
Abstract
Emergency Radiology is a clinical practice and an academic discipline that has rapidly gained increasing global recognition among radiology and emergency/critical care departments and trauma services around the world. As with other subspecialties, Emergency Radiology practice has a unique scope and purpose and presents with its own unique challenges. There are several advantages of having a dedicated Emergency Radiology section, perhaps most important of which is the broad clinical skillset that Emergency Radiologists are known for. This multi-society paper, representing the views of Emergency Radiology societies in Canada and Europe, outlines several value-oriented contributions of Emergency Radiologists and briefly discusses the current state of Emergency Radiology as a subspecialty.
Introduction
Emergency Radiology has developed and established itself in recent years as an important radiological subspecialty. Its recognition as a distinct subspecialty and the availability of dedicated fellowship training programs continue to increase at a rapid pace. Since the first established Emergency Radiology fellowship in 1986, twenty-one Emergency Radiology fellowship programs now exist across the United States and Canada as of 2021. 1 The American Society of Emergency Radiology (ASER) was established in 1988, followed more recently by the European Society of Emergency Radiology (ESER), established in 2011, and the Canadian Emergency, Trauma, and Acute Care Radiology Society (CETARS), established in 2020.
The growth of Emergency Radiology and Emergency Medicine as a whole has occurred in concert in several ways. Prior to the advent of cross-sectional imaging, many patients in the Emergency Department (ED) would ultimately need to be admitted to hospital in order to have more invasive fluoroscopic and angiographic studies performed 2 that would not be feasible in the ED. Since the introduction of widely available around-the-clock access to ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) in many centres, significant positive outcomes have been realized in the ED, including but not limited to improvements in diagnostic confidence (and hence expediting appropriate referrals) 3 and reduction in lengths of hospital stay. 4
In the United States, the number of imaging investigations performed for each attendee has risen in the last 20 years, even allowing for an increase in the number of ED. For example, the use of CT per ED visit increased 153% from 2004 to 2016 with the use of non-cardiac ultrasound increasing by 134% over the same time period. 5 When considering the year-over-year increase in number of Emergency Department (ED) visits, 6 it is expected that the demand for diagnostic imaging of patients in the ED will continue to rise as well.
Ultimately, efficiency and timeliness are of crucial importance in the ED. This ethos is reflected in the layout of emergency departments across the world, as well as their staffing structure, informatics, workflow processes, and communication systems. As such, the role of the emergency radiologist must also adapt accordingly. This paper will review several ways in which Emergency Radiology adds value beyond imaging interpretation, by its integration with the Emergency Department and thereby contributing to high-quality patient care.
Subspecialty Expertise
The primary responsibility of an Emergency Radiologist is to be familiar with a wide variety of radiology modalities, imaging findings, and disease processes that may be seen in the emergency setting, while rapidly transitioning between different organ systems from head to toe. Emergency Radiologists have to be prepared for multiple challenges. Firstly, they need to be able to recognize emergent pathology in a fast paced and fast moving environment, often with frequent interruptions. The radiologist also has to be prepared for unpredictable imaging case volumes, meaning that a work shift is very different in the ED compared to routine outpatient reporting. Finally, subspecialty input on difficult cases from colleagues is much more difficult to obtain during afterhours coverage compared to daytime shifts.
Despite these challenges, emergency radiologists provide an indispensable service to the ED and deliver interpretations that must not only be accurate, as would be expected for all radiologists, but also timely. A landmark study from 2015 found that the use of CT in the ED, relying on the radiologist’s timely interpretations, altered the working diagnosis and substantially changed physician decision-making in over 50% of ED patients presenting with abdominal pain, and 42% and 24% in patients with chest pain/dyspnea and headache, respectively. 3 Another recent study from 2018 demonstrated that a fellowship-trained emergency radiologist’s secondary review of CT scans performed on patients in the ED from a community hospital, initially interpreted by a community radiologist, affected patient management in 16% of cases, emphasizing the significant value of additional expertise and familiarity with the imaging of acute disease processes. 7
Beyond interpretive expertise, there is also some intrinsic value to be gained from having dedicated emergency radiologists who are more accustomed to the needs and preferences of the ordering clinicians compared to rotating radiologists from other subspecialties. Emergency Radiologists also produce reports which are preferred by Emergency Physicians. 8 For example, a Thai study conducted in 2015 found that ordering clinicians preferred itemized structured reports over other formats in the emergency setting. 9 A more recent study from 2020 conducted in the United States identified several actionable recommendations regarding the radiology report from ED clinicians, respectively, such as stratification of urgent findings, report brevity, and clinical recommendations from the radiologist, among several others. 10 The advantages granted by having a dedicated section could enable more cohesive decision-making when choosing to address some of these previously identified areas of improvement.
Optimized After-Hours Coverage
As outlined in the Practice Parameter for Communication of Diagnostic Imaging Findings from The American College of Radiology, 11 timeliness is critical and is more important than the method of delivery, especially emphasized in any hospital operating with an Emergency Department. Timely radiology reports are expected on a 24-hour basis. Imaging delays have been shown in certain circumstances to be a significant contributor to increased lengths of stay in the ED. 12
Historically, several staffing solutions have existed to provide around-the-clock service. Teleradiology services are employed at many hospitals; however, they may be disadvantaged due to the remote nature of the service, introducing potential issues ensuring adequate communication, as well as technologic and regulatory limitations. 13 Outsourcing overnight coverage does provide the benefit of reducing strain on daytime scheduling, especially for small groups, and can permit simultaneous coverage of multiple sites if case volumes permit. For practice groups that assign their own radiologists for 24-hour coverage, oftentimes there is an insufficient number of subspecialty-trained emergency radiologists to cover all shifts except for a select few academic trauma centres. As such, radiologists in these groups are commonly enlisted from other sections of the department such as neuroradiology and musculoskeletal radiology to provide coverage. This raises the concern that a radiologist may not be comfortable interpreting certain emergency studies outside of their usual scope of practice, especially given the relative diversity of radiology subspecialties that exist and only further exacerbated by the disproportionate liability risk that radiologic studies performed in the ED pose. 14 In addition to these models, supplementary strategies that could make overnight coverage more tenable for the practice group include assigning radiologists shorter or less frequent shifts, providing monetary or time-based compensation for non-traditional schedules, 13 and integration of radiology resident coverage with faculty workflow during off-hours. 15 Staggering shift start times is a commonly adopted solution in Emergency Medicine 16 to reduce gaps in coverage and align workloads with anticipated case volumes for that shift based on historical data. This strategy is also seeing increasing rates of adoption among Emergency Radiology sections with associated improvements in timeliness in reporting. 17
Dedicated emergency radiologists provide the diagnostic accuracy that comes with subspecialization 7 and expect to work after-hours. A group composed of such radiologists can not only ensure rapid turnaround times but also provide accurate interpretations on a wide breadth of pathology across several modalities and body parts. Full-time involvement and integration with the emergency and trauma departments would be necessary to ensure consistency across its member radiologists in addition to other benefits for the department as a whole. Given the advancement of virtual technology, radiologists could either work on-site or remotely. Regardless of practice setting, it would be important to foster consistent and predictable service among all its members predicated on their expertise in Emergency Radiology for such a section to warrant its existence. It cannot be emphasized enough that the viability of an Emergency/Trauma Radiology section with reduction of physician burnout relies on proper integration with emergency and trauma clinical departments where everyone feels that they are part of a team-based approach that together contributes to optimized patient-centred care.
Optimized Imaging Protocols
Balancing the combined workloads of choosing the correct imaging protocol, coordinating with technologists to expedite imaging, timely interpretation, and communication of urgent findings are key in ED imaging. Optimizing protocols are necessary to streamline this workflow. Developing such protocols and becoming familiar with them are crucial for both emergency radiologists and radiologic technologists alike to maximize workflow efficiency and ensure patient safety by reducing errors. 18
Summary of time/diagnostic precision (Variant A) and dose-optimized (Variant B) protocols for whole-body computed tomography in polytrauma patients. Adapted from the ‘European Society of Emergency Radiology: guideline on radiological polytrauma imaging and service (short version)’ by Wirth, S., Hebebrand, J., Basilico, R. et al, 2020, Insights Imaging, 11, 135. https://doi.org/10.1186/s13244-020-00947-7.
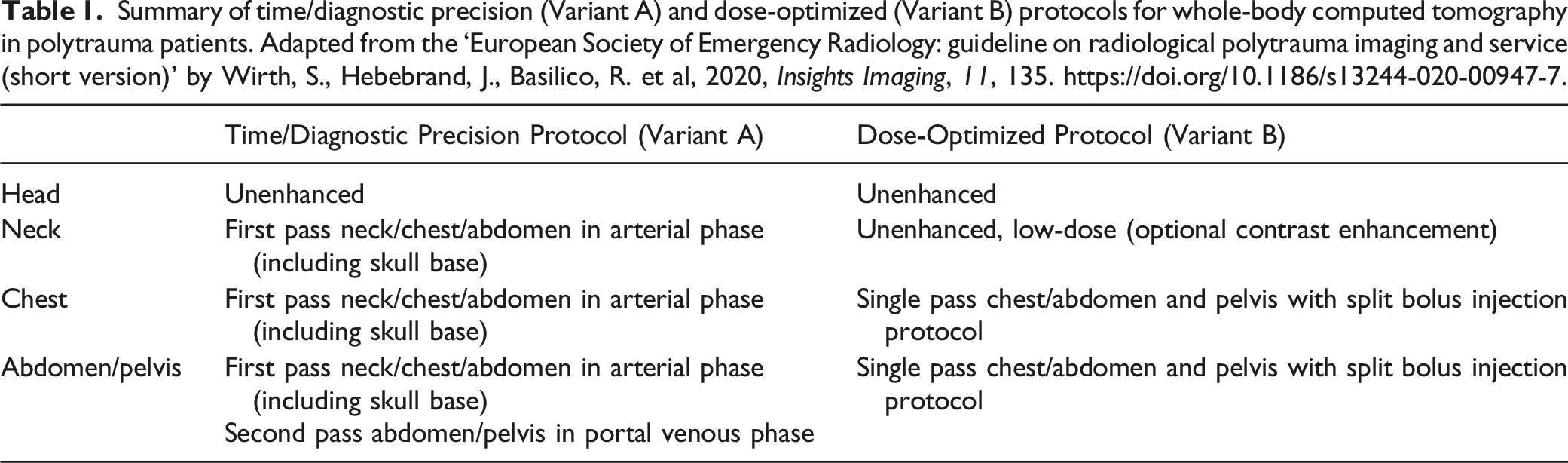
Another instance of the importance of ensuring immediate familiarity with a standard imaging protocol is in the setting of acute stroke care. The management of acute ischaemic stroke is extremely time sensitive. With recent breakthroughs in the role of endovascular therapy within extended time windows,26,27 ED-specific protocols must also follow suit and adapt to the current guidelines. As with polytrauma patients, variation between institutions exists; however, evidence-based guidelines assist in informing timely physician decision-making regarding appropriate therapeutic measures. Both CT and MRI for evaluation and characterization of stroke as well for vascular imaging have been validated for the initial imaging evaluation of patients 28 and used at different frequencies at different institutions depending on local availability. Post-processing of angiographic images as well as CT and MR-based perfusion imaging has also been adopted by many institutions to guide possible endovascular therapy, 28 also dependent on local availability and level of expertise. Stroke imaging is another leading example of the ever-changing landscape of Emergency Radiology and how optimizing imaging protocols and keeping them up to date are of utmost importance in improving care delivery.
While other subspecialized and general radiologists would likely be able to aid in the development of such protocols, it would be difficult to standardize this role across all radiologic subspecialties without the cohesiveness that a dedicated section for Emergency Radiology would offer. Having a dedicated section familiar with the development and implementation of optimized protocols commonly used in the ED essentially creates a one-stop-shop resource that can ensure patients are evaluated with the most modern and appropriate imaging test. From a workflow perspective, the radiologic technologists as well as the emergency physicians also have a more consistent point of contact to discuss appropriate testing and imaging protocols, avoiding any wasted time in tracking down multiple individuals for studies of different organ systems (sometimes ordered in the same patient).
Clinical Decision Support Systems
Clinical decision support (CDS) systems are information systems designed to inform clinicians and provide recommendations on a variety of clinical needs, including within the ED. Tangible benefits have been observed following implementation of CDS systems in the ED, including efficiency improvements in clinical management and better patient outcomes. 29 CDS systems with respect to imaging are based on the implementation of Appropriate Use Criteria collected and summarized from multiple societies and their respective guidelines, such as the American College of Radiology Appropriateness Criteria and the American College of Cardiology.30,31 Their purpose is to inform the appropriateness of imaging and guide the appropriate protocol/modality. Given widespread concern for the inappropriate use of imaging, specifically the associated cost to the health-care system but also unnecessary exposure to ionizing radiation,32,33 recent years have seen a growing trend in the implementation of clinical decision support systems both within and outside radiology. 34 Such systems range from manual aids to computer-based feedback when an electronic medical record system is available. Several studies have demonstrated decreases in inappropriate imaging tests after the implementation of clinical decision support systems, such as the utilization of lumbar spine MRI for low back pain, 35 as well as simultaneous increases in appropriate imaging tests. 36
Although appropriate use criteria exist for many common clinical presentations, they have not been established for many less commonly encountered or more complex clinical presentations in the ED. The development and validation of such criteria would require a collaborative effort between radiologists, clinicians, and technologists. Dedicated emergency radiologists would provide important feedback in this effort given their exposure to a high volume of relevant cases. The close working relationship emergency radiologists have with their emergency medicine colleagues helps to facilitate this multidisciplinary collaboration.
Mass Casualty Incidents
A mass casualty incident (MCI) is defined by the World Health Organization (WHO) as an event which generates more patients than can be managed using routine procedure given locally available resources, necessitating exceptional emergency arrangements. 37 In mass casualty management, the overarching goal shifts to providing the greatest good for the greater number of victims 38 due to the inevitable bottlenecks and delays in downstream care delivery that will occur given the overwhelming number of patients. As the ED is at the front lines of disaster response, preparedness is essential in being able to adapt quickly and appropriately. 39
Radiology-specific disaster plans are no exception to the rule of preparedness. Several challenges exist when formulating a plan for preparedness, which must take into consideration the plan for the rest of the hospital to be executed successfully. 40 For example, over-triaging and under-triaging are well-documented pitfalls during mass casualty management, using up valuable hospital resources in times of strife or delaying care for potentially life-threatening injuries, respectively. 41 Expedited imaging can facilitate more accurate triaging, including measures to temporarily increase throughput by calling in additional staff and/or commissioning additional equipment where available. This also involves optimizing imaging protocols and streamlining communication between clinicians, radiologists, technologists, and other support staff to minimize the risk of additional bottlenecks. Delays in transfer of images from the CT scanner to the radiologists’ workstations can be mitigated by formalizing a process in which preliminary interpretations provided directly at the console are immediately available for clinician review. 42 Analogous to emergency physicians being the core of preparedness plans for the hospital because of the nature of their day-to-day activities, 39 emergency radiologists would be best suited to spearhead such MCI preparedness initiatives for the radiology department as a whole.
A recent example of the response of emergency radiology in mass casualty management is the Coronavirus Disease 2019 (COVID-19), first identified in December 2019 43 and since spread worldwide leading to an ongoing global pandemic, which continues to place heavy burdens on medical resources across the world. Emergency departments globally were forced to adopt new operational measures to adjust for changes in staff workflow, patient triage, and emergency imaging during the pandemic. Emergency radiologists played a major role in developing and implementing departmental changes ensuring that adequate efforts towards containing the spread of the virus were balanced with the ongoing provision of high-quality care to patients with non-COVID-19 conditions. A consensus statement led by emergency radiologists from the Canadian Association of Radiologists in 2020 44 outlined multiple recommendations for emergency radiologists to aid in optimizing care delivery in the ED, such as initial imaging of suspected or confirmed COVID-19 cases, imaging for non-COVID-19 indications, and infection control measures.
Future Growth of Emergency Radiology
Given that department expansion and equipment renewal are often driven by the needs of the Emergency Department, a dedicated Emergency Radiology section can better promote the development and growth of a radiology department, due to the greater degree of dedication of the constituent radiologists towards the success of the section and relationship with the ED. As the demand for imaging in the ED increases, it is essential that radiology coverage of the ED remains flexible to adjust for both the steady increase in volume as well as day-to-day fluctuations in number of cases. Many centres whose ED is covered by local radiologists tend to subdivide after-hours duties into a distinct evening and overnight shifts, occasionally with overlap to cover the busiest portions of the evening. Indeed, it has been shown that fatigue from extended-hour shifts or from consecutive night shifts contributes to errors not only for trainees but also attending radiologists. 45 Having long-term radiologists committed to the section can help minimize scheduling conflicts and ensure equitable division of labor amongst the subspecialty group, compared to radiologists from other subspecialties who have their own separate daytime schedules to contend with as well. Further, a flexible approach with the Emergency Radiologist and patient being in different time zones can overcome the inherent problem of unsociable shifts leading to sleep deprivation-associated errors, 46 enabling the radiologist to be working in their own daytime, while delivering prompt and accurate care to a patient seen on the overnight shift in their own home country. 47
Any other potential improvements to the department mostly stem from the shared goal of optimizing patient care delivery among radiologists and non-radiologists alike, as well as optimizing radiologist workflow and efficiency. Many hospitals have installed CT scanners physically located in the ED itself to reduce delays in imaging caused by patients’ transfers. In many cases, this initiative is driven by an Emergency Radiology section. A study from Canada in 2015 found decreases in time of between 15 and 19 minutes in institutions with ED CT scanners compared to those without one, and in turn decreases in radiology report turnaround time. 48
Additionally, it is vital that emergency radiologists use their subspecialty expertise to provide high-quality resident and fellow education, which is especially apparent with the growing number of emergency radiology fellowships across North America. As Emergency Radiology continues to carve its own niche among other radiology subspecialties given the unique skillset it demands, it is only logical that the educational requirements in Emergency Radiology fellowships must be scrutinized carefully and upheld to certain standards as they have been for other subspecialty fellowships. A survey in 2018 conducted on program directors for Emergency Radiology fellowship programs throughout North America showed agreement in several educational goals that should be made standard to homogenize training requirements, including both interpretive and non-interpretive skills. 49
Instructing radiology residents earlier in training will incentivize more trainees to pursue a career dedicated to Emergency Radiology, fostering global recognition as a subspecialty. A recent study from the United States in 2018 highlighted that more exposure to Emergency Radiology during residency allowed residents to become more familiar with the nature of Emergency Radiology training, potential career opportunities, and adopt a more favourable perception of the field as a whole. 50 Of note, ESER has developed a Curriculum for Subspecialization in Emergency Radiology and a European Diploma in Emergency Radiology (EDER) in order to offer a general proof of qualification. 51 The advent of multiple Emergency Radiology societies in recent decades as well as the year-to-year growth of the Emergency Radiology journal are key milestones highlighting the importance of scholarly contributions towards the continued development of the field.
Conclusion
Emergency Radiology is a rapidly growing subspecialty which is here to stay. The advantages of having a dedicated Emergency Radiology section with full-time emergency radiologists include interpretive expertise, staffing advantages to establish around-the-clock coverage, familiarity with emergency imaging protocols and clinical decision support services, mass casualty preparedness, and the promotion of the growth of the field as a whole. The nuanced nature of its organizational and operational structure and the skillset required to provide a high-quality service together serve to legitimize Emergency Radiology as a distinct subspecialty with distinct value.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.