
Abstract
Purpose:
In Canada, ultrasonography is the primary imaging modality for children with suspected appendicitis, yet equivocal studies are common. Magnetic resonance imaging provides promise as an adjunct imaging strategy. The primary objective of this study was to determine the proportion of children with suspected appendicitis and equivocal ultrasound where magnetic resonance imaging determined a diagnosis.
Methods:
A prospective consecutive cohort of children aged 5-17 years presenting to a tertiary pediatric Emergency Department with suspected appendicitis were enrolled. Participants underwent diagnostic and management strategies according to our local suspected appendicitis pathway, followed by magnetic resonance (Siemens Avanto 1.5 Tesla) imaging. Sub-specialty pediatric radiologists reported all images.
Results:
Magnetic resonance imaging was performed in 101 children with suspected appendicitis. The mean age was 11.9 (SD 3.4) years and median Pediatric Appendicitis Score was 6 [IQR 4,8]. Ultrasonography was completed in 98/101 (97.0%). Of 53/98 (54.1%) with equivocal ultrasound, magnetic resonance imaging provided further diagnostic information in 41 (77.4%; 10 positive, 31 negative; 12 remained equivocal). Secondary findings of appendicitis on magnetic resonance imaging in children with equivocal ultrasound included abdominal free fluid (24, 45.3%), peri-appendiceal fluid (12, 22.6%), intraluminal appendiceal fluid (9, 17.0%), fat stranding (8, 15.1%), appendicolith (2, 3.8%), and peri-appendiceal abscess (1, 1.9%). The observed agreement between magnetic resonance imaging results and final diagnosis was 94.9% (kappa = 0.89).
Introduction
Appendicitis is the most common surgical emergency for pediatric patients. 1 High rates of morbidity are observed in children with appendicitis due to their difficulty with expressing symptoms 2 and delays in seeking medical care. 3 Furthermore, the “classic” signs of appendicitis are not always observed in children. 2,4 Accurate, timely diagnosis for children with suspected appendicitis mitigates the risk of adverse outcomes (e.g., appendix perforation, unnecessary surgery). Ultrasonography (US) is the first-line imaging modality utilized across pediatric emergency departments (EDs) in Canada, 5 yet its accuracy is operator- and patient- dependent 6,7 Recent literature has demonstrated that between 53-69% of US studies do not completely visualize the appendix, and 62-74% are inconclusive. 6,8 -10
Computed tomography (CT) is an alternative imaging modality, demonstrating exceptional diagnostic value in appendicitis, yet concern related to radiation on developing pediatric organs limits its routine use. 11 -13 For suspected appendicitis in children, CT has excellent sensitivity and specificity rates of 95% (95% CI: 92-97%) and 92% (95% CI: 90-94%), respectively, which are slightly higher with contrast administration than without. 14 However, pediatric CT has been associated with an increased risk of leukemia and brain tumors. 15,16 It is likely because of these concerns that pediatric CT imaging for appendicitis in the United States declined by 48% from 2010-2013, 17 and its use in Canada is exceptionally low. 5
Magnetic resonance imaging (MRI) lacks ionizing radiation, can be performed without contrast, and offers high soft-tissue contrast resolution, 18 providing multiplanar images with excellent anatomical detail of the abdomen and right lower quadrant. In cases of incomplete appendiceal visualization, the absence of secondary signs of appendicitis may help exclude acute appendicitis. High respective sensitivity and specificity rates of 98% (95% CI: 96-99%) and 97% (95% CI: 96-98%) have been reported with MRI for suspected appendicitis (N = 990) in children (14). In a meta-analysis of 11 studies (N = 1,698), MRI had a positive-predictive value of 92% (95% CI: 89.3-94%) and a negative predictive value of 98.3% (95% CI: 97.3-99%) for pediatric appendicitis. 19 Disadvantages of MRI relate to its high cost, potential need for anesthesia or sedation (e.g., anxious or young patients), lengthy scanning times, and limited availability of MRI equipment and after-hours technicians. However, increases in the availability and accessibility of MRI, faster effective sequencing techniques, and diagnostic accuracy could improve its use. 20,21 Although MRI has been offered as an optimal secondary imaging modality following equivocal US 14,18,22,23 and considered a viable primary imaging modality in locations with 24-hour access, 24 it is infrequently utilized for pediatric appendicitis in Canada. 5
The primary purpose of this study was to identify the proportion of children with initial equivocal US studies in whom MRI determined a positive or negative result. The secondary aims were to determine agreement between MRI results and pathologically determined final diagnosis and describe common MRI findings of appendicitis present in children with equivocal US. To our knowledge, this is the first study in Canada aimed to observe the diagnostic efficacy of MRI in pediatric suspected appendicitis.
Methods
Study Design and Setting
We conducted a prospective single-center cohort study evaluating ED diagnostics in pediatric suspected appendicitis from November 1 2013 to December 31 2014. This study was completed at the Alberta Children’s Hospital, which provides tertiary pediatric care for southern Alberta, eastern British Columbia, and western Saskatchewan; the annual ED census is approximately 77,000. We obtained study approval through the Conjoint Health Research Ethics Board of the University of Calgary (REB13-0586), and informed consent and assent (for children ≥ 7 years), before initiating study procedures. Participants did not receive remuneration for their participation.
Study Population
Children aged 5-17 years presenting to the ED from 0800-1700 from Monday-Friday with abdominal pain were screened for eligibility. Individuals with suspected appendicitis qualified for inclusion, defined as having a clinically indicated US of the appendix or a surgical consult for appendicitis. Children with a known diagnosis of appendicitis (i.e., transferred to our ED with confirmed appendicitis on US), previous appendectomy or major abdominal surgery, abdominal pain for greater than 5 days, previous enrollment in the study, expectation to require pediatric intensive care, known pregnancy, immunosuppression, or inability to consent due to a language barrier were excluded.
Study Process
We recorded demographic, medical history, course in hospital, laboratory and imaging results, and Pediatric Appendicitis Score (PAS) data (Supplementary Table 1). 25 Children received MRI within 4 hours of informed consent and assent, before or after US. No research related medications (e.g., procedural sedation or diagnostic contrast) were administered, although clinically indicated analgesia was provided at the clinical team’s discretion. Study MRI images were stored on an institutional data server for future interpretation; results were not provided to the clinical team as MRI was not standard of care at our institution for suspected appendicitis. The clinical team performed the remainder of care, according to the institutional appendicitis care pathway.
US Processes
US studies were ordered at the clinical physician’s discretion, completed by trained pediatric sonographers (minimum of two years of experience) and reported by the sub-specialty pediatric clinical radiologist (blind to MRI results) according to clinical standards. Equivocal studies included cases where the appendix was not completely visualized or evidence on the report indicated an inability to conclusively call the study positive or negative.
MRI Processes
MRI studies were performed with a 1.5-Tesla Scanner (Siemens Avanto; Erlangen, Germany) using limited sequences without oral or intravenous contrast administration. Axial and coronal T2HASTE (Half Fourier Acquisition Single Shot Turbo Spin Echo) sequences provided rapid acquisition of images while decreasing motion artifacts. Steady-state free precession [True FISP] and axial diffusion-weighted sequences were employed; a consistent protocol was used across all participants. A sub-specialist pediatric radiologist with a minimum of two years MRI reporting, blinded to clinical information and US results, reported and classified MRI results in the following pragmatic categories: a) No Appendicitis, b) Acute Appendicitis, or c) Equivocal for Appendicitis (i.e. incomplete visualization, borderline diameter).
Secondary Signs of Appendicitis
Radiologists may increase their diagnostic acumen by observing for peri-appendicular signs of inflammation associated with, but not diagnostically conclusive of, appendicitis. 26 Examples of secondary signs of appendicitis included in the study MRI reports were fluid collections, free fluid, appendicoliths, and fat stranding.
Final Diagnosis
A clinical pathologist provided pathology reports on performed appendectomies, and an independent pathologist, blinded to the clinical history and imaging results, subsequently reviewed reports and classified the appendix as no appendicitis, acute appendicitis, or perforated appendicitis based on local standards. Health records were reviewed for 7 days following the index ED encounter to screen for repeat ED visits. A child with no evidence of a) appendectomy, b) non-operative management of appendicitis, or c) percutaneous drain for appendiceal abscess was classified as no appendicitis. Acute appendicitis and perforated appendicitis were grouped together for the purposes of this analysis.
Statistical Analysis
Data were analyzed with STATA 15.1 (StataCorp, College Station Tx). Descriptive and summary statistics (sensitivity, specificity, negative- and positive-predictive values) were calculated, and a chi-squared analysis determined differences in MRI efficacy between sexes. Cohen’s kappa was calculated to determine the observed agreement between MRI results and pathology reports.
Results
Patient Characteristics and Outcomes
Out of 453 children screened with abdominal pain, 369 met eligibility criteria, and 140 were enrolled in the study. MRI was performed on 101/140 children; none were excluded due to situational or technical concerns, such as claustrophobia or difficulty remaining still. The 39 excluded children were discharged home or sent to the operating room before study imaging. Figure 1 outlines the study participant screening, enrollment, and exclusions.
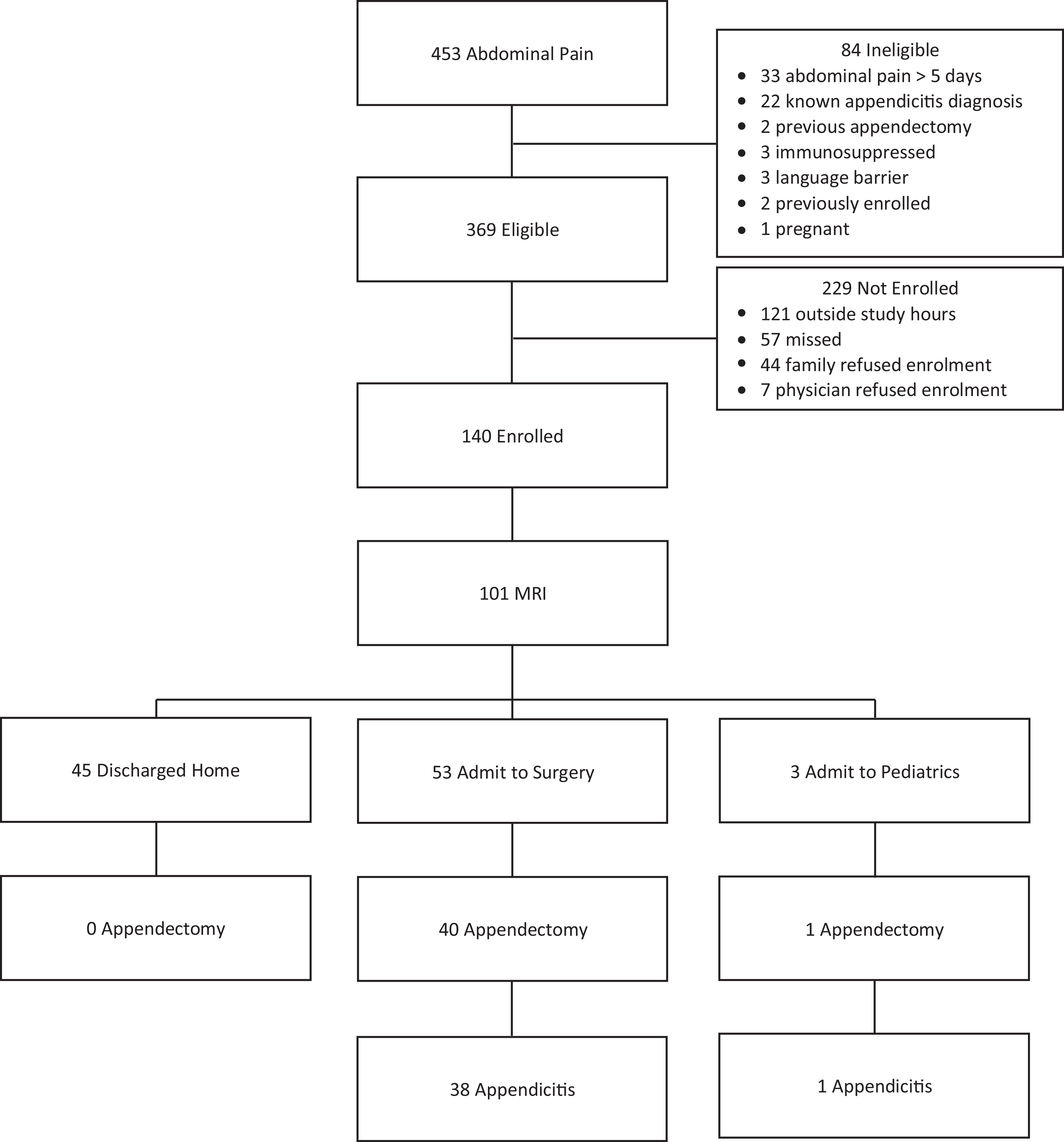
Study screening and enrolment of children with suspected appendicitis.
In patients undergoing MRI, the average age was 11.9 (SD 3.4) years, and 57 (56.4%) were female. The median PAS was 6 [IQR 4,8]. US was performed in 98/101 (97.0%) children, and 53 (54.1%) were equivocal. Thirty-two (60.4%) children with equivocal US were discharged home, and although 5 returned to care within 7 days of enrollment, none were diagnosed with appendicitis. Conversely, 8 (15.1%) children with equivocal US underwent appendectomy and 7 (87.5%) had pathology proven appendicitis. An additional 13 (24.5%) children were admitted to the hospital and discharged home with alternative diagnoses after observation. In total, 41 (40.6%) patients underwent an appendectomy, and 39 (38.6%) were diagnosed with appendicitis, resulting in a negative appendectomy rate of 4.9% (2/41). Three participants had MRI findings of ovarian cyst (<5 cm) and were discharged home. Table 1 outlines the participant characteristics. Select images from study participants are found in Figures 2 -4.
Characteristics of Study Participants With Suspected Appendicitis Undergoing Magnetic Resonance Imaging.
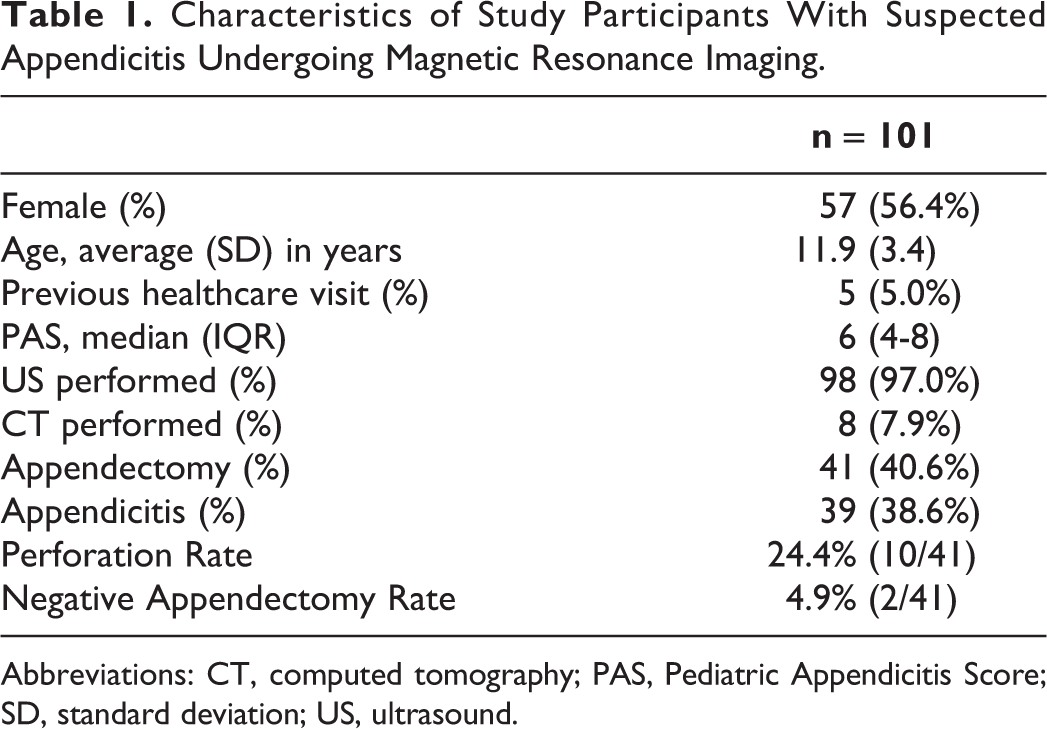
Abbreviations: CT, computed tomography; PAS, Pediatric Appendicitis Score; SD, standard deviation; US, ultrasound.
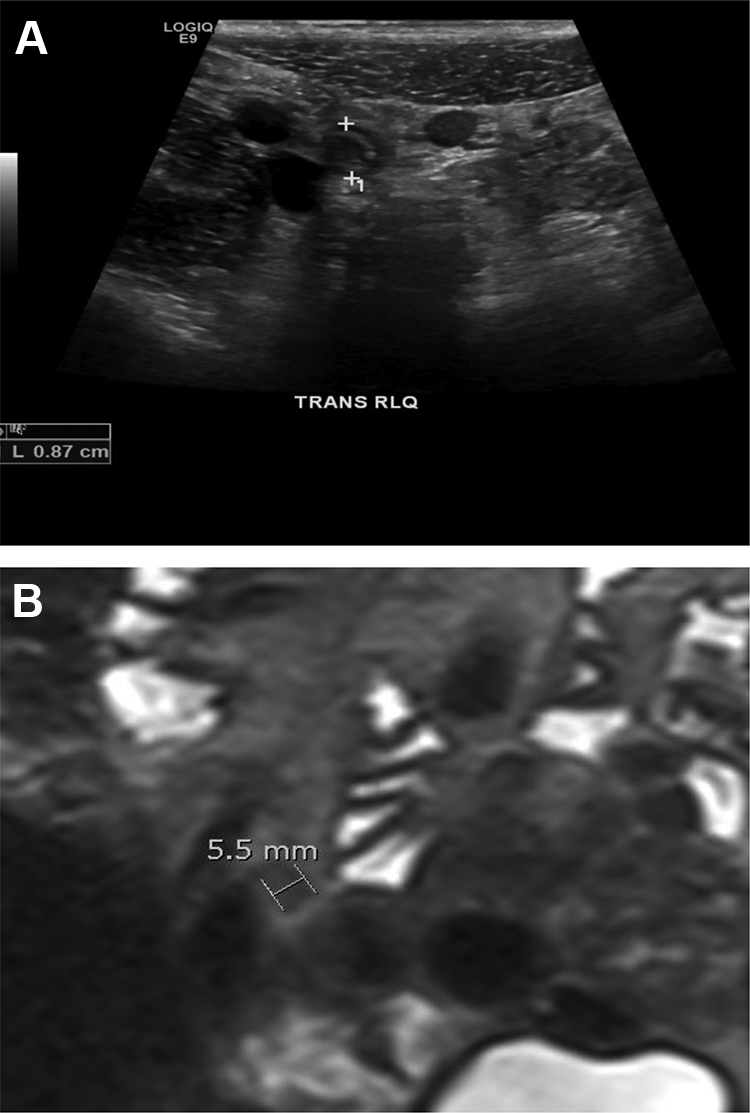
Images of a false negative MRI. A, Ultrasound image demonstrating a dilated appendix measuring 0.87 cm with surrounding echogenic fat. B, Magnetic resonance image (MRI) demonstrating an apparent normal appearance to appendix (0.55 cm).
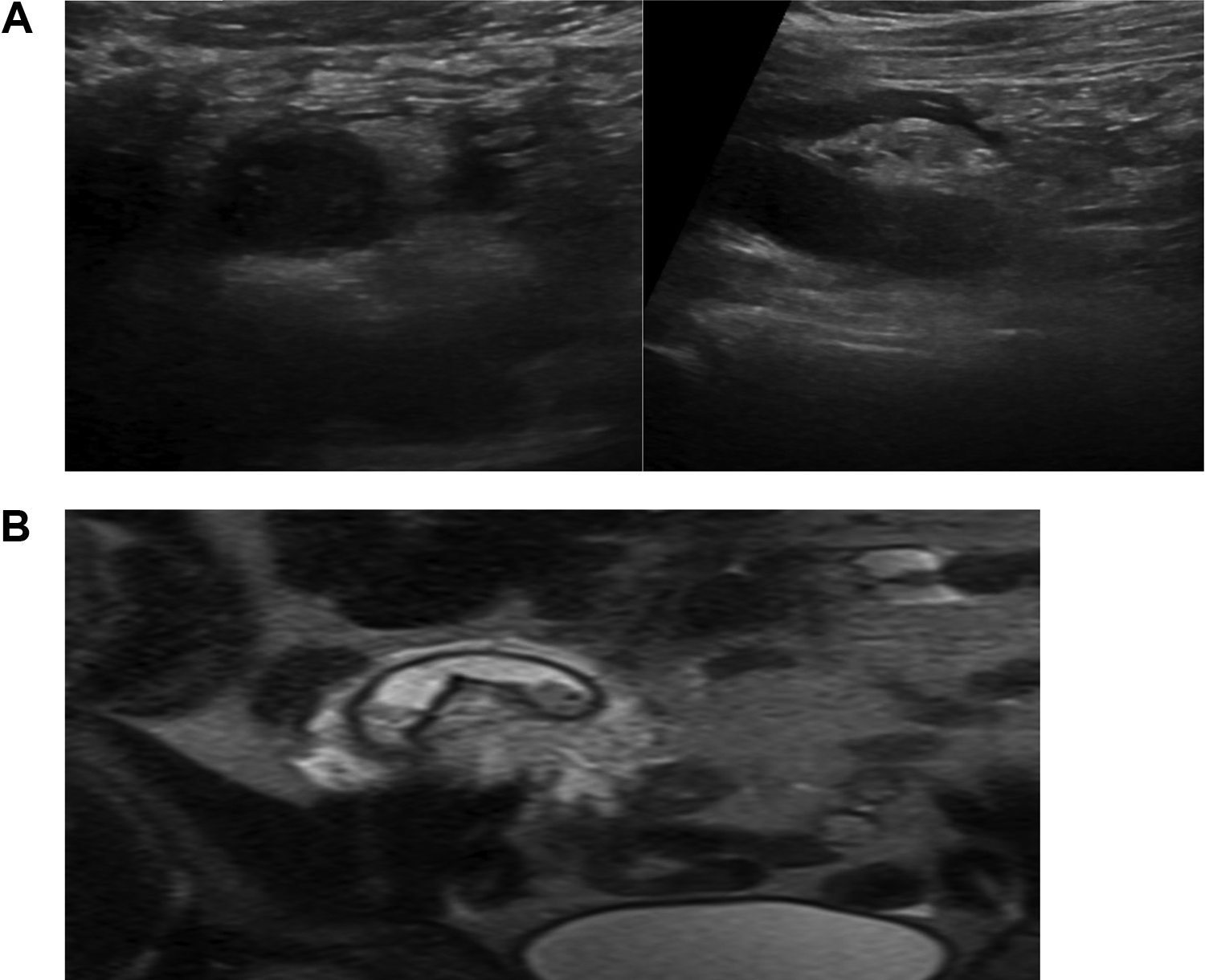
Images of acute appendicitis. A, Ultrasound images of dilated appendix surrounded by echogenic fat. B, Magnetic resonance image of a dilated appendix with echogenic fat surrounded by a small amount of free fluid.
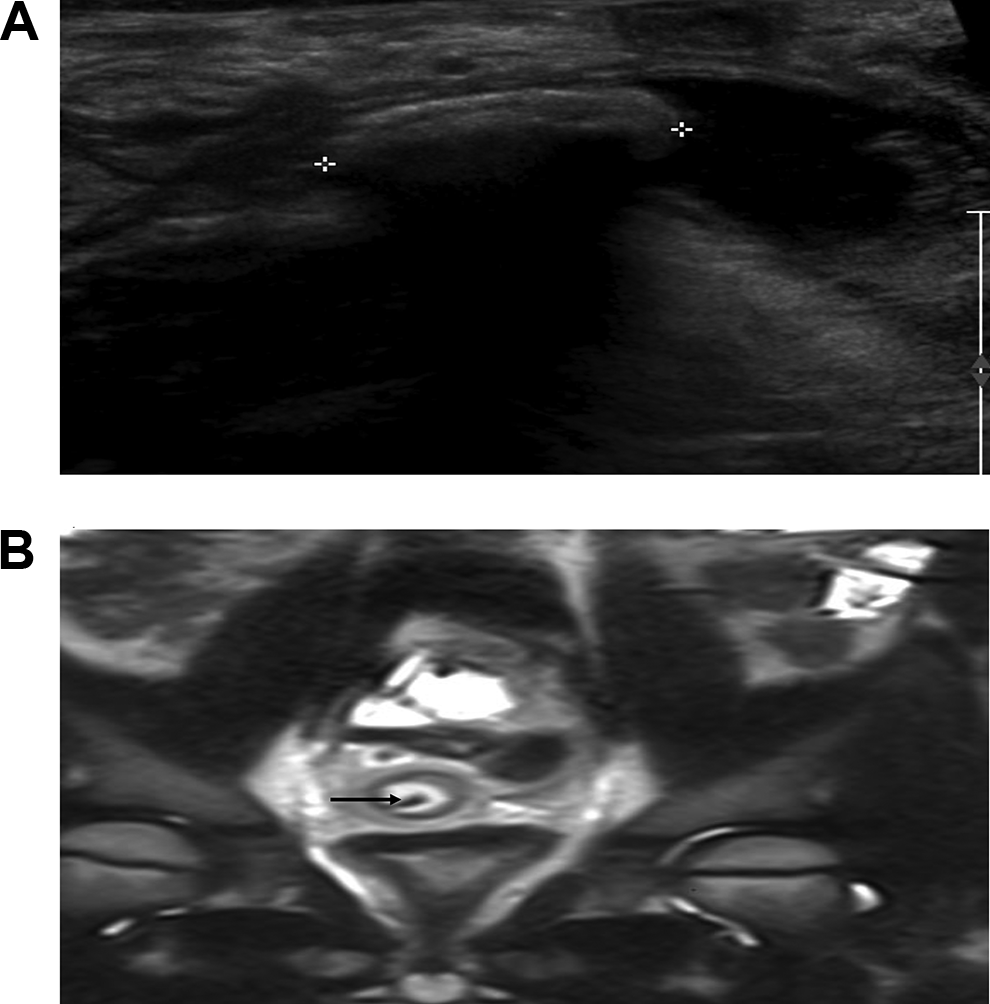
Images of a dilated appendix with appendicolith. A, Ultrasound image demonstrating an appendicolith (outlined by calipers). There is echogenic fat around the appendix. B, Magnetic resonance image demonstrating an appendicolith (arrow) inside the lumen of the appendix which is surrounded by echogenic fat.
Performance of MRI in Equivocal US
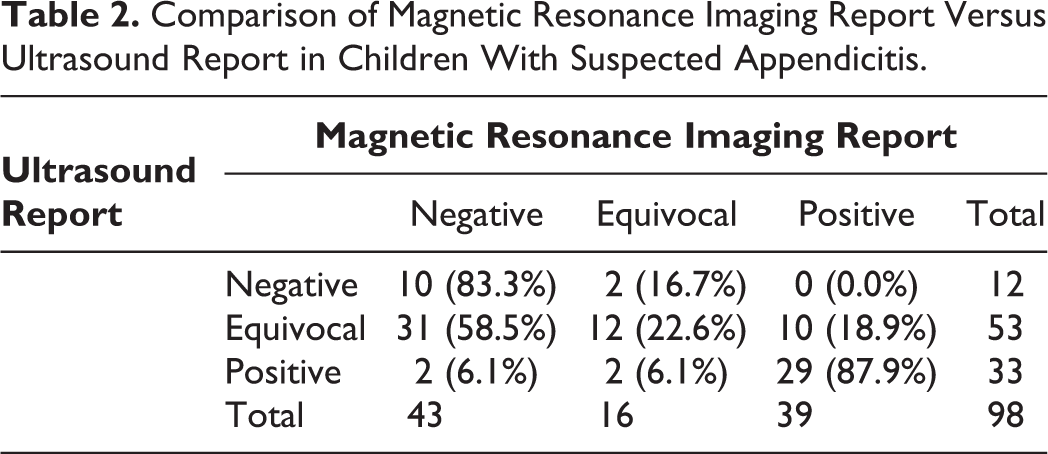
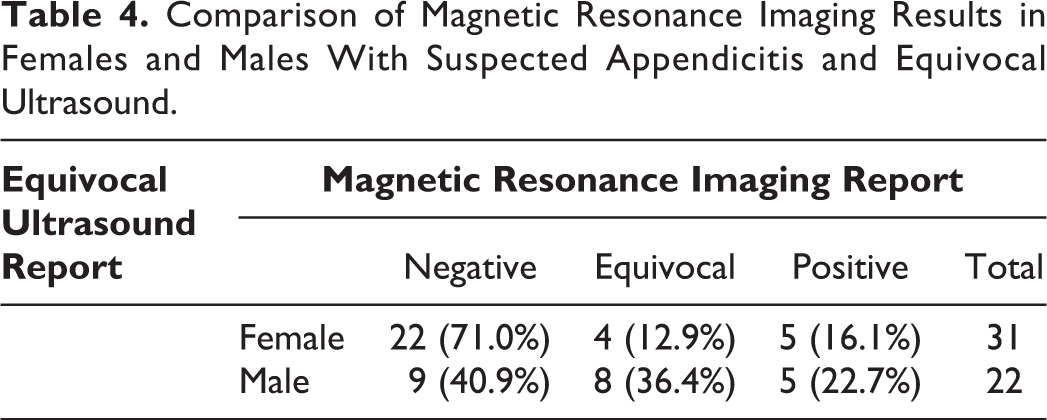
Of the 53 patients with equivocal US, MRI provided diagnostic information in 41 (77.4%); 31 (58.5%) were reported as negative, 10 (18.9%) as positive, and 12 (22.6%) were again reported as equivocal. Diagnostic information provided by MRI was more apparent in females than males (27/31 (87.1%) vs 14/22 (63.6%); P = .04). No children with a) equivocal US and negative MRI (n = 31) or b) equivocal US and equivocal MRI (n = 12) had a final diagnosis of appendicitis; 7/10 (70.0%) children with equivocal US and positive MRI had pathology proven appendicitis. Tables 2 & 3 compare MRI to US reports, and Table 4 outlines differences in MRI impression based on sex.
Comparison of Magnetic Resonance Imaging Report Versus Ultrasound Report in Children With Suspected Appendicitis.
Final Diagnoses in Children With Suspected Appendicitis, Based on Ultrasound and Magnetic Resonance Imaging Results.
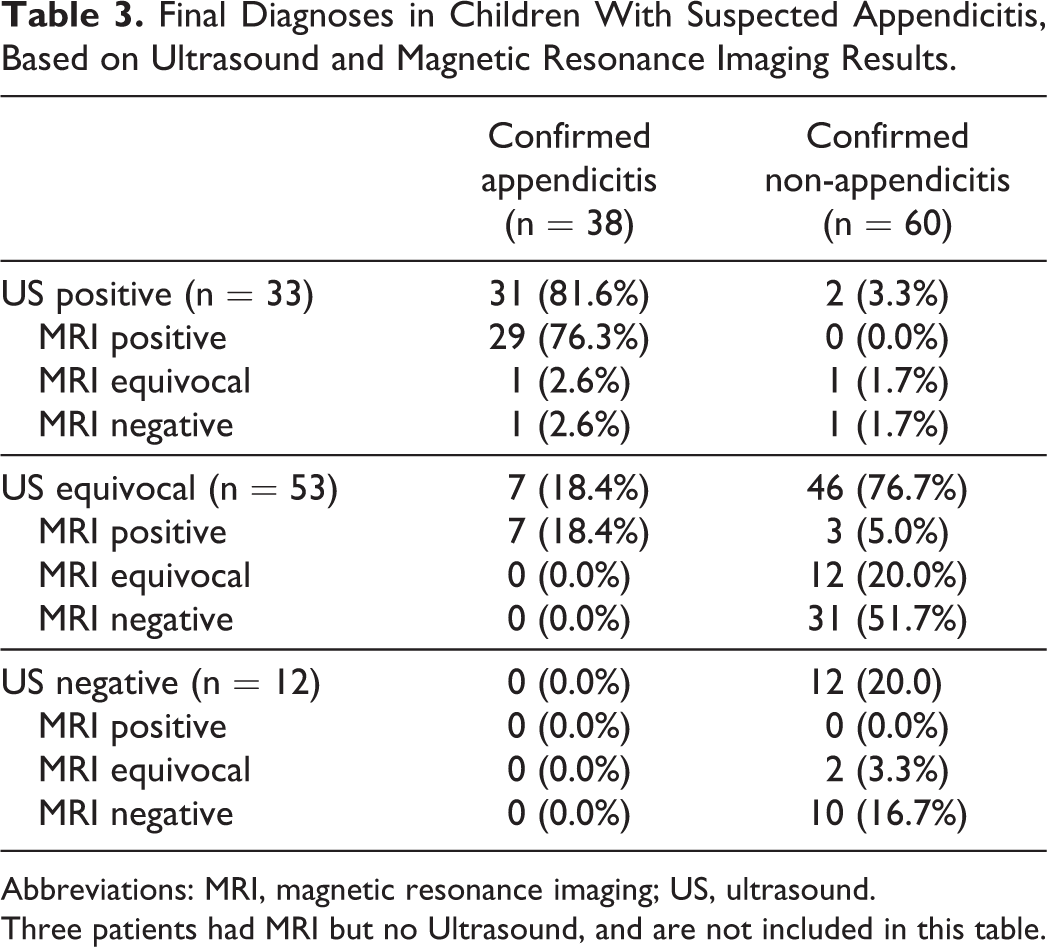
Abbreviations: MRI, magnetic resonance imaging; US, ultrasound.
Three patients had MRI but no Ultrasound, and are not included in this table.
Comparison of Magnetic Resonance Imaging Results in Females and Males With Suspected Appendicitis and Equivocal Ultrasound.
MRI vs Final Diagnosis
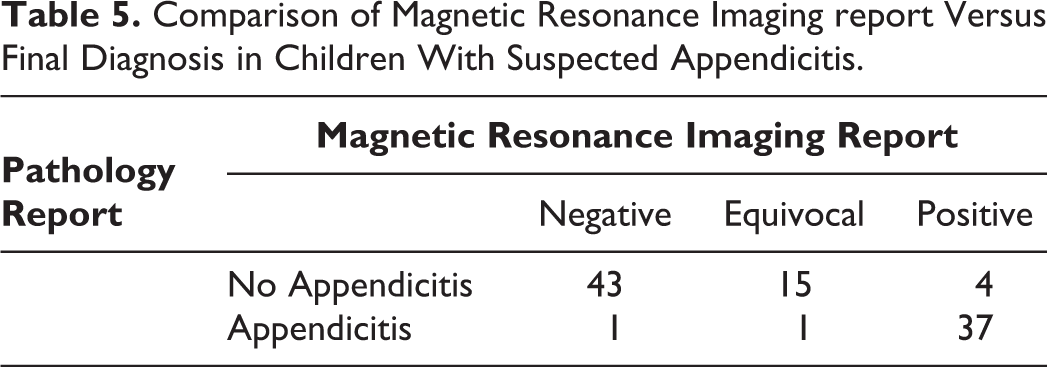
Pathology-proven appendicitis was diagnosed in 37/101 (36.6%) children who underwent MRI. When grouping equivocal MRI reports as negative, the sensitivity, specificity, positive- and negative-predictive values for MRI were 94.9% (95% CI: 82.7-99.4%), 93.5% (84.3-98.2%), 90.2% (76.9-97.3%), 96.7% (88.8-99.7%); the observed agreement was 94.9% (kappa = 0.89). Table 5 compares MRI report with final diagnosis. In comparison, the sensitivity, specificity, positive- and negative-predictive values for US (grouping equivocal US as negative) were 81.6% (65.7-92.3%), 96.7% (88.5-99.6%), 93.9% (79.8-99.3%) and 89.2% (79.1-95.6%), with an observed agreement of 90.8% (kappa = 0.80).
Comparison of Magnetic Resonance Imaging report Versus Final Diagnosis in Children With Suspected Appendicitis.
Out of 4 false-positive MRI reports, three had an equivocal US, and one did not undergo US. Two children with false-positive MRI reports were discharged from the ED based on clinical exam, returned for further assessment, and were again discharged home. The surgical team discharged the other 2 after a brief hospital observation and neither returned to care.
There was 1 false-negative and 1 equivocal MRI result in 2 children with positive US and pathology confirmed appendicitis. The false-negative MRI report occurred in a 14-year-old boy with a PAS of 3, white blood cell count of 6.6 × 109/L, neutrophil count of 2.9 × 109/L, and C-reactive protein of 32 mg/L. His US results showed an 8.7 mm appendix, while the MRI reported a 5.5 mm appendix with no secondary signs of inflammation (Figure 2). The equivocal MRI report occurred in an 11-year-old boy with no available laboratory investigations. His US results showed a 10 mm appendix, while the MRI reported a 7.2 mm appendix and mild peri-appendicular fluid. Both children underwent appendectomy and recovered without incident.
Secondary MRI Findings
In the setting of equivocal US, MRI provided additional information suggestive, but not specific of or diagnostic for appendicitis. These findings included the presence of peri-appendicular fluid (12, 22.6%), intra-luminal fluid (9, 17.0%), fat stranding (8, 15.1%), appendicolith (2, 3.8%), abscess (1, 1.9%), free fluid (24, 45.3%), and trace free fluid (10, 18.9%). The positive- and negative- predictive values of at least 1 secondary sign of appendicitis on MRI were 53.4% (95% CI: 41.4-65.2%) and 100% (95% CI: 87.7-100.0%).
Discussion
In Canadian pediatric hospitals, US is the most commonly utilized diagnostic imaging technique to diagnose appendicitis. 5 Despite its advantages, US faces limitations because more than half of US studies are deemed inconclusive, often due to incomplete visualization of the appendix, 9,26 -28 Equivocal US studies can result in detrimental patient outcomes due to delayed diagnosis and treatment of appendicitis or unnecessary surgical interventions. Additional tools are needed to improve the care of Canadian children presenting to the ED with abdominal pain by assisting clinicians in quickly and reliably identifying pediatric appendicitis.
To our knowledge, our prospective cohort study is the first in Canada to demonstrate that MRI can improve diagnostic certainty in pediatric ED patients with suspected appendicitis and an equivocal ultrasound. In 53 cases where US was equivocal, MRI provided additional diagnostic information in 41 (77.4%). Furthermore, in equivocal US cases, secondary MRI findings suggestive of appendicitis included the presence of peri-appendicular fluid, intra-luminal fluid, fat stranding, appendicolith, abscess, free fluid, and trace free fluid. Additionally, MRI demonstrated excellent test characteristics; the high respective sensitivity, specificity, positive- and negative-predictive values for MRI compared to final diagnosis were 94.9%, 93.5%, 90.2%, and 96.7%, while the observed agreement between MRI diagnosis and final pathology report was 94.9% (kappa = 0.89). Our findings provide additional support for considering implementation of MRI as a second-line imaging strategy within the diagnostic process of suspected pediatric appendicitis (Figure 5).
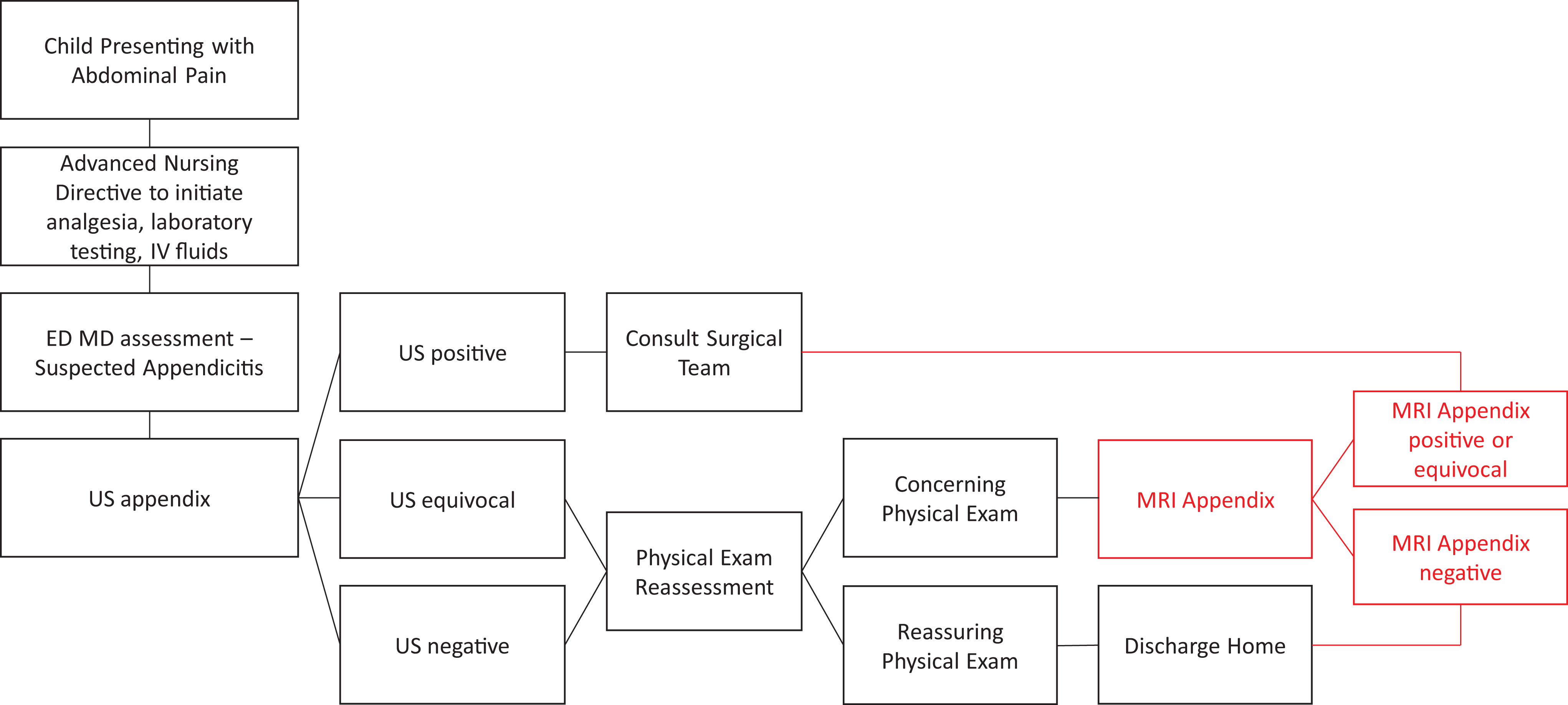
Proposed integration of magnetic resonance imaging in a clinical pathway for suspected pediatric appendicitis. ED indicates emergency department; IV, intravenous; MD, medical doctor; MRI, magnetic resonance imaging; US, ultrasound.
Our results are important for multiple reasons. First, we confirmed that equivocal US results are a clinically relevant limitation for children with suspected appendicitis, even in a Canadian tertiary pediatric health care center with highly trained and experienced US technicians. In our study, 53 (54.1%) US results were equivocal, confirming previous findings that equivocal US can occur in more than half of suspected appendicitis investigations. 8,9,26 -28
Second, it is essential to improve diagnostic certainty in pediatric appendicitis without compromising patient safety. In our sample, MRI performed using fast sequence protocols and without patient sedation provided additional diagnostic information in cases with equivocal ultrasound. Our high sensitivity and specificity values of MRI for suspected pediatric appendicitis are comparable to prior MRI and CT studies. In a meta-analysis of 11 studies reporting the diagnostic certainty of MRI in pediatric appendicitis, MRI was found to have a 96.5% sensitivity (95% CI: 94.3-97.8%) and 96.1% specificity (95% CI: 93.5-97.7%). 19 Similarly, in 4 studies on the diagnostic certainty of CT for suspected pediatric appendicitis, high sensitivity and specificity rates of 95% (95% CI: 92-97%) and 92% (95% CI: 90-94%) were observed, respectively (14). Unlike CT, MRI lacks the long-term risks associated with ionizing radiation, and clinicians have argued for MRI to supplant CT. 20,22,23,29
The absence of secondary MRI findings of peri-appendicular inflammation can help rule out appendicitis, and secondary findings may improve clinicians’ diagnostic acumen. High negative predictive values (97.9-100%) have been observed with incomplete/non-visualized appendixes and no secondary signs of inflammation on MRI, suggesting that these studies could be classified as negative. 30,31 However, a non-visualized appendix with secondary signs can create clinical dilemmas, as 22.2% of these cases have been found to have appendicitis. 30 In our study, secondary findings suggestive of appendicitis on MRI (in equivocal US cases) included abdominal free fluid, peri-appendiceal fluid, intraluminal fluid, fat stranding, appendicolith, and an abscess. While the absence of at least 1 secondary sign of appendicitis predicted absence of appendicitis (high NPV), the presence of at least 1 secondary sign was poorly predictive of disease (low PPV). Prior reports recommend observing for focal peri-appendiceal inflammation, appendicoliths, intraluminal fluid-debris level, and abscesses. 32 In a sample of 97 pediatric patients, intraluminal and localized peri-appendiceal fluid on MRI were associated with appendicitis and found to have high respective sensitivities of 91 and 97% but low respective specificities of 60 and 50%. 33 Additional research is needed to confirm the diagnostic utility of secondary signs of appendicitis on MRI studies.
In the nationally funded and provincially administered Canadian healthcare system, the economic feasibility of implementing MRI for pediatric appendicitis requires consideration. In addition to lacking harmful ionizing radiation and providing highly accurate results, MRI at our site is slightly more affordable ($749) than CT ($786) imaging (personal communication, Department Manager, Diagnostic Imaging, Alberta Children’s Hospital, January 2020). Furthermore, by improving diagnostic certainty, MRI could decrease the number of negative appendectomies (and associated surgical risks and costs) and reduce admissions for observation, compared to US studies alone. In the Netherlands, researchers found MRI could provide an estimated net savings of € 55,746 to € 72,534 over 14 months for patients (N = 138) presenting to the ED with suspected appendicitis. 34 However, one must take into consideration the potential increased financial and human resource costs associated with after-hours imaging. While it is beyond the scope of this study to provide a formal economic analysis for MRI utilization, future evaluation of the potential economic impact of MRI for pediatric appendicitis in Canadian institutions would be beneficial.
Other feasibility considerations include the accessibility of expensive MRI equipment, technicians, and experienced radiologists, which may be limited to tertiary care settings in large urban centers. Finally, MRI equipment and staff may be prioritized for critical cases (e.g., stroke), limiting rapid availability to children with suspected appendicitis.
We conducted this study at a single tertiary pediatric center, with readily available subspecialty emergency, imaging, and surgical expertise, potentially limiting the external validity. Generalizability may also be limited as individuals presenting to our center outside of office hours were excluded (in keeping with regular MRI technician availability at our site); however, our participant demographics are consistent with most other appendicitis cohorts, and there is no reason to suspect different performance of MRI outside of research office hours. We did not include children under 5 years due to concerns of MRI tolerance, as this population may experience difficulty with imaging studies without sedation (21). Our study included a modest sample of individuals who received an MRI (N = 101) and individuals with confirmed appendicitis (n = 39), which is within the range of other MRI study sample sizes (N = 42-208) (21), and our findings are consistent with other studies. Additionally, we performed MRI using a 1.5 T scanner, as it was clinically available and is most readily available in Canada. 3-T MRI scanners offer improved signal-to-noise ratio, which may result in more rapid imaging and improved spatial resolution 35 ; future research may benefit from observing differences in time and image quality for children with suspected appendicitis.
Conclusion
In this study, we demonstrated that MRI can improve diagnostic certainty in children with suspected appendicitis and equivocal US. These findings have the potential to improve patient outcomes by decreasing adverse events, such as missed appendicitis or unnecessary surgery. In children with an equivocal US, those with a positive MRI were very likely to have appendicitis while those with a negative/equivocal MRI were unlikely to be diagnosed with appendicitis. These findings demonstrate the potential utility of MRI as a secondary imaging modality for pediatric patients with suspected appendicitis, and the addition of MRI into Canadian clinical appendicitis pathways/guidelines should be considered.
Supplemental Material
Supplemental Material, sj-pdf-1-caj-10.1177_0846537121993797 - Magnetic Resonance Imaging Provides Useful Diagnostic Information Following Equivocal Ultrasound in Children With Suspected Appendicitis
Supplemental Material, sj-pdf-1-caj-10.1177_0846537121993797 for Magnetic Resonance Imaging Provides Useful Diagnostic Information Following Equivocal Ultrasound in Children With Suspected Appendicitis by Jelena Komanchuk, Dori-Ann Martin, Rory Killam, Robin Eccles, Mary E. Brindle, Ijab Khanafer, Ari R. Joffe, Jaime Blackwood, Weiming Yu, Priya Gupta, Sanjay Sethi, Vijay Moorjani and Graham Thompson in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided as a sub-grant from the Alberta Sepsis Network, funded through an Alberta Innovates—Health Solutions Team Grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.