
Abstract
Purpose:
To discern whether preceding ultrasound (US) results, patient demographics and biochemical markers can be implemented as predictors of an abnormal Magnetic Resonance Cholangiopancreatography (MRCP) study in the context of acute pancreaticobiliary disease.
Methods:
A retrospective study was performed assessing US results, age, gender, elevated lipase and biliary enzymes for consecutive patients who underwent an urgent MRCP following an initial US for acute pancreaticobiliary disease between January 2017-December 2018. Multivariable binary logistic regression models were constructed to assess for predictors of clinically significant MRCPs, and discrepant US/MRCP results.
Results:
A total of 155 patients (mean age 56, 111 females) were included. Age (OR 1.03, P < 0.05), hyperlipasemia (OR 5.33, P < 0.05) and a positive US (OR 40.75, P < 0.05) were found to be independent predictors for a subsequent abnormal MRCP. Contrarily, gender and elevated biliary enzymes were not reliable predictors of an abnormal MRCP, or significant MRCP/US discrepancies. Of 66 cases (43%) of discordant US/MRCPs, half had clinically significant discrepant findings such as newly discovered choledocholithiasis and pancreaticobiliary neoplasia. Age was the sole predictor for a significant US/MRCP discrepancy, with 2% increase in the odds of a significant discrepancy per year of increase in age.
Conclusion:
An abnormal US, hyperlipasemia and increased age serve as predictors for a subsequent abnormal MRCP, as opposed to gender and biliary enzyme elevation. Age was the sole predictor of a significant US/MRCP discrepancy that provided new information which significantly impacted subsequent management. In the remaining cases, however, MRCP proved useful in reaffirming the clinical diagnosis and avoiding further investigations.
Introduction
Multiple imaging modalities are currently available for pancreaticobiliary tract assessment for a variety of infectious, inflammatory and neoplastic pathologies. Despite the often asymptomatic nature of cholelithiasis, an estimated 10–15% of symptomatic patients have associated choledocholithiasis. 1 The presence of common bile duct (CBD) stones in the context of acute biliary disease is of critical importance for clinicians as there are multiple potential associated clinical complications (biliary obstruction, pancreatitis, and cholangitis) alongside procedural complications with significantly increased surgical morbidity and mortality. 2 Additionally, chronic/recurrent choledocholithiasis is a potential risk factor for the development of cholangiocarcinoma. 3
Ultrasonography has been shown to be limited in its performance in the assessment of choledocholithiasis, with sensitivities in the range of 25–58% and specificities of 68–91% for the detection of CBD stones. 4 Conversely, the utility of Magnetic Resonance Cholangiopancreatography (MRCP) has already been established in delineating biliary anatomy and the diagnosis of bile duct stones; in 2003, Romagnuolo et al. reported an authoritative meta-analysis of 67 published studies, demonstrating that MRCP has an excellent sensitivity of 95% and a specificity of 97% for detecting CBD stones.5,6 Additionally, MRCP offers a noninvasive alternative to endoscopic retrograde cholangiopancreatography (ERCP) while avoiding potential complications of ERCP such as hemorrhage, pancreatitis and sepsis.
Multiple clinical algorithms have been developed to attempt to predict the risk of choledocholithiasis according to a combination of imaging, clinical and biochemical markers.7-9 However, these are of mediocre accuracy and there is no current generalized consensus on the ideal utilization of MRCP. 10 The purpose of this study was to evaluate the yield of urgent MRCPs performed for in-hospital and emergency department (ED) patients presenting with acute pancreaticobiliary disease, and to determine potential predictors of a positive study. This was done via scrutinizing multiple variables, including patient age, gender, preceding pancreaticobiliary enzymes, and results of initial US assessment. Additionally, we scrutinized US/MRCP discrepancies and whether any of the aforementioned variables are reliable predictors for a significant discrepancy.
Materials and Methods
Study Design
A single-centre retrospective study was performed. The protocol was approved by the local Integrated Regional Ethics Board at our institution.
Patient Selection and Data Collection
All consecutive inpatient and ED patients who underwent an urgent MRCP following initial US assessment for the evaluation of acute pancreaticobiliary disease at our institution from January 2017-December 2018 were included. Patients with a prior biliary US and pancreaticobiliary enzyme testing during the same hospital stay or ED visit prior to the MRCP were included. Specifically, total bilirubin, alkaline phosphatase (ALP), gamma-glutamyl-transferase (GGT) and lipase were required for inclusion. No specific age limit was set, although the minimum age in our study is 18 years.
For patient recruitment, a search of the local Picture Archiving and Communication System (PACS) was conducted to identify all urgent MRCP exams which were performed during the specified time period. Nonurgent and outpatient exams were excluded. The provided clinical indication for each exam was reviewed to ensure that the exam was performed for investigating acute pancreaticobiliary disease. This included acute symptomatology (e.g., right upper quadrant pain, ascending cholangitis or acute pancreatitis), biochemical or US abnormalities.
Subjects were excluded if they were being investigated for non-acute pathology such as work-up of chronic pancreatitis or chronic biliary conditions such as biliary cystic disease. Patients who were initially assessed with CT instead of US prior to the MRCP were also excluded. Patients with a technically suboptimal and nondiagnostic US assessment were excluded. Prior cholecystectomy was not an exclusion criterion as long as all inclusion criteria were fulfilled.
A review of each patient’s electronic medical record was performed. Patients’ demographics (age and gender) were recorded. Pre-MRCP total bilirubin, ALP, GGT and lipase levels were noted as normal or abnormal. Abnormal biomarkers were defined as total bilirubin > 21umol/L, ALP > 120U/L, GGT > 37U/L, and lipase > 79U/L. Only the first reading at presentation prior to the MRCP was considered, and no analysis of trends or peak values was made. Moreover, ultrasound and MRCP yields were recorded. A positive ultrasound or MRCP study was defined as the presence of any abnormality involving the pancreaticobiliary tree. For both imaging modalities, a positive study was one which demonstrate one or more of: cholelithiasis, cholecystitis, CBD dilatation, intrahepatic biliary dilatation, choledocholithiasis, findings of pancreatitis, pancreaticobiliary masses or collections. Conversely, a negative imaging study was defined as one demonstrating none of the aforementioned abnormalities. If the examination demonstrated an abnormality not related to the pancreaticobiliary tree such as a liver lesion or renal mass, it was still considered negative in the context of the study. Furthermore, if an US failed to demonstrate distal CBD stones or masses in cases of biliary dilatation, it was still deemed “positive” due to the presence of abnormal biliary dilatation. These US studies were not excluded as failure of demonstrating suspected distal CBD stones is related to the intrinsic limitation of US as an imaging modality and this is well established in the literature. Finally, MRCP yield was recorded using the same criteria as US. We further investigated whether the MRCP result was discrepant from the preceding US, and whether this discrepancy affected subsequent management.
MRCP Protocol
Urgent MRCPs at our institution are performed as per a standard institutional protocol on a 1.5 T MRI unit using a phased-array body coil (GE Healthcare). Patients are expected to be in a fasting state for 4 hours prior to the study. Anti-peristaltic agents are not routinely utilized. Initial multiplanar localizer images are acquired to localize and plan subsequent sequences. Depending on feasibility and the patient’s ability, a combination of breath-holding and free respiratory acquisitions are performed. Acquired sequences include an axial Diffusion, Coronal T2, Coronal FIESTA (Fast Imaging Employing Steady-state Acquisition), Axial LAVA (Liver Acquisition with Volume Acquisition), and Coronal 3D MRCP imaging. No contrast is utilized for this abbreviated urgent MRCP protocol.
Image Interpretation
For all US and MRCP studies, our results were based on the staff Radiologist’s report. The imaging was reviewed in complex cases, or ones where ambiguous descriptors were utilized in the report and further clarification was needed. Radiologists at our institution adapt a very similar standard for reporting pancreaticobiliary disease on US and MRCP, with similar cutoff criteria for various parameters (gallbladder wall thickening exceeding 3 mm, gallbladder distension as a transverse diameter of greater than or equal to 5 cm and normal CBD diameter equaling 6 mm with an additional 1 mm given per decade over the age of 60).
For abnormal MRCPs, we scrutinized whether additional and clinically relevant information was provided compared to the preceding US. Examples include detecting CBD stones, strictures, or malignancy which were not appreciated sonographically. We further examined if the decision of undergoing an ERCP was influenced by the MRCP result.
Statistical Analysis
To evaluate the potential factors which may be associated with an abnormal MRCP as well as the potential factors which may be associated with a discrepancy between US and MRCP, multivariable binary logistic regression models were constructed. Odds ratios were calculated and a P-value of < 0.05 was set as the threshold for affirming statistical significance. All statistical analysis was performed using the statistical software SPSS Statistics version 24 (IBM Corp., Armonk, NY).
Results
From a total of 167 consecutive patients who underwent an urgent MRCP for acute pancreaticobiliary disease in the specified time frame, 12 patients were excluded from the study due to the absence of a preceding ultrasound. Of the 12 patients, 8 had a pre-MRCP CT scan in the ED, and the remaining 4 patients had no pre-MRCP imaging and were all being investigated for complications of chronic pancreatitis. No analysis of CT/MRCP concordance was made for this excluded patient population as it was beyond the scope of this study. A total of 155 patients were included in the study [age range: 18-97, mean age 56; 44 males, 111 females]. The time frame between the US and MRCP was less than 2 weeks for 151 patients, and greater than that time period for 4 patients. MRCPs and US studies included in the study were technically satisfactory and none were excluded for nondiagnostic quality. US examinations included in the study were both performed as a general abdominal protocol and focused hepatopancreaticobiliary (HPB) protocol. All US examinations were performed by ultrasound technologists in our department. The US and MRCP results were categorized into 5 groups, shown in Figure 1.
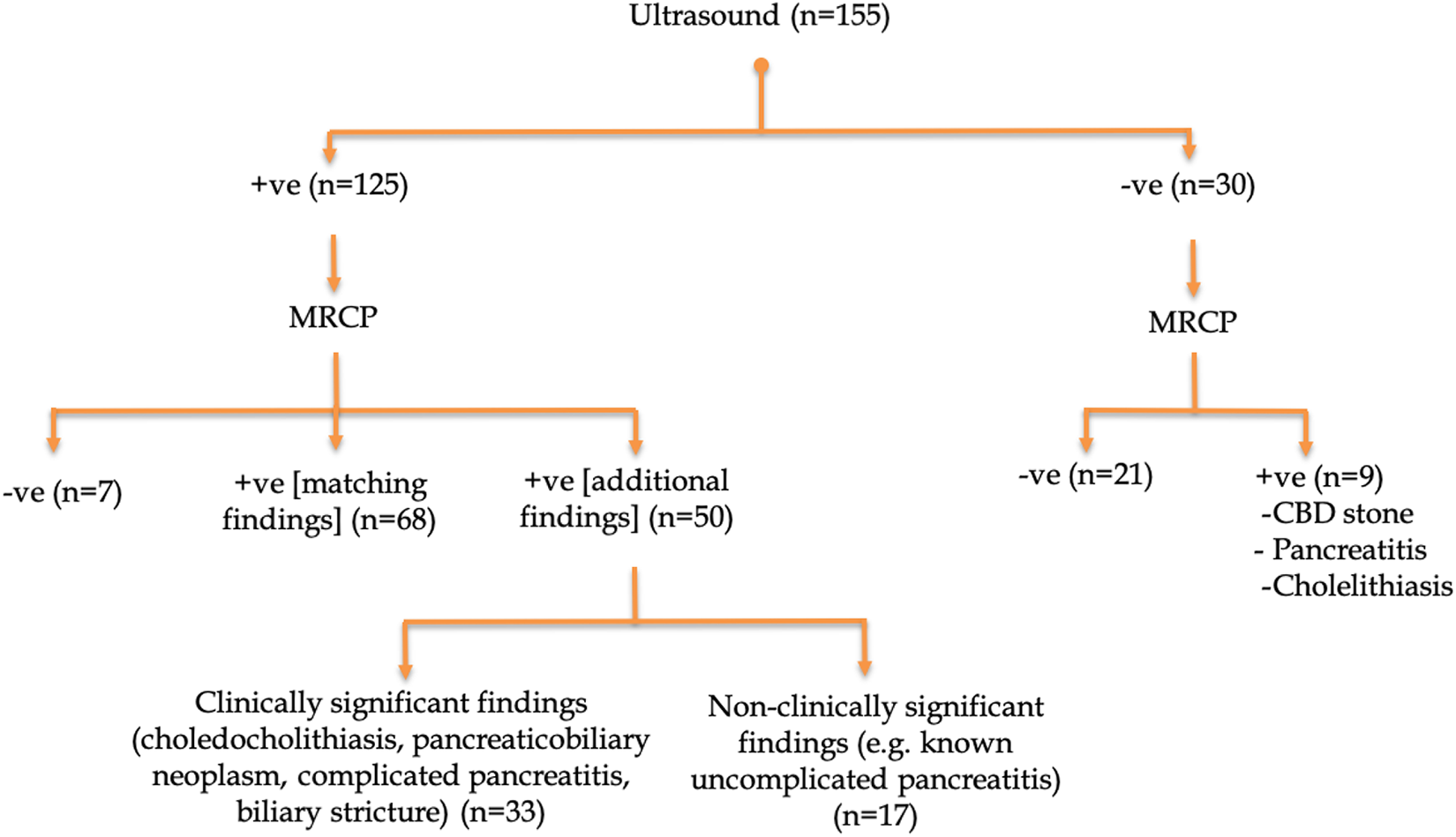
Baseline US and subsequent MRCP results.
Regression Analysis
Elevated serum lipase (OR: 5.33, P = 0.04), a positive US (OR: 40.75, P < 0.01) and increased age (OR: 1.03, P = 0.04) were all independent predictors for a subsequent positive MRCP. Elevated total bilirubin, ALP, GGT and patient gender were not significantly associated with and abnormal MRCP (Table 1).
Multivariable Binary Logistic Regression Model Assessing the Factors Associated With an Abnormal MRCP Result.
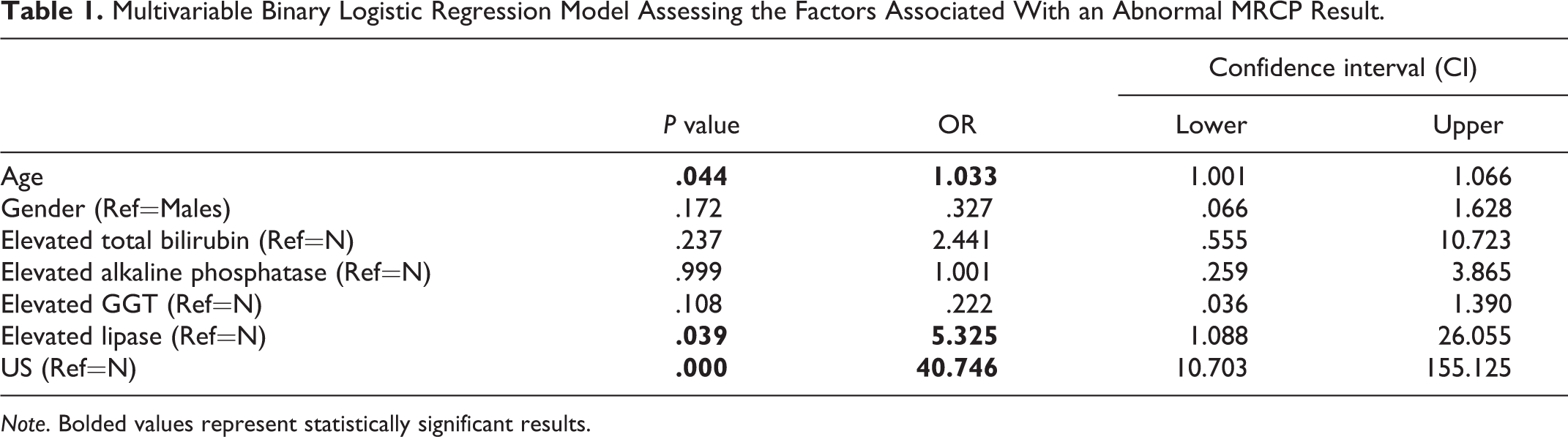
Note. Bolded values represent statistically significant results.
Increased age was the sole independent predictor for a significant US/MRCP discrepancy (OR 1.02, P = 0.03), which may impact clinical management. The analysis specifically showed a 2% increase in the odds of having a discrepant US/MRCP with every year of increase in age (Table 2).
Multivariable Binary Logistic Regression Model Assessing the Factors Associated With a Discrepant US/MRCP Result.
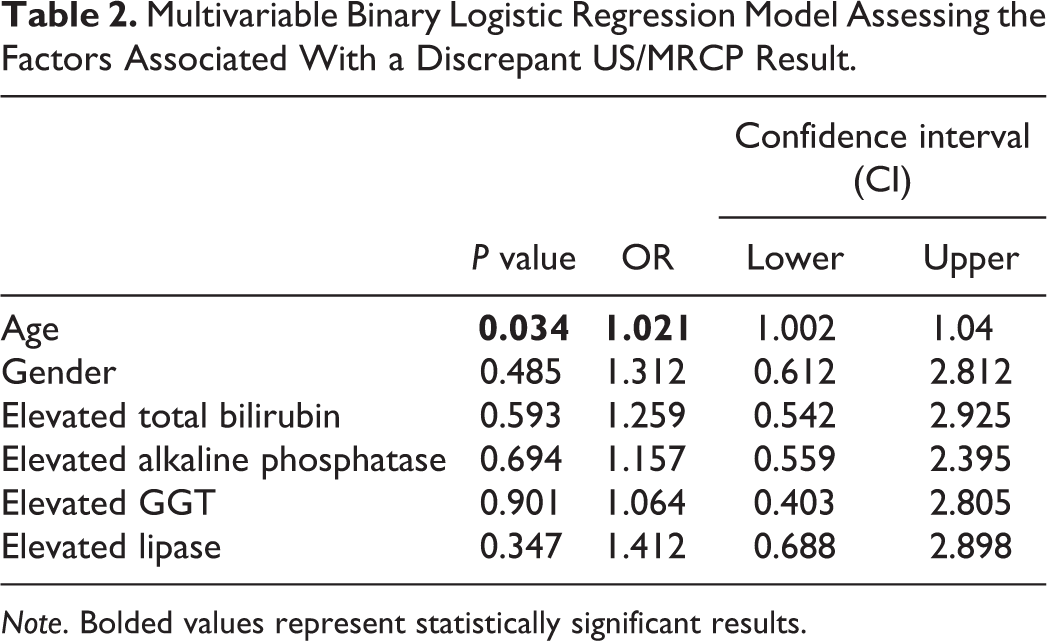
Note. Bolded values represent statistically significant results.
Abnormal Initial US and Subsequent MRCP Results
Of the 155 patients included in the study, 125 (80.6%) had an abnormal initial US. Subsequent MRCP demonstrated concordant positive findings for 68 subjects (54.4%). Of the remaining 57 subjects, 50 (87.7%) had an MRCP that provided additional information. Of these, 33 patients demonstrated clinically significant discrepancies such as the discovery of choledocholithiasis (24 subjects), pancreaticobiliary neoplasms (6 subjects), biliary strictures (2 subjects) and complicated pancreatitis (1 subject). The subsequent management was significantly affected by the outcome of the MRCP, with many patients undergoing ERCP, IR-guided procedures and pancreaticobiliary surgery. Moreover, 17 subjects demonstrated clinically redundant findings, such as changes of acute interstitial pancreatitis not appreciated on initial US. Finally, 7 subjects had a normal MRCP, which refuted the initial US findings. The abnormalities excluded included biliary tree dilatation (4 subjects), gallbladder wall thickening (2 subjects), and CBD sludge (1 subject).
Normal initial US and subsequent MRCP results
A total of 30 patients (19.4%) from the study cohort had a normal initial US exam. Of these, 21 patients (70%) had a subsequent MRCP which was negative and concordant. However, 9 subjects (30%) had a discordant positive subsequent MRCP, with findings of CBD sludge/stones (4 patients), acute pancreatitis (4 patients) and cholecystitis (1 patient). Among the 9 discrepant cases, the 4 cases of CBD sludge/stones necessitated further management with ERCP. Three of the 4 cases were managed with stone retrieval, while one case had a normal ERCP, possibly secondary to stone passage in the interim.
A summary of the US/MRCP imaging discordances is illustrated in Figure 2, and an example of each scenario is depicted in Figures 3–6.
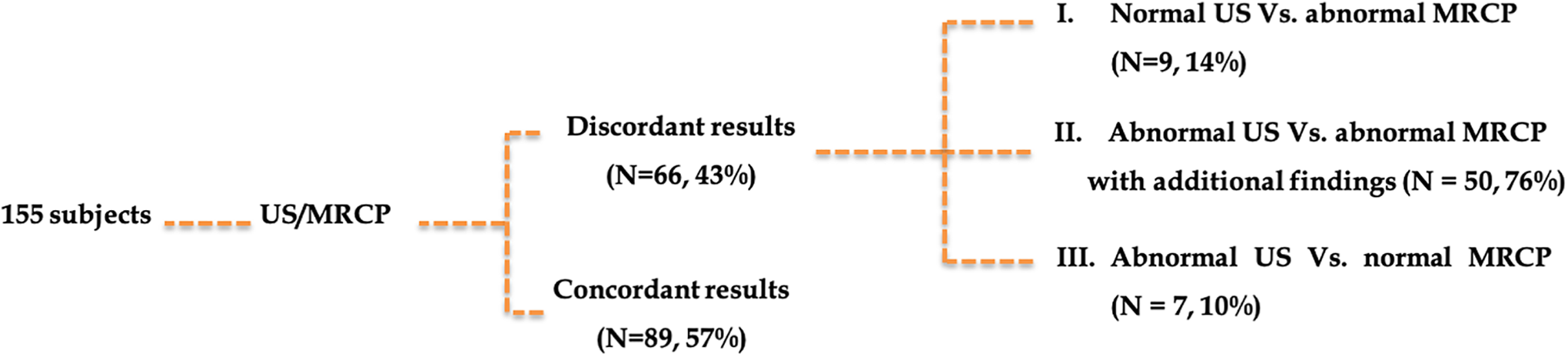
US/MRCP concordance.
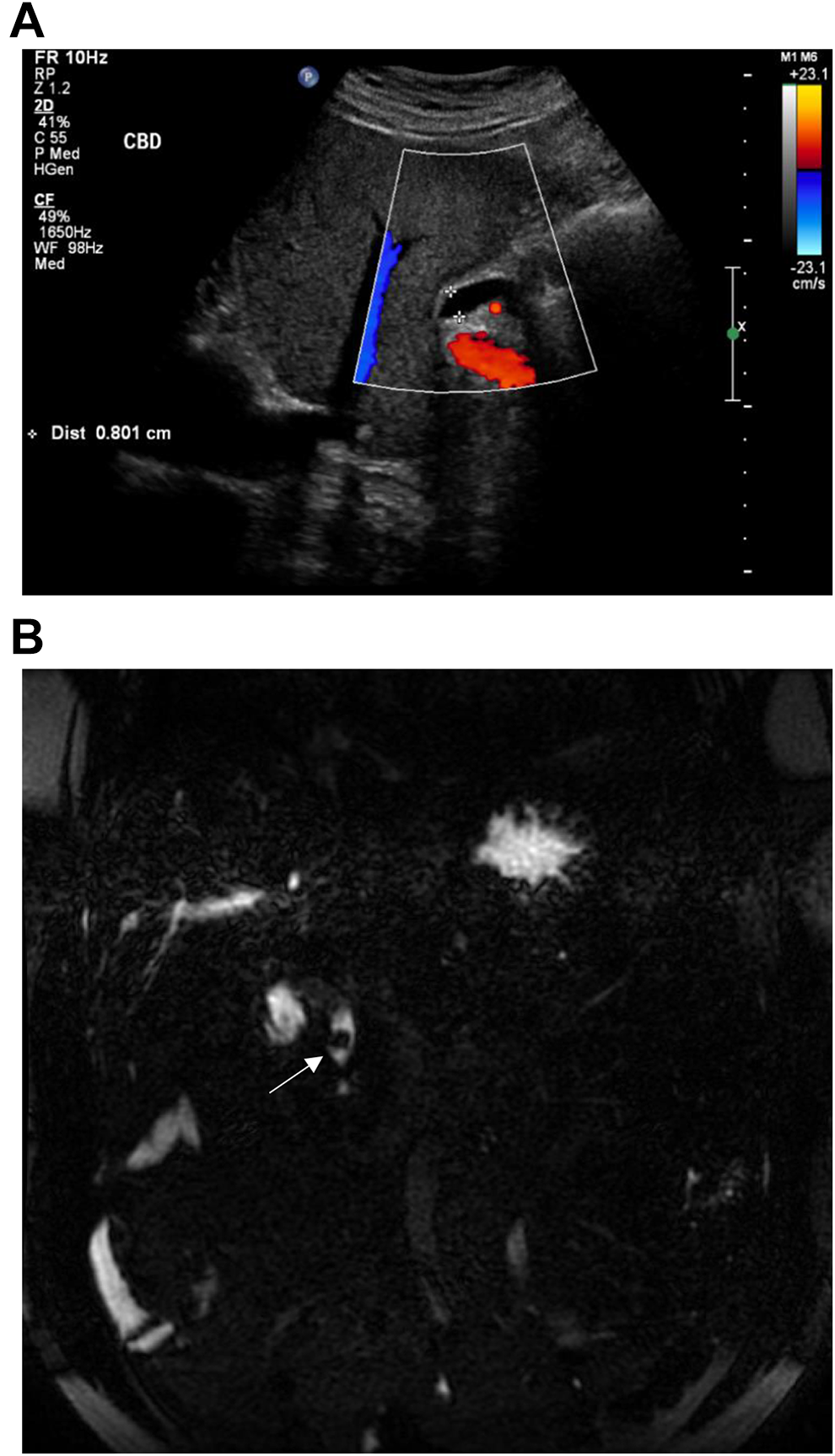
Example of a normal US followed by an abnormal MRCP. US and coronal MRCP images in a 76-year-old male patient who had remote cholecystectomy and presents with pancreatitis and RUQ pain. US image of the epigastrium (A) demonstrates a CBD measuring 8 mm in diameter, considered normal given the patient’s age and post-cholecystectomy status. An urgent MRCP performed the following day (B) demonstrates a distal CBD stone (white arrow) measuring 9 mm.
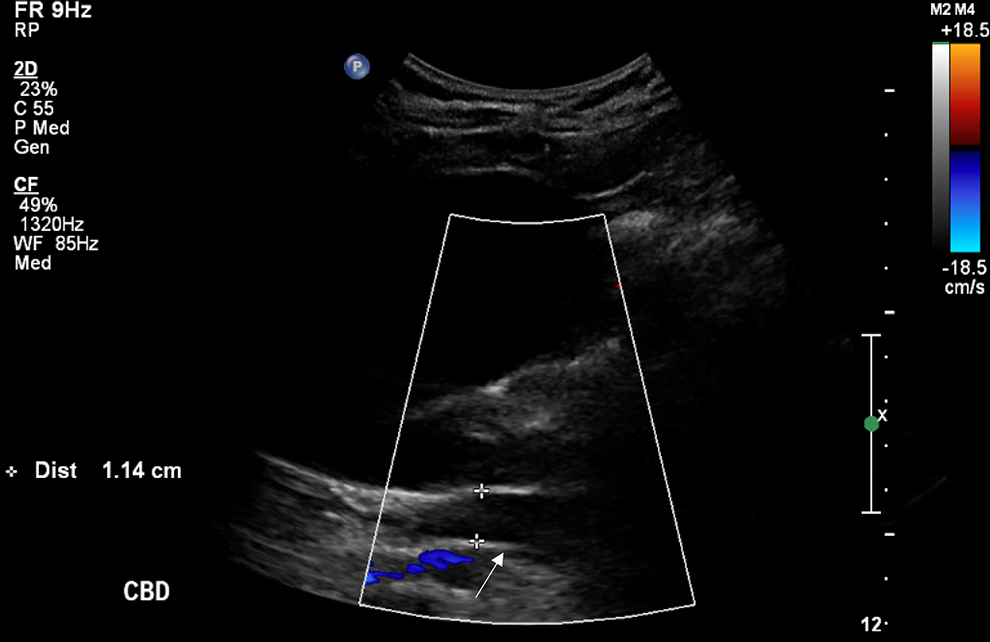
Example of an abnormal US followed by a normal MRCP. Ultrasound image of the right upper quadrant in a 76-year-old female patient presenting with febrile right upper quadrant pain demonstrating gallbladder distension with no cholelithiasis or features of acute cholecystitis. The CBD is dilated, measuring 1.1 cm (white arrow). An urgent MRCP was request thereafter to investigate for choledocholithiasis given reported intrahepatic biliary ductal prominence and CBD dilatation at 1.1 cm [CBD shown in the image, with calipers]. MRCP the next day confirmed dilatation of the CBD to likely be age related, with no evidence of stones or inflammatory biliary disease.
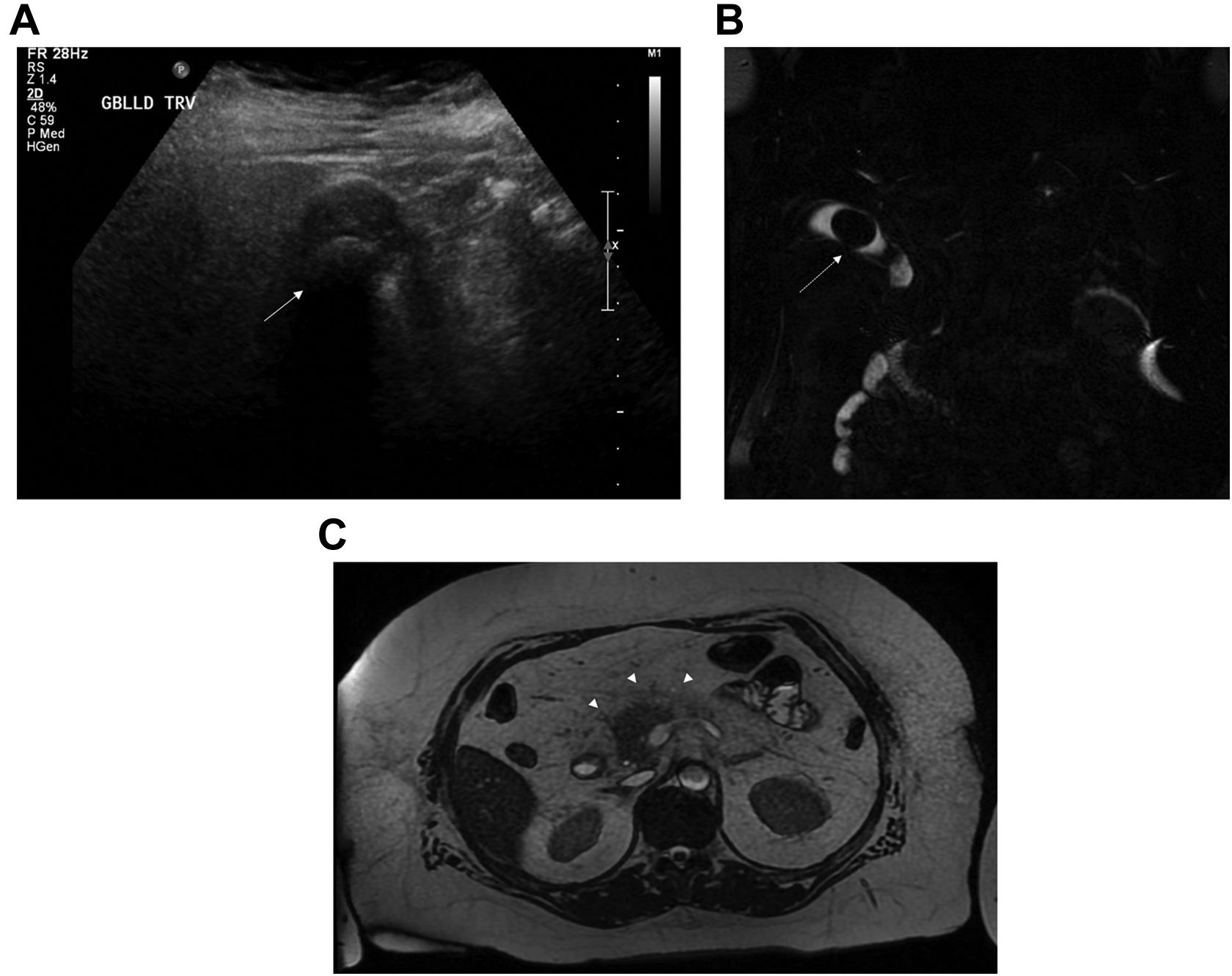
Example of an abnormal US followed by an abnormal MRCP with non-clinically significant findings. 71-year-old female presenting with biliary colic and acute pancreatitis. Initial US (A) demonstrates uncomplicated cholelithiasis with a large stone (white arrows) seen in the gallbladder body. Follow up coronal MRCP image (B) performed 2 days later for increasing bilirubin reiterated findings of uncomplicated cholelithiasis (dashed white arrow). Axial T2 weighted image (C) also demonstrated peripancreatic stranding (arrow heads), consistent with the clinically known pancreatitis. No additional findings were seen on MRCP.
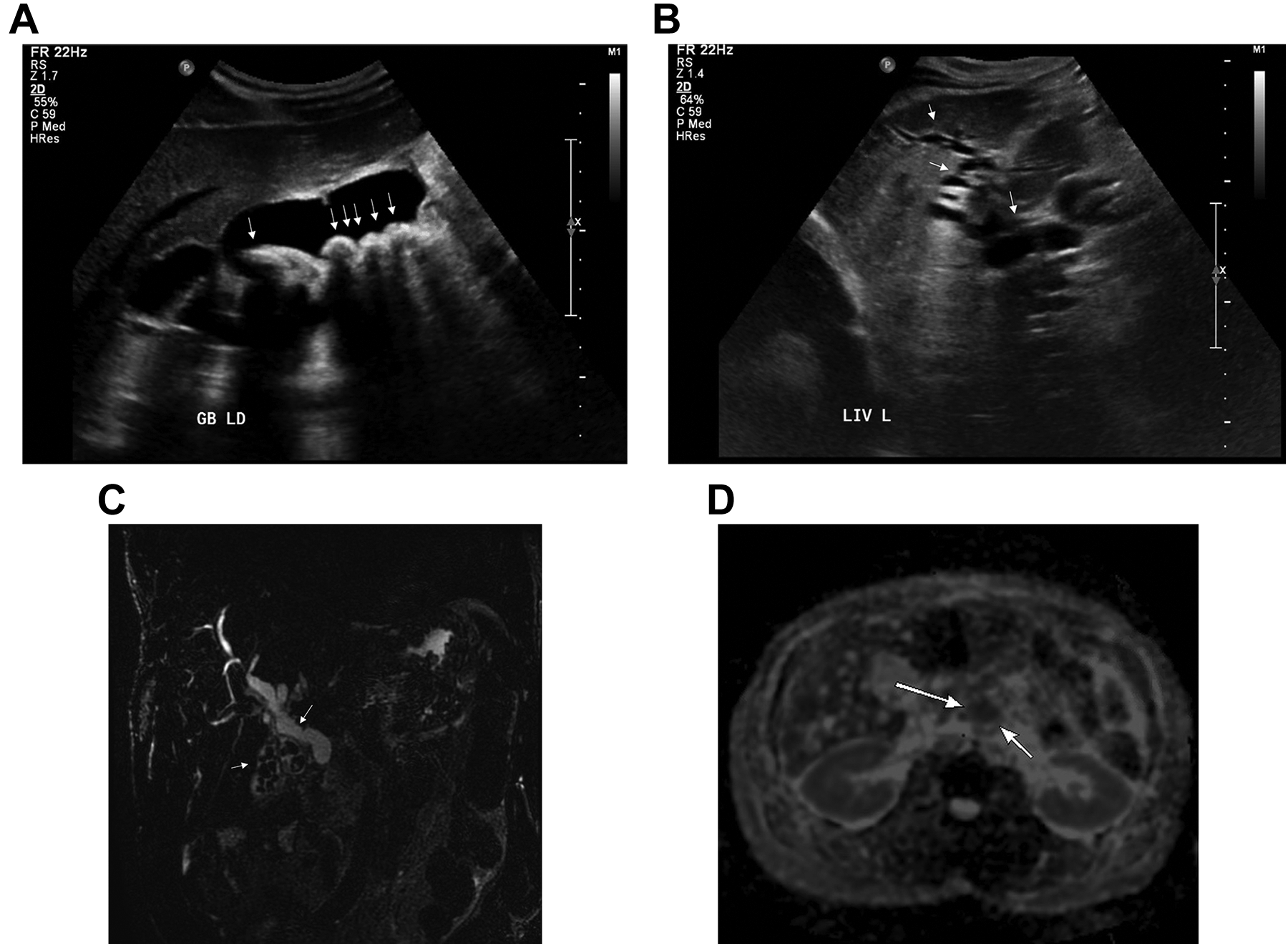
Example of an abnormal US followed by an abnormal MRCP with clinically significant findings. Ultrasound and MRCP assessment in a 57-year-old male patient presenting with painless jaundice. Initial US (A,B) demonstrates significant cholelithiasis (white arrows) with no secondary evidence of acute cholecystitis. There is also significant intrahepatic biliary ductal dilatation (white arrows). Follow-up coronal MRCP image (C) acquired the next day reiterated findings of uncomplicated cholelithiasis and biliary ductal dilatation (white arrows). On the ADC map (D) a low signal mass (white arrows) was identified to involve the pancreatic neck measuring approximately 2.1 x 3 cm. Given the degree of obstruction, the patient underwent decompression via a percutaneous biliary drainage catheter, and follow-up ERCP confirmed suspected malignant findings.
Discussion
Gallstone disease, in the western world, occurs in approximately 20% of adults, with 2-4% of individuals experiencing symptoms each year.11-13 Given that concomitant choledocholithiasis is not a rare complicating factor, and the significant surgical morbidity associated with this, a number of studies have investigated potential algorithms for tackling this dilemma. While the adequacy of sonographic assessment in acute gallbladder and biliary disease is established in the literature, it remains rather limited when investigating CBD stones. 14 MRCP, on the other hand, has emerged as a reliable and non-invasive method with superior performance for ductal disease and stones.15,16
Multiple studies have investigated the role and utility of pre-surgical MRCP imaging for select patients, based on preceding sonographic findings and biochemical derangements.17-19 Some studies advocated against routine MRCPs for the minor possibility of choledocholithiasis, as it is not cost-effective.19,20 Additionally, there is the other potential complication of delaying appropriate care. 17 Conversely, there are studies which support the routine use of MRCP in the preoperative evaluation of patients with suspected acute biliary disease, regardless of sonographic findings or biochemical derangements. 20 Given the importance of identifying patients who would be appropriate candidates for preoperative MRCP, some studies attempted to stratify patients based on clinical, laboratory and US findings.4,11,12,21,22 Results have been variable, and no generalized consensus is currently followed. 23 The guidelines published by the American Society for Gastrointestinal Endoscopy emphasize that biochemical tests have the most utility in excluding CBD stones, based on a series of over a 1000 patients undergoing laparoscopic cholecystectomy.24,25
In our study, we attempted to assess for potential predictors of a positive MRCP, including patient demographics, elevated serum biliary enzyme levels, elevated serum lipase, as well as preceding US findings. Our ultimate goal was to discern which patients benefited most from an urgent MRCP that provided new, clinically significant information compared to the preceding US. While an abnormal US and MRCP were defined as those demonstrating any pancreaticobiliary disease, a significantly discrepant US/MRCP was a case where the MRCP provided discrepant or additional findings from the preceding US, thereby altering subsequent management.
Based on our findings, abnormal biliary enzyme levels were not a significant predictor of a positive MRCP. This is concordant with studies of liver histology in cases of acute cholecystitis, which confirm multiple contributors to abnormal liver indices including nonspecific reactive hepatitis. 25 As in other studies, elevated liver function tests and total bilirubin were noted in cases of acute cholecystitis, whether concomitant choledocholithiasis was present or not. 26 While some suggest that hyperbilirubinemia reflects true biliary obstruction at presentation of acute cholecystitis and pancreaticobiliary disease, another hypothesis is that it may be reactive to hepatocellular injury in the acute setting.7,10,11,27,28 In our study, the majority of our cohort had abnormal biliary enzymes at presentation (80.6% elevated GGT, 73.5% elevated bilirubin and 55.5% elevated ALP), although most of these patients had no choledocholithiasis.
Our study reiterated the predominant female predilection for biliary disease (71.6% of the patient population), while negating the male predominant incidence of choledocholithiasis.7,29 We found no significant association between gender and a subsequent positive MRCP.
Elevated serum lipase was shown to be a statistically significant predictor of an abnormal MRCP exam. In our study, 47 patients (30.3%) presented with elevated serum lipase to varying degrees, some of whom were clinically diagnosed with acute pancreatitis. For these patients, MRCP was superior in demonstrating changes of acute interstitial pancreatitis compared to US [24 subjects, 51.1% on MRCP versus 3 subjects, 6.4% on US]. Given that the diagnosis of acute pancreatitis is primarily based on clinical and biochemical grounds, the majority of MRCPs performed in patients with elevated lipase added no additional clinical information despite being abnormal. However, in a subgroup of 10 patients with hyperlipasemia (21.3%), MRCP demonstrated significant concomitant disease such as choledocholithiasis (8 subjects), biliary stricture (1 subject) and pancreatic neoplasm (1 subject). The management of this subgroup was significantly altered by the MRCP results, with 7 of 10 patients undergoing an immediate subsequent ERCP. Despite this, hyperlipasemia was not shown to be a statistically reliable predictor of significant US/MRCP discrepancies, which may be due to the small sample size in our study.
Furthermore, an abnormal US was a statistically significant predictor of an abnormal MRCP. Collectively, only the slight majority of MRCP results confirmed known sonographic findings (89 cases, 57%). In this scenario, MRCPs served as confirmatory exams to establish the clinical diagnosis and avoid further investigations. Nonetheless, a high US/MRCP discordance rate existed (66 cases, 43%), with the largest category being a positive US followed by a positive MRCP which provided additional information (50 cases, 32%). Among these 50 discordant cases, 17 cases (34%) had additional findings that were occult on US but clinically known and sometimes of no clinical significance, such as imaging features of uncomplicated interstitial pancreatitis. The authors are aware that US is not used in the diagnosis of pancreatitis, but rather to confirm a biliary etiology of pancreatitis, and MRCP continues to exhibit superior sensitivity in making this diagnosis. However, 33/50 cases (66%) had clinically significant discrepant findings including choledocholithiasis, biliary/pancreatic tumors and complicated pancreatitis which were not appreciated sonographically. In cases of a negative US and a positive subsequent MRCP, the underlying missed pathology was often related to stone disease and acute pancreatitis. Similarly, biliary dilatation was the most frequent finding on US to be refuted on subsequent MRCP, followed by cholecystitis and CBD sludge.
An increase in patient age was shown to be a significant predictor of a subsequent abnormal MRCP, and the sole predictor of a significant US/MRCP discordance, with a unit increase in age corresponding to a 2% increase in the odds of having a significant discordance. This may be attributable to increased rates of choledocholithiasis and malignancy with increased age.7,8,30 However, the clinically utility of this is limited as there is no clear age cut-off, and each patient should be treated according to their unique clinical context.
ERCP was performed for 44 patients in the study. In 36 subjects (81.2%), ERCP results matched the preceding MRCP findings. Of the remaining discordant MRCP/ERCP group, 3 cases of ERCP-proven CBD stones were occult on MRCP which solely demonstrated significant ductal dilatation. A single case of ERCP-detected malignancy was occult on MRCP, and 4 cases of MRCP-detected CBD stones were not apparent on follow-up ERCP, possibly secondary to stone passage in the interim. The overall findings emphasize the high concordance between MRCP and ERCP, yet further echo that the need for ERCP remains tailored to individual cases based upon overall clinical gestalt. While MRCP was highly useful in guiding the surgical team for follow-up ERCPs, cases of missed CBD stones and carcinoma highlight the pivotal role for patient-based clinical decision making.
There are a few limitations inherent to our study, related to the retrospective design involving a single institution and the relatively limited sample size. Additionally, there is a degree of bias related to the interpretation of the imaging reports, although ambiguous cases were individually reviewed for clarification. We also recognize the variable nature of biochemical markers throughout the course of a patient’s hospitalization, although we considered the baseline values at presentation for standardization purposes.
In conclusion, given the limited availability and high cost of MRCP, we attempted to assess the true utility of these studies in patients presenting with acute pancreaticobiliary disease. Our findings reveal that hyperlipasemia, increased age and an abnormal US were predictors of an abnormal MRCP, while the sole predictor of a significant US/MRCP discrepancy was age. Although these findings may appear intuitive given the increased incidence of CBD stones and malignancy with age, our study was able to objectively confirm this. In practice, the clinical application of this finding is limited, however. This reiterates the findings of past studies that no discrete clinical, biochemical or imaging algorithm can clearly define the utility of urgent MRCPs. Additionally, our results reflect the significant utility of MRCPs, both in positive or negative cases, as they ultimately served to reach or confirm a definitive diagnosis, guide further management and avoid unnecessary additional investigations. Collectively, this study underlines the challenges in management of acute pancreaticobiliary disease in relation to MRCP imaging. The few cases of MRCP-missed choledocholithiasis and carcinoma which were confirmed on subsequent ERCP reiterate that imaging at this stage cannot replace ERCPs. It is also highly possible that potential overutilization of MRCPs in the acute setting maybe clinically justified given the substantial findings, which affect subsequent management pertaining to ERCPs, surgical planning and avoiding further investigations. Ultimately, further research is required on a larger scale to accurately define pretest probabilities of MRCP yield which would add clinically significant value in the management of acute pancreaticobiliary disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.