
Abstract
Background
Delirium is a common yet underdiagnosed condition in hospitalized older adults, particularly challenging to detect early in cardiology settings. Although delirium assessment tools improve detection rates, observations by family caregivers of patients’ cognitive changes can offer valuable insights, supplementing assessments by healthcare professionals. However, validated French-language tools for family caregivers to assess delirium in acute care settings in Canada are lacking.
Purpose
Translate, culturally adapt, and validate the Family Confusion Assessment Method for French-speaking cardiovascular patients and their caregivers (FAM-CAM-Fr).
Methods
The translation and cultural adaptation of the FAM-CAM were conducted following the guidelines of Sousa and Rojjanasrirat (2011). Criterion validation involved 100 dyads of family caregivers and hospitalized cardiovascular patients. The FAM-CAM-Fr's performance was assessed by comparing it to the Confusion Assessment Method (CAM) and the DSM-5 diagnostic criteria for delirium. Measures of sensitivity, specificity, and agreement with the CAM were calculated.
Results
The FAM-CAM-Fr showed high specificity (92.6%) but low sensitivity (58%) in detecting delirium. Cohen's Kappa indicated a moderate agreement (>0.50) between the FAM-CAM-Fr and the CAM. Despite family caregivers using the tool without prior training, indicating its usability in real-world settings, sensitivity was lower compared to studies that included caregiver training, though specificity was similar.
Conclusion
The FAM-CAM-Fr is promising as a specific tool for screening delirium in cardiovascular patients. Despite its low sensitivity, its high specificity indicates that it is effective at ruling out delirium. Future research should focus on further validation across various settings.
Keywords
Introduction
Delirium significantly increases morbidity and mortality, while substantially affecting the recovery of hospitalized older adults who frequently experience this complication (Wilson et al., 2020). Its occurrence can also impair patients’ baseline cognitive function (Hayhurst et al., 2020). Although early detection of delirium is critical to mitigating its impact, it remains a major challenge (Aikawa et al., 2024). Studies consistently reveal that healthcare professionals accurately identify fewer than 30% of delirium cases in hospitalized older adults (Titlestad et al., 2024; Wand et al., 2014), with even lower recognition rates among those with underlying neurocognitive disorders, such as dementia (Fick et al., 2013, 2015).
The systematic use of delirium assessment tools by healthcare professionals can improve detection rates (Barr et al., 2013; Gélinas et al., 2018; Registered Nurses’ Association of Ontario, 2016). However, even with these tools, identifying delirium remains challenging, particularly in acute care settings or among patients with neurocognitive disorders such as dementia (Fick & Mion, 2008; Holly et al., 2014; Steis & Fick, 2008). The severely compromised clinical condition of patients, combined with their short hospital stays, makes it difficult for healthcare professionals to acquire the knowledge needed to recognize the subtle changes that signal delirium onset. Understanding patients’ baseline cognitive function and personality traits is crucial for detecting these subtle indicators (Fick et al., 2015; Rosgen et al., 2018).
In this context, family caregivers are a valuable source of information that could supplement the health professionals’ assessments and could help identify subtle changes in the usual cognitive functioning of the patient (Bull et al., 2016, 2017; Mailhot, 2017; Martins et al., 2014; Steis et al., 2012). Integrating family caregiver's knowledge of the patient and their observations of changes, using a structured tool, could help health professionals detect delirium more quickly and monitor it more accurately.
A recent systematic review identified three tools that could be independently completed by family caregivers (Rosgen et al., 2018). Among these three tools, the Family-Confusion Assessment Method (FAM-CAM) demonstrated strong psychometric properties and required minimal family training for its completion. The FAM-CAM is based on the most widely used delirium detection tool for healthcare professionals, i.e., the Confusion Assessment Method (Inouye et al.). More importantly, the FAM-CAM includes simple yes-no items along with an item that allows detailed qualitative description of families’ observations. Therefore, the FAM-CAM holds great potential in increasing delirium detection if supplemented to healthcare professionals’ systematic assessments. This tool has been validated in outpatients and long-term care settings and is available in English and other languages such as Portuguese and Chinese (Martins et al., 2014; Steis et al., 2012; Xing et al., 2024). The original American English version is available online at https://help.agscocare.org/login-required. The French version of the FAM-CAM is not available, thereby limiting the potentially significant contribution of families in the rapid detection of delirium in a Francophone population.
The absence of a validated French version of the FAM-CAM restricts the capacity of Francophone caregivers in Canada to engage in delirium screening. In the context of Canada's officially bilingual healthcare system, the availability of culturally and linguistically adapted tools is essential to ensuring equitable access to care for Francophone populations. Canadian healthcare guidelines recommend utilizing validated and culturally appropriate screening tools whenever possible (Registered Nurses’ Association of Ontario, 2016). Language barriers can hinder delirium detection. While professional interpreters may be available in certain contexts, a validated screening tool in the caregiver's preferred language would enhance accessibility and facilitate early detection. Modifying the FAM-CAM for French-speaking populations aligns with these recommendations and addresses a critical gap in delirium detection screening.
The purpose of this study was to create the version of the FAM-CAM for French speaking populations of Canada (FAM-CAM-Fr) and to perform an initial validation in cardiovascular patients in an acute care setting. The primary objective was to translate and culturally adapt the FAM-CAM into a French version for Canada according to the rigorous approach proposed by Sousa and Rojjanasrirat (2011). The secondary objective was to examine criterion validation of the FAM-CAM-Fr using the reference standard in the field of delirium (i.e., medical diagnosis according to DSM-5 criteria) and related criteria (i.e., CAM and keywords associated with delirium (encephalopathy, confusion, agitation, hallucination, somnolence, Haldol (Puelle et al., 2015)).
Methods
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., 2007). The reporting checklist is provided in Appendix 1.
Primary Objective: Translation and Cultural Adaptation
The original English version of the FAM-CAM was translated and culturally adapted to French for Canada using the method suggested by Sousa and Rojjanasrirat (2011). Following the copyright clearance from the author of the FAM-CAM for translation and use in this study, we conducted five steps to translate and culturally adapt the tool presented in Table 1. The table describes a detailed five-step translation and validation process for adapting the FAM-CAM tool from English to French. Step 1 consisted in the forward translation of the tool by two translators, both native French speakers, who independently translated the original English FAM-CAM into French, producing two initial French versions of the tool.
Translation Process.
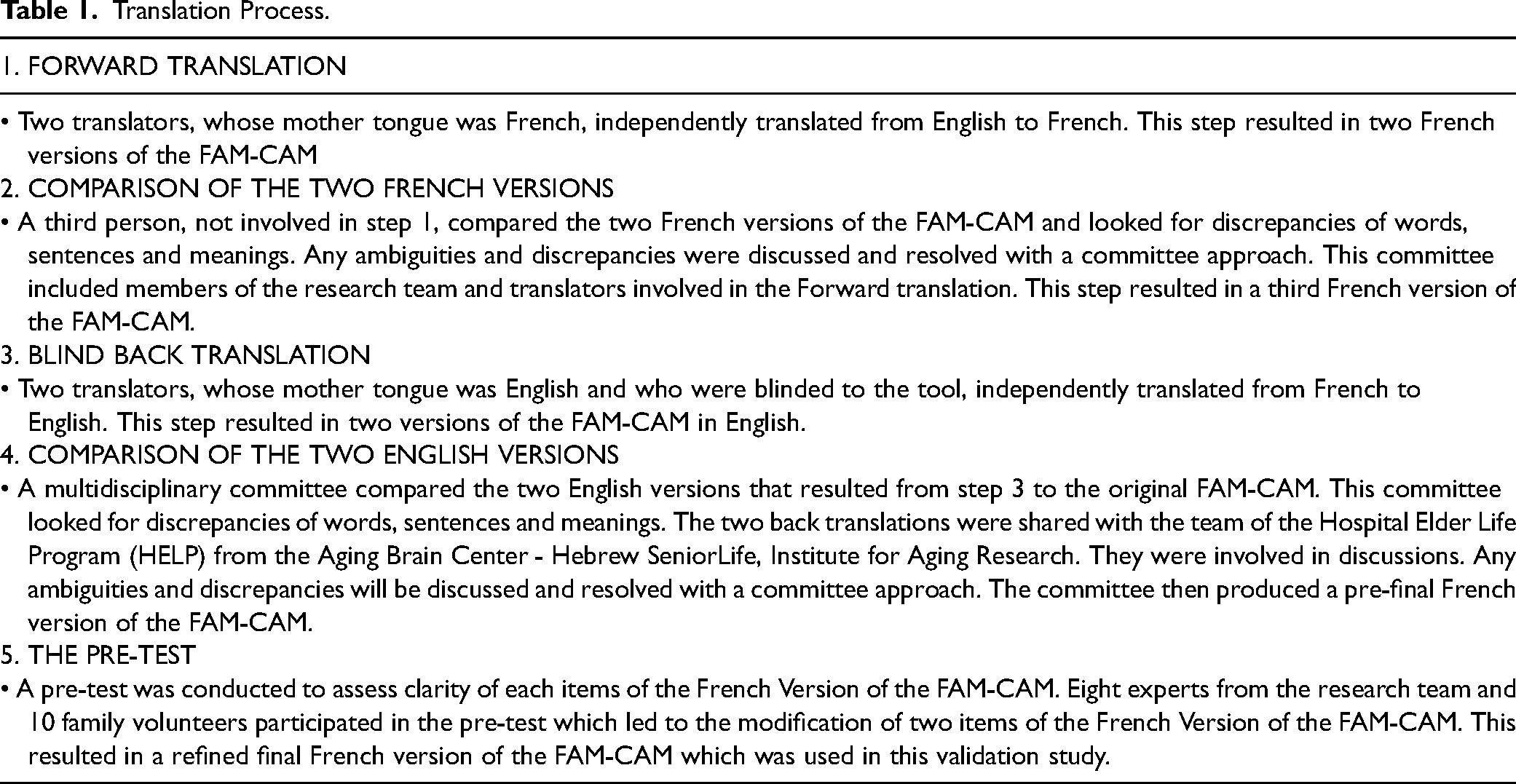
During step 2, a third individual, uninvolved in the initial translation, compared the two French versions to identify discrepancies in words, sentences, and meanings. A committee, comprising members of the research team and the original translators, discussed and resolved any ambiguities and differences, resulting in a unified third French version. Step 3 consisted in the blind back translation with two native English-speaking translators, who were blinded to the original FAM-CAM, independently translated the third French version back into English. This process generated two back-translated English versions for comparison. During step 4, a multidisciplinary committee compared the two back-translated English versions with the original FAM-CAM, carefully analyzing discrepancies in wording, sentence structure, and meaning. The Hospital Elder Life Program (HELP) team at the Aging Brain Center of Hebrew SeniorLife also reviewed these translations. Ambiguities were discussed, and discrepancies were resolved through a committee approach, leading to a pre-final French version.
The last step was a pre-test performed to assess the clarity and appropriateness. This pre-test was conducted with eight experts (i.e., researchers, clinicians, not members of the committee) from the research team and ten family volunteers who assessed the degree of clarity of the FAM-CAM-Fr version of the FAM-CAM. A rate of unclear of ≥ 20% resulted in the revision of the unclear item by the research team and committee members to further refine of the FAM-CAM-Fr. The FAM-CAM instructions were also translated and culturally adapted to the Canadian context during this process (Inouye et al., 2012). The FAM-CAM-Fr is covered under the original copyright and can be obtained from the HELP website (https://help.agscocare.org/login-required).
Secondary Objective: Criterion Validation of the FAM-CAM for French Speaking Populations of Canada
Study Sample
In this validation study, we included family caregivers and patients hospitalized in a specialized cardiovascular acute care hospital in Quebec, specifically on the cardiology unit. The family caregiver was defined as the individuals who provide support and with whom the patient has a significant relationship (Davidson et al., 2017). The family caregiver had to be 18 years old or older; understand and read French; have the capacity to provide informed consent; identify as a family caregiver (spouse, child, other family, friend) of an inpatient; have visited the patient at the hospital at least twice. The family caregiver also had to report having regular contact with the inpatient before hospitalization (≥ once a week). In the literature, this frequency of interaction was considered sufficient for the family member to report the usual cognitive and functional state of the patient, a knowledge necessary to be able to identify changes (Martins et al., 2014; Steis et al., 2012).
The hospitalized patient had to have the ability to provide informed consent or have a legal representative if their cognitive functioning was altered. Patients also had to present a stable clinical condition, allowing assessment of delirium.
Study Procedures
Following consent, data collection was performed at a time that was appropriate, i.e., either immediately following consent or later during hospitalization and included the completion of FAM-CAM-Fr by the family caregiver (described below) and CAM by the research nurse (described below). Both the FAM-CAM-Fr and CAM were to be completed within an hour of each other, independently and included information (i.e., changes in cognitive functioning or state of consciousness) over the last 24 h. – the family caregiver was asked to reflect on their interactions with the patient in the last 24 h and the project nurse completed the CAM based on their interview and on information from the charge nurse. The diagnosis and keywords were abstracted from the medical retrospectively. The project underwent scientific and ethics approval at the study hospital (2019–2426). The participants are identified by a code number. The key linking the name to the research file was kept by the lead researcher in an electronic file secured by a password.
Measures
Sociodemographic and Clinical Data
Among patients, the following data was collected from the medical chart by a research assistant: age, sex, education level, primary diagnosis for current hospitalization, medical history. Among family caregivers the following variables were collected from a self-reported questionnaire completed by families: Age, sex, mother tongue, level of education, relationship to the patient (friend, spouse, child, other), frequency of interactions with the patient and living situation with the patient (cohabitation, number of years), number and average duration of bedside visits during the present hospitalization.
Assessment of Delirium
Statistical Analysis
Sample Size
A sample size of 10 families for the primary objective and 100 dyads of family caregivers and patients for the secondary objective was deemed appropriate to attain the study objectives. Based on the results of a delirium study performed in the same clinical setting, it was estimated that 16% of subjects will present a positive diagnosis for delirium and 84% will be negative (Mailhot et al., 2017). We anticipated the sensitivity to be calculated on 16% of the total number of subjects. It was expected that the sensitivity could vary between 75% and 90% (Martins et al., 2014; Steis et al., 2012) we retained a sensitivity of 75% to be conservative. With a sample size of 100 (i.e., 16 true positives), the precision for the sensitivity estimate was of ± 21% with a 95% confidence interval. With this same sample size, the specificity was expected to be calculated on 84 subjects. Assuming a specificity of 85% (Martins et al., 2014; Steis et al., 2012), the precision for estimating the specificity would be 8% with a 95% confidence interval.
General Statistical Considerations
We used SPSS software 29 (Version 29.0.1.0; IBM SPSS Statistics for Windows Armonk, NY: IBM Corp.). Participants were presented using descriptive statistics with mean, standard deviation, median, minimum and maximum to describe the continuous variables, and frequencies and percentages to describe the categorical variables. The normality of continuous variables was assessed using the Shapiro–Wilk test. Sociodemographic and clinical data were contrasted according to CAM status. All statistical tests were bilateral and a significance level of 0.05 was used.
Descriptive statistics were also used to describe proportion of delirium based on the FAM-CAM-Fr, the diagnosis of delirium, the CAM and the keywords.
Primary Objective
Descriptive statistics were used to describe the results of the pretest on clarity of the FAM-CAM-Fr among the eight research team members and the ten family volunteers. The number of modified items for each round is also reported.
Secondary Objective
We assessed the sensitivity and specificity of the FAM-CAM-Fr by contrasting it to the reference standard (medical diagnosis according to DSM-5 criteria). Sensitivity was estimated by the proportion of FAM-CAM-Fr positives among the DSM-5 positives (true positives according to the reference standard) while the specificity was estimated by the proportion of negatives on the FAM-CAM-Fr among the negatives according to the DSM-5 (true negatives according to the reference standard). Sensitivity and specificity were presented with their 95% confidence intervals.
The following classification of assessments made with the FAM-CAM-Fr were also presented:
True positives (TP) were defined as being positive on the FAM-CAM-Fr matched with the presence of a delirium diagnosis; False positives (FP) were defined as positive on the FAM-CAM-Fr matched with no delirium diagnosis; True negatives (TN) were defined as negative on the FAM-CAM-Fr matched with no delirium diagnosis; False negatives (FN) were defined as negative on the FAM-CAM-Fr matched with the presence of a delirium diagnosis.
The same procedure was used to contrast the FAM-CAM-Fr to the CAM and the delirium key words. For the keywords, the use of any of the keywords was considered as a «yes». Finally, to assess the reliability FAM-CAM-Fr against the CAM and the keywords, Cohen's kappa were calculated. Cohen's Kappa quantifies the level of agreement beyond chance and is particularly suitable for categorical data, making it an appropriate measure for evaluating diagnostic concordance.
Finally, the accuracy of the FAM-CAM-Fr was calculated by computing the following: (true positives + true negatives) / N.
Results
Primary Objective of Translation and Cultural Adaptation
Eight experts evaluated the clarity of the items and instructions in the initial version of the FAM-CAM-Fr tool, comprising four researchers and four clinicians specialized in cardiovascular care. All items were rated as clear by these experts.
Additionally, ten family members assessed the clarity of the tool and instructions. Items rated as unclear by more than 20% of the family members included item 6 (n = 2, 20% rated this item as unclear) and item 11 (n = 3, 30%) from the tool, as well as item 1 (n = 2, 20%) and item 5 (n = 2, 20%) from the instructions. These items were subsequently refined and incorporated into the final version of the FAM-CAM-Fr.
Secondary Objective of Criterion Validation
A total of 100 dyads participated in the study and were recruited between July 2018 and June 2019, thus 100 family caregivers completed the FAM-CAM-Fr while the research nurse assessed the 100 corresponding patients with the CAM. As shown in Table 2, 19 patients (19%) were diagnosed with delirium. More than half of the participants were male, with an average age of around 75 years, and there were no significant differences in age, sex, or education between the delirium and non-delirium groups. Family caregivers visited their loved one who presented delirium more often per week compared to the group with no delirium (Table 2).
Sociodemographic Characteristics of Participants Stratified by Delirium Diagnosis.
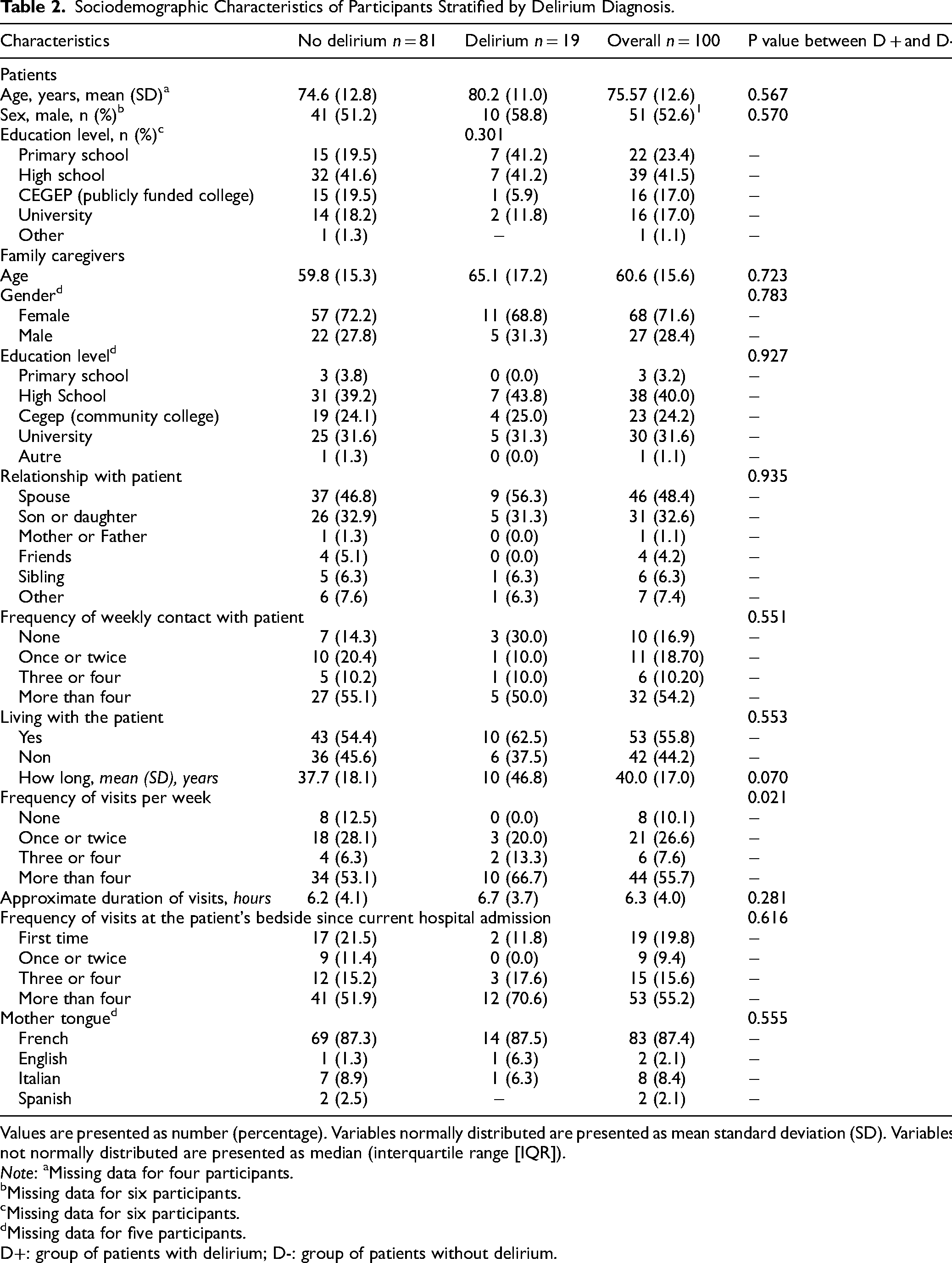
Values are presented as number (percentage). Variables normally distributed are presented as mean standard deviation (SD). Variables not normally distributed are presented as median (interquartile range [IQR]).
Note: aMissing data for four participants. bMissing data for six participants. cMissing data for six participants. dMissing data for five participants.
D+: group of patients with delirium; D-: group of patients without delirium.
Table 3 presents the FAM-CAM-Fr and CAM results according to delirium diagnosis. Overall, the sample included 19 patients with a diagnosis of delirium, 17 patients received a positive score on the FAM-CAM-Fr and 20 with a positive score on the CAM. Keywords were mentioned more frequently in the group of patients with delirium (Table 3), with ‘confusion,’ ‘agitation,’ and ‘drowsiness’ being the most cited keywords in this group.
FAM-CAM-Fr and CAM Results According to Delirium Diagnosis.
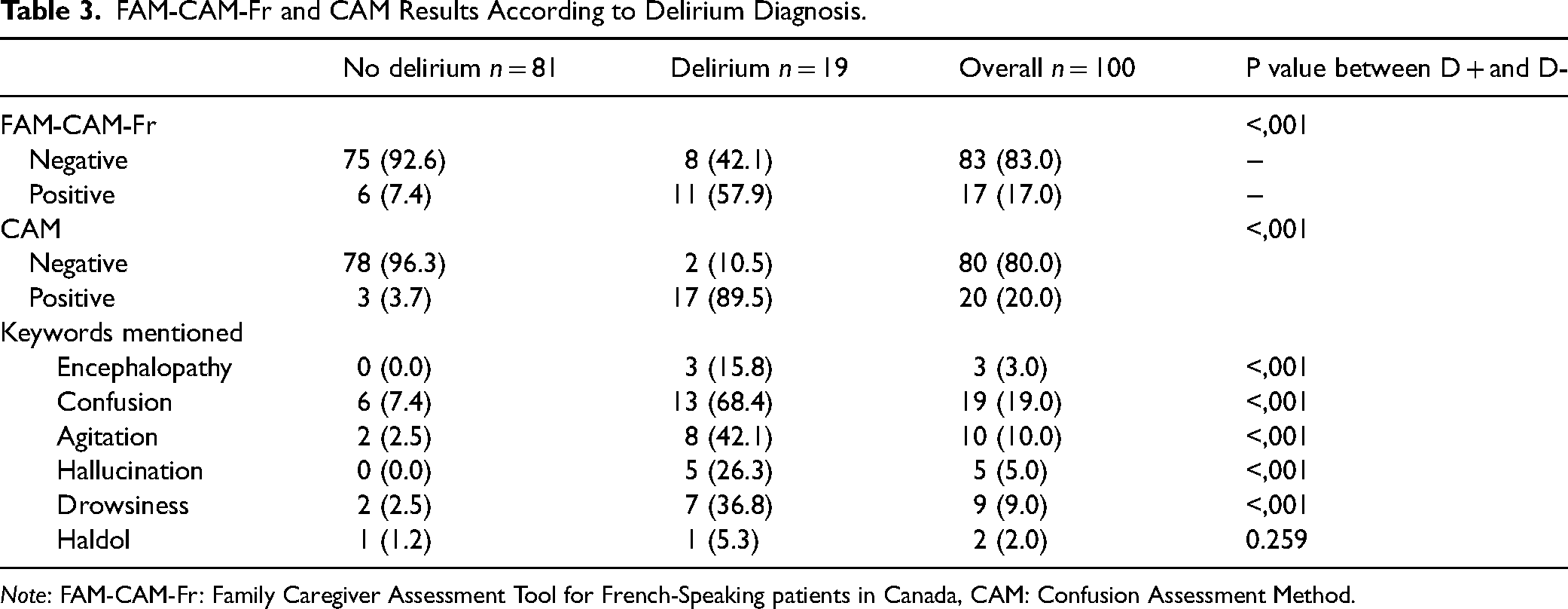
Note: FAM-CAM-Fr: Family Caregiver Assessment Tool for French-Speaking patients in Canada, CAM: Confusion Assessment Method.
The performance outcomes of the FAM-CAM-Fr are detailed in Table 4. Compared to the medical diagnosis, the FAM-CAM-Fr demonstrated low sensitivity (<60%) but high specificity (>90%), showing a similar performance when evaluated against the CAM. The Cohen's Kappa values for the agreement between the diagnosis of delirium and the FAM-CAM-Fr, as well as between the CAM and the FAM-CAM-Fr, were both greater than 0.50. Although the specificity of keywords was >90%, sensitivity was very low (<50%) and Cohen's kappa was the lowest. Finally, its accuracy was of 0.86.
Performance Outcome of the FAM-CAM-Fr.
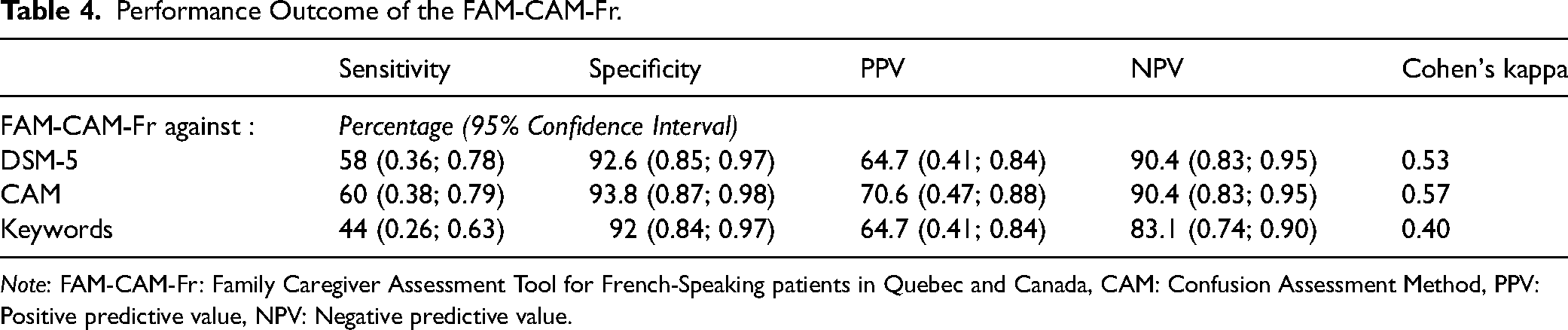
Note: FAM-CAM-Fr: Family Caregiver Assessment Tool for French-Speaking patients in Quebec and Canada, CAM: Confusion Assessment Method, PPV: Positive predictive value, NPV: Negative predictive value.
Discussion
The primary objective of this study was to translate and culturally adapt the original English version of the FAM-CAM for French-speaking cardiovascular patients in acute care settings in Canada. The FAM-CAM-Fr was developed through a rigorous process, involving expert input from translators, researchers, and family caregivers. Our results demonstrated low sensitivity but high specificity for the FAM-CAM-Fr, with moderate agreement with the reference standard and the CAM reference tool (McHugh, 2012). Notably, family caregivers administered the FAM-CAM-Fr without any specific training or detailed information about delirium provided by the research team. They relied solely on pamphlets available in the unit and the written instructions accompanying the tool. Despite this, the tool showed potential for enhancing delirium detection in clinical settings.
The performance metrics observed in our study are consistent with those reported for other versions of the FAM-CAM, though some variation exists. For example, studies by Steis et al. and Martins et al. reported higher sensitivity and specificity in different patient populations, indicating that contextual factors and caregiver training can influence the tool's effectiveness (Martins et al., 2014; Steis et al., 2012). Steis’ study included face-to-face sessions on how to use the FAM-CAM, offering education on each symptom and guidance on item scoring. In contrast, our study did not provide any training, aiming to test the FAM-CAM's validity under conditions more reflective of real-world cardiology practice. The improved sensitivity observed in studies with caregiver training suggests that structured education could enhance the tool's accuracy, particularly in high-risk populations such as older adults with pre-existing cognitive impairments. The rigorous validation of the German FAM-CAM, which demonstrated high sensitivity and specificity, further emphasizes the importance of cultural adaptation and methodological rigor in translating and validating tools (Greindl et al., 2022). While our study's sensitivity was lower, our specificity was comparable, suggesting the French FAM-CAM's robust potential in specific settings despite varying performance metrics across different populations and languages.
A systematic review and meta-analysis by Zhou et al. (2024) reported pooled sensitivity and specificity for the FAM-CAM at 0.74 and 0.91, respectively, based on data from 483 dyads across seven studies (Zhou et al., 2024). These studies primarily focused on older adults and critically ill populations. While our study's sensitivity was lower, the specificity was comparable, suggesting that the FAM-CAM can effectively rule out delirium across various populations and settings.
Studies included in Zhou et al., reported higher performance for various culturally adapted versions of the FAM-CAM (Table 5). For example, Steis et al. validated the original English version among families of older adults living in the community, while Martins et al. assessed the Portuguese version in a sample of critically ill patients. Xing et al. adapted and validated the Chinese version of the FAM-CAM in an ICU setting using a different reference standard. Bull et al. conducted their evaluation among non-cardiac surgery patients and reported levels of agreement comparable to our findings. Aside these translations, the FAM-CAM was translated into German. Greindl et al. used a prospective monocentric diagnostic study to validate the FAM-CAM in a 14-bed medical ICU of a university hospital in Germany (Greindl et al., 2022). The FAM-CAM was translated based on the Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes of the International Society for Pharmacoeconomics and Outcome Research (Wild et al., 2005) and involved three physicians specialized in ICU delirium. Cognitive debriefing interviews followed for the FAM-CAM's cultural adaptation with 28 participants, showing that the German FAM-CAM was understandable in the domain language and content. For the validation process, 50 dyads of critically ill patients and their family members were recruited. A summary of these studies, including the characteristics of the study populations, reference standards, and diagnostic performance metrics, is presented in Table 5.
Performance Outcome for the Original English Version of the FAM-CAM and for Translated and Culturally Adapted Versions of the FAM-CAM.
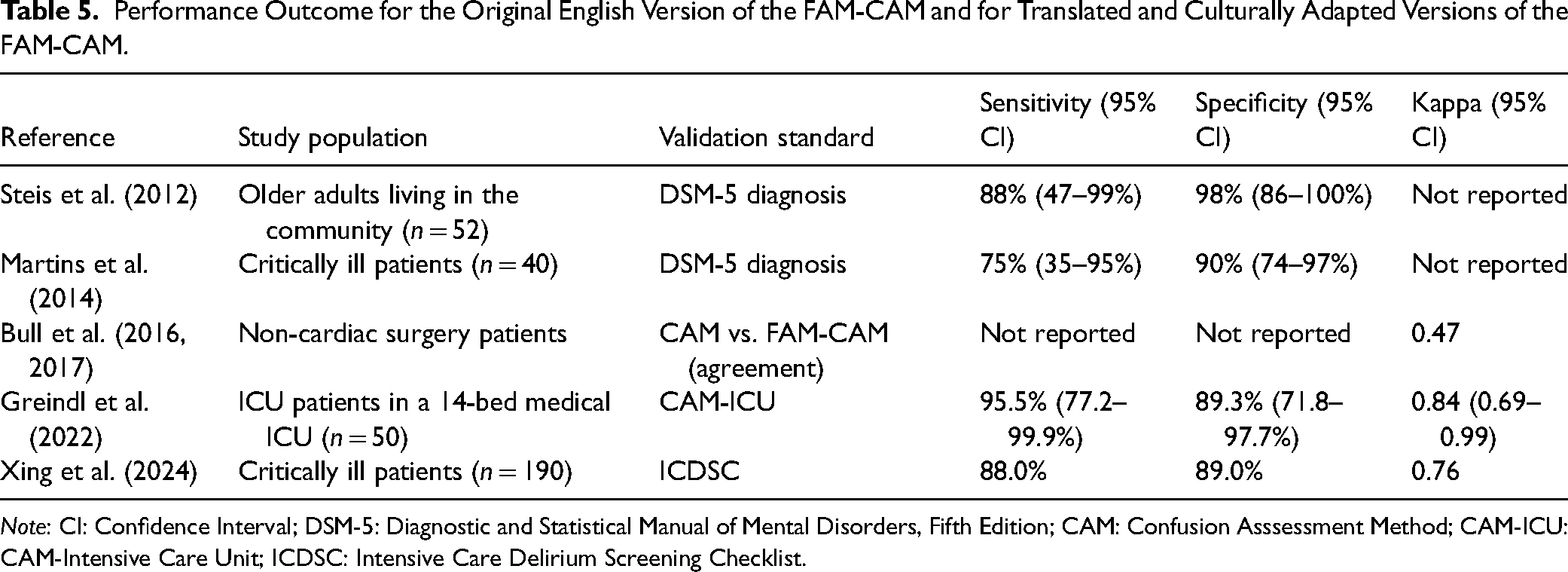
Note: CI: Confidence Interval; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; CAM: Confusion Asssessment Method; CAM-ICU: CAM-Intensive Care Unit; ICDSC: Intensive Care Delirium Screening Checklist.
These studies highlight the FAM-CAM's potential, though small sample sizes limit the precision of sensitivity and specificity estimates. Another key difference between our study and those by Steis and Martins is the level of training provided to families. For example, Steis’ study included face-to-face sessions on how to use the FAM-CAM, offering education on each symptom and guidance on item scoring. In contrast, our study did not provide any training, aiming to test the FAM-CAM's validity under conditions more reflective of real-world cardiology practice.
Despite advancements in delirium understanding, its detection in older cardiology patients, particularly those with pre-existing dementia, remains challenging (Shrestha & Fick, 2023). Delirium is often under-recognized in cardiology, despite its association with poor outcomes. There is growing interest in care models tailored to older adults or to adults presenting with delirium, which emphasize systematic mental status and delirium screening, alongside protocols for managing geriatric syndromes. Its integration into routine practice has the potential to inform national strategies aimed at improving delirium detection among French-speaking populations, thereby promoting equitable care across Canada. Given its ease of use, the FAM-CAM-Fr could be integrated into routine delirium screening in cardiology settings as a complementary tool alongside clinician-administered assessments. Implementing structured caregiver training programs could further optimize its accuracy while maintaining feasibility in clinical practice. Broad adoption of tools such as the FAM-CAM-Fr as part of standardized screening protocols could contribute to reducing the burden of delirium on the healthcare system, align with national geriatric care priorities and improve outcomes through earlier detection.
A limitation of this study is its conduct in a single cardiology unit, which may limit the generalizability of the findings. Additionally, we only included family members who had regular contact (≥ once a week) with the patient before hospitalization, potentially affecting the external validity of the FAM-CAM-Fr. Our patient population may have had undiagnosed cognitive impairments, complicating the detection of hypoactive delirium. Strengths of the study include the use of the CAM reference tool administered by trained staff blinded to caregiver responses on the FAM-CAM, providing a real-world validation of the tool in a cardiology setting. Moreover, the translation process followed a recognized and rigorous methodology.
Conclusion
In conclusion, our study resulted in the development of the FAM-CAM-Fr, a tool that may empower families to communicate observed changes in their hospitalized relative, thereby potentially enhancing delirium detection in cardiology settings. These findings are significant, as family caregivers completed the FAM-CAM without formal training or detailed information about delirium, underscoring the tool's potential to improve detection through the insights of family members, who are often most familiar with the patient's baseline cognitive function. Given the difficulties in identifying delirium, particularly in older cardiology patients with pre-existing dementia, the FAM-CAM offers a valuable and user-friendly screening option. In addition, structured family caregiver training programs should be considered to enhance screening accuracy and better incorporate the French version of the FAM-CAM into clinical workflows. Assessing the feasibility of implementing the French version of the FAM-CAM in routine practice would further strengthen its relevance in delirium detection strategies. Future research should prioritize multi-site validation of French version of the FAM-CAM across diverse clinical settings to enhance its generalizability and relevance. Investigating the impact of structured caregiver training on its diagnostic accuracy remains essential.
Supplemental Material
sj-doc-1-cjn-10.1177_08445621251350027 - Supplemental material for Translation, Adaptation, and Criterion Validation of the Family Caregiver Assessment Tool for French-Speaking Cardiovascular Patients in Canada (FAM-CAM-Fr)
Supplemental material, sj-doc-1-cjn-10.1177_08445621251350027 for Translation, Adaptation, and Criterion Validation of the Family Caregiver Assessment Tool for French-Speaking Cardiovascular Patients in Canada (FAM-CAM-Fr) by Tanya Mailhot, Zineb Bouaouina, Imène Khetir, Céline Gélinas, Judith Brouillette, Claudie Roussy, Stéphanie Jarry and Patrick Lavoie in Canadian Journal of Nursing Research
Footnotes
Author Contributions
T.M. contributed to the study concept and design, data acquisition, data analysis, interpretation of results, and manuscript preparation. Z.B. I.K. participated in data analysis and interpretation, as well as manuscript drafting. C.G., J.B., Z.B., I.K. and S.J. contributed to study design and critical revision of the manuscript. C.R., J.B. and P.L. contributed to study design, data interpretation, and provided critical revisions. All authors reviewed and approved the final version of the manuscript.
Sponsor's Role: NA.
Data Availability Statement
Data available on demand.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This project was approved by the Montreal Heart Institute ethics committee and all participants signed consent forms.
Funding
This study was supported by a grant from the Fond de Recherche du Québec- Santé, as well as institutional support from Montreal Heart Institute Foundation.
Preprint
This manuscript has not been previously published as a preprint.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.