
Abstract
Background
Throughout the COVID-19 pandemic, first-line healthcare leaders across the healthcare system played crucial roles leading, motivating, and supporting staff.
Purpose
This study aims to describe multidisciplinary first-line healthcare leaders’ experiences during the COVID-19 pandemic in Ontario, Canada using transformational and crisis leadership theory.
Methods
A descriptive two-phase (quantitative & qualitative) design was conducted in the spring of 2021. Phase 1 employed an online survey sent via email to first-line leaders from various sectors who were members of healthcare professional associations in Ontario. Participants included nurse managers, professional practice leaders (e.g., occupational and physiotherapists), advanced practice nurses, and clinical educators. In Phase 2, a subset (n = 19) of the Phase 1 participants were interviewed to gain a deeper understanding of these leaders’ experiences including role impact and support available. Semistructured individual interviews were conducted and recorded via Zoom©. Inductive and deductive analysis approaches identified key themes. This paper reports the qualitative findings from Phase 2.
Results
Leaders’ behaviors were representative of the key dimensions of transformational and complexity leadership theories. Recommendations for leading during a crisis included: engaging in self-care activities to manage the personal impact of the crisis; teamwork and collaborative leadership; and support from fellow first-line leaders and senior leaders. Findings can inform healthcare leadership education programs designed to manage future crises for both academic and practice settings.
Conclusion
Descriptions of first-line healthcare leaders’ roles and experiences during multiple waves of the COVID-19 pandemic validated their important contributions within various health sectors.
Keywords
Background and purpose
Over the past three years, healthcare leaders from all health sectors have played an important role in guiding and supporting frontline healthcare workers through and beyond the COVID-19 pandemic. The pandemic challenged healthcare leaders to focus on constantly changing quality, safety, patient-family, and workforce issues (Aquila et al., 2020). The pandemic became a prolonged crisis and a new normal where the experiences and needs of first-line managers must be understood to improve practices (Morse & Warshawsky, 2021). Much of the research on nursing leadership during the pandemic has focused primarily on the leadership responses during early phases of the pandemic.
Many studies have focused on nurse leaders in senior leadership roles such as clinical nurse executives (Freysteinson et al., 2021; Hartney et al., 2022; Jeffs et al., 2020; Riddell et al., 2022). Fewer studies have examined the role of middle level healthcare managers (Bookey-Bassett et al., 2021). There is even less published on the experiences of multidisciplinary first-line leaders in non-nursing disciplines such as physiotherapists, occupational therapists, social workers, and pharmacists) and other first-line leaders whose role includes leadership responsibilities such as professional practice leaders (PPL), managers, and clinical educators. In addition, much of the existing research has been conducted in hospital settings with less known about the experiences of leaders working in the home or community setting (Lefebre et al., 2020). For example, recent studies have explored the experiences of frontline leaders who were working in one hospital system or institution (Cathro & Blackmon, 2021; Freysteinson et al., 2021; Holge-Hazelton et al., 2021a, 2021b, 2021c) with the exception of Hartney et al. (2022) who explored Canadian healthcare leaders’ experiences in different sectors such as hospitals, long-term care and academic centres. Only two studies were found that were specific to the experiences of first-line healthcare managers in the Canadian health care system (Bookey-Bassett et al., 2021; Jackson & Nowell, 2021). Much of the research on healthcare leaders’ experiences during COVID-19 has been in health care systems in Europe (Holge-Hazelton et al., 2021a, 2021b, 2021c; Jonsdottir et al., 2022; Nevala & Vuorela, 2022), the Middle East (Abu Mansour & Abu Shosha, 2022; Mollahadi et al., 2021) and the United States (Alvarez et al., 2022; Cathro & Blackmon, 2021; Freysteinson et al., 2021). Further, many studies focused on leader experiences during the first wave of the COVID-19 pandemic in 2020 and wave two, early 2021 (Holge-Hazelton et al., 2021c; Nevala & Vuorela, 2022). This study, conducted during wave three in Ontario, the spring and summer of 2021, aimed to explore how first-line multidisciplinary healthcare leaders’ experiences of leading practice and work environment changes evolved throughout the different phases of the pandemic. Understanding how leader roles have been affected on a multidisciplinary level may provide insight on how leaders from various healthcare sectors can be more adequately prepared for future pandemics. This study addresses the gaps in the existing literature by describing multidisciplinary first-line healthcare leaders’ roles and experiences across various health sectors during the COVID-19 pandemic in Ontario, Canada, and provides an understanding of the impact of the pandemic on first-line leader roles and competencies needed to lead during a pandemic. The research questions guiding the study were as follows:
How do first-line leaders experience leadership during the current COVID-19 crisis?
How did they enact their leadership? What were the supports available to leaders? How are/were first-line leader roles impacted during COVID-19? What strategies do first-line leaders use to lead and manage during COVID-19? What recommendations do first-line leaders have for leading during future pandemic crises?
Methods and procedures
Study design
A descriptive two-phase (quantitative & qualitative) design was used to explore and describe the experiences and impact of COVID-19 on first-line health care leaders across various health care settings. In phase 1 (under review), an online survey was used to quantify leadership support, transformational leadership, crisis leadership self-efficacy, work engagement, resilience, and demographic characteristics. A qualitative descriptive approach was selected for Phase 2 as the researchers wanted to explore participants’ descriptions of their first-line leadership experiences and perceptions during the COVID-19 pandemic. This paper reports the qualitative findings from Phase 2.
Ethical approval for this study was obtained from the research ethics board of the primary Toronto Metropolitan University (REB# 2020-560). Participation was voluntary. All participants were given an explanation about the study and informed about their right to withdraw, after which they provided verbal informed consent.
Participant recruitment
Healthcare professionals employed in organizations providing patient care services who held first-line leader roles that included leadership, education, and/or management responsibilities (e.g., day-to-day operational activities such as staffing and resource allocation) were invited to participate in the study. First-line leader roles, provide a critical link between direct-care staff and senior administrative levels (Laschinger & Wong 2010). Exclusion criteria included individuals holding a senior-level leadership role (e.g., director or above in acute care settings), point-of-care staff with no formal leadership responsibilities, or those who may have been on leave at the beginning of the COVID-19 outbreak in March 2020. Participants were invited through an e-mail invitation sent out through three provincial professional associations whose membership included various health profession leaders across all healthcare sectors. Participants were invited to complete the Phase 1 survey which included an option to indicate if they would be interested in participating in an interview for Phase 2. Twenty-four of the Phase 1 respondents indicated they wanted to participate in an interview. All 24 participants were assessed for eligibility and then contacted by the study research assistant to schedule an interview with a member of the research team.
Data collection and analysis
Semi-structured individual interviews were conducted by various members of the research team via the Zoom © platform with each interview lasting between 30 to 60 min. The interview guide was adapted from an earlier study by Bookey-Bassett and colleagues (2021) to ensure it was relevant for nursing and non-nursing leaders. Further, responses to the Phase 1 open-ended survey question included references to leaders feeling unprepared in their role. The interview enabled participants to discuss how they were supported in their roles. Sample interview questions included: “In your role as a first-line leader, how is leading during COVID-19 different from pre-COVID-19? How was your role as a first-line leader impacted? What strategies/resources/supports were available to you? Describe what is different in the first versus the third wave.”
Interviews were audio-recorded with transcripts generated by Zoom©. Each interview transcript was cleaned and checked for accuracy. Any identifying information was removed from the transcripts prior to analysis. Cleaned transcripts were stored on a secured shared drive with only members of the research team having access.
The coding process involved members of the research team working in dyads. Both deductive and inductive coding occurred (Bingham, 2023). To answer the first research question, deductive coding was used as follows. Transformational leadership theory was used to deductively analyze responses to better understand the leader-staff relationship during the pandemic. According to this theory, there are four dimensions of effective leadership. The first dimension,
Going beyond the leader-staff relationship, we wanted to understand the operations component of the leader role and how leaders were able to adapt to pandemic conditions. Responses were therefore analyzed for evidence of concepts related to complexity theory. Uhl-Bien (2021) updated the notion of complexity theory in the context of the pandemic to describe ‘how leaders and followers can work together to enable adaptability in a highly interconnected, complex social system’ (p. 147). According to complexity theory, the adaptive process has three phases. In the first phase,
Inductive analysis (Braun & Clarke, 2006) was further performed to answer research questions 2, 3, and 4. Inductive analysis involved reading through the interview transcripts identifying codes, categories, patterns, and themes as the emerged from the data rather than having predetermined codes and categories (Bingham, 2023). Each research team member coded separately and then came together in dyads to discuss initial impressions, develop initial codes, and determine common themes for each research question (Bingham, 2023). The full research team came together to agree upon the final themes and sub-themes.
Results
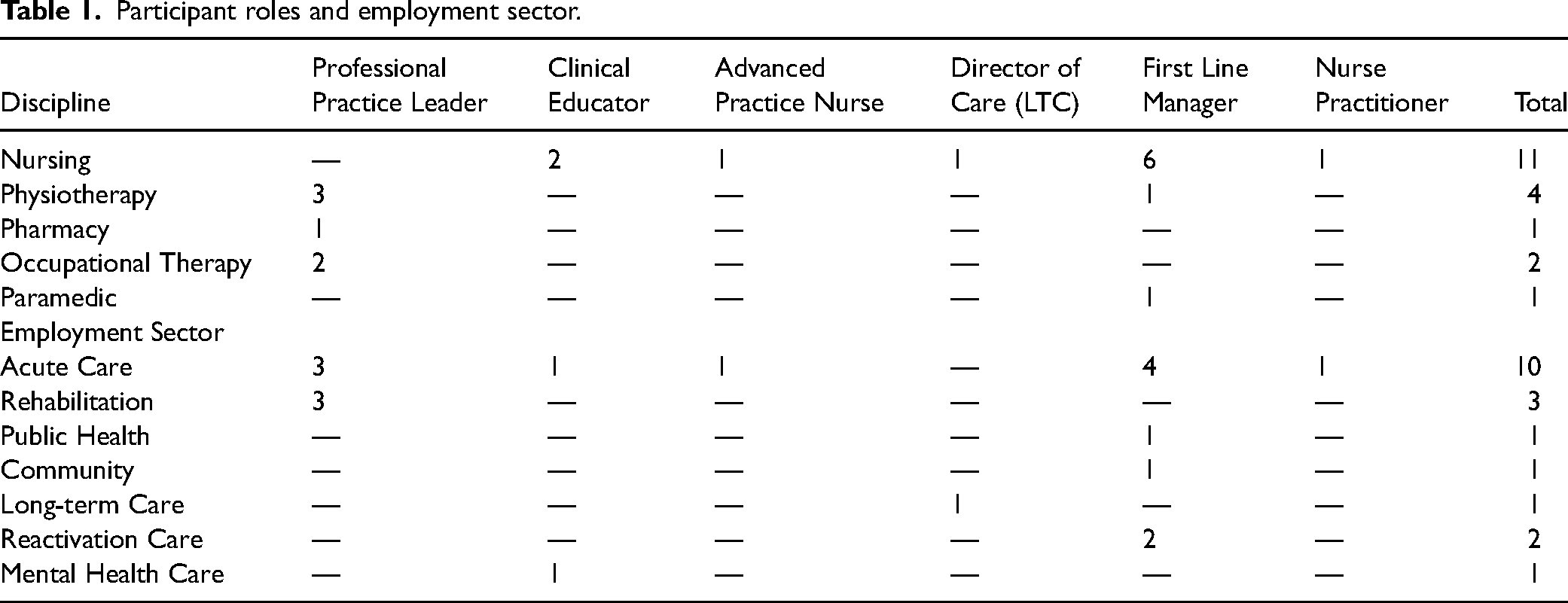
Nineteen first-line leaders participated in the interviews. Participants were diverse in the professions represented, roles, sectors, and geographical regions. Approximately 50% of the sample were in nursing leader roles. However, participants also included physio- therapists, occupational therapists, pharmacists, and paramedics. Participant roles were diverse and included professional practice leads, clinical educators, advance practice nurses, directors of care, first-line management and nurse practitioner roles as shown in Table 1. Participants worked in various health sectors such as acute care, rehabilitation, public health, community, long-term care, reactivation care, and mental health. Most participants (68%) were from urban centers with 32% of participants working in rural smaller towns and cities across Ontario.
Participant roles and employment sector.
Multidisciplinary leaders enacted and adapted their leadership roles throughout the crisis of the pandemic in ways that reflected both transformational and complexity leadership theories. The results section begins with a description of deductive findings from these theoretical perspectives. The inductive findings are then described with key themes addressing research questions 2, 3 and 4.
Transformational leadership
The four dimensions of transformational leadership behaviors were apparent in the interviews. “I was always a good listening ear, but I would share my own fears and stuff with the staff to let them know that we're all on the same page, that we all have the same fears and anxieties but we're going to get through it (Participant [P]9 - Paramedic/First-line Manager (FLM).” “I became more vulnerable, and my team and I would cry together because I didn't know how to lead them. So, the only thing I knew how to do was to create a safe space (P17, Nurse/FLM).” “I did a lot more walkthroughs on the floors to see how people were doing…and just sort of checking in with them, we have a chat, a WebEx chat group that we use just for the therapies. And just see how things were going, checked in at specific areas that I knew were under pressure. (P7, Physiotherapist [PT], PPL)’. “Just helping to navigate the emotional rollercoaster of [managing patients with COVID as well concerns about personal and family safety]” (P6, Occupational Therapist [OT], PPL).
Complexity theory
Leader responses provided evidence of their ability to adapt and reflected two of the three phases of complexity leadership theory. For the initial phase,
Supports available to leaders
Participants identified multiple sources of support available to them as leaders. Support came from within the organization via people and departments such as the infection prevention and control (IPAC) team, senior leaders, staff wellness and mental health programs and from their peer leaders. “I’m fortunate that I work closely with other practice leaders, and we can share our challenges and successes and experiences with one another, so that was very helpful.” (P10, OT/PPL). Other participants spoke about the importance of external support through being able to access critical care databases and having opportunities to consult with other health professionals. “A lot of consultation with other facilities in my professional practice network of physio leaders in the city; lots of consultation seeing who is doing what, how we're all dealing with the discrepancies and what was going on” (P15, PT/PPL).
Some participants from different health professional groups also noted having limited support. For example, “Initially I didn't feel I had a lot of support, it was kind of like you're dumped in and you got to roll with it and, and do the best you can” (P1, PT/PPL). Support also varied across organizations with those in smaller hospitals noting the differences in human resources available. As noted by one leader: “I didn’t know who to go to…very limited players, three nurse managers and a chief nurse, so very limited access to those types of resources” (P12, RN, Educator). In addition to leaders adapting how they led during the pandemic, through further analysis, we gained insights into COVID-19 impacted first-line leader roles, strategies used to lead during the pandemic, and recommendations these leaders had for practice, education, senior leadership, and policy makers. These findings are summarized below.
Impact of COVID-19 on first-line leader roles
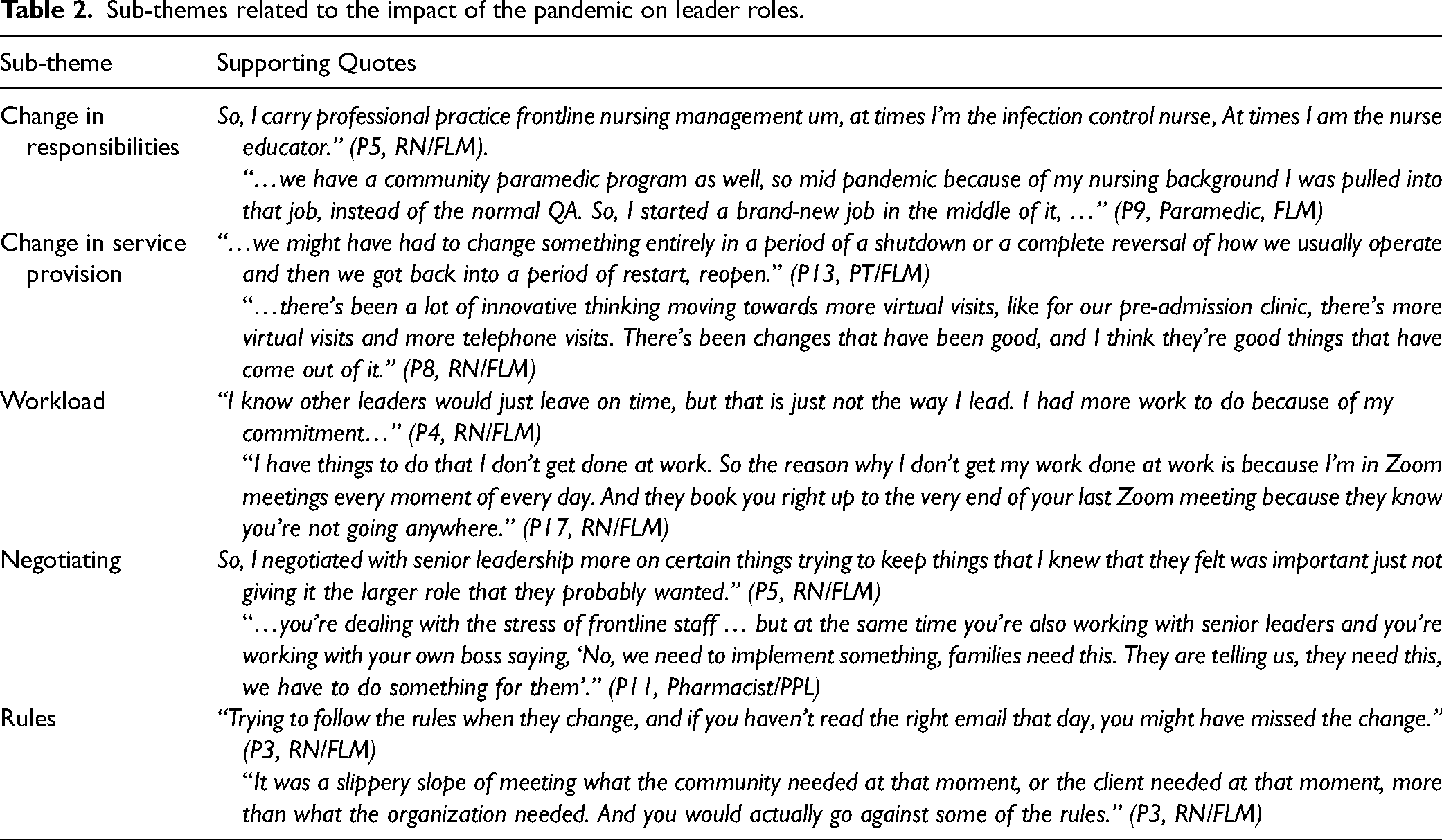
Leaders described several ways in which their roles were impacted by the pandemic. A major theme was
Sub-themes related to the impact of the pandemic on leader roles.
Strategies for leading during COVID-19
Participants identified four examples of strategies as a first-line leader that they found worked and helped them continue their work as leaders during the pandemic. Participants were grateful for the opportunity to be able to
“Being able to take days at home and work from home is good, because we do have dyads, manager dyads, where we cover for each other that's been really helpful.” Others spoke about the
Strategies used in “I think part of it was networking with my colleagues and other organizations. I do belong to several interest groups and professional practice networks, other professional practice leader groups, university [large city] groups…” (P10, OT,/PPL).
Differences in wave one and wave three
Participants noted differences in leading during waves one and three of the pandemic. Leading during wave one was described as “scary and all hands-on deck” (P3, RN, FLM) and a period of “constant stress” (P7, PT/PPL). Much of the focus was on crisis management, “policies and procedures” and “universal PPE” (P5, RN, FLM). Whereas they described wave three as a period of increased comfort “more relaxed…more controlled” (P4, RN, FLM) and “we’re much calmer” (P5, RN, FLM). As described by another participant, “third wave, it's kind of old news…we’re still continuing the same things, the responsibilities were not removed” (P16, RN/Educator). One leader noted how the pandemic had taken a toll and described wave three as perhaps not such extreme emotions as wave one but still “a completely different level of exhaustion. It's brutal. I have no desire to do anything that I enjoy” (P17, RN/FLM). A final comment reflected the notion that as the pandemic went on there was less appreciation for staff and leaders from the community and public at large “In wave one, the community sent us food…in waves two and three, there was no more appreciation for what was actually being done by the healthcare team” (P18, RN, FLM).
Participant recommendations
Participants were asked to provide recommendations for: 1) leading practice during a pandemic; 2) educating students and health professionals; 3) senior leaders in health care organizations; and 4) policy makers and/or government.
Recommendations for leading practice during a pandemic
Five key recommendations were noted by participants: engaging in teamwork- collaborative leadership; being flexible; communicating frequently; caring for yourself; and having a stronger voice with senior leaders.
Engaging in Collaborative Leadership. Participants spoke of the need to work together as an interprofessional team, to eliminate the hierarchy, to meet frequently not only for decision-making but also for support. Finding a colleague or another leader that you can trust and vent with was noted to be important to deal with all the changes. A quote from one participant recognized the value of collaborative leadership. “It's about teamwork right so leadership isn't about doing it on your own, … try not to be an autocratic leader… try to be a really collaborative leader who admits that you don't have the answers to all the questions and that you might be figuring it out as you go along with your colleagues” (P6, OT/ PPL).
Being flexible. With continuously having to adapt to changing practices, services, policies, and staffing, first-line leaders emphasized the need to be flexible as a leader. “You modify the way you lead, depending on the group that you're leading at that moment, depending on what it is that you need to lead you modify that. So, whether it's a crisis or not, I think that you're always changing as a leader, you're always modifying how you do your job.” (P3, RN/FLM).
Frequent communication. Participants made specific comments about the importance of communication with staff and others during the pandemic. First, participants recommended leaders truly “listen to your team.” Taking the time to listen to staff concerns, experiences, stressors, and suggestions can help leaders develop better ways to lead their teams. For example, participants also spoke about being able to “provide up to date information” for staff using multiple communication strategies such as email, team huddles, walk-arounds, and communication boards. A final comment about communication was to “be transparent about the information that you have” as represented in the following quote: Get transparent real fast. Get transparent, get a communication board happening, make sure people know where to find information - and update it every day. And even if it's not updated, change the date on the board, or you know no update on this day or something. But get really comfortable with having a lot of conversations all the time, and then get really comfortable with having conversations about how you're feeling, as a group” (P17, RN/Manager).
Caring for yourself. First-line leaders recommended several strategies related to taking care of themselves. Strategies included taking a day off, accepting any help available and acknowledging the importance of mental health. Looking after oneself physically, mentally and emotionally was deemed necessary in order to continue to support staff. One participant quote emphasizes these key points. “Make sure you have an outlet. Make sure you have good, solid self-care tools in your back pocket for when you need them. Don't be afraid to ask for help or take time for a break. Make sure you're caring for yourself mentally, physically, emotionally” (P9, Paramedic/FLM).
Having a stronger voice with senior leaders. Participants described their relationship with senior management in their organizations and the importance of being able to connect with senior leaders and increasing senior leader visibility with staff. I think having a greater voice to higher administration, probably would have been helpful and not just me personally, but our whole middle management group, I think we felt like. At times, we were kind of an inconvenience, because we were constantly looking for more information and clarity and our senior administration didn't have the time to actually connect with us to the degree that we wanted, so, I think having a stronger voice, going through this in the future would be very helpful” (P18, RN, FLM).
Recommendations for education
Participants were specifically asked to offer education-related recommendations to prepare future healthcare professionals to lead during a pandemic. Various knowledge and skills were identified by leaders as necessary: collaborative leadership, change management, critical thinking, resilience and flexibility, communication skills, conflict management skills, confidence building, and appreciation for other roles and professions. Quotes from two participants reflect these ideas. “Training leaders to be collaborative leaders” (P6, OT/PPL). “Understanding change and the impact it has on people and what to do with people who don’t do well with change. I think that is a big piece of [the] curriculum that may be helpful…” (P1, PT/PPL).
Recommendations for senior leadership
Participants offered several recommendations for senior leaders’ consideration during crises such as the pandemic. Participants emphasized the need for senior leaders to listen to managers and staff as they felt their voices or staff voices were not being heard at senior levels. Senior leaders should “draw in the front-line staff or middle level people” when decisions were being made. First-line leaders noted that senior leaders should “adjust expectations” around the quality and quantity of work or service and acknowledge that all staff were trying to do the best that they can and the need for flexibility and compassion to get through the pandemic. Recognition and acknowledgement of first-line staff work by sending a card to unit staff was suggested. Participants reported that senior leaders were not as visible as staff and first-line leaders would have preferred (i.e., to be present and acknowledge when people are struggling). “It might have been nice to see them wandering around now or even being near the entrance as people were coming in and leaving…just to be there.” (PT) First-line leaders also thought it was important for senior leaders to be transparent in their communication with staff throughout the organization. For example, to acknowledge if they don’t know the answers, to be open with staff as to how and why decisions are being made rather than telling staff what decision has been made. Participants recognized the efforts of senior leaders, for example holding town hall sessions, but suggested leaders alter the days/times of these sessions so that more people can attend (e.g., those working evening or night shift).
Organizational recommendations
Given the nature of their roles as first-line leaders, who were on the ground day-to-day with their staff, participants offered some specific organizational recommendations that could be helpful for other leaders during pandemic situations. It was suggested that first-line managers get to know staff at an individual level, to value every person for what they contribute. One example included “identifying frontline nurses who could jump into leadership roles if needed.” Having to redeploy staff to different areas was noted to be stressful for staff and first-line leaders. Participants noted the importance of knowing the skills and strengths of the people who are being moved around; realizing that this is stressful for people; people need retraining and education. As noted by one leader, “you can’t be taking someone from mental health and putting them in the surgical OR, that's not a good idea. Additional training and mentoring [is needed] so that staff are comfortable doing whatever they are being asked to do.” (P10, OT/PPL)
Participants recommended that an open communication plan is necessary to ensure all staff have access to the same ongoing and frequent information about the COVID-19 virus such as new research findings and evidence to support them in their practices. They encouraged “sharing of information as much as possible about the situation.” (P10, OT/PPL). Other recommendations included providing staff training and professional development such as pandemic preparedness training, professional development to prepare to move across programs, ongoing support/education for those redeployed to new areas, and IPAC training. The notion of ongoing training being necessary to provide quality care is reflected in the following quote “it's not just about day-today survival, it's how we continue to create and enhance environments for our staff through continuing education” (P12, RN/Educator).
Recommendations for policy makers and government
Several recommendations were suggested for policy makers and the government. Participants indicated that there is a need for better health human resource planning in regard to the pandemic. For example, one manager indicated “we have to have better plans in place for another pandemic…because we had people leave their frontline [position] to go to the vaccine clinic. And it's like well ‘hold on a second, we need them here’” (P8, RN/FLM). Leaders suggested it would be helpful to work with human resources staff and unions regarding the deployment of staff.
First-line leaders noted the need for province-wide policies in which health care organizations work more closely with the Ministry of Health. They described experiencing conflict with the “public health policies versus individual organizations’ policies. I think there has to be some commonality there.” (P16, RN/Educator). Clarity of policies would have helped staff respond to crisis situations faster. “If we had provincial standards - somebody to pull this together quickly…this is what we are going to do across the board…that would have been very helpful.” (P18/RN/FLM).
Study participants noted the inequity of access to services and resources during the pandemic. One example was in response to having to shut down services during the first wave. “We didn’t experience a surge up here of COVID-19 patients, so why couldn’t we continue doing surgeries right?” (P8, RN, FLM). Other leaders noted the need for “more equalized [access] in terms of resources.” (P18/RN/FLM). Specifically, the issue of access to PPE was noted “the shortage of PPE at the beginning of this was just astounding. They had a supply, but it had expired.” (P8, RN/FLM).
Discussion
This paper presents the experiences of a sample of first-line leaders from nursing and a small number of other health professions during COVID-19 within one province in Canada. Specifically, this study gives voice to perspectives previously not considered, namely the experience of various Canadian healthcare professionals from different disciplines in first-line leadership roles in all sectors, through the lenses of transformational and complexity leadership. A more nuanced understanding of leading in a crisis was possible by applying two theoretical models to the data collection and analysis processes. Transformational leadership helped to identify strategies that were used to enhance the leader-staff relationship during the crisis while complexity theory offered an understanding of how leaders acted to address operational demands at a systems level during the crisis. This duality in responsibilities is present in most formal first-line leadership roles.
In this study healthcare leaders demonstrated the four dimensions of transformational leadership reflecting the importance of the leader-staff relationships even during times of crisis such as the pandemic. Supporting and empowering staff through listening to their concerns, sharing information, keeping staff safe and being flexible was important. These findings are similar to other studies in which leaders have been recognized for their ability to build trusting relationships with staff (Freysteinson et al., 2021), navigate differently, and empower staff at the frontlines to continue to provide care throughout the pandemic (Bookey-Bassett et al., 2021; Lefebre et al., 2020). The results of this study further indicate the necessity for leaders to uphold principles of transformational leadership when dealing with crises.
In the quantitative phase of the study, transformational leadership was measured using the Multifactor Leadership Questionnaire (MLQ-5x-Short) (Avolio & Bass, 2004) where participants assessed their own leadership style before and during the pandemic (n = 118). The scores for the total scale were higher pre-pandemic (mean 3.08, SD .34, range 0–4) than during the pandemic (mean 2.81, SD.51, range 0–4) and these differences were statistically significant (p = 0.002). Therefore, transformational leadership was moderately high overall but fell somewhat as the COVID pandemic continued. For both time points, the highest ratings were for individualized consideration (mean 3.32, SD .44 and 3.06, SD .60 respectively) which is consistent with the qualitative findings where leaders noted the importance of supporting their staff and keeping them safe. The lowest scores were found for idealized influence (mean 2.76, SD .52 and 2.53, SD .63 respectively) which might be due to the demonstrating authenticity but also showing vulnerability as revealed by the leaders in Phase 2 of the study. Comparisons were made between how nursing (n = 85) and non-nursing disciplines (n = 31) expressed their leadership style and no statistically significant differences were found between these groups pre-COVID, but non-nursing leaders reported higher levels of transformational leadership than nursing leaders during the pandemic (mean 2.96 and 2.73 respectively, t = −2.17, p = 0.02). The reasons for this difference need to be explored further and could be due to variations in role expectations, the number of direct reports or other factors that impact the ability to enact dimensions of transformational leadership.
Complexity theory elucidated the leaders’ ability to adapt to the pandemic conditions to lead staff and ensure the delivery of care during the pandemic. Leaders demonstrated entrepreneurial actions as they found solutions on the go. They created supportive conditions for the adaptive process by being fluid and flexible and supporting teamwork. There was little direct evidence of operational leadership where, according to complexity theory, leaders work to embed new ideas or solutions across the organization. The lack of movement into this third phase of adaptation may be due to the phase of the pandemic when data was collected or could be due to role expectations where system-level change is part of the mid or senior level leader and not the first-line leader. Given the complexity of the current healthcare system and the new crisis of the health human resources, a deeper understanding of complexity theory and its application could serve as a fruitful area for further development of leadership skills for first-line leaders.
Leaders in this study experienced a multitude of changes involving additional responsibilities, changing policies, changes to service delivery, and increased workload. These findings are similar to those of other studies where ambulatory care leaders described having to realign ambulatory care services to enable alternate or virtual care delivery (Alvarez et al., 2022). Some leaders in this study reported working longer hours in order to complete all that was required of them such as attending Zoom© meetings while still managing the day-to-day operations of their units and checking in with staff (Alvarez et al., 2022; Bookey-Bassett et al., 2021; Freysteinson et al., 2021). Leaders emphasized their role in negotiating and advocating with senior leadership for resources to support staff and maintain safe care delivery. This finding is similar to other studies that stated that advocacy is one of the key roles that leaders must balance (Cathro & Blackmon, 2021).
Leadership strategies used by leaders in this study align with those reported in the literature. For example, leaders appreciated the ability to work virtually from home as a strategy to balance their work and personal lives (Freysteinson et al., 2021). Self-care came across as both a strategy and as a recommendation for leading during pandemics. This finding illuminates the importance of self-care for managers and leaders during COVID-19 as identified in several studies representing leaders from different countries (Behget & Modi, 2021; Chipps et al., 2022). Supporting staff and protecting staff well-being requires that first-line leaders have time and support systems available to manage their own stress, mental health, and well-being (Behget & Modi, 2021). Peer support within and networking outside their organizations were also recognized as effective leadership strategies by the leaders in this study (Cherepanov, 2022).
Participant recommendations concur with findings from previous studies. Participants identified various skills and competencies necessary to lead during a pandemic. These included: developing skills in collaborative leadership, change management, critical thinking, resilience and flexibility, communication skills, conflict management skills, confidence building, and appreciation for other roles and professions. These findings align with those of previous studies identifying leader competencies for leading during crises such as pandemics and disasters (Asgari et al., 2021; Behget & Modi, 2021; Wymer et al., 2021). In addition, our findings support the importance of leadership development to prepare and support current and future leaders to lead interprofessional teams in and across all healthcare sectors. Recent studies acknowledge the importance of cross-training staff (Freysteinson et al., 2021) and disaster training for all staff (Asgari et al., 2021; Freysteinson et al., 2021). Further, the need for additional management and formal leadership training and mentoring within practice and academic settings is recommended to support leader development and the ability to lead during a crisis (Holge-Hazelton et al., 2021a, 2021b). Recommendations include incorporating disaster management programs into academic curricula (Asgari et al., 2021). Further, Behget and Modi (2021) recommend making self-care part of leadership development education.
Similar to a previous Canadian study, (Bookey-Bassett et al., 2021), participants in this study emphasized the importance of senior leadership visibility and in-person presence. Frontline leaders noted the importance of senior leadership taking time to be present with and listening to first-line staff as a source of support. Leaders are considered a resource for staff - visibility. should be seen as a priority for supportive work environments (Bergstedt & Wei, 2022). Leaders can support staff through increasing their presence and visibility by taking the time to round and meet with employees in small huddles (Freysteinson et al., 2021).
Organizations have a responsibility to ensure leaders and staff have the support they need to enable safe care delivery. For example, ensuring that staff receive the necessary training, adequate resources, and access to ongoing support services as needed (Alvarez et al., 2022).
Support for leaders may include peer support, as well as formal mental health resources (e.g., psychiatrists, psychologists). Leaders noted the need for better health human resource planning at both the organizational and provincial level and for clear policies for health care organizations to work more closely with the Ministry of Health. Evidence indicates that leaders play a key role in advocating for equitable access to services across health care systems and sectors (Asgari et al., 2021; Lefebre et al., 2020; Wymer et al., 2021).
Limitations and implications and future research
To further extend our understanding of first-line leaders in all disciplines and roles, it would be useful to conduct a secondary analysis of the data to compare multidisciplinary versus nursing leaders. This comparison may reveal useful similarities and differences that could guide leadership development specific to crisis situations. Although our recruitment strategy aimed to include representation from various sectors, we had few participants from the long-term care sector. It would be useful to repeat the study and include strategies to ensure adequate participation from across healthcare sectors as well as including other geographic areas beyond Ontario. A range of crisis situations could also be explored beyond the pandemic to determine if and how leadership experiences are impacted. These findings could also provide further insights about change management practices in crisis/pandemic situations.
Conclusion
Descriptions of first-line healthcare leaders’ roles and experiences during multiple waves of the COVID-19 pandemic have illuminated and validated the contributions of multidisciplinary leaders across various health sectors. Leadership behaviours exhibited during the crisis were representative of the key dimensions of transformational and complexity leadership theories. Explicit recommendations for leading during a crisis were obtained from the participants thereby providing additional insights into how first-line leadership roles can be effective under these extenuating circumstances. Engaging in self-care activities to manage the personal impact of the crisis, teamwork and collaborative leadership were highly recommended as was support from fellow first-line leaders and senior leaders. These theoretical views and leadership reflections can be used to inform leadership development programs designed to manage future crises for both academic and practice settings. Improved healthcare human resource planning by organizations and government would be beneficial so that redeployment of staff could be optimized to meet changing needs in a crisis. Multidisciplinary first-line healthcare leaders also saw the potential for enhanced collaboration between health care organizations and government to promote more equitable access to services across all sectors during crisis situations.
Footnotes
Acknowledgements
The authors would like to thank Karen Spalding, RN, PhD, Professor Emeritus, Daphne Cockwell School of Nursing, Toronto Metropolitan University for her important insights and support during the initial phases of this research. In addition, we wish to thank the leaders who took the time to share their experiences and perspectives of continuing to lead during the multiple waves of the COVID-19 pandemic in Ontario.
We also thank the following professional associations in supporting recruitment of leaders for this study, The Nursing Leadership Network of Ontario, The Professional Practice Network of Ontario and WeRPN, Registered Practical Nurses Association of Ontario.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Community Services, Toronto Metropolitan University
Ethical statement
Ethical approval to conduct this study was provided by the Toronto Metropolitan University's Research Ethics Board.