
Abstract
Introduction
According to the American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS), a finding assessed as probably benign (BI-RADS 3) should carry a likelihood of malignancy of less than or equal to 2%. 1 Short-interval follow-up of probably benign lesions, typically performed at 6, 12, and 24 months after the initial BI-RADS 3 assessment, allows the radiologist to establish stability of the finding before recommending return to routine screening. The purpose of the BI-RADS 3 assessment category is to reduce biopsies of benign findings while retaining a high sensitivity for early breast cancer detection.
The BI-RADS 3 assessment category is not intended for use when the radiologist is uncertain whether to render a benign (BI-RADS 2) or suspicious (BI-RADS 4) assessment. It is intended for baseline studies with findings requiring stability over time for assessment as benign. Three specific mammographic findings have been validated as probably benign in several prospective clinical studies, including a noncalcified circumscribed solid mass, a focal asymmetry, and a solitary group of punctate calcifications.2-7 For breast ultrasound, there is robust evidence that a solid mass with a circumscribed margin, oval shape, and parallel orientation (most commonly, a fibroadenoma), and an isolated complicated cyst or cluster of microcysts may be characterized as probably benign.2,8,9 The radiologist may designate other findings as probably benign on a discretionary basis if he or she has observed a sufficient number of cases of this additional finding to suggest a likelihood of malignancy of less than 2%.1,10
In practice, there is significant interobserver variability in the assessment of BI-RADS 3 findings. 11 Indeed, inappropriate utilization of the BI-RADS 3 assessment category can result in delayed diagnosis of breast cancer or excessive follow-up of benign findings, increased healthcare costs, unnecessary radiation exposure, and undue patient anxiety. 12 The aim of this study was to evaluate outcomes of breast lesions assessed as probably benign following mammographic and/or ultrasound evaluation at a single tertiary breast cancer screening center.
Materials and Methods
This study was approved by the institutional research ethics board. The retrospective analysis was limited to average-risk women with a mammographic and/or ultrasound examination first assessed as BI-RADS category 3 at a single tertiary breast cancer screening center between January 1 and December 31, 2017. The Ontario Breast Screening Program (OBSP) recommends screening with mammography every 2 years for average-risk women ages 50–74. 13 We excluded high-risk women (under the High Risk Ontario Breast Screening Program) and those with a first BI-RADS 3 assessment before January 1, 2017, or on an outside examination referred to our center for consultation.
Outcomes of biopsies and follow-up imaging were extracted from the electronic medical record (EMR). All cancers were pathologically proven. Benign lesions were pathologically proven, downgraded to BI-RADS 1 or 2 at follow-up, or demonstrated imaging stability at 36 months. Cancer yield, positive biopsy rate, and loss to follow-up were calculated at each interval, and cumulatively at 36 months. Women were defined as lost to follow-up if they did not did not return for follow-up of a probably benign lesion in surveillance up to 36 months. Women who returned for follow-up of a probably benign lesion later than recommended, but within the 36-month follow-up period, were not considered lost to follow-up.
Patient characteristics including age, breast density (taken from the most recent mammography report, when available), availability of prior breast imaging (documented in the EMR or referenced in the radiology report), and personal history of breast cancer were recorded. Breast imaging indication and modalities used for follow-up were documented.
Lesion characteristics including description and size of the most significant findings on mammography and/or ultrasound were extracted from the radiology report. In women with more than 1 significant finding on mammography and/or ultrasound, the descriptions were recorded separately. Only the largest single dimension was recorded. A finding was considered significant if it was included in the conclusion of the radiology report with the BI-RADS 3 assessment category and follow-up recommendations.
All mammographic and ultrasound examinations were performed at our tertiary breast cancer screening center and interpreted by 1 of 5 breast radiologists. Ultrasound images were acquired by 1 of 7 breast sonographers and reviewed with the on-site breast radiologist, who rescanned patients with detected breast lesions at his or her discretion prior to image interpretation. At our center, screening and diagnostic mammograms are interpreted on the date of the examination by the on-site radiologist. Women requiring additional evaluation of a screening mammogram are recalled. Ultrasound examinations are performed on the same date as diagnostic mammography, when indicated. The interpretation of both studies is summarized in a single report. Results are sent to the patient (and referring physician) by mail. The radiologist may also communicate results directly to the patient on the date of the examination, although this is not routine.
Statistical Analysis
Descriptive statistics (median and range) were produced to provide a quantitative description of the population. Binary multivariate logistic regression models were created to investigate the relationship between loss to follow-up and each of age, availability of prior breast imaging, breast imaging indication, and breast density. This analysis produced adjusted Odds Ratios (OR) and 95% Confidence Intervals (95% CI). The threshold for statistical significance was P < .05 for all comparisons. All statistical analyses were performed using Stata, Version 16 (StataCorp., College Station, TX).
Results
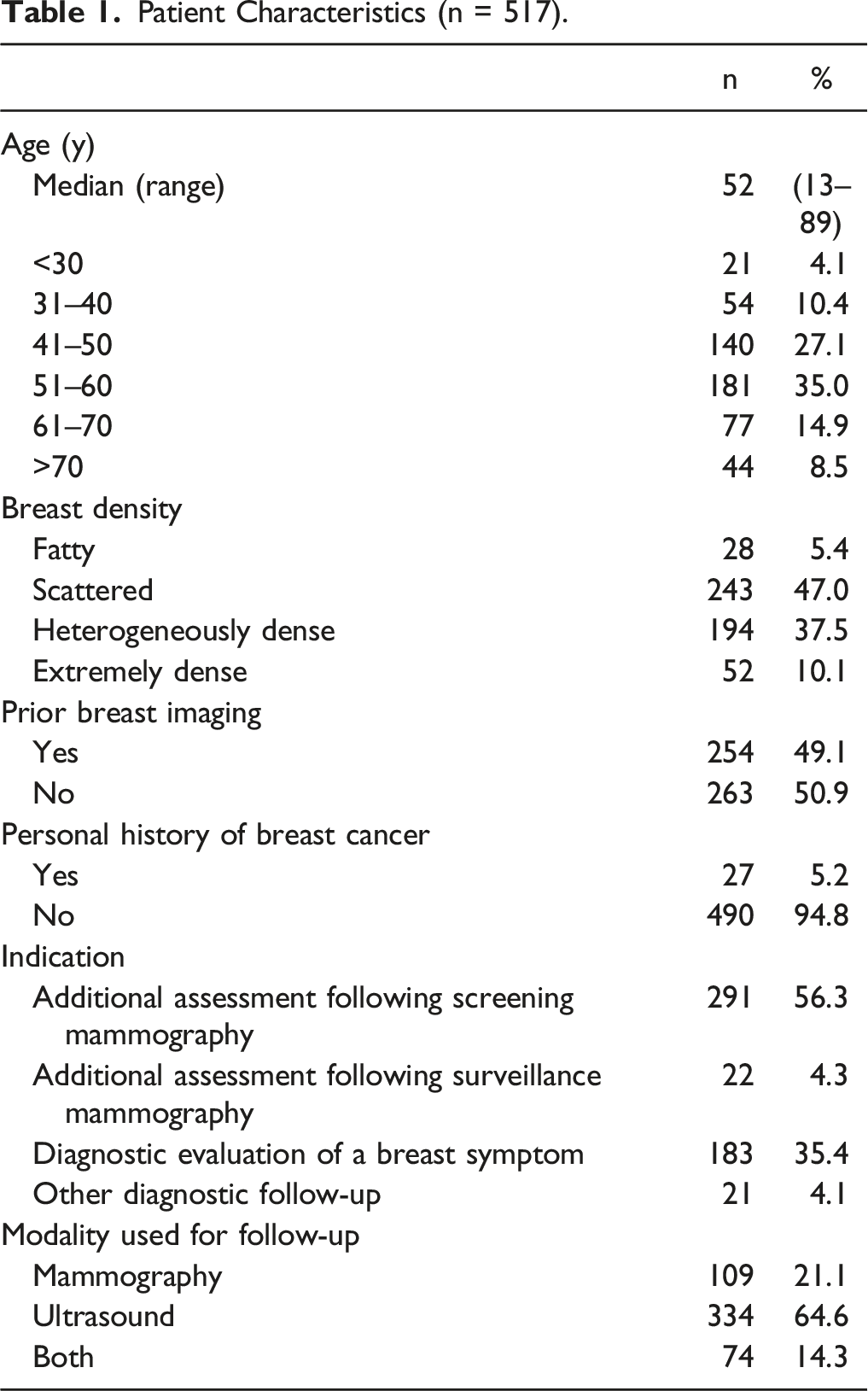
Patient Characteristics (n = 517).
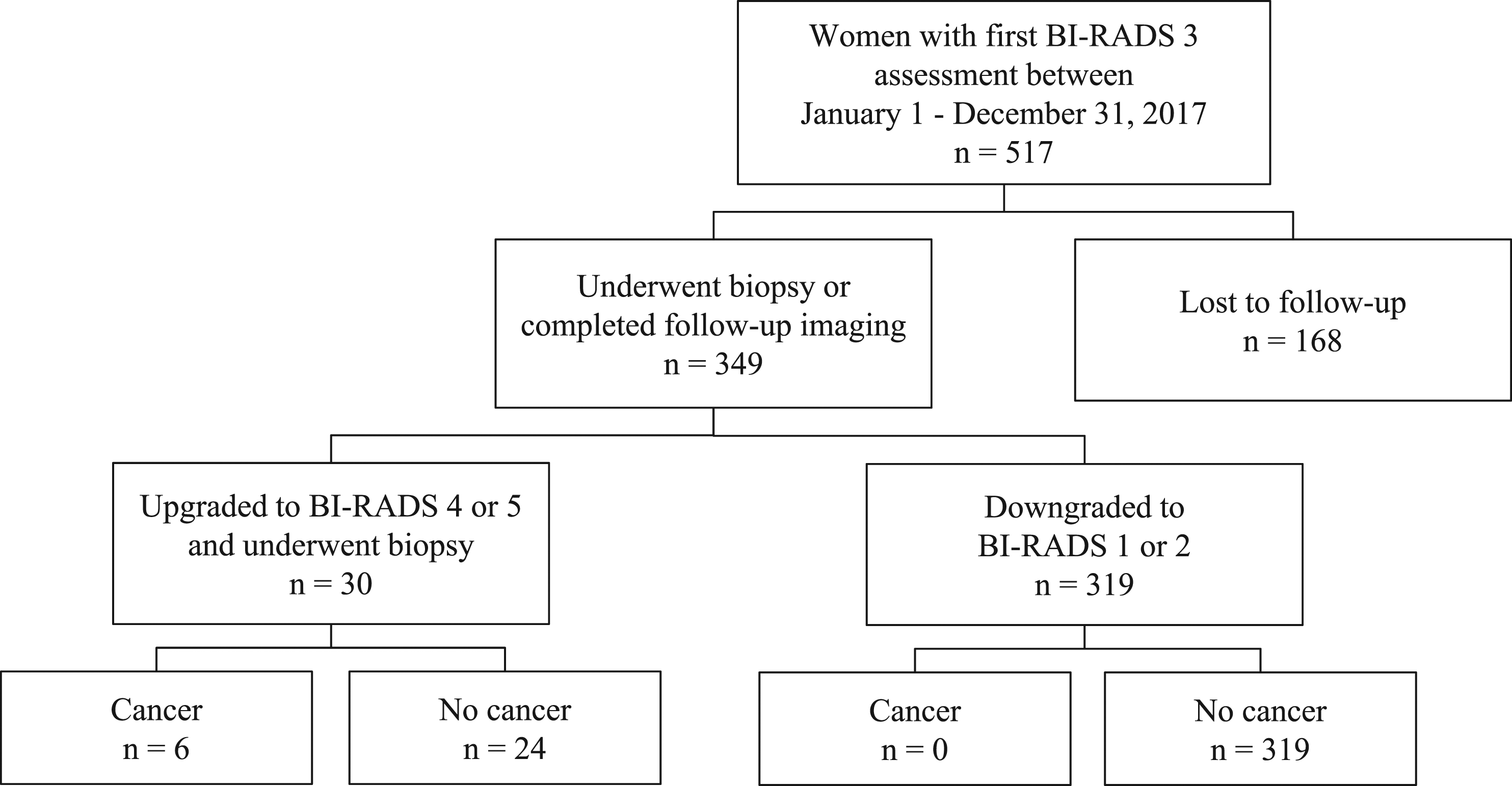
36-month outcomes of 517 women with BI-RADS 3 lesions on mammography and/or breast ultrasound.
0–90-Day Follow-Up
Follow-Up (n = 517).
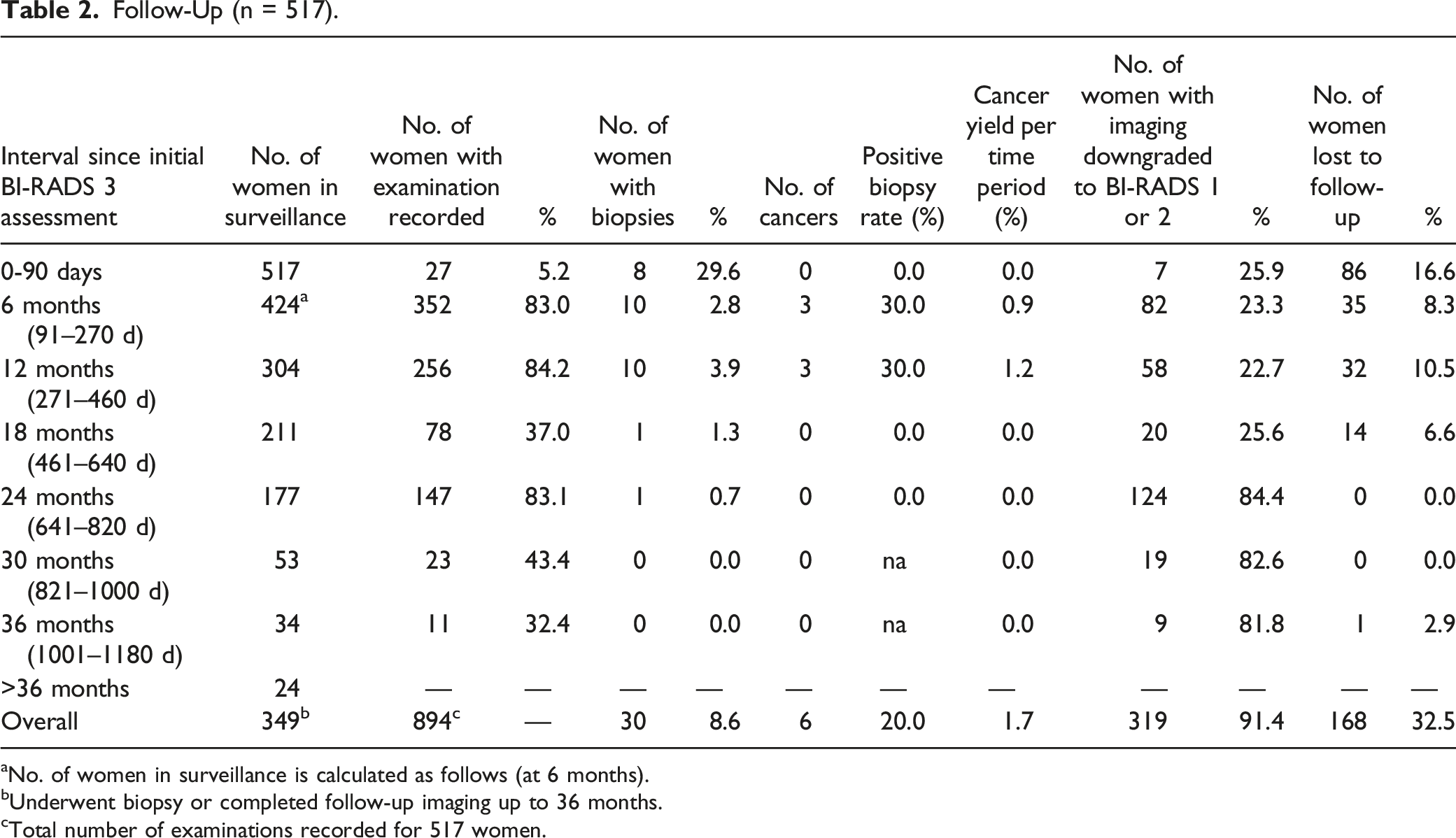
aNo. of women in surveillance is calculated as follows (at 6 months).
bUnderwent biopsy or completed follow-up imaging up to 36 months.
cTotal number of examinations recorded for 517 women.
Biopsy Results (n = 30).
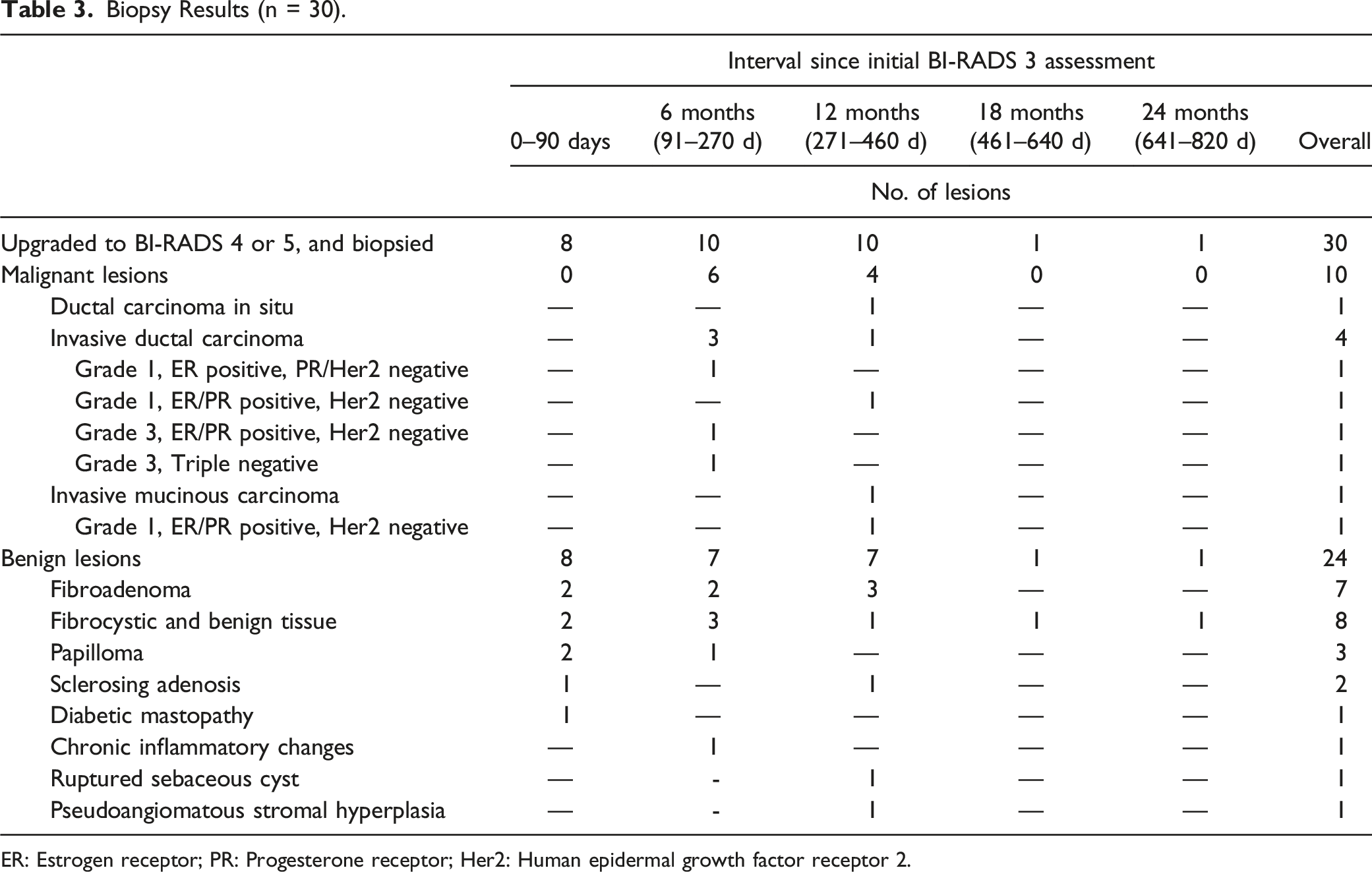
ER: Estrogen receptor; PR: Progesterone receptor; Her2: Human epidermal growth factor receptor 2.
6-Month Follow-Up
Among 424 women requiring follow-up, 352 (83.0%) underwent repeat imaging at 6 months (Table 2). Ten of 352 women (2.8%) underwent biopsy, and 3 of 10 biopsies were malignant (cancer yield, 3 of 352 women [.9%]; positive biopsy rate, 3 of 10 women [30%]). The indications for biopsy included lesion growth (3 women), suspicious calcifications (2 women), non-circumscribed margins (2 women), other suspicious change in appearance (2 women), and patient preference (1 woman). All 3 women were diagnosed with invasive ductal carcinoma (IDC) (Table 3). Findings in 82 of 352 women (23.3%) were downgraded to BI-RADS 1 or 2. Thirty-five of 424 women (8.3%) were lost to follow-up at 6 months.
12-Month Follow-Up
Among 304 women requiring follow-up, 256 (84.2%) underwent repeat imaging at 12 months (Table 2). Ten of 256 women (3.9%) underwent biopsy, and 3 of 10 biopsies were malignant (cancer yield, 3 of 256 women [1.2%]; positive biopsy rate, 3 of 10 women [30%]). The indications for biopsy included suspicious calcifications (4 women), lesion growth (3 women), non-circumscribed margins (2 women), and other suspicious change in appearance (1 woman). One woman was diagnosed with ductal carcinoma in situ (DCIS), 1 with IDC, and 1 with invasive mucinous carcinoma (Table 3). Findings in 58 of 256 women (22.7%) were downgraded to BI-RADS 1 or 2. Thirty-two of 304 women (10.5%) were lost to follow-up at 12 months.
18-Month Follow-Up
Among 211 women requiring follow-up, 78 (37.0%) underwent repeat imaging at 18 months (Table 2). One of 78 women (1.3%) underwent biopsy for lesion growth, which demonstrated benign fibrocystic changes (cancer yield, 0 of 78 women [0%]; positive biopsy rate, 0 of 1 woman [0%]) (Table 3). Findings in 20 of 78 women (25.6%) were downgraded to BI-RADS 1 or 2. Fourteen of 211 women (6.6%) were lost to follow-up at 18 months.
24-Month Follow-Up
Among 177 women requiring follow-up, 147 (83.1%) underwent repeat imaging at 24 months (Table 2). One of 147 women (.7%) underwent biopsy for lesion growth, which demonstrated benign fibrocystic changes (cancer yield, 0 of 147 women [0%]; positive biopsy rate, 0 of 1 woman [0%]) (Table 3). Findings in 124 of 147 women (84.4%) were downgraded to BI-RADS 1 or 2. No women were lost to follow-up at 24 months.
>24-Month Follow-Up
Fifty-three of 517 women (10.3%) remained for follow-up beyond 24 months (Table 2). No women underwent biopsy after 24 months (cancer yield, 0 of 53 women [0%]). Findings in 28 of 53 women (52.8%) were downgraded to BI-RADS 1 or 2 at the 30- or 36-month follow-up. One of 34 women (2.9%) was lost to follow-up at 36 months. Twenty-four of 517 women (4.6%) required follow-up beyond 36 months.
Effect of Age on Loss to Follow-Up
Binary Logistic Regression Model for Loss to Follow-Up With Age as a Continuous Variable (n = 517).
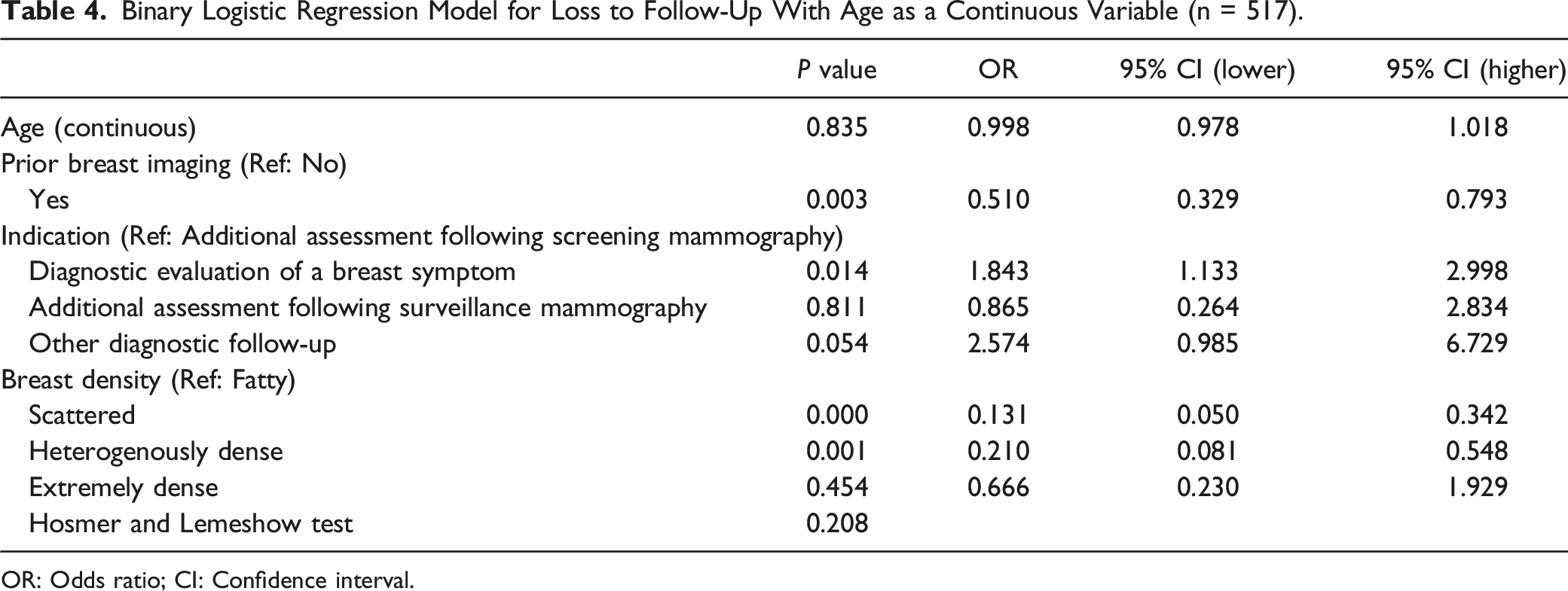
OR: Odds ratio; CI: Confidence interval.
Effect of Prior Breast Imaging on Loss to Follow-Up
Among 517 women with BI-RADS 3 assessments in the study period, 254 (49.1%) had prior breast imaging available (Table 1). Women with prior breast imaging were significantly less likely to be lost to follow-up compared to those without prior imaging (OR .510, P = .003) (Table 4).
Effect of Breast Imaging Indication on Loss to Follow-Up
Four hundred and ninety of 517 women (94.8%) had no personal history of breast cancer. The majority of women received their first BI-RADS 3 assessment on imaging acquired for additional evaluation following screening mammography (291 of 517 women [56.3%]) or diagnostic evaluation of a breast symptom (183 of 517 women [35.4%]) (Table 1). Women who underwent breast imaging for diagnostic evaluation of a breast symptom were significantly more likely to be lost to follow-up compared to those recalled for additional assessment following a screening mammogram (OR 1.843, P = .014) (Table 4).
Effect of Age, Prior Imaging, or Personal History of Breast Cancer on Cancer Yield
Six women (median age, 70 years; range, 49–72 years) with a mammogram and/or ultrasound first assessed as BI-RADS 3 were diagnosed with breast cancer. Among them, 5 (83.3%) had prior breast imaging available for comparison. None had a personal history of breast cancer. All examinations were performed for additional evaluation following screening mammography. Four of 6 women (66.7%) had breast density characterized as scattered, and 2 (33.3%) as heterogeneously dense. The modalities used for follow-up in these women included mammography alone in 2 women (33.3%), ultrasound alone in 3 women (50.0%), and both mammography and ultrasound in 1 woman (16.7%). It was not possible to generate a stable regression model for the effect of age, prior imaging, or personal history of breast cancer on cancer yield due to the small sample size of women diagnosed with cancer in our cohort (n = 6).
Effect of Lesion Type on Cancer Yield
Lesion Characteristics (n = 569) a .
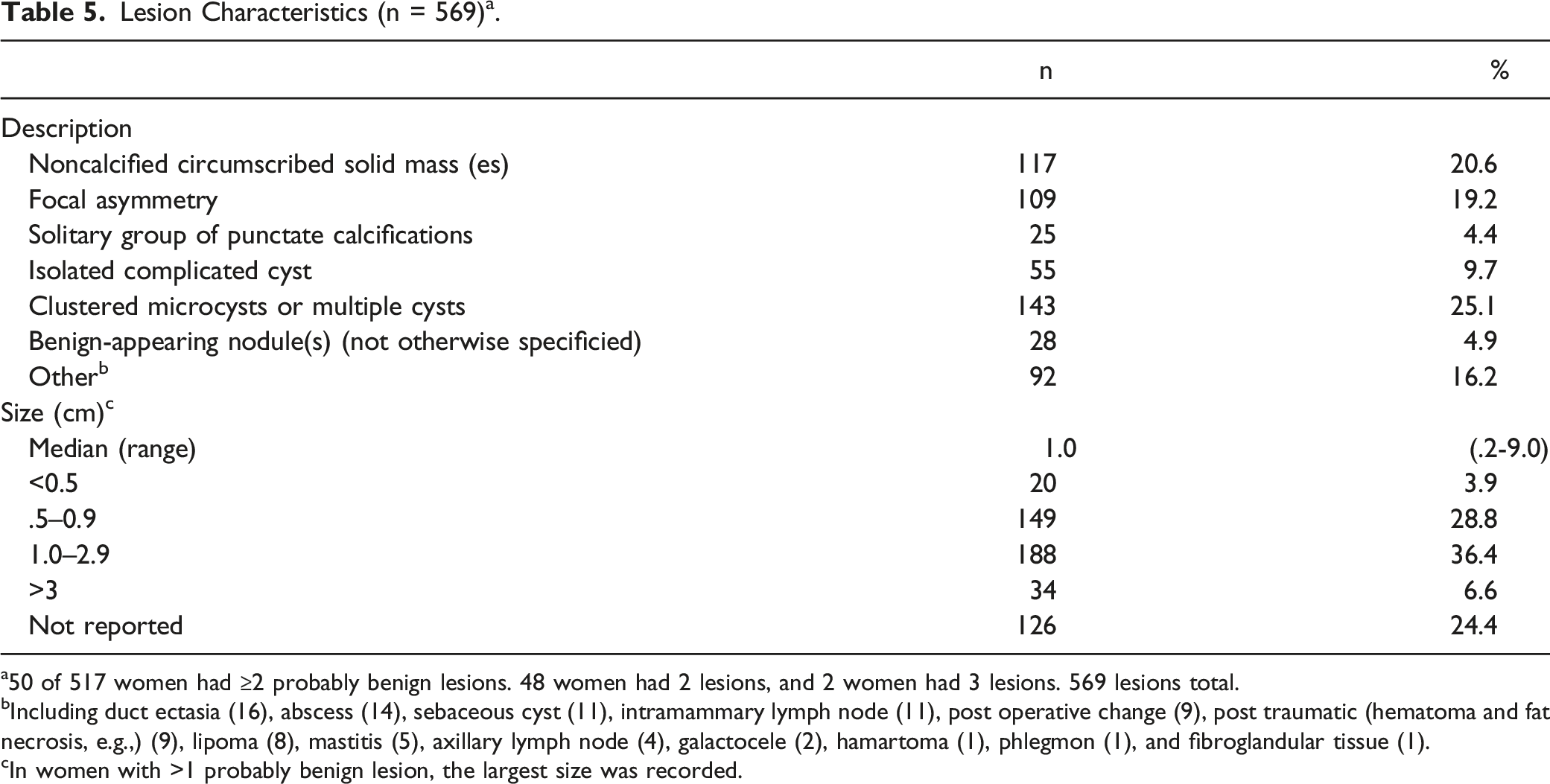
a50 of 517 women had ≥2 probably benign lesions. 48 women had 2 lesions, and 2 women had 3 lesions. 569 lesions total.
bIncluding duct ectasia (16), abscess (14), sebaceous cyst (11), intramammary lymph node (11), post operative change (9), post traumatic (hematoma and fat necrosis, e.g.,) (9), lipoma (8), mastitis (5), axillary lymph node (4), galactocele (2), hamartoma (1), phlegmon (1), and fibroglandular tissue (1).
cIn women with >1 probably benign lesion, the largest size was recorded.
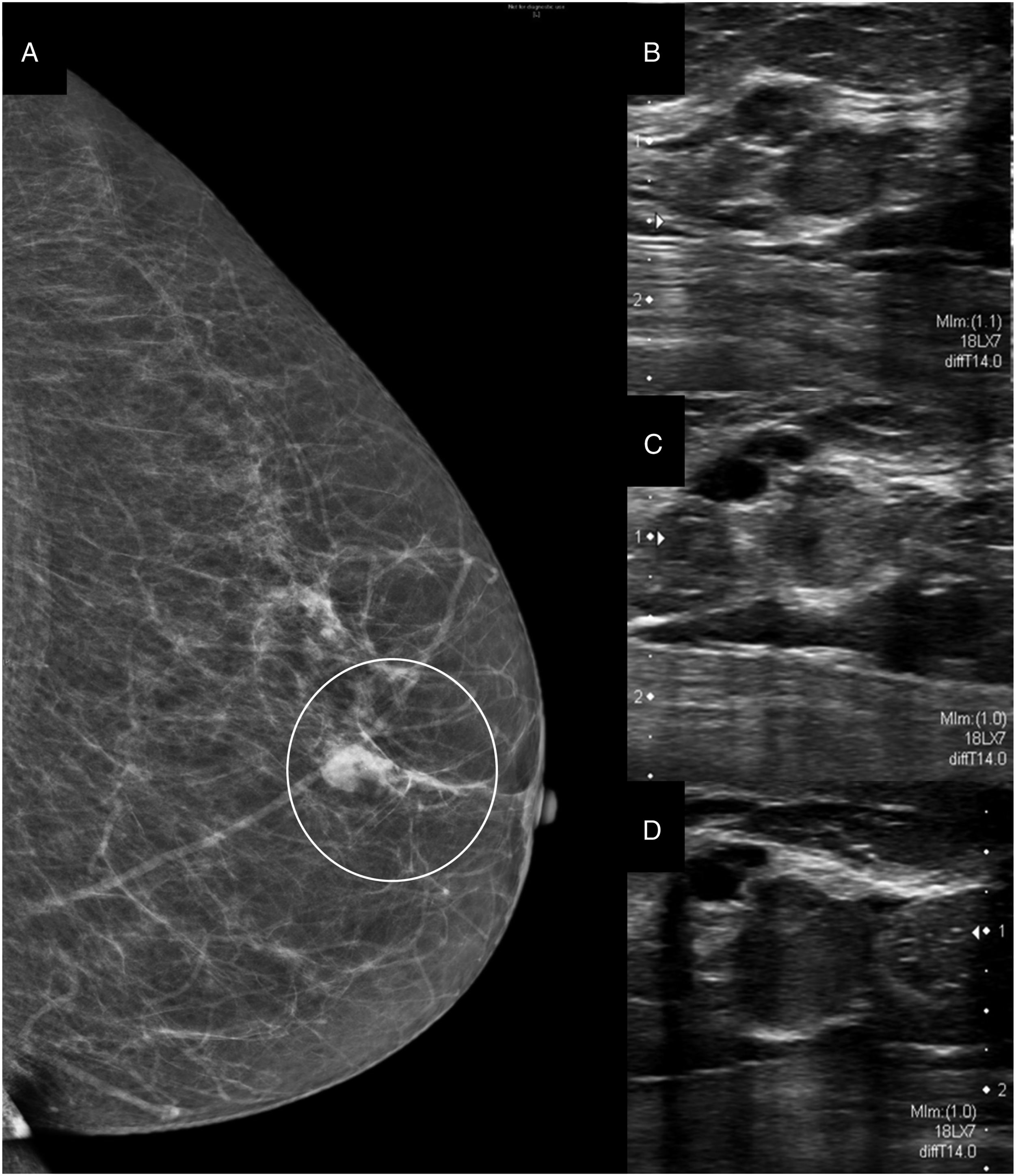
71-year-old woman recalled from screening mammography for a focal asymmetry (circled) in the retroareolar region of the left breast, best demonstrated on the mediolateral oblique (MLO) view (A). The asymmetry persisted on additional tomographic views (not shown). Targeted ultrasound (B) demonstrated a cluster of microcysts adjacent to a “circumscribed” hypoechoic mass measuring 8 × 8 × 6 mm. This should have been described as microlobulated, prompting suspicious assessment and biopsy. However, these lesions were assessed as probably benign (BI-RADS 3), and a 6-month follow-up ultrasound (C) was recommended. At 6 months, the cluster of microcysts was not significantly changed. The microlobulated hypoechoic mass had increased in size minimally measuring 9 × 9 × 7 mm, and a 6-month follow-up ultrasound (D) was advised. At 12 months, the cluster of microcysts remained unchanged. The microlobulated mass had once again increased in size, now measuring 11 × 10 × 10 mm. The lesion was upgraded to suspicious (BI-RADS 4), and ultrasound-guided biopsy (not shown) was consistent with an invasive mucinous carcinoma.
Discussion
The overall utilization of the BI-RADS 3 assessment category at our center is appropriate with 3.4% of mammographic and ultrasound examinations in our study period assessed as BI-RADS 3 and a 1.7% cancer yield at 36 months. This is similar to previous retrospective studies of probably benign lesions with cancer yields ranging from .3% to 1.86%.2,3,5-7,14-16 The most significant finding in our study was the 37.5% rate of loss to follow-up. Loss to follow-up in our cohort was highest in the first 12 months with 86 of 517 women (16.6%) lost to follow-up within 90 days, 35 of 424 women (8.3%) at 6 months, and 32 of 304 women (10.5%) at 12 months. Early loss to follow-up is also documented in previous studies.14-17
Among women who were lost to follow-up in our cohort, compared to those who were not, there were significant differences for prior breast imaging, imaging indication, and breast density. Namely, women with prior breast imaging were less likely to be lost to follow-up than those without. It is possible that women who have regular breast imaging as part of the Ontario Breast Screening Program or who have previously had diagnostic breast imaging may be more compliant with short-interval follow-up. Women who underwent breast imaging for diagnostic evaluation of a breast symptom were also more likely to be lost to follow-up than those with imaging for additional evaluation following screening mammography. Women with a breast symptom may subjectively assess for stability of their lesion over time based on self-breast examination, and may not complete follow-up imaging if they determine it is unchanged or has resolved. This may also explain the high rate of loss to follow-up observed within 90 days in our cohort given that symptomatic breast pathologies (including abscess and hematoma, e.g.,) are usually followed at shorter intervals.
There was considerable use of the BI-RADS 3 assessment category in our cohort for non-validated findings with 92 of 569 lesions (16.2%) characterized by morphologic features other than those validated in prospective clinical studies.2-9 Among these, none were pathologically proven cancers. Although some flexibility in the BI-RADS 3 assessment category is necessary for its practical application, the lack of target benchmarks for its utilization contributes to excessive follow-up of benign findings (as in our cohort), unnecessary healthcare costs, and increased patient anxiety.12,18,19
There was significant redundancy in follow-up of BI-RADS 3 lesions in our cohort. The ACR currently recommends short-interval follow-up at 6 and 12 months from initial BI-RADS 3 assessment. 1 If the lesion remains stable at 12 months, the follow-up interval is usually lengthened to 12 months. However, an extra 6-month follow-up at 18 months remains common in practice. In our cohort, 78 of 211 women (37.0%) with lesions assessed as BI-RADS 3 at 12 months had additional follow-up at 18 months, yielding no cancers. After 2–3 years of stability, the ACR suggests changing the final assessment category to benign (BI-RADS 2) accompanied by a recommendation for routine mammographic screening.1,13 Among 517 women in our cohort, 53 (10.3%) and 24 (4.6%) underwent follow-up beyond 24 and 36 months, respectively. This follow-up yielded no cancers. All pathologically proven cancers were detected at 6 and 12 months, similar to previous studies.16,20 One of 6 cancers in our cohort could have been detected earlier had close attention been paid to its non-circumscribed margin, a commonly missed finding on ultrasound leading to delayed cancer diagnosis in a study by Song et al. 21
To address the high rate of loss to follow-up at our center, we have implemented a patient handout explaining the significance of the BI-RADS 3 assessment category and the importance of short-interval follow-up imaging. All women will also receive an automatic booking for their follow-up appointment on the date of their assessment. Previously, notifications were sent by mail. The efficacy of these interventions will be assessed in a future study.
Our study has several limitations beyond those inherent to its retrospective, single-center design. First, women who went to other centers for follow-up imaging were considered lost to follow-up. As such, non-compliance may be overestimated in our study. We also considered women with imaging downgraded to BI-RADS 1 or 2 before 24 months as cancer-free, including a significant number of women with imaging downgraded at or before 12 months. Most other studies required tissue diagnosis or 24-month imaging stability for inclusion in their analyses. According to the ACR guidelines, probably benign lesions that decrease in size or disappear at any follow-up interval may appropriately be downgraded to BI-RADS 1 or 2. 1 However, cancer yield may be underestimated in our cohort if lesions that remained stable in size were inappropriately downgraded before 24 months.
In conclusion, overall utilization of the BI-RADS 3 assessment category at our center is appropriate with 3.4% of mammographic and breast ultrasound examinations assessed as BI-RADS 3 and a 1.7% cancer yield. However, our study highlights a number of limitations of the BI-RADS 3 assessment category, including patient non-compliance with follow-up imaging, overuse of the assessment category for benign findings, and significant resource expenditure for a very low cancer yield. Our results support the need for a quality assurance tool specific to the BI-RADS 3 assessment category similar to target benchmarks set for screening recall rates. In addition, further research is needed to identify and address barriers to compliance with follow-up imaging. To that end, the efficacy of the interventions addressing non-compliance at our institution will be assessed in a future study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.