
Abstract
Background/Purpose
Racism and hidden bias experienced by underrepresented nursing students contribute to a loss of confidence and anxiety. The A-CHARM nursing project developed virtual simulation experiences for nursing students to practice how to address racism. ‘Nik's Story’ virtual simulation was created as part of the A-CHARM project. The purpose of this study was to examine the effectiveness of an education intervention, that included Nik's story, on cultural humility and cultural diversity awareness.
Method
This quasi-experimental study included a convenience sample of final year nursing students. After informed consent, participants completed a pre-intervention questionnaire that included the Cultural Humility Scale “context for difference in perspective” subscale, and the Cultural Diversity Awareness questionnaire to assess baseline knowledge. Students participated in an education intervention that included a lecture, Nik's story virtual simulation experience, a debrief and then completed a post-education/simulation questionnaire that included usability/learner engagement questions and the Cultural Humility Scale “context for difference in perspective” subscale, and the Cultural Diversity Awareness questionnaire.
Results
Forty-seven students consented and completed the pre/post intervention questionnaire. Participants rated the effectiveness, engagement and usability of the simulation experience highly. There was a significant positive change in cultural humility “context for difference in perspective” subscale (pre-scores = 6.9, SD = 3.3; post-scores = 31.0, SD = 3.8, p < 0.001), and cultural diversity awareness (pre-scores = 95.4, SD = 8.9; post-scores = 103.4, SD = 9.8, p < 0.001).
Discussion
This intervention was effective in improving cultural humility and cultural diversity awareness in nursing students.
Conclusion
Simulation experiences regarding racism in the clinical setting provide a strategy for students to learn how to professionally navigate unwanted experiences.
Background & purpose
Racism and hidden bias experienced by underrepresented nursing students (Black, Indigenous and other Non-White Persons of Colour) contribute to a loss of confidence, burnout, and feelings of anxiety (Ackerman-Barger et al., 2020). These experiences affect the students’ academic performance, and personal wellbeing (Ackerman-Barger et al., 2020). Although there is little published literature that reports racism that nursing students experience, there is literature that highlights racism that nurses experience. When nurses who are Black or non-White persons of colour experience racism in the clinical setting, they often do not report or underreport these incidents (de Bourmont et al., 2020; Thomas-Hawkins et al., 2022). A study conducted with nurses (n = 788) in New Jersey, United States, examined the direct, indirect, and interactive effects of individual (race), interpersonal (workplace racial microaggressions), and institutional (racial climate) factors on hospital-based nurses’ emotional well-being (Thomas-Hawkins et al., 2022). Compared to White nurses, non-white nurses reported higher emotional distress, more negative racial climates, and more microaggressions/negative comments or actions due to their cultural or ethnic background (Thomas-Hawkins et al., 2022).
Cultural competence is characterised by the ability to engage in self-reflection on one's cultural values and recognise how these values influence the care one provides to others. It involves the ability to understand and honour of the values, attitudes and beliefs people from diverse cultural background hold and the ability to integrate health-related beliefs, cultural values, awareness of disease occurrence, prevalence, and treatment effectiveness. It includes each health professional's ability to assess and respect the values, attitudes, and beliefs of persons from other cultures and respond appropriately in planning, implementing, and evaluating a plan of care that incorporates health-related beliefs and cultural values, knowledge of disease incidence and prevalence, and treatment efficacy (Aboriginal Nurses Association of Canada, Canadian Association of Schools of Nursing & Canadian Nurses Association, 2009; Baba, 2013). Cultural humility is centred on a lifelong commitment to self-evaluation and self-critique in order to examine and address power imbalances based on the healthcare provider and patient relationship. It also involves forming collaborative and non-patronizing partnerships with communities for effective clinical and advocacy efforts (Tervalon & Murray-Garcia, 1998). While cultural awareness is focussed on ‘others’ and their culture, it acknowledges differences between cultures (Baba, 2013).
Cultural competence, cultural humility and cultural awareness learning strategies in nursing education and in other healthcare sciences programmes are designed to promote cultural awareness, cultural sensitivity, knowledge and skills. Education regarding these strategies are usually integrated throughout the formal education process and can vary in terms of specific learning objectives, curricula, and educational interventions (Gallagher & Polanin, 2015). This education usually focuses on cultural humility and cultural awareness when providing care to patients and families. This education may not directly address the issue of race, ethnicity and racism, and it usually excludes what the student nurse should do if they personally experience or witness racism or bias. Nurses and nursing students need support and strategies regarding how to professionally respond to or navigate situations where they are the recipient of racism or they witness racism. However, due to their lack of clinical experience, nursing students may not possess the strategies needed to respond to racism or hidden bias in the academic or health care setting (Wilkins et al., 2021).
Traditionally, the method of coping when a student experiences racism has been avoidance or silence (Wilkins et al., 2021). However, by not addressing racism or hidden bias it can indicate that inappropriate behaviours are acceptable. Nursing students require the opportunity to observe and practice how to navigate racism or hidden bias they experience or witness. Virtual simulation games (VSG) or virtual simulation experiences (SEs) are a platform utilised by healthcare educators, including nursing, to provide a safe and effective method of teaching students and other learners (Foronda et al., 2020). Virtual simulation immerses learners through the digital environment to foster a perceived lived experience (Foronda, 2021; Foronda et al., 2022b). Scenarios can be created to mimic clinical settings to provide learners with the opportunity to be exposed to an environment or situation in a non-threatening way (Chae et al., 2021). Virtual simulation experiences may be helpful in creating a safe environment for all nursing students to critically assess how they could address racism prior to experiencing or witnessing it in healthcare settings. They may also be helpful for White nursing students to learn how to be an ally, to provide assistance by intervening and support, if they witness racism.
A search of the literature using the search terms “Virtual Simulation” or “Simulation” and “Racism” and “Microaggression” yielded 2 results on CINAHL, and 17 results on Medline. Of the 16 results on Medline, one paper focused on recommendations for the use of simulation to address racism (Vora et al., 2021), and one descriptive study provided the results of a virtual reality racism experience that was piloted as a component of professional development for medical school and health system leaders, faculty, and staff (Roswell et al., 2020). There was one cohort study that examined an didactic educational intervention with reflective questions regarding cultural competence for third year medical students completing a psychiatry rotation (Khoury et al., 2022). The remainder of the publications focused on patients’ perspectives or how physicians or residents interact with people from diverse cultural backgrounds but did not provide educational opportunities. The 2 results from CINAHL described virtual simulation pre-briefing and debriefing for cultural humility (Foronda, 2021; Foronda et al., 2022a). No publications examined the use of simulation interventions for nurses or nursing students to address racism or culturally-based hidden bias.
There are published frameworks that outline ways to address racism, hidden bias (or unconscious bias), and inappropriate comments in healthcare settings. Four frameworks that nursing students could utilise to address racism, hidden bias or inappropriate comments include the: 1) Six-Step Approach (Overland et al., 2019), 2) ERASE framework (Wilkins et al., 2021, 3) SENSE debriefing model (Ko & Choi, 2020), and 4) Microaggression Triangle model (Ackerman-Barger & Jacobs, 2020). Our team created 5 virtual simulation experiences as part of the A-CHARM project (1. Nik's story, 2. Christian's story, 3. Sophie's story, 4. Yasmin's story, 5. Da-eun's story). These simulation experience use the frameworks as a guide on how an individual could navigate an inappropriate or racist comment experienced or witnessed in the clinical setting, however they have not been tested.
Due to the lack of available resources a didactic presentation and virtual SEs were developed through the A-CHARM (Addressing Culturally based Hidden bias and RacisM) nursing project. The A-CHARM nursing project consists of a didactic presentation, that is delivered in person, and includes definitions of race, racism, microaggression, discrimination and justice, and five SEs with learning outcomes and reflective questions. The Canadian Alliance of Nurse Educators Using Simulation (CAN-Sim) VSG/SE Design Process and International Nursing Association for Clinical Simulation and Learning (INASCL) standards of best practices were utilised for the development of the virtual simulation experiences (Canadian Alliance of Nurse Educators Using Simulation, 2022; Sittner et al., 2015). Both nursing students and faculty were involved in the development and filming of the virtual simulation experiences. Each virtual simulation experience scenario was meticulously designed to ensure user safety and provide evidence-informed approaches in addressing inappropriate comments or racism experienced in clinical settings. The A-CHARM virtual simulation experiences are available as an open access resource on the CAN-SIM website at https://can-sim.ca/addressing-culturally-based-hidden-bias-and-racism-a-charm/, or through e-CAMPUS Ontario.
The Microaggression Triangle Model is utilised in Nik's story and it includes strategies for the source of the microaggression, the recipient, and the bystander (Ackerman-Barger & Jacobs, 2020). It was developed to encourage people to view the microaggression from all three perspectives. The acronym ACTION is used by the recipient and includes Ask a clarifying question; Come from curiosity; Tell what you observed; Discuss the impact of the statement; Own your thoughts and feelings; and Next steps or follow up. The acronym ASSIST is used by the source and includes Acknowledge your bias; Seek feedback; Say sorry; Recognise the impact, not the intent; Say thank-you. While the bystander can follow the ARISE acronym: Awareness of what happened; Respond with empathy and non-judgement towards the source or recipient; Inquire about the situation or reason for comment; Use I Statements; Educate and engage.
In Nik's story (he/him) simulation experience, Nik is a 4th year nursing student of East-Indian descent. He is starting his final clinical placement on a medical unit at the local hospital. James and Sarah, are Nik's White peers and they are also completing their final clinical placement on the same unit. All three students are attending the hospital's orientation. During their lunch break Nik overhears Sarah make a racist comment regarding the number of immigrant nurse working in the clinical setting. Nik's story includes nine opportunities to respond to a scenario in the simulation (decision points), with three options with each decision point. This allows to the learner to explore options that are not part of the Microagression Triangle Model. Nik's story takes up to 15 min to complete, if all options are explored.
Purpose
The purpose of this study was to examine the usability, learner engagement and effectiveness of an education intervention that included a virtual simulation experience, Nik's story, with final year nursing students. The primary research question was: In final year nursing students what the effectiveness of an education intervention, that included a didactic presentation plus Nik's story virtual simulation experience, as compared to the knowledge gained in their usual nursing education, on cultural humility and cultural awareness. Additional questions examined usability and engagement of learners with the virtual simulation experience.
Methods
This quasi-experimental study was conducted in the Spring of 2023 at a University in Southern Ontario, Canada. Following Health Science Research Ethics Board review (HSREB# 6034728), a convenience sample of all final year baccalaureate of nursing students (n = 60) who were starting their final clinical placement were invited to participate in this study. Students were eligible to participate if they were starting their final clinical placement in June 2023. Informed consent was obtained using an electronic consent form through Qualtrics© that was posted on the students learning management system (Desire to Learn [D2L]©) 24 h prior to the start of the intervention. Students were informed that participation in this study was voluntary and anonymous, their course professor and study facilitator would not know if they participated in the study. After providing consent to participate in this study, students accessed the pre-intervention questionnaire through a web-based survey (Qualtrics©) that was also posted on their course page 24 h prior to the intervention.
Each student created a unique identifier, that was entered into Qualtrics© after providing consent and in the post-intervention questionnaire, that was not shared with the study investigators. This unique identifier (this identifier included the 2 digits representing their month of birth (e.g.,: January = 01), the first 2 letters of their current street address (e.g.,: Barton = BA) and the last 2 digits of their telephone number (e.g.,: 613-533-2121 = 21); from example identifier = 01BA21) was entered into the pre and post intervention questionnaires in Qualtrics© so participants’ responses could be paired for analysis to assess for changes in responses.
Usual education
At the University where this study was conducted there was no specific content regarding cultural competency, cultural diversity, cultural humility or cultural safety. These topics are generally covered in clinical and theoretical courses. However, there were no specific course objectives that include this topic.
Intervention
The intervention consisted of a 1.5 h in-person education session that included a education session (didactic lecture), a virtual simulation experience and a debrief that was focused on anti-discrimination and racism in clinical nursing settings. The education session was led by a Non-White faculty member who helped develop the A-CHARM virtual simulation experiences. The content of the workshop included in person didactic education regarding the a) definitions of race, racism, microaggressions, and social justice, b) an overview of the Microaggression Triangle Model, c) a description of the simulation experience, Nik's Story, including the objectives of the simulation. Nik's story was the virtual simulation experience used in this study as it scenario included final year nursing students in their final clinical practicum and the students included in this study were final year nursing students in their final clinical practicum.
Following the education, all students completed Nik's story, independently. This was done intentionally so that each student had the opportunity to complete the simulation experience and explore the options to facilitate their personal learning. All students were asked to bring an electronic device (laptop, tablet or cellphone) and headset so they could complete the simulation independently.
Outcome measures
Demographic information was collected as part of the pre-intervention questionnaire. Usability and learner engagement was collected as part of the post-simulation questionnaire. Foranda's Cultural Humility Scale was used to assess Cultural Humility and the Cultural Diversity Awareness Questionnaire was used to assess cultural awareness in both the pre-intervention and the post- intervention questionnaires.
To evaluate usability, engagement, and impact as perceived by participants the ClassRoom Instructional Support Perceptions (CRISP-VS) was included in the post-simulation questionnaire. The CRISP-VS is 26 item, valid and reliable measure has been previously used to evaluate the usability of a virtual simulation game used as a preparation for a respiratory distress simulation for nursing students (Luctkar-Flude et al., 2021). Reliability testing for the CRISP-VS reports a Cronbach's α of 0.79 for the usability subscale, a Cronbach's α of 0.89 for the engagement subscale, and a Cronbach's α of 0.82 for the impact subscale (Luctkar-Flude et al., 2021). With the CRISP subscales, usability refers to the ease of use of a technological intervention, engagement refers to the level of interest and appeal, and impact on learning refers to the learner's perceptions of the value of the intervention on their learning. Interpretation of CRISP subscale scores was published in a study examining the use of classroom response systems. A face value interpretation by relating raw scores for each subscale (i.e., usability 0–20, engagement 0–55, learning 0–60) to a five-point ordinal scale (e.g., strongly disagree, disagree, neutral, agree, strongly agree) was used (Sheng et al., 2019). To reduce questionnaire burden, a total of 15 of the questions were used in this study, three usability questions, five engagement questions, and seven impact on learning questions, for a total maximum score of 75.
The Foronda Cultural Humility Scale (2021) includes three subscales 1) “context for difference in perspective”; 2) “self-attributes”; and 3) “outcomes of cultural humility”. The Scale includes 19 questions and each item is rated with a Likert scale of 1 to 5 (1 = never, 2 = almost never, 3 = sometimes, 4 = almost always, 5 = always). To score this tool all of the numbers are totalled. The scores are interpreted as follows: 19 to 38 = Rarely Culturally Humble; 39 to 75 = Sometimes Culturally Humble; 76 to 85 = Usually Culturally Humble; and 86 to 95 = Habitually Culturally Humble. The scale was validated and tested with 322 undergraduate nursing and health sciences students and it has a high reliability (Cronbach's α = 0.85) (Foronda et al. 2021). For the purposes of this study the “context for difference in perspective” subscale was used as this subscale evaluates an individual's differences in perspectives regarding diversity, environment, historical precedent, political climate, power imbalances, and being open to different points of view. In addition, this subscale aligned with the objectives of the virtual simulation experience, Nik's story. This subscale consists of seven questions and has a high reliability (Cronbach's α = 0.85) (Foronda et al. 2021). This subscale's maximum score is 35, and the interpretation of this subscale scores are as follows: 7 to 14 = Rarely Culturally Humble; 15 to 21 = Sometimes Culturally Humble; 22 to 28 = Usually Culturally Humble; and 29 to 35 = Habitually Culturally Humble.
The Cultural Diversity Awareness Questionnaire is based on the Developmental Model of Intercultural Sensitivity which includes 6 stages, with the first 3 being ethnocentric (one's own culture is experienced as central to the understanding of others), and the second 3 stages are ethnorelative (one's own culture is experience within the context of other cultures) (Bennett, 1986; Van Hook, 2000). It has been used with educators at the Illinois State Board of Education (2022). This outcome measure has 32 questions. This questionnaire is designed to measure beliefs and behaviours regarding cultural diversity and inclusion. It is scored by summing the numbers chosen on the questionnaire (1 = never, 2 = almost, 3 = sometimes, 4 = almost always, 5 = always). A very high score (130–160) and a high score (100–129) indicates the individual/participant has a good awareness of their biases and how their behaviours may impact others, the individual relates to others in ways that value diversity. If the score ranges between 70–99 it is considered in the moderate range. A low score (40–69) or very low score (0–39) indicates that the individual/participant is not fully aware of the impact that their bias or behaviour has on other people and they may communicate in ways that does not value diversity (Illinois Leadership Project, 2016). The validity and reliability for the Cultural Diversity Awareness Questionnaire was tested with public school educators and it reports a high reliability (Cronbach's α = 0.9) (Henry, 1995). For the purposes of this study the first 23 questions will be used, with a maximum score of 115 and a high score ranging between 95–115.
For the post simulation questionnaire, participants were asked to re-answer the “context for differences in perspective” subscale of the Cultural Humility Scale and the Cultural Diversity Awareness questionnaire. While answering these questions participants were asked to reflect on how the education intervention that included the simulation experience has impacted their thinking and future actions. Questions were slightly reworded to ask ‘how often do you or would you’.
Data collection
Data was collected using a web-based survey through Qualtrics©. Qualtrics has achieved SOC2 Type 2 certification and has achieved ISO 27002, which ensures security, availability, and confidentiality trust principles and best practices.
Data analysis
Data were analyzed using IBM SPSS Statistics (Version 29; IBM Armonk, New York, United States). Differences in the pre and post intervention questionnaire were analyzed using paired t-tests. All other data including demographic data were analyzed using descriptive statistics and reported as a mean result and standard deviation, and frequencies. Reliability testing was conducted on the revised Cultural Diversity Awareness questionnaire as the number of questions were reduced from the original format.
Results
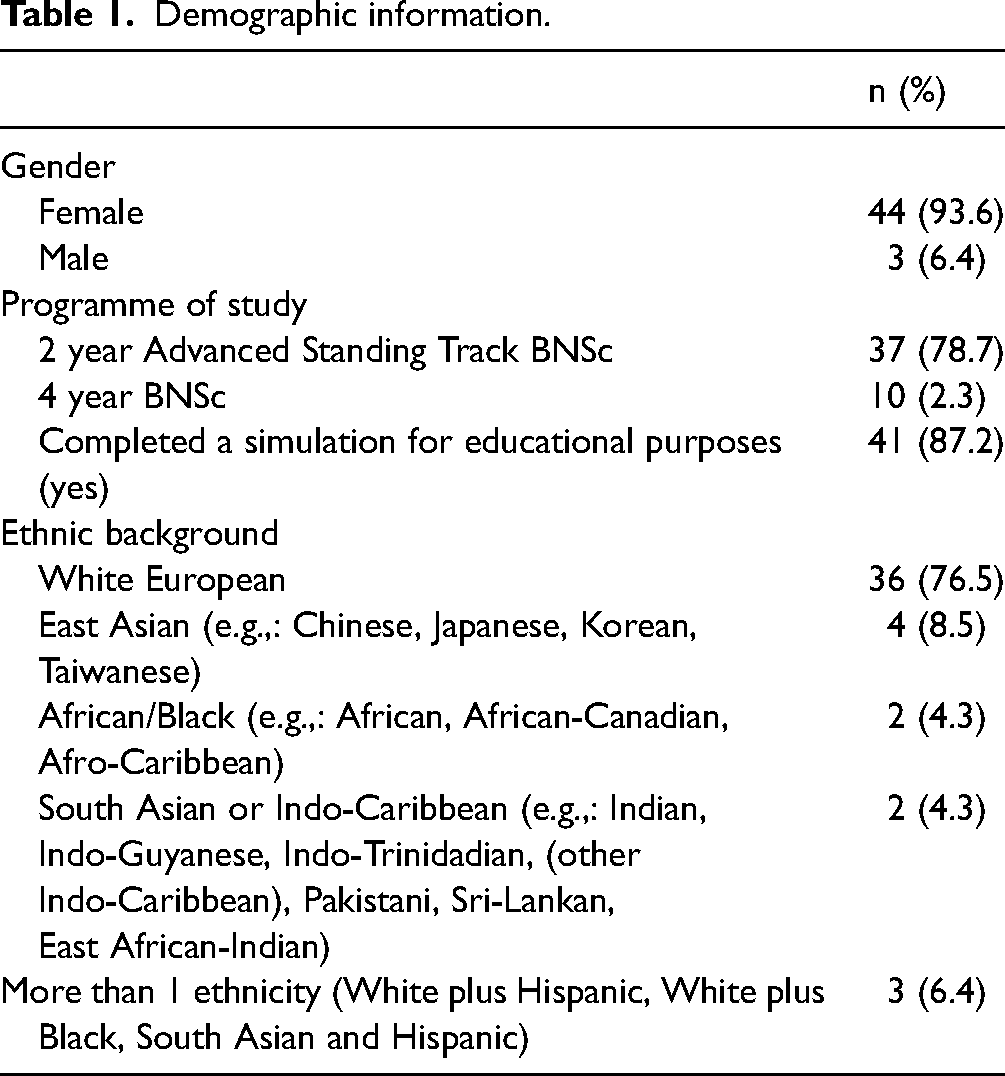
A total of 47 final year nursing students consented to participate in this study and completed the pre-intervention questionnaire and post-simulation questionnaire. The majority of participants self-identified as female, self-identified as being of White, had previously completed virtual simulations for educational purposes, and were enrolled in the accelerated two-year baccalaureate of nursing programme (Table 1). The mean age of participants was 24.4 (SD = 5.4).
Demographic information.
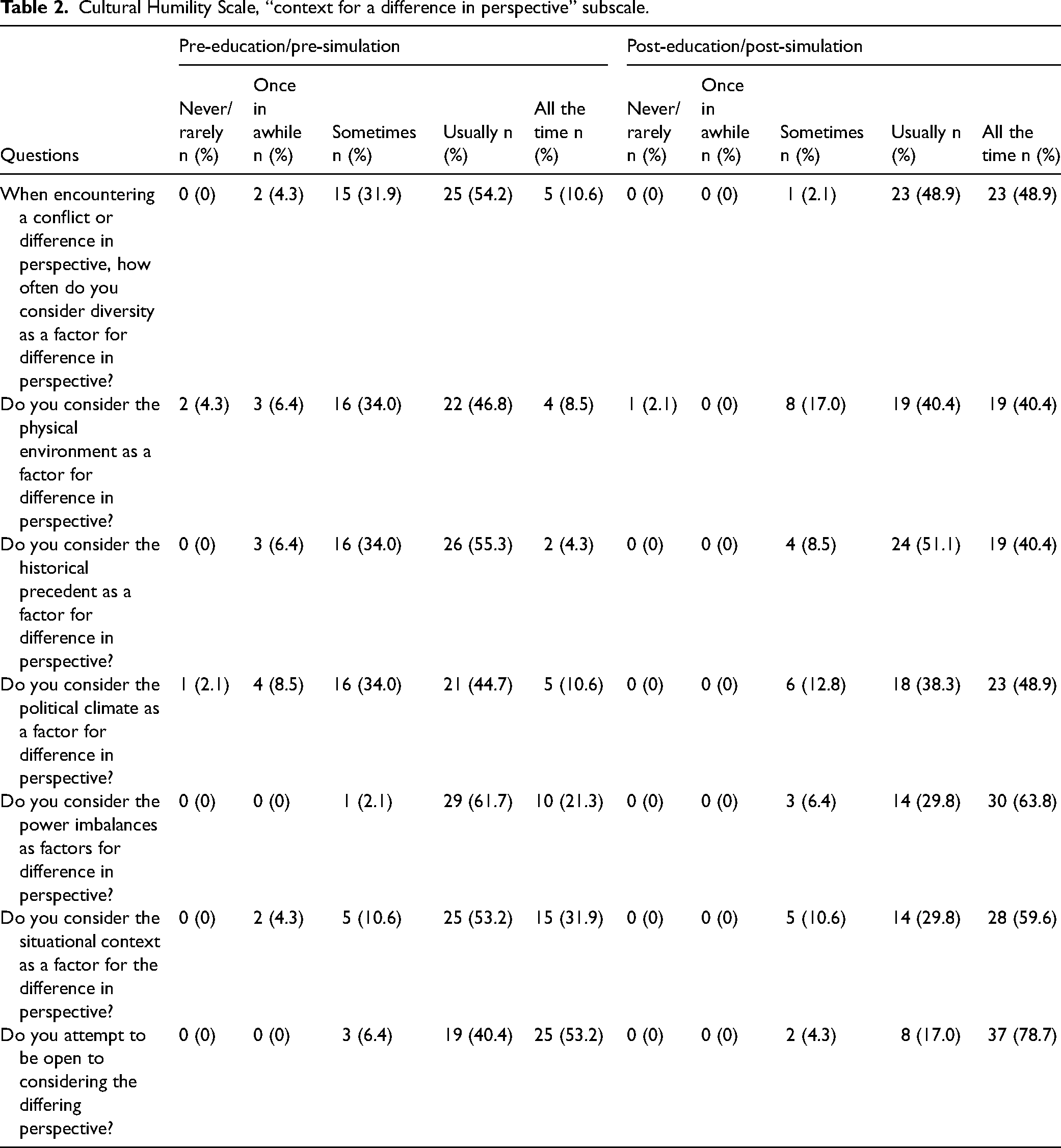
Cultural Humility Scale, “context for a difference in perspective” subscale.
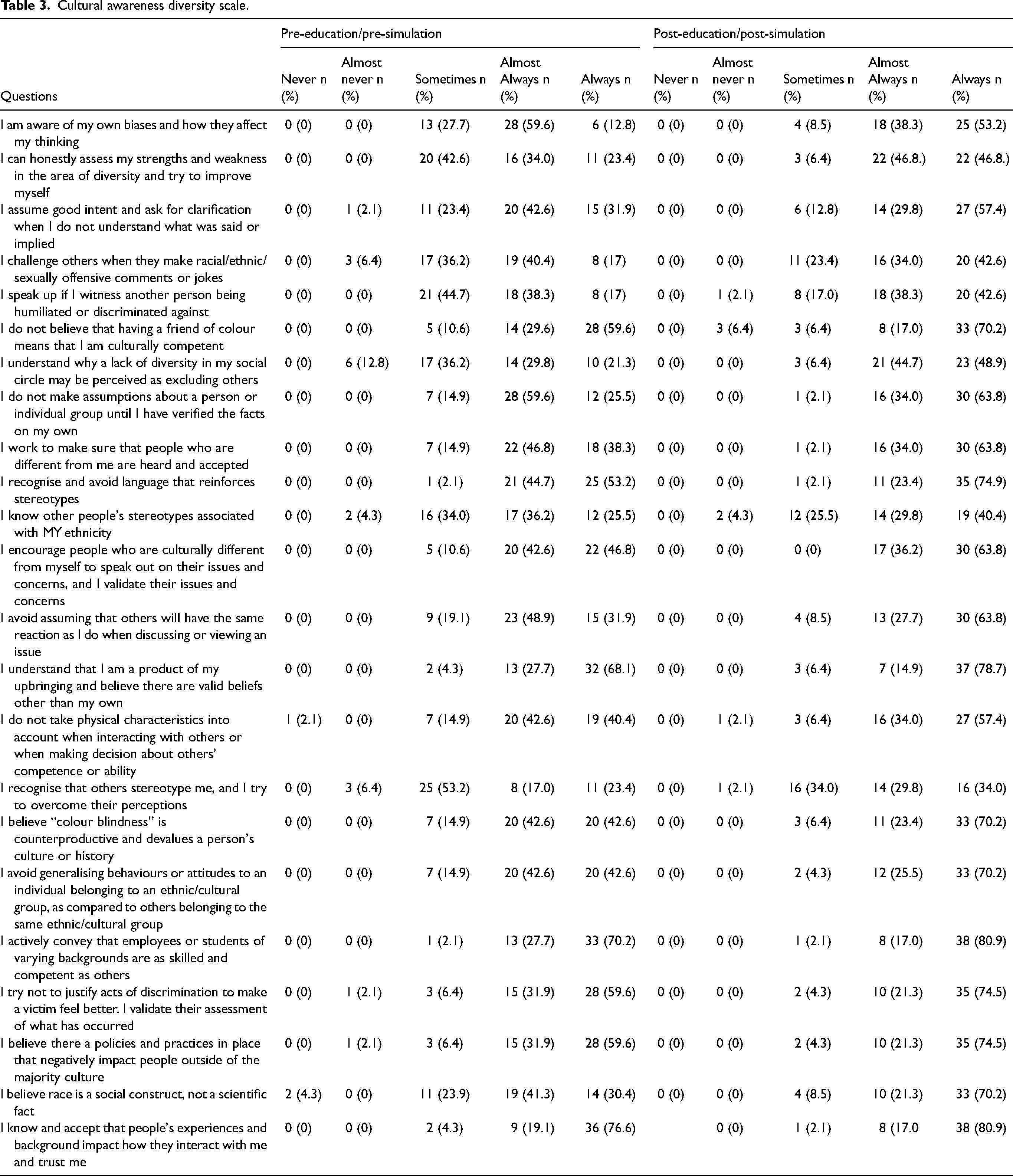
Cultural awareness diversity scale.
Usability engagement and impact
The mean CRISP-VS score was 67.6 (SD 7.6) out of 75, with a high mean usability score of 14.7 (SD 1.1) out of 15, a high mean engagement score of 22.1 (SD 3.4) out of 25, and a high mean impact on learning score of 30.8 (SD 4.3). The majority of the participants (n = 46) indicated they strongly agreed or somewhat agreed with the statement: ‘I would recommend that the faculty/course instructor continue to use the SE as a learning activity.’ The majority (n = 46) also indicated they strongly agreed or somewhat agreed with the statement: ‘Using the SE helped me think more deeply about the topic.’
Cultural humility
A paired t-test was conducted to evaluate the impact of the education intervention and simulation experience on the participant's cultural humility. There was a significant positive change in cultural humility after participants completed the education intervention. The mean pre-intervention cultural humility context for difference in perspective subscale scores were 26.9 (SD = 3.3), interpreted as usually culturally humble. The mean post- intervention scores were 31.0 (SD = 3.8, p < 0.001), interpreted as the intention to be habitually culturally humble. The mean increase in scores on the Cultural Humility the context for difference in perspective subscale was 4.1 with a 95% confidence interval ranging from 2.9 and 5.3. The eta squared statistic (0.5) indicates a large effect size. Cultural humility the context for difference in perspective subscale significantly increased following the education intervention that included Nik's story virtual simulation experience (Table 2).
Cultural diversity awareness
A high score was achieved by 25 participants on cultural diversity awareness on pre-intervention questionnaire (range 95–113), and 36 participants achieved a high score on the post-intervention questionnaire (range 97–115). A paired t-test was calculated to evaluate the impact of the education intervention and simulation experience on the participant's cultural diversity awareness. There was a significant positive change in cultural diversity awareness after participants completed the education intervention. The mean pre-intervention cultural diversity awareness scores were 95.4 (SD = 8.9) and the mean post- intervention scores were 103.4 (SD = 9.8, p < 0.001). The mean increase in scores on the Cultural Diversity Awareness Questionnaire was 8.1 with a 95% confidence interval ranging from 5.6 and 10.3. The eta squared statistic (0.5) indicates a large effect size. The revised questionnaire demonstrated good reliability with a Cronbach's α of 0.8. Cultural diversity awareness significantly increased following the education session and simulation experience (Table 3).
Discussion
This quasi-experimental study addresses an often-overlooked issue in nursing education – racism and hidden bias experienced by nursing students in clinical settings. This study examined the effectiveness of a virtual simulation experience, Nik's story, on final year nursing students’ cultural humility- related to the context for difference in perspective, and cultural diversity awareness. This study utilised an innovative intervention which included a combination of a didactic education session and a simulation experience to help nursing students practice how they can respond if they personally experience or witness racism or hidden bias. In addition, the educational content provided as part of this study filled a gap in the curriculum at this school of nursing and can potentially be used at other schools of nursing.
This innovative intervention was effective in improving cultural humility, in the context for difference in perspective, and cultural diversity awareness in final year baccalaureate of nursing students who were starting their final clinical placement. Participants rated the effectiveness, learner engagement and usability of the simulation experience, Nik's story highly with a recommendation to continue to use this simulation experience as a learning activity. Participants also indicated that the use of the simulation experience helped them think more deeply about the topic.
The Canadian Association of Schools of Nursing (CASN) publication Promoting Anti-Racism in Nursing Education in Canada (Muray et al., 2023) clearly outlines the history of racism within Canadian schools of nursing. Admission to schools of nursing were reserved only for single White women until the 1940's (McPherson, 2005). Today, nursing students are from diverse ethnic backgrounds, and non-White students and faculty often experience covert racism that impacts their ability to complete their education or advance in their careers (Zappas et al., 2021). In addition, nursing faculty are often unprepared, uncomfortable, or lack the ability to discuss racism or address racist incidents when they occur to students or their colleagues (Bell, 2020). There is a need to provide education to students and faculty about racism and how to identify and address racism and hidden bias (or covert racism) (Coleman, 2020). One strategy is to include anti-racism education programmes for both students and faculty.
Studies examining cultural competence education or sensitivity interventions have included a lecture and discussion format, where students listened to an instructor and discussed cultural information (Gallagher & Polanin, 2015) or cultural immersion international learning experiences (Gallagher & Polanin, 2015; Matthews et al., 2021). A critical integrative review of international learning experiences on cultural competence of nursing students reported that international learning experiences had positive outcomes regarding cultural competence (Matthews et al., 2021). Unfortunately, not all nursing students can participate in international learning experiences. In addition, it is not clear if the cultural competence outcomes are applied to the local setting once the students return to their home country.
A meta-analysis and a systematic review of the literature of educational interventions designed to enhance cultural competence in professional nurses and nursing students indicated that the results of lecture and discussion format interventions, using pre-test post-test study designs, report a moderate positive increase in student's cultural competence (Chae et al., 2020; Gallagher & Polanin, 2015). This study also used a pre-intervention/post-intervention design to evaluate an education intervention, however, in addition to didactic education, experiential learning was introduced through the use of a simulation experience. The simulation experience was designed to mimic an interaction that has happened to students in the clinical setting. In addition, the results of study report a large effect size for improvements in both cultural humility and cultural diversity awareness.
This study has several limitations, including sampling bias, response bias, and an inability to assess the long-term effects of the intervention. A sampling bias could have affected our findings since the participants were not selected randomly, and the study integrated into a mandatory in-person session. However, it is important to note that all students were told that participation in this study was voluntary, and their responses were kept anonymous. The researchers had no means of linking responses to the individual students. Respons bias is another potential limitation, as participants may have answered questions about cultural humility and cultural diversity awareness in a socially acceptable manner, potentially affecting the accuracy of the data. This study reported positive effects of the intervention it is important to recognise that we are not able to assess the long-term effects of the intervention or if the participants applied any of the strategies they learned in the clinical setting or in their everyday life.
Future research should include a multi-site trial with groups of students from many different universities and provinces across Canada. A mixed method explanatory study would provide a deeper understanding of the impact of the simulation experience. It is also recognised that there are five A-CHARM virtual simulation experiences all depicting different scenarios and utilising different frameworks. Future studies should examine the usability and effectiveness of these other simulations with nursing students and nursing faculty.
Conclusion
Virtual simulation experiences regarding racism in the clinical setting provide some strategies for students to learn how to professionally navigate uncomfortable and unwanted experiences. Although the use of frameworks and simulations are band aids to the larger problem of racism in the health care system and nursing education, this is a starting point. The study ‘s findings indicate the simulation experience, Nik's story, was effective in enhancing cultural humility and cultural diversity awareness among final year nursing students. Participants reported high levels of usability, engagement, an impact showing that the intervention is well received and has the potential to stimulate deeper thinking about this topic.
The five virtual simulation experiences developed through the A-CHARM project could be used to promote understanding and provide opportunities for reflection. These virtual simulation experiences provide nursing students, nurses, and nurse educators, an opportunity to examine the principles of cultural competence, awareness and cultural safety in encounters involving racism and culturally based hidden bias.
This research contributes valuable insights to an aspect of nursing education and highlights the potential of virtual simulation experiences to equip nursing students with the tools to address racism and hidden bias. It also opens the door for further exploration and development of antiracism education programmes for both students and faculty, promoting cultural humility and cultural diversity awareness.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from e-Campus Ontario to create the virtual simulation experiences.
Ethical approval
Was obtained from Queen's University Health Science Research Ethics Board (HSREB# 6034728).