
Abstract
The Canadian Association of Radiologists (CAR) Incidental Findings Working Group consists of both academic subspeciality and general radiologists tasked with either adapting American College of Radiology (ACR) guidelines to meet the needs of Canadian radiologists or authoring new guidelines where appropriate. In this case, entirely new guidelines to deal with incidental musculoskeletal findings that may be encountered on thoracoabdominal computed tomography or magnetic resonance imaging were drafted, focussing on which findings should prompt recommendations for further workup. These recommendations discuss how to deal with incidental marrow changes, focal bone lesions, abnormalities of the pubic symphysis and sacroiliac joints, fatty soft tissue masses, manifestations of renal osteodystrophy and finally discuss opportunistic osteoporosis evaluation.
Introduction
The Canadian Association of Radiologists (CAR) Incidental Findings Working Group consists of both academic subspeciality and general radiologists tasked with either adapting American College of Radiology (ACR) guidelines to meet the needs of Canadian radiologists or authoring new guidelines where appropriate. Guidelines on incidental renal, 1 hepatobiliary 2 and pancreatic findings 3 have become a popular resource for both academic and community radiologists. The working group conducted a literature search and assessed the current regional practice patterns and felt that there was a general lack of recommendations concerning incidental musculoskeletal (MSK) findings seen on CT and MRI.
Two subspecialized MSK radiologists (GD and GB) were recruited to the working group to help develop these guidelines. The group initially met and created a list of relevant or frequently encountered MSK incidental findings in adults. Following a comprehensive evaluation of the available literature, all incidental findings and management recommendations were discussed as a group for consensus.
While the information and tables presented below are based on the best available scientific evidence, significant gaps in the literature remain. Ultimately these management recommendations reflect consensus recommendations rather than a fully evidence-based standard of care. An imaging atlas of selected commonly encountered incidental MSK findings has also been produced as an Supplementary Appendix to this article for quick reference.
Incidental Marrow Changes on MRI
A full review of the appearance of normal marrow and age-related marrow changes is beyond the scope of this paper, but these guidelines aim to address the most commonly encountered incidental findings and how to efficiently triage bone marrow lesions.4-13
Marrow Signal Heterogeneity
An understanding of the composition and signal characteristics of normal marrow is essential if one is to identify pathologic changes. Bone marrow sits within the medullary cavity around a network of trabecular bone (mineralized matrix). Marrow is divided into two forms: a) active haematopoietic marrow (red marrow) consisting of erythrocytes or precursors and protein and b) inactive fatty or yellow marrow. It is the distribution of these two forms that results in the marrow signal heterogeneity that can be seen on MRI. Red marrow still contains fat but is mainly haematopoietic cells (60%) which consist of water and protein (40% water, 20% protein) intermixed with fat cells (40%), while yellow marrow is composed mainly of fat (95%) and the rest nonfat (5%), which on a cellular level is still approximately 80% fat, 15% water and 5% protein.4-11
The distribution of red and yellow marrow changes with age6-9,12,13 and in the adult, red marrow is centred within the axial skeleton (spine, pelvis and the proximal aspect of the long bones) while yellow marrow occupies the appendicular skeleton (long bones, extremities), mainly the diaphysis and epiphysis.4,6,7,12,13 With age the proportion of marrow fat cells increases in a diffuse and homogenous pattern beginning in the diaphysis & epiphysis of long bones and extending to the metaphysis and then to the axial skeleton. This is the reason for marrow heterogeneity commonly recognized in the spine and pelvis of abdominal/pelvic MRI studies.
The major determinant of the appearance of marrow is the fat and water content, and to a much lesser extent the mineralized matrix or trabecular bone.
Fat (yellow marrow) appears hyperintense on T1-weighted images (T1WI) and the contrast between fat and water (red marrow) on T1 is the greatest. Spin-echo (SE) T1WI are thus the most accurate in evaluating the cellular content and for characterizing marrow lesions. In abdominal MRI studies, conventional SE T1W or turbo/fast spin-echo (TSE/FSE) T1WI are often replaced with spoiled gradient echo sequences (SPGR) for speed.
Red marrow is the cause for marrow signal heterogeneity on MRI. Recognizing normal red marrow and distinguishing it from pathology requires the understanding that fat is present in normal red marrow and to use this to characterize the marrow with fat-sensitive sequences.
Within the same patient red marrow heterogeneity should be consistent, however, the pattern of heterogeneity can be widely variable between patients within the same age range.4,10 Four patterns of physiologic marrow have been described in the spine but the key to determining that red marrow heterogeneity is normal (not replaced with abnormal cellular foci) is to recognize that there are islands of fat intermixed with the non-fat cellular component of red marrow following one of the patterns described in the literature. 5
In abdominal MRI studies, this marrow signal heterogeneity is commonly recognized on fluid sensitive or T2-weighted images (T2WI) which can be problematic but often these studies include at least one fat-sensitive technique – usually fat-suppression (FS) pulse or chemical shift (CS) SPGR sequences. If a lesion shows complete fat suppression it contains mature fat and is benign. If on CS imaging the signal of the heterogeneous marrow drops on out-of-phase images (similar to lipid rich adenomas), the voxels contain microscopic or intracytoplasmic fat and can be dismissed as red marrow heterogeneity. It is recognized and accepted that a drop in signal intensity (SI) of 20% is considered 95% sensitive and specific for microscopic fat.14-16
Normal red marrow will show intermediate SI on both SE/TSE T1WI and SE/TSE T2WI and the marrow signal should be higher than the adjacent normal muscle. On T2WI with FS, the marrow signal is typically intermediate to moderately increase in signal compared to the adjacent muscle, making it more difficult to characterize. Therefore, always fall back to what the marrow looks like on the T1WI to determine if you should be concerned.
A radiologist should be concerned when there is marked hypointensity of marrow on T1, homogeneous low SI on T1 with sharp margins, or when there is trabecular destruction or high signal on T2WI replacing the trabeculae. If there is no change in signal with FS, this tells us that the lesion does not contain mature/macroscopic fat but it does not indicate if a malignant process is present as proteinaceous fluid, haemorrhage or some blood products may not drop in signal intensity but are still benign (classic example being a spinal haemangioma). Similarly, CS imaging will not necessarily tell you that a process is pathologic but the confirmation of intracellular fat implies a benign process that does not require further workup. Though early studies 16 suggested that if marrow did not drop in signal it was malignant, it has been shown that up to 25% of lesions that do not drop in signal on CS imaging can still be benign. Therefore, it is better to refer to these lesions as indeterminate rather than malignant. 14
Marrow Patterns
In the spine, four main vertebral body marrow patterns have been described on T1W sequences.5,12 See Figure 1. In abdominal imaging, fat-sensitive sequences are often limited, and the imaging planes may make pattern recognition more difficult. Marrow patterns.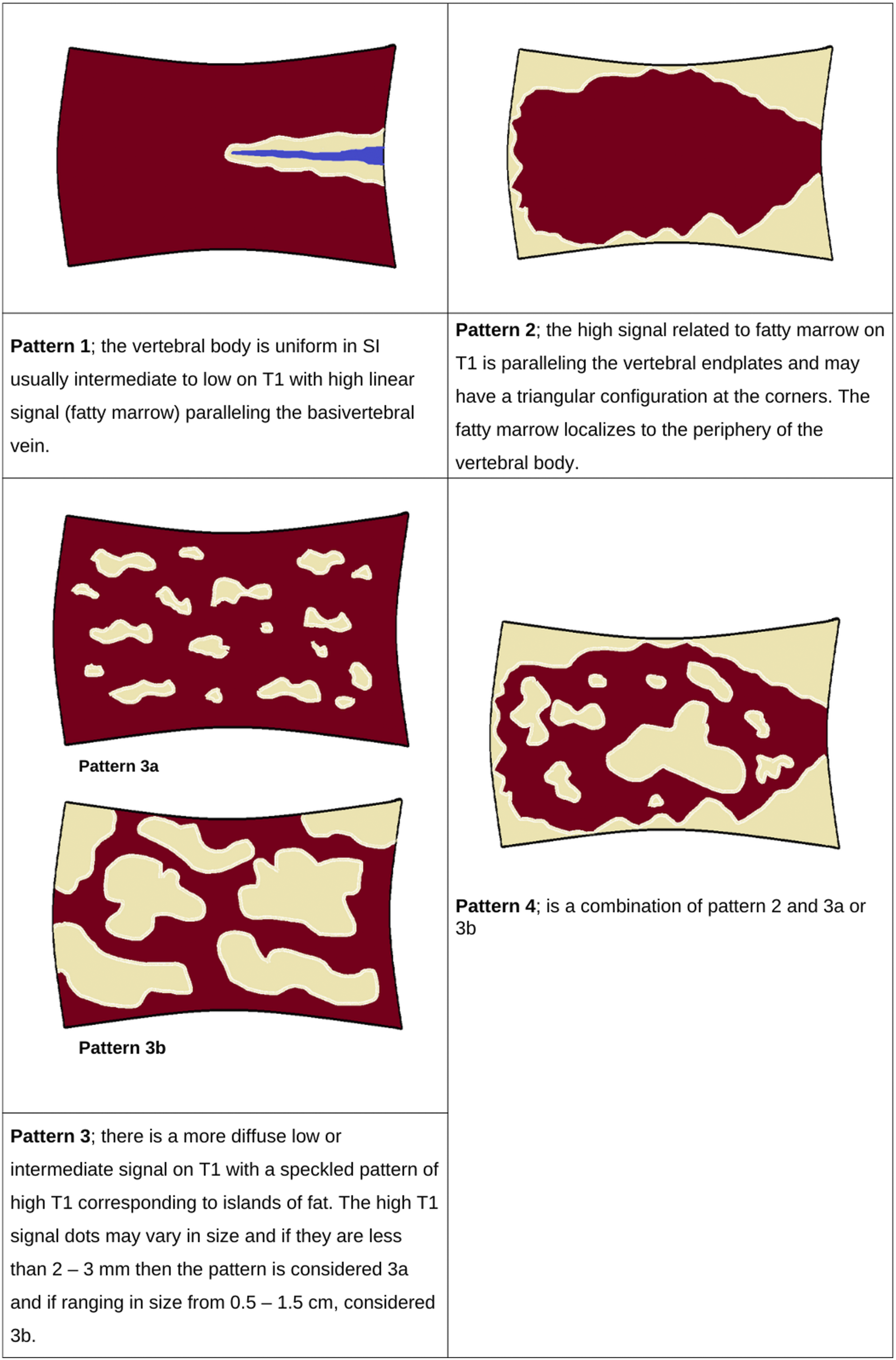
In the pelvis, the red marrow heterogeneity was originally described as two patterns – pattern 1) the areas of fatty marrow (hyperintense on T1WI) are localized to the acetabular roof and medial hip/acetabulum and pattern 2) the areas of fatty marrow start to increase in the ilium bilaterally and around the sacroiliac joints (SIJ) in a relatively symmetric fashion. 5 However, these two patterns are variable with widespread intermixing of fatty and red marrow with indistinct margins and this can present as wide confluent zones or islands of residual red marrow throughout the pelvis with red marrow typically absent around the hips and the symphysis, especially true in the male patient, while in adult females areas of red marrow may be seen in the subcortical area of the femoral/humeral heads and apophysis. It is atypical in the adult to see residual red marrow in the region of the hips and symphysis.13,17
When to Worry
The key parameters in determining if something is concerning includes SI, morphology and location of the red marrow or marrow heterogeneity.7,13
Focal lesions are easier to address. Focal marrow-replacing lesions may be the result of neoplasm, infection or trauma/ischemia and though their presence will not necessarily be specific for pathology, it should be a cause for concern. 12 Focal lesions are especially concerning when located in regions that should normally be replaced with fat. If a focal lesion is seen in the acetabulum or the symphysis, typically replaced with fat in the adult patient, it should be considered worrisome or indeterminate. Similarly, focal lesions seen around the basivertebral vein or along the endplates of the vertebral bodies (especially at the periphery) should also be a cause for concern. These focal lesions are usually similar or lower in SI than the muscle or intervertebral disc on T1WI, higher in SI on T2WI and typically sharply outlined unless surrounded by reactive oedema that may be more ill-defined (the classic T2 ‘halo sign’ that may indicate a metastasis). 18
A focal marrow lesion on T1WI that shows a signal void on T2WI, similar to the cortical bone, can also be referred as a ‘signal void lesion’ and unless it has a T2 halo on T2WI can be dismissed as an enostosis/bone island. 8
When a lesion is focal and well defined but not in a region that is typically replaced with fat then its behaviour on FS and CS imaging must be assessed. Establishing that a lesion contains fat indicates a benign process. Even a central dot of fat may be enough to confirm that the lesion is benign or represents a prominent focal island of red marrow.4,13 Focal lesions that cannot be confirmed to contain fat should be considered indeterminate/worrisome and require further investigation which may include bone scan or biopsy.
When the lesion is not focal and a heterogeneous marrow pattern is identified, one must again assess the signal on FS and CS imaging but also the location and change in pattern over time. Marrow heterogeneity associated with foci of fat (high SI) on T1W or any fat-sensitive sequence should be considered a non-significant finding and can be dismissed. 13
Normal foci of red marrow will have concave margins due to the intermixing of fat while marrow-replacing lesions will often have convex margins. 11 Normal red marrow heterogeneity will either suppress completely on FS imaging or drop in signal on CS imaging. Any regions that are not behaving in this fashion are a cause for concern.
Another cause for concern is when the pattern of marrow heterogeneity has changed within the same patient on a follow-up MRI. An increase in size or number of focal lesions or areas of heterogeneous marrow should be viewed as suspicious for a pathologic process. One should again review any FS and CS imaging to determine if the region contains fat. If fat can be confirmed, then it can be dismissed but a reason for the change in red marrow should be sought. Typically, this is the result of some stimulus to the red marrow and resultant hyperplasia, which has been described in middle-aged obese women, heavy smokers and long distance runners but is also recognized in patients with haemoglobinopathies, systemic inflammation or in cancer treatment with granulocyte-colony stimulating factors (G-CSF).6,13
A final pattern of marrow heterogeneity that should always raise concern is when the marrow is diffusely and almost completely replaced, which should raise concern for diffuse marrow infiltration or proliferative marrow disorders.5,6,13
In most situations, patterns of marrow heterogeneity can be dismissed with these techniques and it is uncommon that further investigation is required.
Focal Osseous Lesions
Incidentally discovered osseous lesions on MR and CT are a common diagnostic dilemma, with a frequency of up to 10%.19,20 The objective is to accurately categorize lesions into those that can be ignored, vs those that require further workup.
Indeterminate bone lesions incidentally discovered on MR imaging should be correlated with conventional radiographs (or CT when available). Lesion margination predicts the aggressiveness of the process. Well defined, sclerotically marginated lesions are indolent and unlikely to be malignant (6%), whereas permeative lesions have a high likelihood of malignancy (80%). Intermediate-aggressivity lesions with ill-defined margination have a 50% likelihood of malignancy. 21 The size of the lesion, zone of transition and presence of periosteal reaction and internal matrix (or absence of such) can be assessed on plain radiographs/CT. The presence of chondroid or osteoid matrix can help categorize the nature of the lesion. Mineralized matrix, cortical integrity and periostitis can be difficult to recognize on MR alone. Other important clinical parameters to consider are patient age and history of malignancy, particularly with tumours that have a propensity to metastasize to bone.
Fatty Lesions
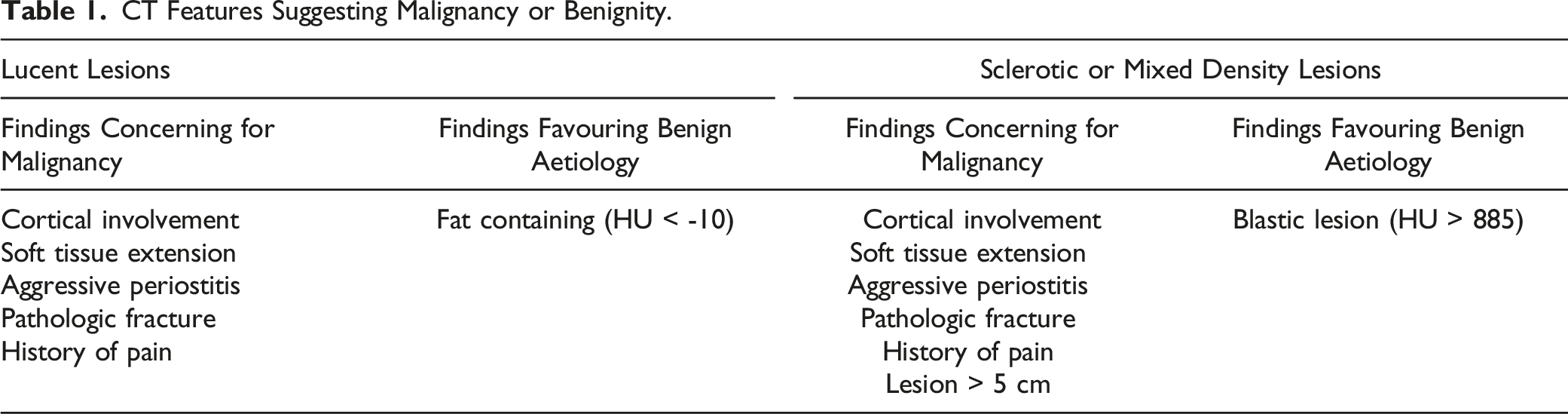
All lesions should be evaluated for the presence of fat. Hounsfield units of less than −10 or grossly visible fat on CT allows for the diagnosis of an intraosseous lipoma. Similarly, a lesion that is isointense to fat on all sequences on MR is a benign lipoma. Up to 35% of benign lipomas will have non-fatty components, making the diagnosis challenging. 22 Nonetheless, the presence of fat within the lesion allows it to be characterized as a lipomatous tumour. The identification of macroscopic fat in an intraosseous lesion on MR has a 99.5% likelihood of benignity. 18
Lytic Bone Lesions
Lytic (focal marrow-replacing) bone lesions incidentally discovered on MR imaging should be correlated with conventional radiographs (or CT) as previously outlined. In patients over age 40, metastasis, lymphoma and multiple myeloma must be considered.
As a generalization, benign MR imaging characteristics include homogenous internal signal, well circumscribed margins, lack of perilesional T2-hyperintensity and lack of involvement of contiguous structures. Malignant MR features include heterogenous internal signal, ill-defined borders, perilesional T2 hyperintensity and abnormal signal in adjacent structures. 23
Haemangiomas are common incidentally discovered intraosseous lesions. 24 In the vertebral body, a haemangioma is characterized either by vertical striations (corduroy cloth appearance) or by multiloculated lytic foci. 25 On CT, haemangiomas have low attenuation (fat) interspersed with thickened bone trabeculae, causing a characteristic salt and pepper appearance.
Sclerotic Lesions (Low T1 Low T2)
Bone islands (enostoses) are common, present in up to 14% of individuals. 26 Almost one-third of enostoses will change in size on serial imaging. 27 Diameter change of up to 25% in 6 months or 50% in 1 year is possible. Growth rates greater than this may require biopsy to exclude a neoplastic lesion. 28
On CT, bone islands should be densely sclerotic, with a brush border (jagged or spiculated borders that blend with the adjacent bone/trabeculae). A mean CT attenuation of >885 HU is a reliable threshold for the diagnosis of enostosis. Untreated blastic metastases will have lower mean attenuation values than enostoses. 29 On MR, enostoses should be homogenously low in signal (signal void) on all sequences. Conversely, the ‘halo sign’ (a peripheral rim of T2 hyperintensity surrounding a low signal lesion) on MR is highly specific for blastic bony metastatic disease. 18
Other sclerotic lesions will be discussed in subsequent sections.
Low T1 Low T2
These signal characteristics suggest calcification, fibrous tissue or blood products (hemosiderin).
Osteoblastic tumours include enostoses, osteoblastic metastatic disease, lymphoma, osteoblastic myeloma, osteoblastoma, osteoid osteoma and involuting non-ossifying fibroma. The calcified components of cartilaginous lesions (osteochondroma, chondroblastoma, chondrosarcoma and chordoma) will be low in signal on T1/T2.
Fibrous dysplasia could demonstrate low signal on T1/T2, but it is often variable in signal. The ground glass appearance on CT is specific. Benign and malignant fibrous tumours may have components that are low in signal on T1/T2. Approximately 2/3 of giant cell tumours will demonstrate T2 hypointensity. 30 The hemorrhagic component of any lesion (benign or malignant) will demonstrate low T1/T2 signal if it contains hemosiderin.
Low T1 High T2
This pattern of signal change is most common in intraosseous lesions. The presence of fluid, marrow oedema or mature cartilaginous matrix can lead to these signal characteristics. Enchondromas and intraosseous cysts often have a pathognomonic appearance on MR. The hyaline cartilage component of cartilage lesions is not evident on x-ray or CT, but on MR its high-water content will be low in signal on T1 and bright on T2WI. Atypical, lipid poor haemangiomas will also demonstrate this signal pattern.
There is a relatively small subset of lesions with fluid-fluid levels on MR. If the lesion is entirely composed of fluid-fluid levels then the diagnosis is aneurysmal bone cyst. Two-thirds of aneurysmal bone cysts are primary, whereas one-third are secondary in nature, where fluid–fluid levels may be seen in association with signal change indicating the presence of an underlying giant cell tumour or chondroblastoma. 31 The most important differential consideration is telangiectatic osteosarcoma. The presence of solid components, with enhancement and cortical destruction with an extraosseous soft tissue component make telangiectatic osteosarcoma the preferred diagnosis. 32 Solid lesions infrequently have fluid–fluid components but can include osteoblastomas, fibrous dysplasia and brown tumours.32,33
High T1 High T2
Lipomatous lesions, methemoglobin, proteinaceous fluid, melanin and haemangiomas are examples of entities in this category. Fatty lesions are discussed above. The majority of haemangiomas are lipid rich and will demonstrate T1 hyperintensity. Methemoglobin and proteinaceous fluid are usually small components of other principal lesions. Although T1 hyperintensity is considered a classic finding, this pattern is present in only 24–47% of melanoma metastases. 34
Cartilage Lesions
The imaging appearance of cartilage forming tumours depends on their composition. The annular or arc-like calcified component is sclerotic on Xray/CT and low in signal on all MR sequences. The hyaline cartilage component is not evident on x-ray/CT, but its water content will be low in signal on T1WI and bright on T2WI.
The differential diagnosis for cartilage forming tumours includes enchondroma, osteochondroma, juxtacortical chondroma (the surface version of enchondroma), chondroblastoma and chondrosarcoma.
Features that suggest chondrosarcoma (over enchondroma) include endosteal cortical scalloping involving greater than two-thirds cortical depth, cortical destruction, periostitis, lesions greater than 5 cm in size and soft tissue extension.35,36
Pain and an increase in size of a known osteochondroma raise the possibility of malignant transformation. In skeletally mature individuals, a cartilage cap that measures 2 cm or greater is predictive of chondrosarcomatous transformation. 37 Adventitial bursa formation mimics the appearance of malignant transformation on conventional MR imaging, as each of these demonstrate T2 hyperintensity. Fat-suppressed SPGR is helpful in distinguishing a thickened cartilage cap from adventitial bursal formation. 37 On fat-suppressed 3D SPGR images, hyaline cartilage appears as a high signal intensity structure relative to all other tissues, including fluid.
Summary of Intraosseous Lesions
MR imaging findings allow for a specific histologic diagnosis in the minority of intraosseous lesions, such as lipomas, haemangiomas, osteochondromas, enchondromas, aneurysmal bone cysts, intraosseous cysts and some liposarcomas. A history of a malignancy should raise the level of suspicion in the evaluation of all osseous lesions.
CT Features Suggesting Malignancy or Benignity.
MR Features Suggesting Malignancy or Benignity.
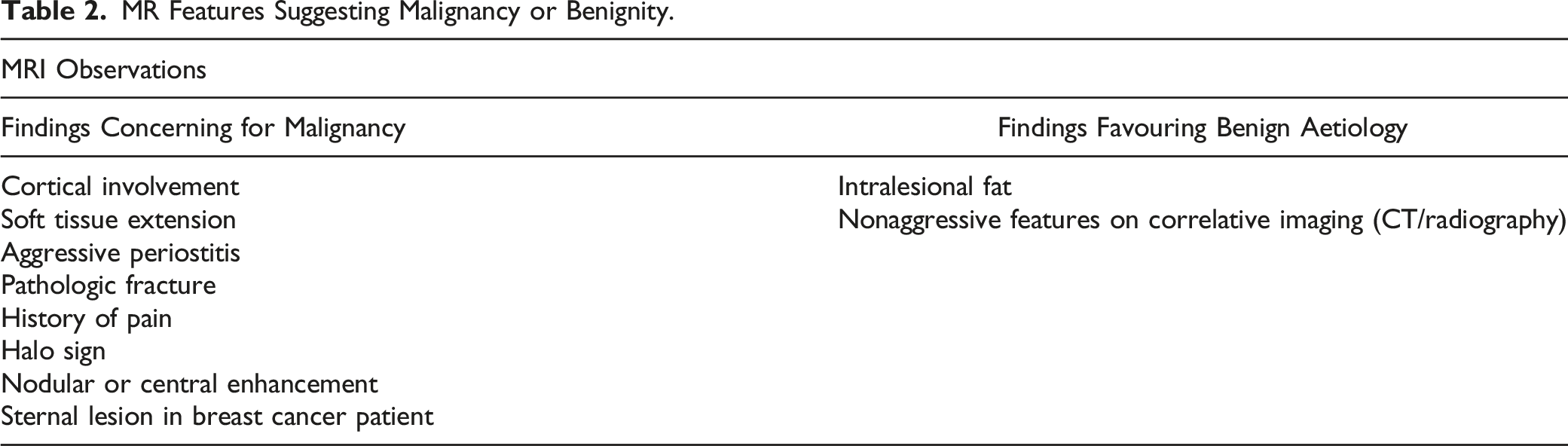
In the absence of these concerning features, lesions in low risk patients are likely to represent benign fibro-osseous lesions of no clinical concern.
Changes in and Around the Pelvis
Pubic Symphysis
Marginal irregularity, sclerosis, erosive changes and widening (>7 mm) of the pubic symphysis are incidental findings which can result from several conditions. These include osteitis pubis, which is an inflammatory response to mechanical stress particularly common in athletes, and severe cases can be associated with symphyseal fluid as well as marrow and adjacent soft tissue oedema on MR. Similar findings can also be seen in septic arthritis/osteomyelitis but this is rarely an asymptomatic incidental finding. Infection may show more prominent osseous destruction, gas, prominent soft tissue oedema or loculated perisymphyseal fluid collections. Seronegative spondyloarthropathies can also overlap with this appearance but may have more prominent bony proliferation or ankylosis as well as characteristic distribution involving more than one joint. Symphysis pubis diastasis of pregnancy can result in widening of >1 cm and could be associated with irregularity and sclerosis and is not uncommonly associated with findings in the SI joints. Post-traumatic changes (including parasymphyseal insufficiency fractures) and hyperparathyroidism may also result in some of these same changes. Ultimately, the clinical context is vital in narrowing the differential diagnosis.38,39
Mild sclerosis or irregularity of the pubic symphysis is sufficiently common in middle-aged to elderly individuals that it can be ignored. The Working Group recommends that findings of erosions, symphyseal widening, marrow oedema, soft tissue oedema or fluid collections should be reported with a recommendation to correlate to clinical symptomatology and context.
Sacroiliac Joints
Findings of SIJ asymmetry, irregularity, focal joint space narrowing (defined as <2 mm), subchondral sclerosis (on both sides or iliac predominant) and osteophyte formation (sometimes with ossification of the nonarticular part of the joint) are increasingly common with age and usually not associated with significant pathology when seen as an incidental finding in an asymptomatic patient. Erosive changes, intraarticular ankylosis (fusion of the synovial portion, typically the inferior half to one-third of the joint), uni- or bilateral uniform joint space loss and sacral-side predominant sclerosis in patients under 40 years of age are all quite rare in the normal population and should prompt more concern for sacroiliitis.40,41
Osteitis condensans ilii is typically triangular-shaped sclerosis involving the iliac side of the inferior aspect of the joint without other findings (such as erosions or narrowing). It is usually symmetric and occurs most commonly in asymptomatic multiparous women (although an association with low back pain may be seen). Its appearance is characteristic enough that it can usually be diagnosed and dismissed. 42
SIJ oedema and/or enhancement on MRI is a sign of inflammation or infection, but its prevalence in asymptomatic individuals and the likelihood of it being secondary to joint degeneration compared to more aggressive processes when incidentally identified is not well described in the literature. In the absence of such scientific guidance, the Working Group recommends that incidental SIJ oedema and/or enhancement be commented on in a report with a recommendation to evaluate if the patient is symptomatic to guide further testing and management.
Iliopsoas Bursitis and Cystic Inguinal Masses
The iliopsoas bursa is a potential fluid filled space located between the iliopsoas muscle and anterior capsule of the hip and lateral to the femoral vessels. The bursa is typically collapsed but when irritated, synovial fluid overproduction and synovial hypertrophy leads to the appearance of a fluid filled structure on cross sectional imaging.43,44 Although it can be isolated, it is most commonly associated with osteoarthritis of the ipsilateral hip joint. 43 The cystic nature can be easily determined with imaging and characteristic location and communication with the hip joint on MRI (in approximately 15% of patients 44 ) allow for accurate diagnosis. 44 Fluid filled inguinal or femoral hernias can mimic iliopsoas bursitis. 44
Fluid in the iliopsoas bursa can mimic an inguinal mass or lymphadenopathy when it is solid appearing from haemorrhage, synovium or proteinaceous material. 45 The bursa can even contain normal gas from the ipsilateral hip joint communicating with the bursa, leading to the false diagnosis of an abscess. 46 If the patient has had a prior hernia repair, it is important not to confuse a prolene plug as a mass or lymphadenopathy. These are typically located anterior to the iliac vessels at the inguinal canal, appearing ring-like with central fat on CT, have low T1 and low to intermediate T2 signal on MRI, and can enhance post contrast. The presence of an overlying surgical scar or other surgical clips can be helpful. 47 Coronal image reformats can help see the characteristic conical shape.
In females, the differential for a cystic mass in the inguinal region also includes a hydrocele of the Canal of Nuck. The Canal of Nuck is a thin evagination of peritoneum extending along the round ligament from the uterus and into the inguinal canal. Rarely, it does not completely disappear and is analogous to the patent processus vaginalis in males. It may also give rise to an indirect inguinal hernia in females. 48
Soft Tissue Fatty Masses
A consensus paper on the ultrasonography of superficial soft tissue masses was recently published by Jacobson et al, reviewing the US features of common superficial soft tissue lesions with suggested management guidelines based on current literature and practice patterns. 49 The Working Group endorses this paper, while recognizing that many lesions found on ultrasound are typically palpable and are not found incidentally. As such, the Working Group decided to focus on incidental soft tissue and fatty masses commonly found on CT and MRI.
Lipomas
The vast majority of fat-containing soft-tissue masses are benign, especially those discovered incidentally. Lipomas are by far the most common fat-containing masses and account for almost half of all encountered benign soft tissue tumours. 50 Lipomas are most commonly located within the superficial soft tissues of the extremities and back. Deep lipomas in the retroperitoneum or chest (beneath the superficial fascia) are rare and when encountered, an alternative diagnosis should also be considered for lesions in these locations. 51 Additionally, tumour size greater than 10 cm is an independent risk factor for ALT/WDLPS. 52 With these exceptions, incidental benign lipomas can be confidentially diagnosed on CT or MRI, demonstrating homogenous attenuation/signal similar to subcutaneous fat. These lesions require no additional evaluation. They may contain a few thin septa measuring up to 2 mm in thickness. 53 Unlike lipomatosis, lipomas are clearly defined with a discrete capsule.
Atypical Lipomatous Tumours, Well-Differentiated Liposarcomas and Dedifferentiated Liposarcomas
Atypical lipomatous tumours (ALT) and well-differentiated liposarcomas (WDLPS) are the most common liposarcomas and arise most commonly in the deep soft tissues of the limbs, especially the thigh, followed by the retroperitoneum, paratesticular area and mediastinum. 54 While both these tumours have identical morphology, karyotype and biological behaviour, ALT is preferred when referring to lesions arising in the limbs and trunk, while tumours located in the retroperitoneum, mediastinum or spermatic cord are often referred to as WDLPS. This is due to the relative poorer prognosis when located in these regions, due to the difficulty of resection with clear margins. 55 These tumours are slow growing and may be locally aggressive but have no potential for metastasis. They demonstrate high rates of local recurrence and potential for dedifferentiation into higher grade sarcomas. True spermatic cord lipomas or WDLPS are rare and the working group suggests refraining from using either term unless the lesions are large (greater than 5 cm in diameter) and have complex features to suggest liposarcoma. To avoid confusion, the working group suggests using the term fatty hypertrophy for the more common fatty proliferation seen in the spermatic cord on CT. ALT/WDLPS are predominately fatty with small non-adipose components, usually less than 2 cm in size. They can contain thick irregular septa or calcifications in up to 30% of these tumours. 53
High grade sarcomas such as dedifferentiated liposarcomas (DDLPS) are aggressive with metastatic potential. These are usually larger at presentation and often contain a larger non-fatty component, although the imaging appearance of DDLPS can overlap with ALT/WDLPS. Biopsy of the non-fatty component is often required to assess lesions that cannot be confidently characterized as lipomas or other benign entities to assess histology and molecular markers and to guide therapy. Immunohistochemistry for the trio of CDK4, MDM2 and p16 is a useful adjunct in the histologic diagnosis of ALT/WDLPS and DDLPS, helping to distinguish this group of tumours from other adipocytic neoplasms. 56
Soft Tissue Cavernous Haemangioma
Soft tissue cavernous haemangiomas (also known as slow-flow venous malformations) are often intramuscular and occur in the 2nd or 3rd decade of life. They are composed of dilated, blood-filled spaces, smooth muscle and reactive overgrowth of fat. 57 These lesions are well defined, lobulated and heterogenous. They contain large internal vessels with avid enhancement on CT and MRI. Approximately 50% of soft tissue cavernous haemangiomas contain calcified phleboliths and this is a key differentiator. 58 Most lesions demonstrate fat along the periphery of the lesion and extending into it, which is believed to be a reactive process resulting in fat hypertrophy. 57 Benign soft tissue cavernous haemangiomas can be confused with more sinister liposarcomas due to the soft tissue and fat components. An understanding of the imaging appearance of this entity is crucial in alerting the radiologist to this benign diagnosis, especially in patients under the age of 40 years.
Elastofibroma Dorsi
Elastofibroma dorsi is a benign soft tissue tumour with a characteristic location and appearance at CT, often found incidentally and more common in women. Elastofibroma dorsi are classically found in the infrascapular regions, deep to the serratus anterior and latissimus dorsi muscles. They occur bilaterally in up to 60% of cases, and when occurring bilaterally the diagnosis is further supported. 59 On CT, elastofibroma dorsi appear as poorly defined, lentiform shaped, soft tissue masses with attenuation similar to muscle and internal linear striations of fat attenuation. 60 Further imaging studies or tissue sampling is not required for diagnosis of elastofibroma dorsi when the classic CT findings are present. Atypical features, including adjacent bone destruction or intense contrast enhancement, should raise suspicion of a more concerning aetiology such as a sarcoma or metastatic disease and warrant further evaluation and biopsy.
Renal Osteodystrophy
Renal osteodystrophy occurs in patients with chronic renal insufficiency secondary to both vitamin D deficiency causing osteomalacia and secondary hyperparathyroidism as a response to low serum calcium levels. In chronic renal failure, elevated serum phosphate depresses serum calcium levels leading to hyperplasia of the parathyroid glands and increased levels of parathyroid hormone.61,62
Brown tumours are typically solitary, expansile and lytic and can easily be mistaken for a primary bone lesion especially in younger patients if the appropriate history of chronic renal failure is unknown. 63 They more frequently occur in the mandible, ribs, clavicle, pelvis and femora.61,64 Brown tumours can be expansile with cortical disruption and associated with a soft tissue component which can appear nonspecific on MR.65,66 Brown tumours are usually incidental but can present with insidious pain or as a pathologic fracture. 66 Imaging evaluation should include the search for evidence of either primary or secondary hyperparathyroidism (such as alternating bands of increased density at the vertebral body endplates – the ‘rugger jersey spine’). 67 Examples can be seen in the Supplementary Appendix.
Although the finding of subperiosteal bone resorption on the radial aspect of the index and long finger middle phalanges is pathognomonic for secondary hyperparathyroidism, bone resorption can still occur around joint margins and the SIJ mimicking septic arthritis, rheumatoid arthritis and seronegative spondyloarthropathies61,63 Resorption can involve the distal phalangeal tufts, ribs, long bones, AC joints, skull (‘salt and pepper’ appearance) and subligamentous/subtendinous regions.68,69 Osseous resorption can be so extensive that it can even mimic multiple myeloma and metastatic disease.
Other imaging findings of renal osteodystrophy include the deposition of calcium or amyloid in soft tissues and organs. 63
Opportunistic Osteoporosis Evaluation
Osteoporosis is a common, treatable and under-diagnosed condition which significantly increases lifetime risk of fracture. 68 While central dual-energy x-ray absorptiometry (DEXA) remains the standard to diagnose osteoporosis, recent publications have suggested CT attenuation may be useful as a surrogate to opportunistically prompt consideration of further workup or treatment. In 2013, Pickhardt et al measured the attenuation of the L1 vertebral body (120 KvP, axial plane, anterior, largest region of interest without including the posterior venous plexus), with >90% sensitivity and specificity in the diagnosis of osteoporosis at 110 HU, and a 99% negative predictive value at 200 HU. 67 A more recent review of over 20,000 patients stratified by age demonstrated that, regardless of age, L1 measurement <100 HU (120 KvP) raises concern for osteoporosis. This study also found minimal change in measurement with CT contrast use among the middle-aged or elderly populations, supporting evaluation opportunistically on unrelated CT examinations. 69
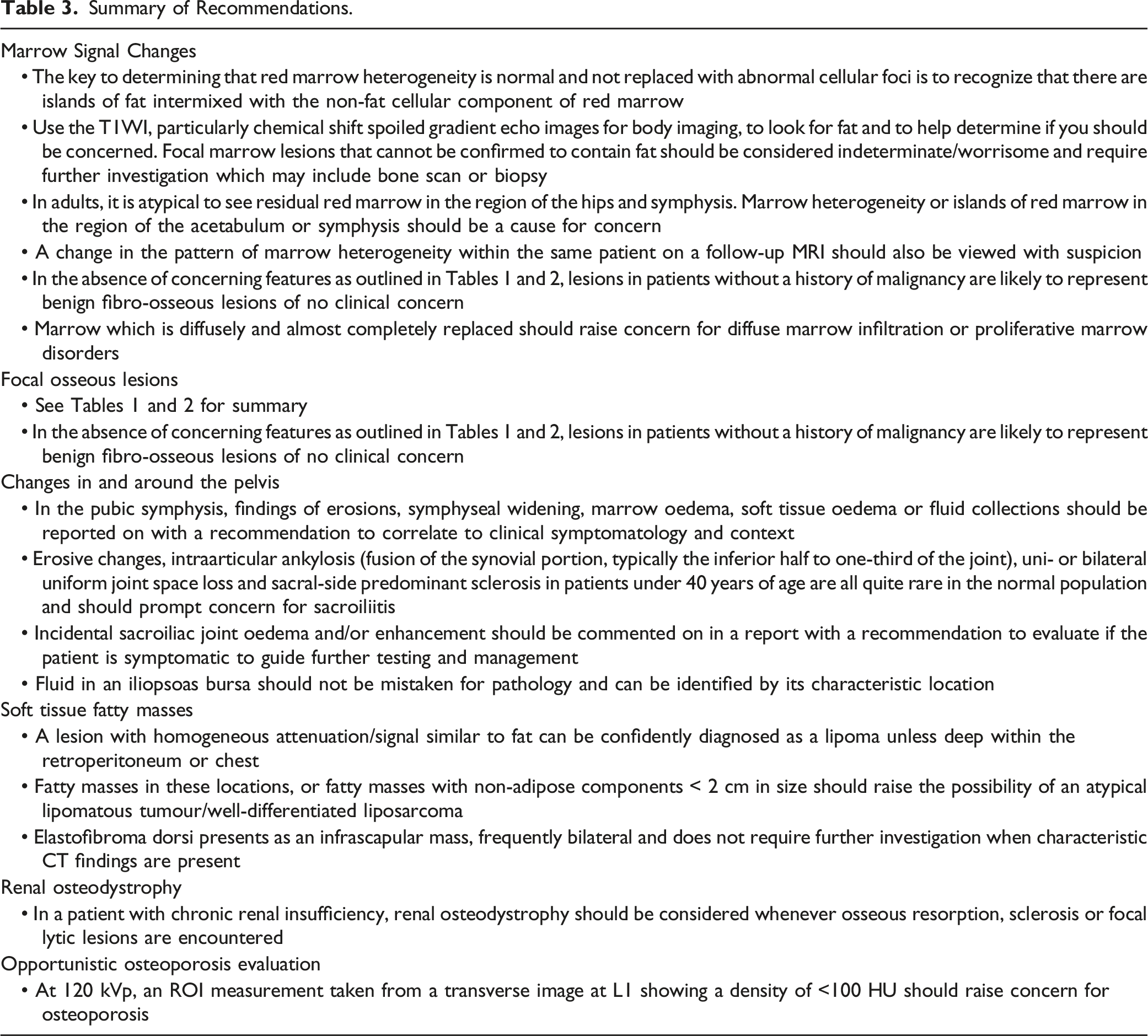
Summary of Recommendations.
Supplemental Material
Supplemental Material - Recommendations for the Management of Incidental Musculoskeletal Findings on MRI and CT
Supplemental Material for Recommendations for the Management of Incidental Musculoskeletal Findings on MRI and CT by Gina Di Primio, Gordon J. Boyd, Christopher I. Fung, Casey Hurrell, Gary L. Brahm, Jeffery R. Bird, Steven J. Co and Iain D. C. Kirkpatrick in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
The authors would like to thank the members of the Canadian Association of Radiologists who took the time to provide their feedback and peer review during the drafting of these guidelines.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.