklist.
Cohen’s Κappa values with 95% CI were calculated as estimates of interrater reliability. 24 The following standardised strength of agreement categories were used for the Κ values of <.00 indicate poor, .00–20 slight, .21–40 fair, .41–60 moderate, .61–80 substantial and >.81 almost perfect agreement. 25 SAS version 9.2 or R version 3.5.3 is used for all analyses.
Statistical analysis was performed to compare the baseline and evaluation outcomes. Data on categorical variables were reported as frequencies and percentages. Continuous variables were described as means ± standard deviations. Summary statistics are reported according to the assessment periods. Statistical significance was reported using Chi-square or Fisher Exact test for categorical variables and Student’s t-test or ANOVA for continuous data. Statistical significance is considered as p < .05.
Results
The study cohort of patients undergoing an OP abdominal or abdominopelvic CT was n = 1615, comprising baseline (pp) n = 575, baseline (p) n = 495 and post-intervention n = 545 groups. The mean age was 59.4 years (P = .78, sd ± 16.1, range 19.6–96.5 years), with 42.7% female and 57.3% male (P = .23), with no significant differences in age or gender between the baseline and post-intervention groups.
Oral Contrast Use (Intervention 1)
The fraction of abdominal CT scans performed using oral contrast is as follows: baseline (pp) 420/575, 73.0%, baseline (p) 309/495, 62.4% and post-intervention 178/545, 32.7%. This amounts to a 48–55% decrease in patients receiving oral contrast for abdominal CT. There was a significant reduction in the number and percentage of oral contrast scans performed in the post-intervention group, compared to the baseline groups (P < .001). This reduction was sustained at the 9 months follow up, with 430/1213, 35.4% patients having oral contrast which was not statistically different compared to post-intervention group (P < .001).
Time Efficiency (Intervention 1 and 2)
The post-intervention mean patient waiting room time was significantly lower than both the baseline groups, with a mean reduction of 15.3 minutes and 15.8 minutes, compared to the baseline (pp) and baseline (p) groups respectively (P < .001). Original turn-around time was 70.0 minutes and after the intervention, the turn-around time was 54.7 minutes, with a sustained turn-around time of 54.2 minutes.
Cost Differences (Intervention 1 and 2)
The new shorter oral contrast regime had a lower unit price (per patient) of $2.99 from $6.00 in the barium-based oral contrast in the baseline groups. The expenditure for oral contrast in each group was: baseline (pp) $2478, baseline (p) $1730.40 and post-intervention $534. There was oral contrast cost reductions of 69.1–78.4% (P < .001). We did not account for possible differences in patient indications and variation over time, thus a full cost analysis was not performed.
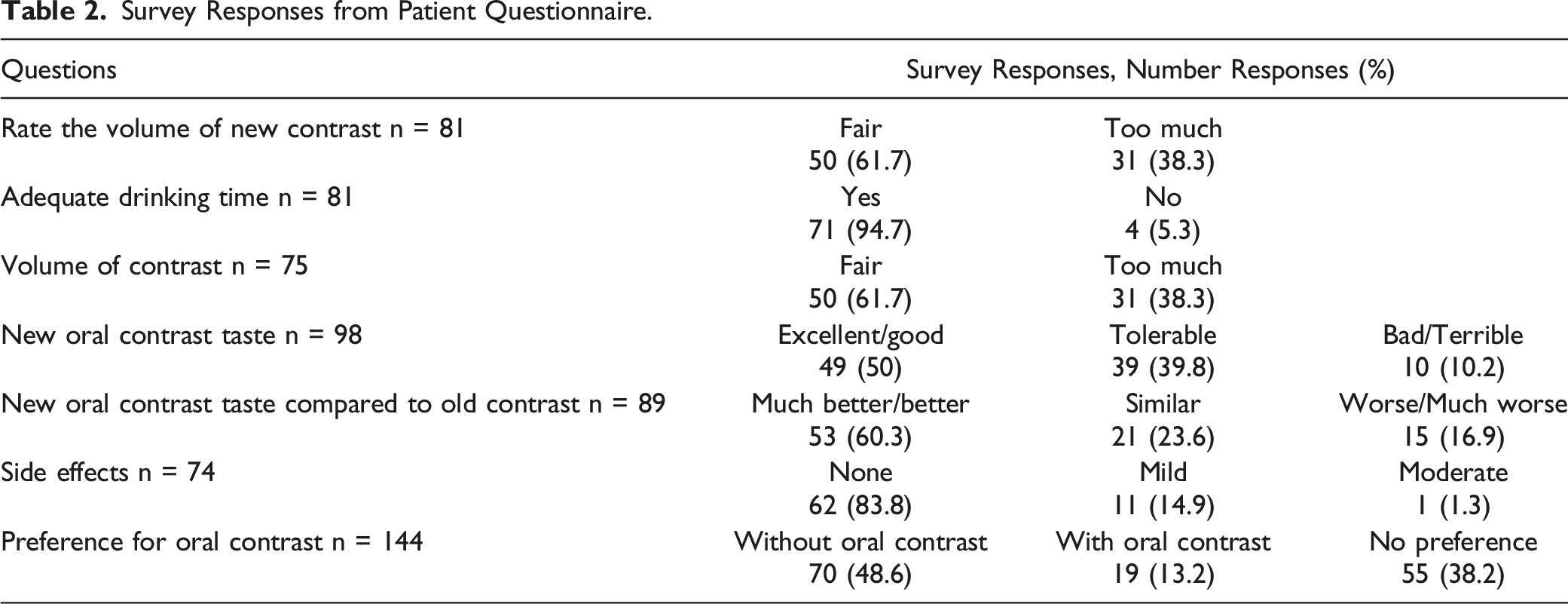
Patient Experience (Intervention 1 and 2)
Survey Responses from Patient Questionnaire.
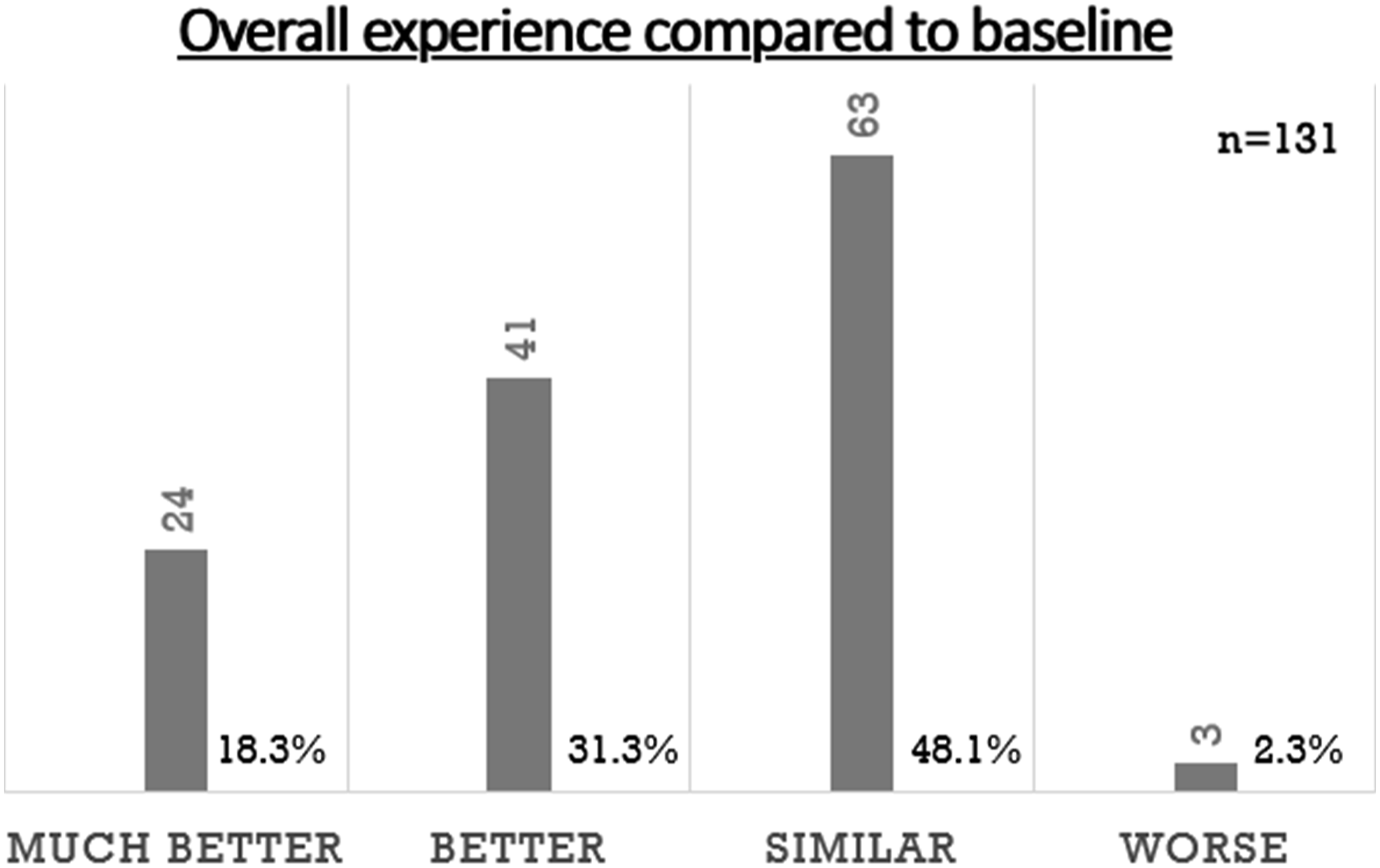
Patient survey responses regarding overall experience compared to baseline.
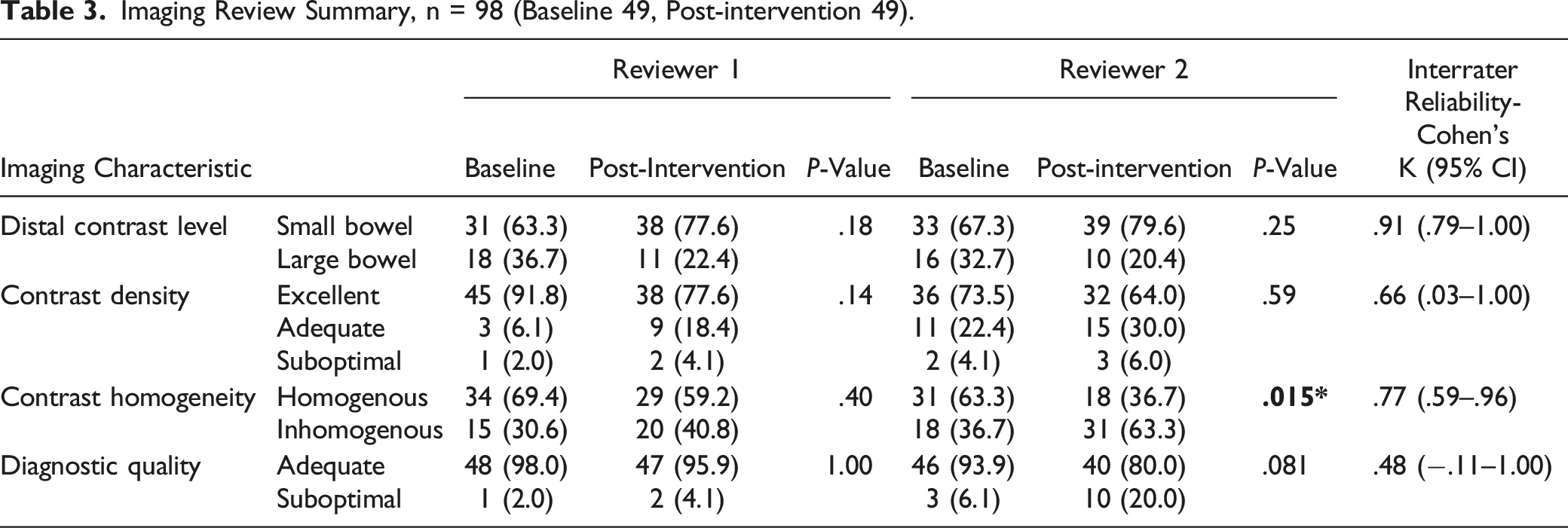
Blinded-Image Evaluation (Intervention 2)
Imaging Review Summary, n = 98 (Baseline 49, Post-intervention 49).
Discussion
The main focus of our COVID-19 pandemic response initiative was to reduce overcrowding in our outpatient CT service. We achieved this by judicious use of oral contrast combining it with using a shorter oral contrast regime, when oral contrast was still felt to be required. In addition to reduced patient wait times, we have demonstrated per-patient cost-savings and improved patient experience, whilst preserving diagnostic image quality. Our PDSA framework review confirmed sustained implementation of this service change.
After implementation of new oral contrast policy, oral contrast use decreased from 62.4 to 73.0% in the baseline groups to 32.7% in postintervention group. This reduction in oral contrast use is supported by national and international guideline recommendations and is in line with a large body of literature supporting the trend in its reduction with advances in CT technology. 26 Our planned reduction in oral contrast use also conserved contrast during the time of global contrast shortage crisis, which has since recovered. 27 Patient wait-time was shortened by 15.3–15.8 minutes in our study. Previous literature shows discontinuing routine oral contrast improves CT workflow with a significant decrease in time to CT completion, ranging from reductions of 23 minutes to 66 minutes.5,7,28-31 Our less dramatic wait-time reduction may be in part due to patients arriving early to accommodate potential delays related to additional pandemic precautions in the hospital. Whilst studies have shown reducing use of oral contrast improves service efficiency in an Emergency Department setting, our study establishes the optimal role of oral contrast in an outpatient setting.9,26,32
In our study, the reduction of oral contrast used led to a per-patient cost-savings, although a full economic evaluation was not performed. Overall cost-reductions were calculated in a study by Shankar et al, 33 where authors reported a 52% CT oral contrast annual cost reduction following a policy change limiting the use of CT oral contrast in patients with non-traumatic abdominal pain to patients those with recent surgery, inflammatory bowel disease or BMI <25 kg/m2. The oral contrast cost-savings in our study included both reduction in net percentage of patients receiving oral contrast, as well as switching from a more expensive barium-based oral contrast agent to an iodine-based oral contrast agent with half the unit cost per patient, in cases where oral contrast was still felt necessary to be administered.
Patient experience is a critical component of quality improvement and healthcare delivery. Oral contrast agents occasionally cause diarrhoea, bloating and cramps and prevalence and degree may vary with the oral contrast agent used. Patient experience was overall positive in response to our interventions. Patients preferred CT studies without oral contrast. If oral contrast needed to be administered, they preferred the iodine-based oral contrast which was reported to have improved palatability compared to barium. This is in line with prior studies which show similar findings of improved palatability of Telebrix compared with barium suspension. 34 Woolen et al 35 showed in an n = 218 patient survey study, that if oral contrast material has any diagnostic benefit, most outpatients (89%) would rather drink it than accept any risk for missing an important finding. 35 Further studies are needed to assess patient preference balanced with risk estimates of missed diagnosis.
Diagnostic quality imaging is of utmost importance and decisions to administer oral contrast should not compromise diagnostic integrity for the sake of time or cost-savings. Different oral contrast agents may have different performances on density and homogeneity of opacification in addition to differences in speed of transit. Our results show preserved diagnostic image quality in our new shorter oral contrast regime compared to the old regime, which is supported by other studies, including Wadhwani et al demonstrating that one- and three-hour oral contrast regimes have similar diagnostic performance. 36 This is likely due to faster intestinal transit of iodine-based oral contrast as compared to barium suspension as has been reported previously. 22 A large body of literature establishes that diagnostic quality is preserved despite the omission of oral contrast.9,10 In a study on a cohort of oncological patients, Buttigeig et al showed that CT diagnostic quality was preserved with and without oral contrast administration 12 and Uyeda et al (n = 1992) showed similar results in an ED setting. 11 Conversely Wadhwani et al reported improved reader confidence in visualising the appendix after administration of oral contrast. 36 Oral contrast may not have reached the point of interest at the time of image acquisition, as reported in 30% (n = 1561) by Laituri et al 8 and 31.1% (n = 61) by Kessner et al 10 We report that in up to 73.5% of our oral contrast studies the contrast does not reach the large bowel. The homogeneity of contrast in various parts of the small bowel may also be variable depending on how the patient ingests the oral contrast (frequent, small sips vs less frequent, larger quantities) and function of the pyloric valve as well as general peristalsis throughout the small bowel. This highlights the need for optimizing oral contrast use in specific scenarios. However, contrast density was excellent and both readers rated diagnostic adequacy as quite high, and no patient was called back for a repeat examination for diagnostic inadequacy. We did not explore if there is any impact on diagnostic accuracy and this could be an area of future research.
We were limited by our retrospective study design which could introduce bias. To avoid it, we had 2 separate baseline groups to eliminate any bias introduced by the pandemic as there were many sudden changes in imaging volumes which were externally driven due to pandemic responses at governmental levels. We specifically chose two time points where patient imaging volumes were less volatile. It has been previously reported that patients with lower BMI may benefit from oral contrast administration, but we did not evaluate the effect of BMI and image quality.19,37 Nevertheless, there was no difference between the 2 groups. Although diagnostic image quality was not affected, we did not specifically look for diagnostic accuracy, which needs to be explored in future. There was some reluctancy to fill in the paper survey due to the on-going pandemic precautions at the time limiting paper interactions and this could introduce bias whereby only patient with excellent experiences, or terrible experiences, would volunteer to fill out the survey. However, given the situation in our hospital system, with many cases of COVID-19 were treated, we did not have an alternate solution to encourage patient participation. The survey was only available in English and as a standard visibility form, limiting accessibility. However, our reasonable number of responses were considered representative given the nature of the questionnaire survey. There is also potential memory recall bias in patients who had previously had the barium-based oral contrast and switched to the iodine-based oral contrast however, due to the need to act quickly, we could not implement a survey for patients prior to making the changes in oral contrast use. We did look at savings on a per-patient oral contrast use (or lack therefore) but did not perform a full cost analysis for the purpose of this study. We also did not perform individual audits of each protocoling radiologist in order to determine the level of per-radiologist adherence to our consensus driven plan to reduce oral contrast use in specific indications. Finally, some of our results may not be applicable in other centres where patients may consume the oral contrast before arriving for their scan, either at home or in a remote location. Despite these limitations, this quality improvement project demonstrates that despite the many challenges posed by the COVID-19 pandemic, it has also created an impetus for initiatives to improve services, streamline workflow and have a positive impact on patient experience.
Conclusion
We have shown how collaborative radiology pandemic response initiatives: limitation of oral contrast use and switch to a cheaper iodine-based oral contrast medium with quicker intestinal transit and improved palatability, can improve outpatient services. These initiatives not only helped achieve improved social distancing in the pandemic, but also led to decreased patient wait, reduced overall costs and improved patient experience.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.