
Abstract
Background
Access to primary care is a challenge across Canada. In the province of New Brunswick (NB), approximately 15% of citizens do not have a primary care provider (PCP). The Government of NB recently implemented clinics staffed by nurse practitioners (NPs) in various regions in the province to reduce the provincial waitlist for a PCP.
Purpose
This study aimed to identify facilitators and barriers to NP-led clinic implementation, as perceived by clinic staff.
Methods
Using a cross-sectional qualitative descriptive design, data was collected using semi-structured interviews and analysed using qualitative content analysis.
Results
Study participants included 16 employes of two NP-led clinics in NB (NPs, registered nurses (RN), licensed practical nurses (LPN), administrative staff, and managerial staff). Facilitators include having experienced mentors, collaborative practices, and well-equipped clinics. Barriers include rushed timelines, complex decision-making processes, large and complex caseloads, inadequate clinic space, and difficulty in staff recruitment and retention. Participants discussed the positive impact of NP-led clinics through improved access to primary care, resulting in reduced burdens on emergency departments and walk-in clinics. Participants recommend adding additional NP-led clinics and integrating multidisciplinary allied health professional teams to enhance care integration.
Conclusion
NP-led clinics are increasingly being implemented across Canada to improve primary care access, particularly in areas where there are shortages of PCPs. Findings from this study will help inform the development and implementation of other NP-led clinics across NB and Canada.
Background
Access to primary care is challenging in Canada due to multiple factors, such as shortages of healthcare providers, geographical barriers, socioeconomic disparities, and fragmented care systems (Martin et al., 2018). Primary care refers to the first point of contact individuals have with the health care system, providing access to essential health services such as diagnosis, treatment, and ongoing care. It typically involves generalists like family physicians, nurse practitioners, and other health professionals and focuses on prevention, health promotion, treatment of common illnesses, management of chronic diseases, and coordination with specialized services (Hutchison et al., 2011; Starfield & Macinko, 2005). One in six Canadians report not having a regular primary care provider (PCP), and less than half of Canadians are able to see a PCP on the same or next day (Flood et al., 2023). In the Canadian province of New Brunswick (NB), primary care accessibility is a growing concern. The latest survey conducted by the New Brunswick Health Council (NBHC, 2022) indicates that while 85% of New Brunswickers have access to a PCP, only one in three can secure an appointment within five days. This reflects a significant decline from the previous year, where 90% reported having access to a PCP and 51% could obtain an appointment within the same timeframe (NBHC, 2022). This barrier to access increases demand at local walk-in clinics and causes patients to seek care at emergency departments (ED) for non-urgent conditions. As a result, both walk-in clinics and EDs experience longer wait-times and reduced accessibility to care (NBHC, 2022; O'Cathain et al., 2020). Considering these potential issues with access to care, receiving timely attention from a PCP is the preferred option for most non-urgent health care needs (NBHC, 2022).
Across North America, NPs are increasingly meeting the demand for primary care services, delivering high-quality, cost-effective health care, with high patient satisfaction (Black et al., 2020; Liu et al., 2020; Marceau et al., 2020; Marceau et al., 2021; O’Byrne et al., 2020). NPs in NB are advanced practice registered nurses who have successfully completed a masters-level, university-based NP program and are licensed to practice as primary care NPs (Heale et al., 2018; Marceau et al., 2020; O’Byrne et al., 2020). In 2024, 7,841 NPs were employed in direct patient care across Canada, marking a 10% growth from the previous year (Canadian Institute for Health Information, 2024). The majority of NPs work in community health care settings or hospitals and their scope of practice varies across provinces and territories (Canadian Institute for Health Information, 2024). In NB, 421 NPs are licensed and the majority work in salaried group practices (New Brunswick Department of Health, 2024). NP scope of practice includes advanced assessments, diagnosis, prescribing, and patient management. However, their ability to prescribe controlled substances is limited, and they lack full hospital privileges and the authority to perform involuntary admissions (Canadian Institute for Health Information, 2020; Nurse Practitioner Association of Canada, 2024).
In response to ongoing challenges with primary care access, the Government of NB implemented new primary care clinics staffed by NPs throughout the province beginning in 2020. Although NPs have been practicing in NB since 2003 (Government of New Brunswick, 2018; Canadian Nurses Association, 2006), NP-led clinics represent a new primary care model in the province, designed to address provincial waitlists for PCPs. Unlike traditional clinic models led by physicians, NP-led clinics feature NPs at the forefront, offering primary care to patients (Heale et al., 2018). At the time this study was conducted there were three NP-led clinics in NB, situated in the province's three major cities. These clinics are publicly funded and governed by one of two regional health authorities (RHA), depending on their health zone (New Brunswick Department of Health, 2024). In addition to providing accessible primary care, NP-led clinics aim to improve continuity and comprehensiveness of care by facilitating better health system navigation and care coordination, linking patients to other services within the healthcare system (Black et al., 2020; Heale et al., 2018).
While research on community-based clinics in Atlantic Canada has examined settings where NPs provide primary care, these studies typically focus on models where NPs work alongside physicians as part of broader healthcare teams (Curnew & Lukewich, 2018; Johnson et al., 2024). There is limited research specifically examining NP-led clinics, particularly from the perspective of clinic staff. Given that NP-led clinics in NB were recently introduced to address the shortage of PCPs, it is essential to understand the facilitators and barriers influencing their implementation. By exploring the experiences of NP-led clinic staff, this study fills a critical gap in knowledge. These findings will contribute to evidence-based policy decisions and inform the ongoing development of NP-led primary care models across Canada.
The Current Study
The primary goal of the current study was to explore staff experiences during the implementation of two NP-led clinics in NB, Canada. Three NP-led clinics were invited to participate in this study. However, only two clinics took part, one clinic from each RHA in the province. Our study addressed the two following research questions:
What are the facilitators and barriers to NP-led clinic implementation perceived by clinic staff? What are the recommendations of clinic staff for improving NP-led clinic implementation?
Methods
Design
We used a cross-sectional qualitative descriptive design to explore staff experiences with the implementation of NP-led clinics in NB (Bradshaw et al., 2017; Kim et al., 2017). This method allowed us to clearly and accurately summarize participants’ experiences, staying closely connected to the data with minimal interpretation (Bradshaw et al., 2017; Kim et al., 2017). Data was collected using semi-structured interviews and this data was analysed using qualitative content analysis (Graneheim et al., 2017; Vaismoradi et al., 2013; Vaismoradi & Snelgrove, 2019). Rooted in critical realism, our approach emphasizes participants’ subjective experiences, while recognizing the limitations and potential biases inherent in our observations and interpretations (Fletcher, 2017; Willis, 2023).
Sample
Study participants included 16 current and former employes of two NP-led clinics in NB. These participants included nurse practitioners (NP), registered nurses (RN), licensed practical nurses (LPN), as well as administrative staff and managerial staff.
Data Collection
Ethics approval was granted by the institutional review boards of the host academic institutions and the RHAs. Data collection took place between September 2021 and January 2022. Purposive sampling was used to recruit staff members to participate in this study. A recruitment email was distributed to all staff members at the two NP-led clinics by the managerial staff. This email included information about the study, as well as the contact information of a member of the research team for interested participants to contact.
Data was collected using a semi-structured interview developed by the research team and piloted with a healthcare professional. The interview included questions relating to the planning, set-up, and operation of the clinic (e.g., staffing structure, resource use, patient load), as well as questions around recommendations for the implementation of other NP-led clinics in NB. In line with our qualitative descriptive approach, the interview guide was designed to capture detailed descriptions of staff experiences during the implementation process, focusing on the “who, what, and where” of these experiences (Kim et al., 2017). The interviews were conducted by members of the research team (KL, SB, and EJ) in the language of the participant's choice (English or French). Participants met with the interviewer virtually over the phone or through the Zoom video-conference platform, depending on participant preference. All interview participants were sent an informed consent form electronically prior to the interview and were asked to provide either a valid electronic signature or audio-recorded verbal consent before proceeding with the interview questions. Participants who completed the interview were entered into a draw to win one of two $50 Amazon gift cards.
Data Analysis
The interviews were transcribed verbatim by a trained research assistant. The audio recordings and interview transcriptions were reviewed by the interviewer, to ensure accuracy of the data. All interview transcripts were uploaded to NVivo 12 software for review, organization, and analysis. Qualitative content analysis was used to examine the interview data (Graneheim et al., 2017; Vaismoradi et al., 2013; Vaismoradi & Snelgrove, 2019). Three members of the research team (LM, KL, and SB) worked together to generate initial codes and to develop a coding guide. The entire data set was analyzed independently by at least two members of the research team (LM, KL, and SB) and then the coded transcripts were merged for comparison. Discrepancies in coding were discussed and resolved by consensus. Categories were developed using both inductive and deductive qualitative content analysis, which allowed us to organize data with and without preexisting categories (Elo & Kyngäs, 2008; Graneheim et al., 2017). A deductive content analysis was informed by the research questions and the interview guide, which provided preexisting categories for organizing the data. Specifically, main categories such as facilitators and barriers to clinic implementation, impact, and recommendations were identified deductively. In contrast, subcategories were developed inductively from the interview content itself (Elo & Kyngäs, 2008; Graneheim et al., 2017). The qualitative findings are presented using these categories. Interview data collected in French was translated into English for reporting, and filler words (e.g., “um”, “uh”) were omitted to improve readability when presenting direct quotes as evidence.
Results
Study participants shared insights into the facilitators and barriers encountered during both the set-up and operation of the clinics. They also reflected on the clinic's impact on the community, particularly in improving access to primary care. Additionally, participants provided personal recommendations for future NP-led clinic implementation, emphasizing the need to expand the number of NP-led clinics in NB and strengthen connections with other health and social care providers across clinics (see Figure 1).
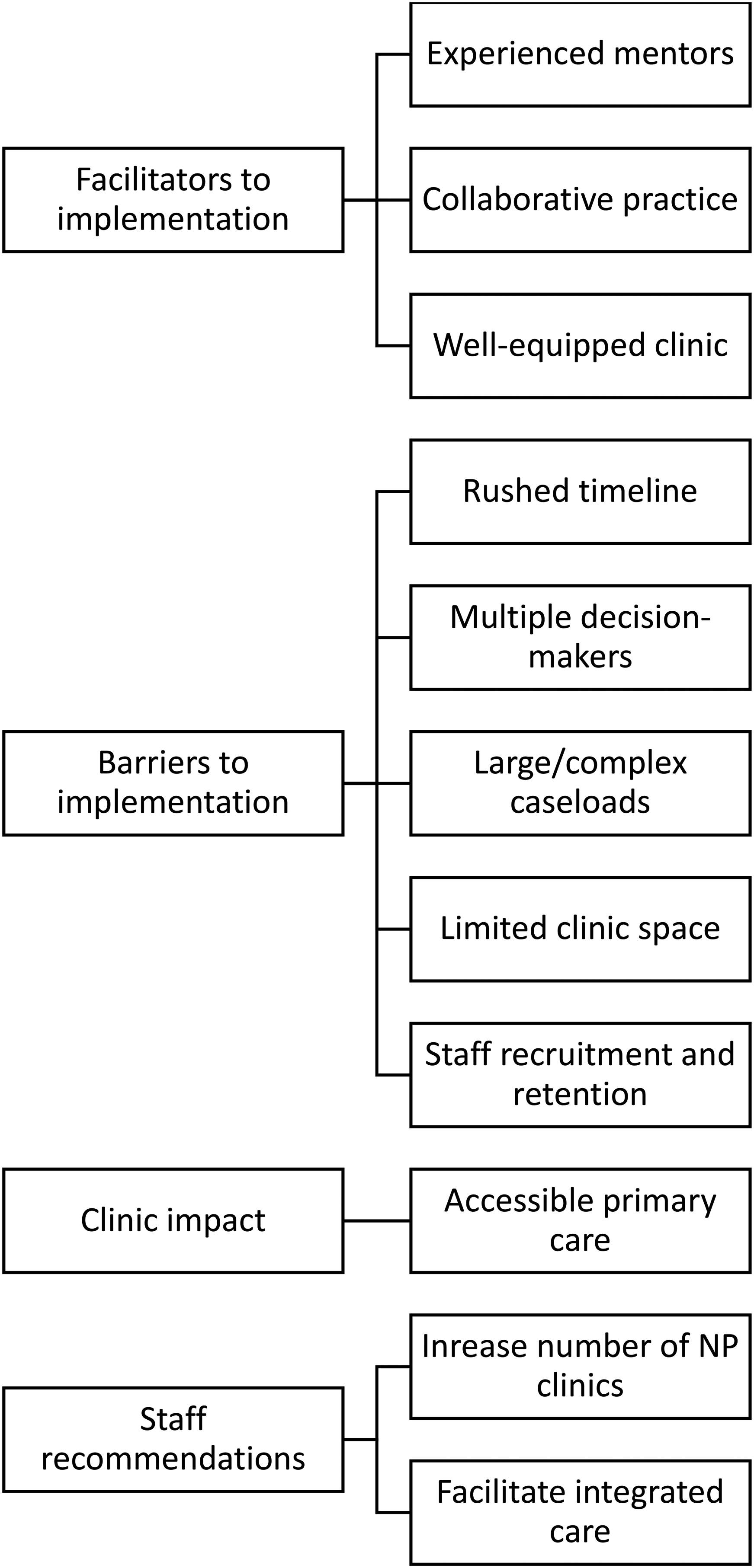
Content analysis category map.
Participant Demographics
Across the two NP-led clinics, 15 current staff members and 1 former staff member took part in the study (8 NPs, 2 RNs, 4 LPNs and 2 administrative staff members). The length of time participants had been practicing in their professional role ranged from 7 months to 26 years. The length of time participants worked at the NP-led clinic ranged from 4 months to 1.5 years. Most of these participants had been involved in the set-up of the clinic, while four participants had joined the staff shortly after set-up.
Facilitators to Clinic Implementation
Facilitators to program implementation included: having experienced mentors, a collaborative practice, and a well-equipped clinic.
Experienced Mentors
Support from colleagues was seen as a facilitator to the clinic implementation process, particularly having experienced NPs involved at the time of clinic set-up. Experienced NPs could draw on their backgrounds and expertise to help other NPs and could build on their previous experiences to help throughout the clinic implementation. For example, one participant said: You know [colleague's name] has a lot of experience and she helps us a lot, she helped us figure out a lot of new things. So, that's it, having people who have experience, I think that's important, I think that if you open a new clinic, you need to have at least one or two NPs that have more than a year of experience. (Participant 07) [The manager] was helpful with setting it up and we had a couple of people over from different clinics helping us set up some of the things… like the processes… how we’re faxing things and prescriptions and things like that, we got a lot of that from the [other clinic name] and how they operate, and just copied how they do their processes and brought it over here. (Participant 15)
Collaborative Practice
Following a team-based approach was viewed as a facilitator to clinic implementation. NPs appreciated receiving support from fellow NPs and other nursing staff for many reasons, such as helping with large caseloads, consulting for complex cases, and supporting each other in the process of implementing the clinics. For example, NPs mentioned that LPNs and RNs, when working to their full scope of practice, made patient care more efficient and helped NPs take on a larger caseload. One participant stated: “LPNs and the nurses involved, it helps relieve the weight of the tasks, that's nice. I like the collaboration between the different positions” (Participant 06). Having team members with different backgrounds and areas of expertise was also viewed as a facilitator. For example, a participant mentioned: And in terms of RNs, we had different medical pasts, so we know there is one who is an expert in emergency, there is one who is a specialist in infectious diseases, one is more into intensive care, pediatrics, so it's fun, we have a little multi-team between all of us. (Participant 08)
Well-equipped Clinic
Participants felt they had access to a wide range of appropriate technology, equipment, and supplies at the clinics. For example, participants liked having the ability to perform blood tests at the clinics and appreciated having the most up to date equipment and supplies for other in-office procedures (e.g., wound care, reproductive care). For example, one participant stated: I’m super satisfied with the equipment. We have top-notch brand-new equipment. I can’t say anything bad about it. [Colleague's name] performs so many procedures, so she thinks of everything we need to order, everything, sometimes I’m even like: ‘Oh wow, we even have this!’. (Participant 07) Everything is brand new, up to par in terms of expiry dates and manufacture data. Things are checked on a weekly basis. Supplies are stocked on a weekly basis. Anything that I’ve needed, in fact I feel spoiled because anything I’ve needed is there. If I were ever at the point where I felt I would need to work anywhere else, I would be lost a little bit because it's so well organized that way. (Participant 09)
Barriers to Clinic Implementation
Barriers to implementation consisted of rushed timelines for implementation, multiple decision-makers during clinic set-up, large and complex caseloads, limited clinic space, and issues with staff recruitment and retention.
Rushed Timeline
The participants indicated that they felt the clinic implementation was difficult due to how rushed the clinic set up was. Staff felt that they had to open quickly and “jump in” before being ready. In the case of one clinic, they had to open at a temporary location, which also brought challenges, including offices that were not adapted to health care delivery, (e.g., inadequate space, no desks, carpeted flooring). For example, one participant stated: [That] was the temporary location we had at first, if we could go back and do it again, I would have done it differently and gone directly to the current clinic because the temporary location had carpets, it wasn’t very sanitary… and it was really like… you were doing a Pap-test and couldn’t wash your hands. I feel like it would have been better if they had waited for it (the current location) to be ready before moving in. (Participant 06)
Multiple Decision-makers
Having multiple stakeholders involved (provincial government, minister of health, health authorities, etc.) made decision-making more time consuming. Moreover, these stakeholders had different interests, goals, and values for the clinic which rendered the task more difficult. For example, one participant said: “The biggest barrier was just there's too many hands in the pot and no one wanted to make a decision…it just seemed like…when you wanted something done it has to go through four people” (Participant 12). Additionally, staff felt that their voices and opinions were not taken into consideration in the decision-making process. NPs voiced concerns over having an NP-led clinic without NPs as part of the management staff. One participant mentioned: Obviously, it would have been nice before we started this clinic to have more practitioner input cause [sic], I think it would have looked a lot different, but I guess overall I’m happy to be here… I enjoy the job. I think there could have been some changes that could have been foreseen. (Participant 14) Even when it came to decision-making when building the new clinic, when we brought certain things up, like having two NPs in one office to answer phone calls and fill out paperwork. Well, you know we’re often talking to specialists, so there were two people per room hearing everything the other person is saying. [It] isn’t ideal, and it was really small. They (decision-makers during clinic set-up) didn’t want to make any changes even though it was the right time to do it, before the plan was already made. In the end, as NPs we understand how things work, we knew they (offices) wouldn’t work well that way. It's fine but less than ideal for confidentiality and everything, but you know if the managers had been NPs, it would have been different because they would have understood. (Participant 06)
Large and Complex Caseloads
Workload was a recurring theme in barriers to clinic implementation. The goal set by the government was to see a substantial decrease in the provincial registry of unattached patients and there was constant pressure to meet this goal. NPs felt like they were constantly opening new files, with some of these patients having been on the provincial registry of unattached patients for a long time or coming from different provinces or countries. The patients were often complex and had many health conditions, resulting in increased time and effort to open these new files. For example, one participant said: Some of these orphan patients… what I see from when I came in April is that these NPs have their patients but they’re all [complex cases], they haven’t had appropriate medical care in a year, two years, three years because they’ve been orphaned. You can’t just go to the ER and be like I need my normal bloodwork for this year cause they’re not gonna [sic] do it. (Participant 01) It was hard because we were trying to open so many files and we had so much paperwork and it felt like they (decision-makers) didn’t want to understand because all they looked at were the numbers, how many patients they saw and everything. When you open files, it's fine when the person is young and doesn’t have any health problems but when you open a file for someone who has traveled elsewhere and has many health problems, it takes time, a lot of paperwork, you have to go through their health records. (Participant 06)
At one of the clinics, the caseload size was also related to the redirection of emergency department (ED) patients to the NP-led clinic, which was implemented as part of the clinic mandate. This program was put in place for patients that were triaged as non-urgent at a hospital under the same regional health authority. ED triage nurses could, when they considered appropriate, redirect patients to the NP-led clinic for evaluation and/or treatment. This ED redirection program means that NPs have less time in their schedule to see their rostered patients, and that their patients may have to see other NPs, consequently affecting continuity of care for the patients. One participant stated: With this introduction of the ER program, it limits our time so even if all of my colleagues are in office and practicing, they may not be available for when their own patients are available because they have to use the time for the ER and then unnecessarily the patient is redirected to another provider that may or may not be familiar with [the patient] and the provider may or may not be familiar with the current treatment plan. So, in my opinion it does actually interrupt the continuity of care for the patients. (Participant 02) With the redirection of emergencies, those sort of eat up some spots that my caseload otherwise cannot access. So, it's great that we are accessing people without primary care providers from the emergency room but a lot of the time a lot of people that we’re seeing through the emergency departments have family doctors, so, I feel like I’m seeing people who have family doctors and those people are sort of eating up the spaces of room where I cannot see my own patients, their own needs. So, it's sort of bittersweet. (Participant 09)
Limited Clinic Space
Most participants noted that the physical clinic space was a barrier to clinic operation, particularly that sharing office space was a barrier to providing proper care. NPs mentioned that sharing their office with other NPs resulted in confidentiality and communication issues while communicating with patients via telephone or when communicating with other health professionals about patients. Moreover, the number of exam rooms as well as the design and size of the rooms were considered inadequate. For example, one participant stated: Yes, they are expanding but it's not going to give us much more room because the space is going to [another program] and all those programs that are being added-on will have a few rooms as well, so it doesn’t leave the NPs with much space. They say we will be able to borrow them, but I feel like we’ll always need them because we’re not even fully staffed yet and there are days where I look around and all the doors are closed, all the rooms are busy, so I know that when we go back to full staff, it won’t work. It's just that it’ll be the patients who will be asked to wait longer in the waiting room, there will be delays. I just think it's not thought through very well. (Participant 07) This clinic is too small for our needs. We only have seven rooms, so our nurse practitioners do virtual days to kind of, make it so it's not so congested in here cause [sic] even on the days we have three NPs in, we have the rooms full. (Participant 11)
Staff Recruitment and Retention
Recruitment and retention of staff, especially NPs, was seen as challenging by many participants. Participants mentioned that staff members chose to leave for many different reasons, including wanting better salaries, better benefits, jobs with less pressures and/or responsibilities, or getting better support to take on their responsibilities. Continuous short staffing and vacant positions made working conditions more difficult and made it harder to reach quotas. For example, NPs shared instances where they had to assume responsibility for patients who found themselves without a healthcare provider following the departure of their NP from the clinic, due to resignations or parental leaves. One participant shared: There are some jobs that have been posted, maternity leaves not yet filled. So right now, those of us who are currently working are just picking up the slack. So right now, I feel like it's not good, but I understand that it's only temporary until I guess some dust settles with the hiring process, big decisions and these maternity leaves returning, so, should we be fully manned with the FTE's that are allocated, I think that it would be functioning very well, very smoothly. We briefly saw that [earlier] this year! (Participant 09)
Administrative support was also an area where there was high staff turnover. One participant stated: Yes, yes, a big turnover. We had [two] of them (administrative staff) that just… left…, we had one full timer who left for another job, we had another one who just found out she got another job elsewhere, there's one who had a temporary position, so she also left, so, in terms of clerks, we’ve had a lot. It's a mess. (Participant 10) [Administrative staff] are doing… a lot. And sometimes there's one clerical for three of us (NPs). They’re supposed to be registering people when they show up, faxing their orders, those are the most acute things they need to manage. Answering the phone when people call to book appointments, and they’re also supposed to be filling out my schedule with meet and greets for later, it's not realistic. (Participant 16)
Impact of Clinic
Accessible Primary Care
All the participants agreed that one of the most positive impacts of the clinic was that it made primary care more accessible to the population. In addition to reducing the provincial registry of unattached patients, participants believed the clinic also contributed to relieving the pressure in our healthcare system and reducing the burden on walk-in clinics and the ED. For example, one participant stated: I think that we definitely increased the availability of services for primary care patients. When I began, our file numbers started in the high 2000's and the other day I opened a file, and it was somewhere in the 6000. In four months, [that is] 4000- give or take- files that have been opened between us. Of course, those files do include some of the re-orientations from the [ED]. Not many, but I would say we have registered close to 4000 patients in 6 months, so that has certainly increased the availability of primary care to the citizens of [city name]. (Participant 02) I think it's huge, I think it's been received really, really well. I know personally I have about six hundred out of the eight hundred patients rostered that I’m gonna [sic] take, and I don’t know where the other clinicians are, but I think everybody's in the hundreds anyway. So, I think that patients are super happy… and overall, it's a really positive thing. (Participant 14) I think it's done amazing things for sexual health. We do a lot of sexual health appointments, and I feel like that's very needed in this city. Same with taking patients off the patient connect list (provincial registry for unattached patients) there's a ton of patients without providers, who have a ton of different things going on that need to be looked at by a healthcare provider. So, I feel like we’ve done really well with the amount of people that we’ve taken on and the care that we’ve given to them. (Participant 15)
Staff Recommendations
Participants made recommendations for future NP-led clinic implementation. This included adding additional NP-led clinics and integrating multidisciplinary allied health professional teams to enhance care coordination and comprehensiveness.
Increase the Number of NP-led Clinics
Participants viewed NP-led clinics to be very beneficial for the population and wanted to see more of these clinics implemented. Participants mentioned that despite actively taking many patients off the provincial registry of unattached patients, more patients keep getting added to the list. One participant mentioned: “We’re at a point where even if we take 8000 people off the list, there will still be some left on the list, and more to be added to it” (Participant 03). Participants also mentioned that there are more areas in the province that would benefit from NP-led clinic implementation (e.g., rural areas). For example, one participant said: In small rural areas like Campbellton, they always have a hard time, that's where I come from. You know like, obstetric nursing, you haven’t been able to give birth in that region since forever. They’re always looking for family doctors, it would be great to have a clinic like this. (Participant 03) Especially I think when you look at some of the smaller communities, especially whose healthcare's like Sussex and Shediac and all those places and Sackville, [where] hospitals are closing on the weekends due to nursing [shortages], I think that if you had these clinics more readily available people would be able to get primary health care and they wouldn’t be in the ER so much. (Participant 12)
Facilitate Integrated Care
Clinic staff recognized the benefit of coordinated, multidisciplinary teams and recommended expanding services offered by the clinics to include a variety of allied health professionals. For example, one participant said: I also think having a few allied health professionals would be awesome, but I would love to have a dietician, and a counsellor. Those would be my big ones. A physio would be great. We do all of these things in house, and it’d be way better collaboration, but there's no way we could do that here, there's not enough room. (Participant 06) ‘Hey here's a pool of social work, here's a pool of dietitians in the city’, we don’t actually have to necessarily even have them in our clinic. But better access instead of just having access to maybe one of them… that would probably be super beneficial. (Participant 03)
Discussion
This study explored staff experiences with and recommendations for NP-led clinic implementation in NB, Canada. NP-led clinic staff members in the current study identified facilitators to clinic implementation such as having experienced mentors, being equipped with the appropriate tools and technology to deliver care, and having a team-based approach to service delivery. Barriers to clinic implementation included rushed timelines, multiple decision-makers, large and complex caseloads, constraints in clinic space, and challenges with recruitment and retention. Participants emphasized the importance of expanding the number of NP-led clinics across the province and underscored the importance of integrated care.
Facilitators to Clinic Implementation
Staff members identified facilitators that contributed to the successful implementation of NP-led clinics. Most importantly, participants described the importance of working alongside others, within a collaborative practice and with experienced mentors. Indeed, the presence of experienced mentors played a crucial role in guiding NP-led clinic staff through the complexities of their roles and responsibilities. These results align with previous studies that identified mentorship as integral to the professional development of new NPs, helping new practitioners navigate clinical challenges and develop necessary competencies (Barker & Kelley, 2020; Rioux-Dubois & Perron, 2023). The emphasis on a team-based approach to service delivery underscores the importance of collaborative practice within NP-led clinics. Indeed, the importance of cultivating a collaborative, intra-professional community of practice within NP-led clinics has been long established and research has demonstrated that such collaborative efforts benefit NPs in terms of professional development and integration into the workplace (Burgess & Sawchenko, 2011; Tori et al., 2023). Moreover, collaboration across nursing roles, particularly with RNs and LPNs, is considered crucial (Prentice et al., 2020). Therefore, emphasizing team-based care delivery in NP-led clinics not only promotes mentorship, but also strengthens the broader collaborative practices essential for effective healthcare service delivery. Further research is needed to explore how NPs collaborate with other nursing professionals, such as RNs and LPNs, in NP-led primary care settings.
Interprofessional collaboration was recognized as a key factor in enhancing patient care. In this study, the NP-led clinic staff suggested that incorporating allied health professionals into their team would be highly beneficial, or at the very least, they could strengthen their connections with other care providers in the community. Indeed, interprofessional teamwork fosters synergistic relationships among healthcare professionals, promotes holistic care, and maximizes the utilization of each team member's expertise (Heale et al., 2018; Torrens et al., 2020). By leveraging the diverse skills and perspectives within the team, NP-led clinics could address the multifaceted needs of their patient population more effectively.
Barriers to Clinic Implementation
Despite the potential benefits of NP-led clinics, several barriers were identified that impeded their successful implementation. One significant challenge highlighted by staff members was the presence of rushed timelines during the initial setup phase. Limited timeframes may lead to inadequate preparation and planning, increasing the risk of operational inefficiencies and staff dissatisfaction (Martin et al., 2018). Moreover, the involvement of multiple decision-makers in the implementation process can result in conflicting priorities and delays in decision-making. Clear communication channels and streamlined decision-making structures are essential to navigate bureaucratic complexities and ensure the timely execution of clinic initiatives. Furthermore, participants that were not in managerial positions expressed feeling excluded from the decision-making process, noting that their views and opinions could have been valuable. This sentiment aligns with the findings from a recent scoping review, which concluded that the sustainability of advanced practitioner roles hinges on adequate organizational support to facilitate effective leadership (Elliott et al., 2016). The review underscored that enhancing leadership capacity relies on implementing organizational-level strategies and support mechanisms for nurses in advanced practitioner roles (Elliott et al., 2016).
The issue of large and complex caseloads posed a considerable challenge for NP-led clinic staff in the current study, affecting their ability to deliver comprehensive care within the constraints of available resources. Addressing workload management strategies and optimizing patient panel sizes are crucial considerations to prevent burnout and maintain service quality (Martin-Misener et al., 2016, 2024). NPs in the current study shared that they were overwhelmed by the constant pressure to open new case files. Furthermore, they felt that the focus was solely on the number of patients, without considering the complexity of these patients. Recent research emphasizes the significance of accounting for patient acuity level or disease burden score when determining appropriate caseloads for NPs (Martin-Misener et al., 2016, 2024). Shekelle et al. (2020) adds that the panel size should be shaped by diverse factors such as differing time requirements of patients, demographic and health indicators, the resources available to providers including the number of exam rooms, task delegation capacities, clinical staff support, and the integration of telehealth services. A more recent review highlights various factors that influence patient panel size, including factors related to the healthcare system, provider preference, patient characteristics, and considerations for the interprofessional team collaboration (Harrington, 2022).
NP-led clinic staff in the current study expressed concern regarding staff recruitment and retention, among administrative and clinical staff. It was observed that staff shortages made it more difficult to handle large caseloads and organize feasible schedules, including time off, for the existing staff. These findings align with research studies examining NP recruitment and retention in primary care. One consistent trend is the need to provide opportunities for professional growth and autonomy within the NP role. Studies suggest that NPs are more likely to stay in positions where they have a higher degree of autonomy and involvement in decision-making processes (Hagan & Curtis, 2018; Nowrouzi et al., 2015; Poghosyan et al., 2017). Furthermore, understanding the challenges of the work environment, such as staff shortages and heavy caseloads, is essential for developing effective recruitment and retention strategies (Hagan & Curtis, 2018; Nowrouzi et al., 2015; Poghosyan et al., 2017). By creating supportive work environments that prioritize NP well-being and professional development, healthcare organizations can improve retention rates and ensure the quality and safety of patient care.
Recommendations and Implications
The findings of this study underscore the importance of addressing both facilitators and barriers to optimize the implementation of NP-led clinics in NB, Canada. To enhance the success of future clinic initiatives, several recommendations should be considered. First, the government should establish clear decision-making frameworks and communication channels to facilitate collaboration among stakeholders and expedite the implementation of NP-led clinic initiatives. The sustainability of these clinics also hinges on adequate organizational support to facilitate effective leadership. Therefore, enhancing leadership capacity relies on implementing appropriate organizational-level strategies and support mechanisms that include NPs (Elliott et al., 2016). Next, decision-makers should prioritize the development of mentorship initiatives to support the professional growth and development of clinic staff and foster a culture of intra-professional and interprofessional collaboration within NP-led clinics (Barker & Kelley, 2020; Heale et al., 2018). Finally, strategies should be implemented to optimize patient panel sizes and workload distribution among NP-clinic staff (Martin-Misener et al., 2016). We recommend moving away from a targeted number of patients per NP and consider caseload formulas that consider patient characteristics known to affect patient panel size and account for organization factors (Shekelle et al., 2020). By addressing these recommendations and leveraging the lessons learned from the experiences of NP-led clinic staff, decision-makers and healthcare leaders can promote the successful implementation and sustainability of NP-led clinics as a valuable model of primary care delivery in NB, Canada.
Strengths and Limitations
This study provides valuable insight into the experiences of NP-led clinic staff, shedding light on the facilitators and barriers identified during the implementation of these clinics. By including a diverse range of staff members (NPs, RNs, LPNs, managers, and administrative personnel) the study offers a comprehensive understanding of the challenges faced across many levels of clinic operation. However, it is important to note some limitations. First, was the inability to label participant quotations by staff role, which may have provided useful context for the reader. However, due to the small number of clinic staff in a relatively small geographical area, doing so could have compromised participant anonymity. Moreover, the small numbers of staff in each category also made it impractical to analyze differences without risking identification, further limiting our ability to explore role-based perspectives in depth. Next, the study's qualitative nature limits generalizability as the findings are context specific and may not be applicable to other settings or healthcare systems. The reliance on self-reported data also introduces potential biases and the cross-sectional design of this study does not allow for monitoring of clinic staff experience over time. Finally, the interview questions touched on various aspects of clinic development and functioning, but did not directly focus on system-level barriers to implementation (e.g., policies, funding structures, regulatory frameworks) and how these could influence the clinics’ ability to operate effectively. In future work it would be beneficial to include questions that explore how external systems impact NP-led clinic implementation and address barriers at a more macro level.
Conclusion
The implementation of NP-led clinics in NB represents a significant step towards improving timely access to primary care, thereby improving overall health care delivery. The current study provides valuable insights into the experiences and recommendations of staff members involved in implementing NP-led clinics in NB, Canada. The findings highlight both facilitators and barriers encountered during the establishment and operation of these clinics, offering essential guidance for future interventions and policy decisions aimed at strengthening primary care services in NB.
Footnotes
Author Contributions
LM contributed to study design, data collection, data analysis, manuscript preparation, and final manuscript review. KL contributed to data collection, data analysis, manuscript preparation, and final manuscript review. SB contributed to data collection, data analysis, manuscript preparation, and final manuscript review. AL contributed to study design, data analysis, manuscript preparation, and final manuscript review. EJ contributed to data collection, manuscript preparation, and final manuscript review. SD contributed to study design, manuscript preparation, and final manuscript review.
Consent to Publish
Not applicable.
Data Availability
Aggregated data used and/or analyzed during the current study are available from the corresponding author on reasonable request. Access to raw data (e.g., interview transcripts) is restricted due to ethical guidelines imposed by the host institutions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by a Research New Brunswick (formerly New Brunswick Health Research Foundation) Summer Studentship Grant (2021). No additional grant support was received by any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Considerations
This research project was reviewed by the Research Ethics Boards at the University of New Brunswick, Université de Moncton, Horizon Health Network, and Vitalité Health Network.
Informed Consent
All participants in this study provided informed consent to participate.