
Abstract
Background
Policies and services for older adults are increasingly focused on living in the community, rather than relying on institutions. A total of 70–80% of community care for older adults is provided by family and friend caregivers. With Canada's aging population, the number of caregivers to older adults is growing.
Purpose
The purpose of this paper is to describe the research methodology that was employed in the Saskatchewan Caregiver Experience Study. The methodology was used to map the experiences and gather perspectives of caregivers in Saskatchewan and to identify their priority support needs.
Methods
Qualitative description was the approach in this study. An online qualitative survey was administered via SurveyMonkey and distributed via Facebook and community newsletters. The survey collected caregiver demographics and asked three open-ended questions regarding: (1) the challenges that caregivers experience; (2) the positive aspects of caregiving; and (3) the support needs and priorities of Saskatchewan caregivers. A fourth question where caregivers could freely express any other experiences or perspectives was included. Content analysis was the method used for data analysis.
Results
355 individuals met the inclusion criteria for this study. Participants were evenly distributed amongst urban-large, urban-small/medium, and rural settings in Saskatchewan. The average age of caregivers and care recipients were 61 and 83 respectively.
Conclusion
This study has implications for research, practice, and policy. By gathering the full spectrum of the caregiver experience in Saskatchewan, this study can help to inform how communities, governments, and our healthcare system can best support caregivers in their role.
Background and purpose
One-fifth of the overall population in Canada is 65 years of age or older (Public Health Agency of Canada, 2020; Statistics Canada, 2020). The increasing number of older adults is attributed to population growth worldwide and improved longevity (World Health Organization, 2014). Older adults typically have complex medical problems and higher rates of healthcare utilization (Grady, 2011; Vaingankar et al., 2016). It comes as no surprise that policies and services for older adults are increasingly focused on living in the community, rather than relying on institutions as the primary means of care delivery, resulting in the sustainability of healthcare systems (Vanleerberghe et al., 2017). In fact, a total of 70–80% of community care for older adults is provided by family and friend caregivers, also known as carers (Carers Canada, 2021). There are approximately 8.1 million Canadians that fulfill the role of an family or friend caregiver (Carers Canada, 2021). Moreover, caregivers contribute upwards of $25 billion CAD in unpaid labor to the Canadian health system (Hollander et al., 2009). Coupled with the aging population, the number of caregivers is growing. The definition of caregiving used in this study was crafted in a concept analysis, comprehensive of nursing, sociology, and psychology perspectives: “Caregiving is the process of helping another person who is unable to do for themselves in a ‘holistic’ (physically, mentally, emotionally, and socially) manner. Caregiving is facilitated by certain character traits, emotional skills, knowledge, time, and an emotional connection with the care recipient” (Hermanns & Mastel-Smith, 2012, p. 15).
Saskatchewan is one of Canada's 10 provinces and one of the three prairie provinces and is situated on Treaty territories 2, 4, 5, 6, 8, and 10, Homeland of the First Nations and Métis peoples. Saskatchewan's population is distributed throughout the geography of the province in a mix of urban and rural settings. In 2021, the proportion of Saskatchewan's population aged 65 years and older was 17.5%, which was a 2.0% increase from 2016 (Saskatchewan Bureau of Statistics, 2022). Caregivers play a significant role in the lives of older adults in Saskatchewan and the need for family and friend caregivers is increasing with the aging population. However, there have been few efforts to identify the experiences of Saskatchewan caregivers and to involve caregivers in setting priorities for support services they access (Hall & Holtslander, 2022). Since Saskatchewan's population is diversely distributed in geography, and it has been previously ascertained that the needs of older adults differ between urban and rural settings (Dal Bello-Haas et al., 2014; Saskatchewan Seniors Mechanism Research & Issues Committee, 2019), it was important to conduct a study that sought to understand the experiences and perspectives of Saskatchewan caregivers, while reaching all geographic locations of the province.
This paper elucidates the research methodology employed in the Saskatchewan Caregiver Experience Study (Hall, 2023). We aimed to map the intricate landscape of caregiver experiences in Saskatchewan, shedding light on their perspectives and identifying their priority support needs. The methodology described herein facilitated the inclusion of participants from various geographic locations, ensuring a comprehensive understanding of the caregiver landscape within the province. Therefore, we emphasize through this methodology paper the importance and feasibility of engaging with caregivers via this methodological approach to address the diverse needs of caregivers across urban and rural settings.
Methods and procedures
The methods for the Saskatchewan Caregiver Experience Study are reported in accordance with the Standards for Reporting Qualitative Research (SRQR) guidelines (O’Brien et al., 2014). SRQR guidelines improve the transparency of qualitative research by providing clear reporting standards (O’Brien et al., 2014). Reporting items that will be addressed in this section are purpose and research question; qualitative approach and research paradigm; researcher characteristics and reflexivity; context; sampling strategy; ethical issues pertaining to human subjects; data collection methods; data collection instruments and technologies; units of study; data processing; data analysis; and techniques to enhance trustworthiness.
Purpose and research question
The purpose of the Saskatchewan Caregiver Experience Study was to describe the experiences and perspectives of caregivers in Saskatchewan and to identify their priority support needs. The research questions for the study were: (1) What are the challenges and positive aspects of the caregiver experience in Saskatchewan? (2) What do caregivers to older adults in Saskatchewan identify as priorities for support? The specific objectives were to: (1) Explore family and friend caregiver experiences in both large urban and small center or rural areas of Saskatchewan; and (2) Identify Saskatchewan caregivers’ priority support needs.
Qualitative approach and research paradigm
In this study, caregivers to older adults participated in an online qualitative survey via SurveyMonkey. The qualitative approach used in this study is qualitative description (Sandelowski, 2000, 2010). Qualitative descriptive studies offer comprehensive summaries of events, seeks descriptive validity of the meanings which participants assign to those events; and allows for study findings to be close to the data (Sandelowski, 2000). Being close to the data is critical in this project as the goal is to describe the caregiver experience in Saskatchewan. The research paradigm in this study is naturalism. Various qualitative methods are used in health research, with them all sharing an orientation towards naturalism (Green & Britten, 1998). Naturalism is the understanding of health behavior in everyday context and involves exploring the complexities of behavioral contexts such as barriers to healthcare behaviors and the antecedents and consequences of behavior (Green & Britten, 1998; Newton, 2000). Further, naturalism is a commitment to studying a phenomenon in a manner that is free from duplicity or the inventiveness of the researcher (Sandelowski, 2000, 2010).
The qualitative descriptive methodology draws from tenets of naturalistic inquiry, meaning the phenomenon is studied in its natural state (Bradshaw et al., 2017; Sandelowski, 2000). Researchers attest that an understanding of the alignment between qualitative description and naturalistic inquiry offers a practical way to explore and answer research questions (Cutler et al., 2021). In any naturalistic study, there is no pre-selection of variables, no manipulation of variables, and no a priori commitment to any certain theoretical view of a target phenomenon (Sandelowski, 2000, 2010). Data are acquired from studying real-world settings to inductively construct patterns, categories, and themes (Patton, 2005).
Researcher characteristics and reflexivity
The research team for this study is a group of nurse researchers and a nurse research trainee. Nurses are well-positioned to study the phenomenon of caregiving. Nurses have been found to be the most frequent category of healthcare professionals that provide instruction and education to family and friend caregivers (Reinhard & Brassard, 2020). As well, nurses worldwide are leading several initiatives intended to support caregivers (Reinhard & Brassard, 2020). The research team for this study is experienced, albeit to different extents, in engaging with older adults and their caregivers in research initiatives.
Context
The setting for this study is the province of Saskatchewan. Saskatchewan offers a diverse geographic profile with both large and small urban centers. In Canadian geography, rurality is defined based on different criteria, such as population size, density, labor market, settlement context, and delivery mode assigned by Canada Post (du Plessis et al., 2002). However, participants in this study self-identified their residences as urban-large, urban-small/medium, or rural environments.
Sampling strategy
Purposive maximum variation sampling methods were used to recruit caregivers to older adults (aged >55 years for this study) via community newsletters, an online Facebook post in Saskatchewan community Facebook groups, and a paid Facebook advertisement. Caregivers were asked to complete an open-ended qualitative survey on the SurveyMonkey (Momentive Inc., 2021) platform. A member of the Saskatoon Council on Aging's Caregiver Committee generously translated all study materials to be inclusive of the Francophone community in Saskatchewan. No restrictions were imposed on what the relationship of the caregiver was to the care recipient, however the participant needed to be an family or friend caregiver to an older adult aged 55 years or older. Bereaved caregivers were also welcomed to participate in the survey. Excluded survey respondents were those who were healthcare workers formally caring for older adults and those who were caregivers to younger adults.
Ethical issues pertaining to human subjects
Ethical approval was received for this study from the University of Saskatchewan's Behavioural Research Ethics Board (Beh ID #3377). SurveyMonkey data were collected anonymously. When prospective participants accessed the survey link, a consent form was presented first, where individuals had the opportunity to review the project's aims and understand their rights to informed consent. Those who wished to participate then selected “Continue to Survey” to confirm their consent prior to providing their survey responses. Postal code data were collected and used to generate a pinpoint map to show the geographic distribution of participants (Figure 1); however, since only the first three characters were collected, the pinpoints only demonstrate the general area of residence so that anonymity was protected. Names of healthcare professionals, facilities, community programs, and locations were redacted from quotes used.
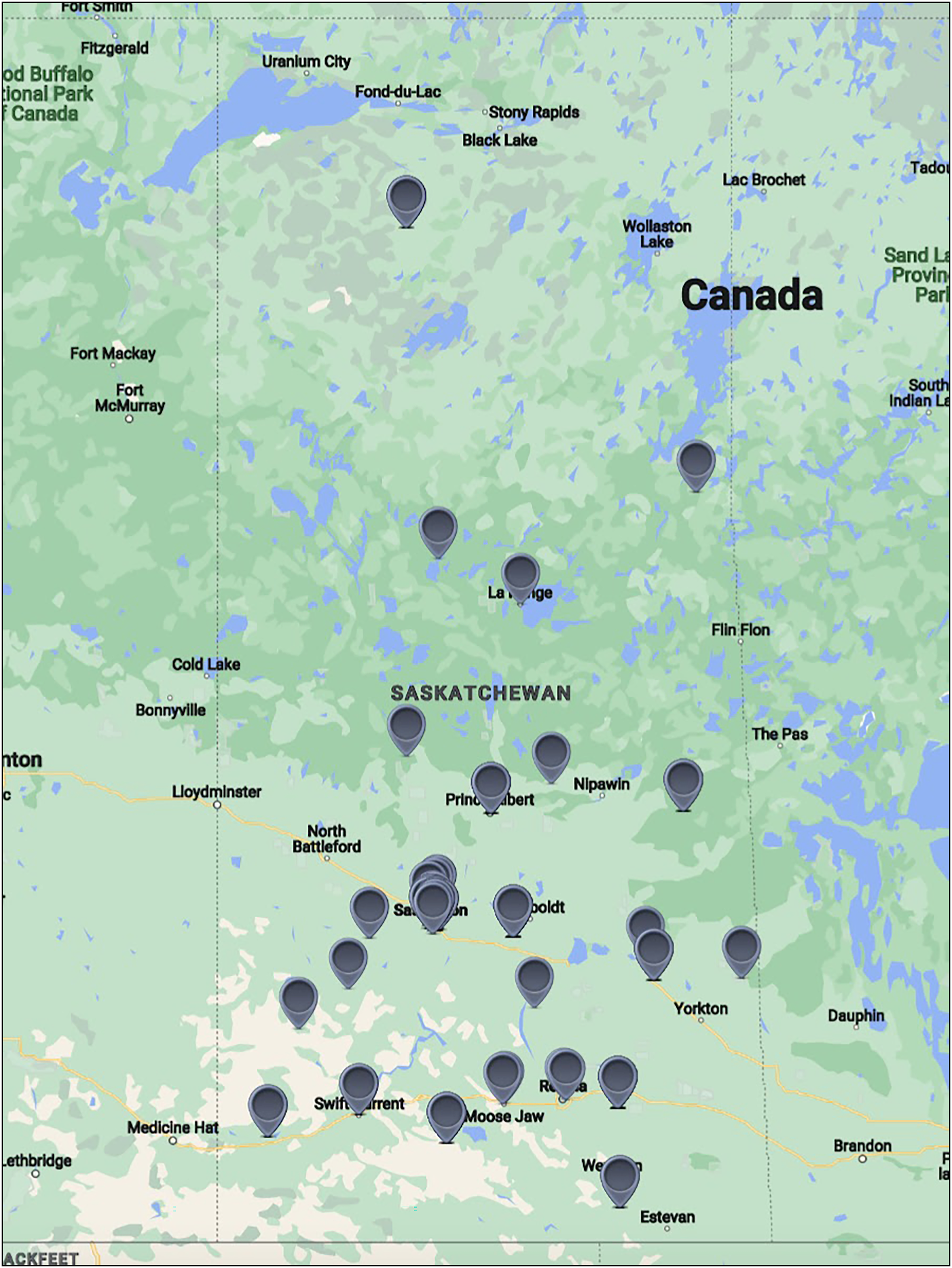
Map of participants from postal codes.
Data collection methods
The data collection method was informed by the literature on qualitative surveys provided by Braun et al. (2020). This study used a researcher-developed online qualitative survey to collect caregiver demographic and response data. Online qualitative surveys can harness the rich potential of qualitative data and the option for online delivery offers much opportunity to qualitative researchers (Braun et al., 2020). Online qualitative surveys have been described as congruent with the qualitative descriptive approach (Seixas et al., 2018) because qualitative description aims to record facts and the meanings participants ascribe to these facts (Sandelowski, 2000). Structured surveys allow participants to express their ideas on their own terms (Seixas et al., 2018). The online survey's access link was distributed in community newsletters, on Facebook in community groups, and via a paid Facebook ad that was targeted to appear in Saskatchewan residents’ newsfeeds. Data collection opened on June 2, 2022, and closed on July 20, 2022.
Data collection instruments and technologies
The study's online survey was hosted on SurveyMonkey (Momentive Inc., 2021) for feasibility and ease of data collection, which also eliminated the need for postage funds. To safeguard participant responses, internet security measures within the SurveyMonkey interface were described within the consent form. This safeguard included a transport layer security encryption (i.e., HTTPS://) which was active for all submitted responses. Demographic data were collected before the qualitative questions in the survey. The survey then presented four open-ended questions for qualitative data collection, which were: (1) What do you find most challenging about being a caregiver? (2) What do you find is positive about your caregiving role? (3) What do you think is most important for support in your caregiving role? In other words, what are your top priorities for support? (4) Is there anything else you would like to add about the experiences, perspectives, and priority support needs of caregivers in Saskatchewan?
After designing the questions and overall survey, five caregivers who were recruited by the Saskatoon Council on Aging and anonymous to the researchers reviewed the pilot survey. Feedback was sought based on the language of the survey, length of time to complete the survey, and the survey's overall structure. The pilot participants shared that they did not have any concerns with the survey. Data collected from the pilot participants was retained for the study.
Units of study
The purpose of this reporting item is to describe the characteristics of the units of study (O’Brien et al., 2014). In the case of this research, the units of study were caregiver participants. Participants who accessed the survey were asked to provide the following demographic information to gather descriptive characteristics: first three digits of their postal code for later data presentation of geographic distribution, self-identified urban or rural setting, age of caregiver, age of care recipient, years of caregiving experience, whether training was received for the caregiving role, relationship to care recipient, and care recipient condition. One characteristic that was not collected was participant's sex and/or gender. Although this was an oversight in our data collection tool, the study's aims were not to explore or analyze differences in the experiences and perspectives of caregivers based on their sex or gender. This notion is also addressed in this paper's limitations section.
Data processing
After the survey data collection period closed, the data was exported from SurveyMonkey and sorted into spreadsheets in Microsoft Excel. Demographics were tabulated in Microsoft Excel and open-ended responses to demographic questions were cleaned (specifically, care recipient condition and caregiver training received). The responses to each of the four qualitative survey questions were separated and viewed as individual data corpuses. Demographics that remained attached to each response were geographic setting, caregiver-care recipient relationship, and care recipient medical condition. The reason for this was to allow for identification of important context within the response. For example, a rural caregiver may have shared details of their experience of caring in a rural setting, without explicitly stating they live rurally. As well, a caregiver to an older adult with dementia may have been referring indirectly to dementia in their open-ended response. Lastly, a caregiver to a parent could have expressed salient details of their relationship with their parental care recipient. Therefore, these three demographics were considered important to attach to the qualitative responses, whereas ages and training received could be retrieved separately if necessary. Each question's data set was then converted in Microsoft Excel to a .PDF file, which was subsequently imported into NVivo 12 (QSR International Pty Ltd., 2019) qualitative coding software. Each of the four open-ended qualitative questions received its own NVivo file, for a total four NVivo files. Each data set was coded independently with its own coding matrix.
Data analysis
The content analysis method by Hsieh and Shannon (2005) guided our qualitative data analysis. Sandelowski (2000) shares that the analytic strategy of choice in qualitative description is content analysis. Content analysis is a method of analyzing written, verbal, or visual communication messages (Elo & Kyngäs, 2008). The use of content analysis in the qualitative descriptive approach is suitable due to the relatively low level of interpretation it yields, in contrast with grounded theory or hermeneutic phenomenology, in which a higher level of interpretive complexity is required (Vaismoradi et al., 2013). Qualitative content analysis focuses on the content or contextual meaning of data (Hsieh & Shannon, 2005). In qualitative research, codes are derived from relevant research findings and defined during data analysis (Hsieh & Shannon, 2005). An inductive, bottom-up approach to coding was employed in this study. The following steps, outlined by Hsieh and Shannon (2005), were carried out for the process of content analysis:
All survey responses were read by the researcher in their entirety to become familiar with the data. No coding of any type was used at this stage. The coding process began following an initial readthrough of the data (Hsieh & Shannon, 2005). Survey responses were re-read, and passages were sorted into low-level codes. These low-level codes were then sorted into higher-level categories. Lastly, rank order comparisons of frequency of codes were used to identify which categories of codes are most prevalent (Hsieh & Shannon, 2005), and subsequently identified what was most important to caregivers in Saskatchewan.
Techniques to enhance trustworthiness
Credibility, transferability, dependability, and confirmability are criteria used to ensure rigor in qualitative research (Lincoln & Guba, 1986). Credibility is described as whether the reality of the participants is accurately represented by the researcher (Lincoln & Guba, 1986). To ensure credibility in this study, regular contact was established and maintained between the first and second authors during data analysis. Furthermore, updates on data collection and analysis were provided monthly to the entire research team and a local committee of caregivers to older adults. Transferability refers to the ability to demonstrate study findings have applicability in other contexts (Lincoln & Guba, 1986), which can be achieved through a review of relevant literature. We conducted and published a scoping review of caregiver-identified priorities for support prior to this study (Hall et al., 2022), which allowed us to understand how the experiences of Saskatchewan caregivers align with caregivers in other geographic contexts. Dependability is described as an audit trail (Lincoln & Guba, 1986), which was accomplished by keeping detailed notes about the analysis process and recording specific limitations to the study and its data collection. Lastly, confirmability was achieved through salient immersion in the data through adherence to the content analysis process (Hsieh & Shannon, 2005).
Results
This research methodology was successful in gathering a total of N = 387 responses, and N = 355 respondents met the inclusion criteria. Reasons for exclusion included: being an older adult caregiving to a younger adult (<55 years old), being a healthcare worker but not a family caregiver, or being from a province other than Saskatchewan. The family caregiver self-identified the geographic area they lived in as rural, large urban, or small/medium urban. These areas were almost evenly distributed amongst each setting. Since the first three characters of the participants’ postal codes were collected, a map was able to be generated to display the geographic distribution of participants, presented in Figure 1.
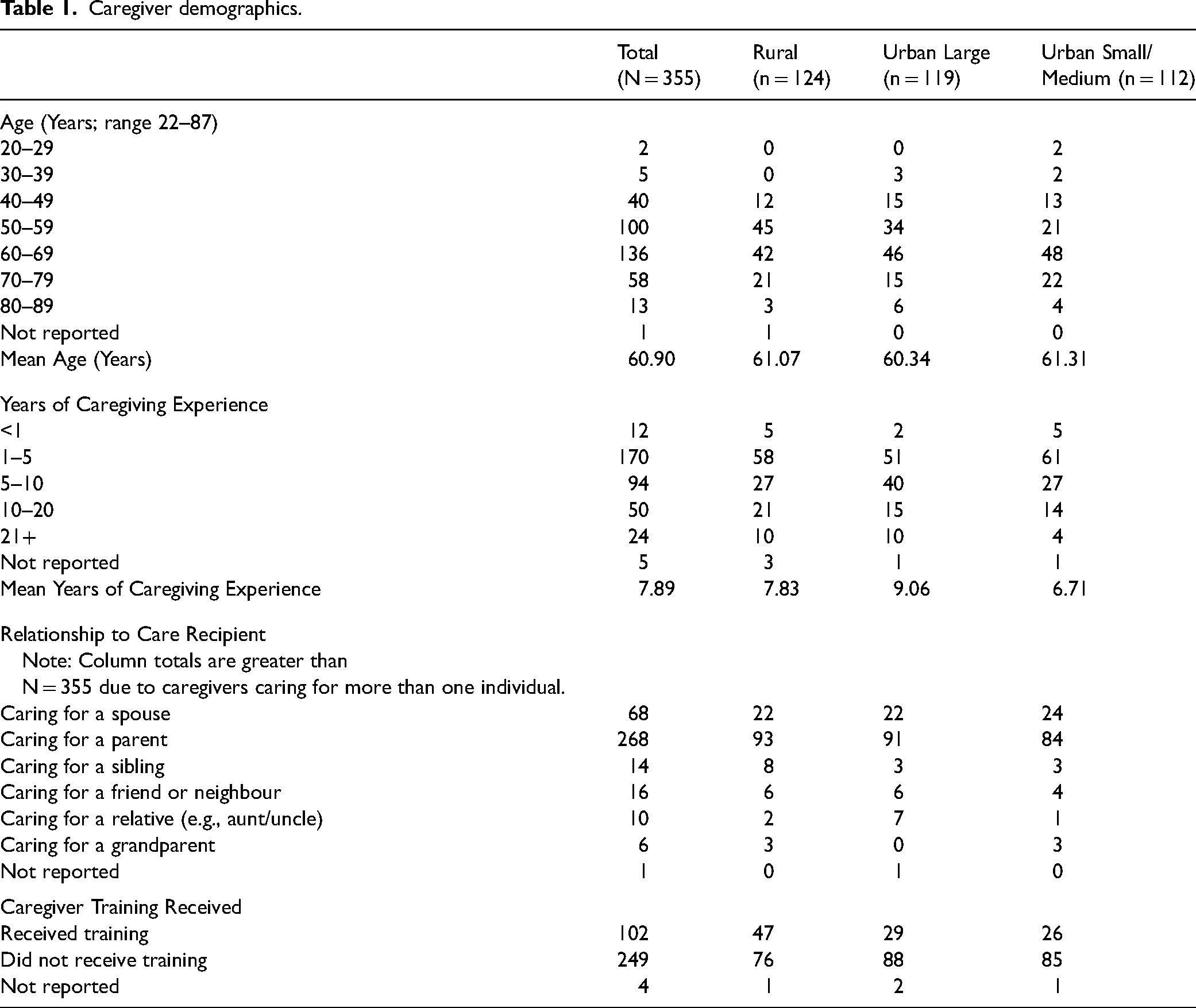
Participant (caregiver) characteristics are presented in Table 1. The overall mean caregiver age was 60.90 years with an age range of 22 to 87 years. The majority of participants were caring for a parent (n = 268), followed by those caring for a spouse (n = 68). Participants had a mean 7.89 years of caregiving experience, although the majority of participants in the study had 1–5 years of caregiving experience (n = 170). Lastly, only 29% of participants (n = 102) within the study had received any form of formal training to carry out their caregiving role, such as previous experience as a healthcare professional. Care recipient characteristics are presented in Table 2. Care recipients to which the caregivers provided care had a mean age of 83.02, with an age range of 55 to 104 years. The most common medical condition reported for care recipients was Dementia/Alzheimer's or related disorders, followed by heart/kidney/lung conditions. Eleven participants chose not to disclose their care recipient's condition.
Caregiver demographics.
Care recipient demographics.
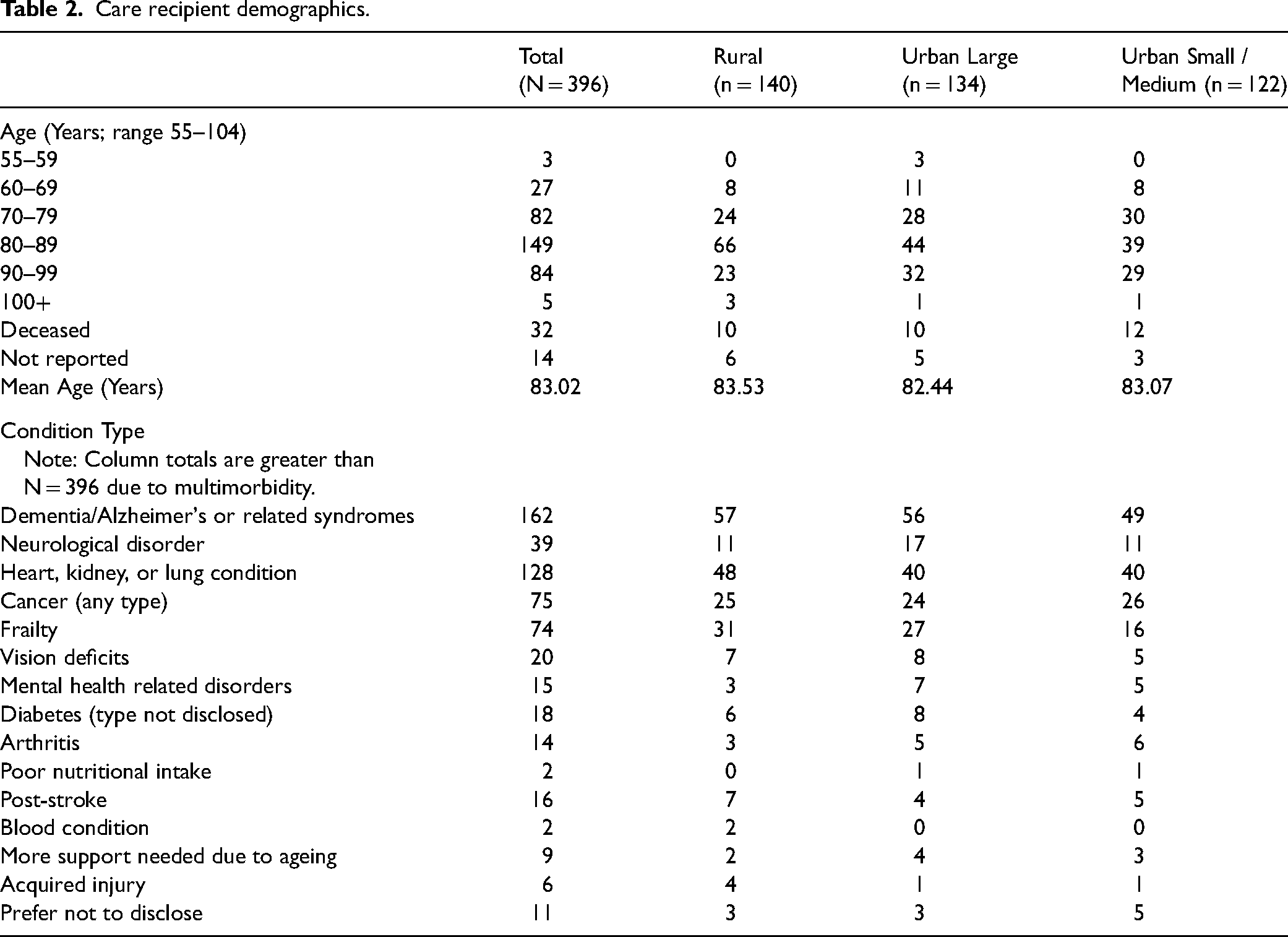
Table 3 presents the word counts and response rates to each survey question. Not all participants provided responses to all of the survey questions – a common phenomenon in survey-based research (Hendra & Hill, 2019). The response rates signify the level of participation and engagement from the caregiver population. The high response to the survey indicates a great level of interest and willingness to contribute to the study. The first question (challenges experienced by caregivers) was the most answered question (n = 354 of 355), and also had the largest average word count per response (n = 29), and the widest word count range, with the most words in a single response (n = 843). Word counts were considerably useful in gauging the depth of responses, as a higher word count generally indicated a more detailed and elaborate response. The variation in word counts highlights the diversity in the caregivers’ experiences. The first question, focusing on the challenges of caregiving, was the most answered and had the highest average word count, which suggests that caregivers are particularly inclined to share their challenges in more detail. The wide word count range, especially with the first question, indicates a spectrum of responses, from concise to highly detailed narratives. This diversity enriched the dataset, capturing a broad range of perspectives within the caregiver population. Future publications from this dataset will describe the challenges, positive experiences, and support needs of Saskatchewan's caregiver population.
Response word counts by question.
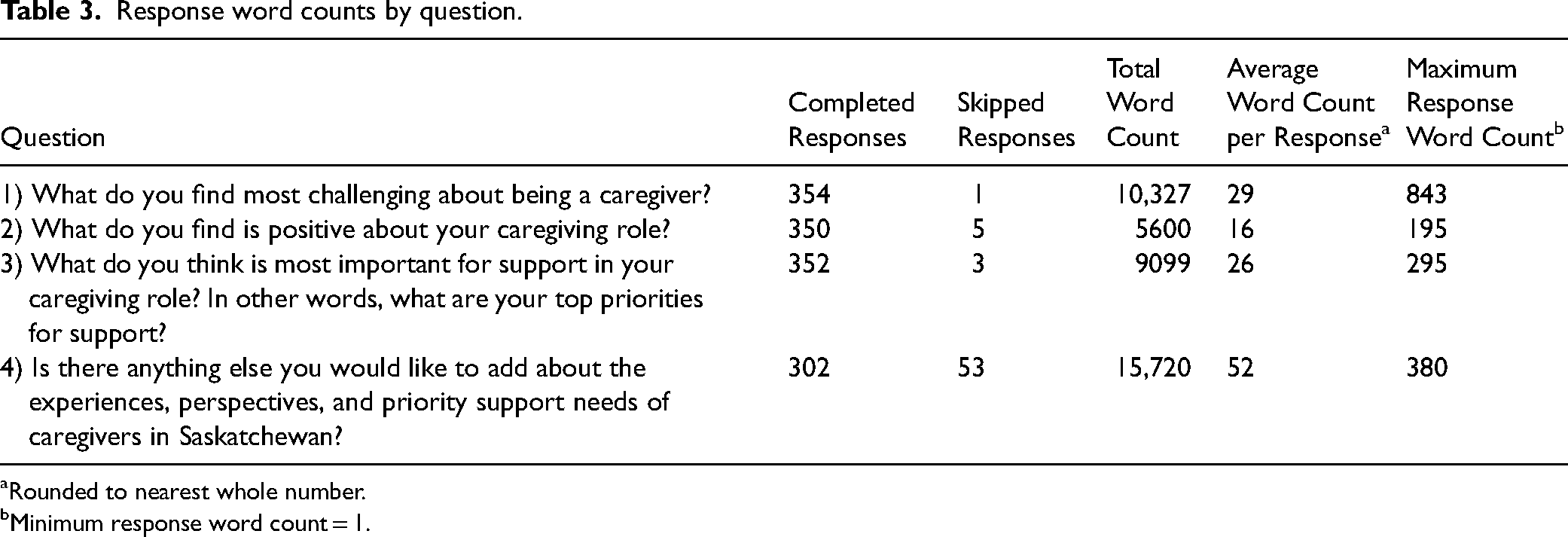
Rounded to nearest whole number.
Minimum response word count = 1.
Discussion
The methodology for the Saskatchewan Caregiver Experience Study employed an online qualitative survey, which is an up-and-coming technique for data collection in qualitative research. Traditional data collection techniques in qualitative research include direct face-to-face interviews, free-flowing conversation, and building rapport with participants (Moises, 2020). As such, preconceptions exist regarding qualitative surveys, as this approach differs from the traditional technique in the qualitative paradigm of participant engagement. Braun et al. (2020) have challenged these preconceptions of qualitative surveys and argue that qualitative surveys are an exciting and flexible method with several applications and advantages for both researchers and participants. Furthermore, the benefits of online qualitative surveys became more apparent during the COVID-19 pandemic, when in-person data collection was limited due to public health orders, social distancing, and isolation requirements (Ali et al., 2020; Moises, 2020).
The online qualitative survey was feasible to implement, as evidenced by the size of our dataset. There are several benefits to online qualitative surveys described in the literature. The online qualitative survey technique is found to be more enjoyable to participants due to its shorter duration, in comparison to focus groups or semi-structured interviews (Nayak & Narayan, 2019). The necessity of data entry is eliminated allowing for a decrease in processing costs while still allowing standardization and anonymity (Nayak & Narayan, 2019). Previous published literature stood testament to the justification that the online qualitative survey technique was acceptable for this study. In a study by Whitehead and Torossian (2021), 825 older adults (>60 years) completed an online qualitative survey to gather the experiences and perspectives of older adults during the COVID-19 pandemic. The questions that older adults responded to were “What are you finding most challenging or stressful today?” and “What is bringing you joy or comfort today?” (Whitehead & Torossian, 2021, p. 38). These questions are of similar genre to the questions for this study.
In a study conducted in Ontario, Canada by Bainbridge et al. (2018), the qualitative comments of bereaved caregivers were collected in an online survey. In their survey, caregivers reported what was positive and negative about the services provided during the last three months of their care recipient's life as separate open-text responses. The questions were “What if anything was good about the care?”, “What if anything was bad about the care?”, “What would you keep about the care provided?”, and “What would you change about the care provided?” (Bainbridge et al., 2018, p. 423). A total of 550 caregivers participated in the online qualitative survey study, with 69.8% of the sample (n = 380) being >70 years of age.
Online qualitative surveys also align with the qualitative descriptive design. An example of this, albeit unrelated to caregiving, is the study by Hart and Mareno (2014) that explored challenges and barriers to culturally competent care through the voices of nurses. In their study, Hart and Mareno (2014) used open-ended surveys to give their participants an opportunity to describe their perception of challenges and barriers in the provision of culturally competent care. A total of 374 nurses participated in the study by providing descriptions or comments within the open-ended questions (Hart & Mareno, 2014). Using thematic analysis (Braun & Clarke, 2006), Hart and Mareno (2014) were able to create three themes from the collected data. Since the purpose of the Saskatchewan Caregiver Experience Study was to describe the experiences and perspectives of caregivers from across the province of Saskatchewan, the online delivery of a qualitative survey facilitated data collection across a large geographic area.
Considering our study focused on the experiences of caregivers to older adults, it was expected that many eligible participants would be older adults themselves, such as spousal caregivers. There was initially some concern regarding whether or not Facebook was an appropriate tool for recruiting older adults. However, a review of Canadian statistics showed that 1 in 3 older adults use social media (Schimmele et al., 2021). Furthermore, Whitaker et al. (2017) conducted a systematic review of the use of Facebook for recruiting participants for health research. They found that recruitment of older adults through Facebook is feasible and successful. As well, in one of our previous studies, a sample of Saskatchewan older adults from both urban and rural settings reported actively engaging with technology, specifically with social media and Apple iPads (Hall et al., 2021).
Facebook was also an economical method of recruitment. While the social media announcements within the community Facebook groups were posted without cost, a small fund provided in kind by the Saskatoon Council on Aging allowed the employment of a paid advertisement for additional recruitment. These advertisement campaign options offered by Facebook have also been previously successful in recruiting research participants. Ali et al. (2020) used a web-based survey for data collection and advertised on Facebook. The total reported cost of the advertisement was $906 USD, which cumulatively reached 236,017 individuals and resulted in 9609 link clicks (Ali et al., 2020). Almost a third of respondents (28.5%) were over the age of 60 years. For this study, $200 CAD was invested in two paid Facebook advertisements, which reached a total of 26,876 individuals in Saskatchewan, and received 1414 link clicks.
Relevance of the study
New and experienced caregivers alike may experience difficulty accessing assistance, community resources, support, and adequate finances (Garcia-Ptacek et al., 2019). Therefore, the necessity of developing accessible and acceptable services that address the range of needs is critical to assisting this population (Harrop et al., 2014). There is also a need for a Saskatchewan context within the Canadian literature, which highlight the needs and priorities of individuals in a province blended in urban and rural settings. Therefore, it is critical to report what Saskatchewan caregivers need for support in their role by empowering their voice, listening to their experiences and perspectives, and disseminating analyzed findings to the wider community of stakeholders, decision-makers, and service providers in the province and Canada-wide.
Relevance to nursing
Caregivers need to feel supported by healthcare professionals, in addition to family, friends, and community. Regardless of setting, nurses are involved in every aspect in the care of patients and families. Home care nurses are often in regular contact with the caregivers to older adults and are positioned to assess the caregiver-care recipient dyad on a regular basis for the quality of the caring relationship and can monitor for caregiver role strain (Van der Lee et al., 2014). For nurses in acute care settings, an understanding of the caregiving role can support nurses to acknowledge the range of emotions and feelings that may be experienced by caregivers (Svavarsdottir & Sigurdardottir, 2013). This knowledge and understanding can be applied in cases such as when a care recipient is admitted into the hospital.
Study implications
Qualitative health research is a powerful approach to inform and advance health systems at different levels (Kozleski, 2017). Sallee and Flood (2012) describe how findings from qualitative research can be bridged into future research, policy, and practice. Researchers can use findings to develop and answer key questions in future studies; practitioners can implement research on the ground; and policymakers can utilize findings to create effective policies (Sallee & Flood, 2012). As such, the Saskatchewan Caregiver Experience Study has implications for research, practice, and policy.
Research
Since this study is exploratory and seeks to map caregiver experiences in Saskatchewan, the findings can help to develop support services and interventions to facilitate meeting the needs that were reported by participants. Caregivers to older adults have previously iterated they have an interest in research engagement (Haase et al., 2021; Hall & Holtslander, 2022). Researchers should capitalize on this interest by co-creating solutions to improve the caregiver experience.
Practice
Recognition of the caregiver experience by healthcare professionals is essential in planning services to support care recipients and caregivers in ways that are meaningful and effective. A systematic review by Mitnick et al. (2010) also reported that recognizing the caregiver experience contributes to the positive aspects of caregiving and decreases rates of patient hospitalization and institutionalization due to the associated decrease in caregiver role strain and burden. Additionally, Semere et al. (2022) interviewed 15 physicians regarding their perspectives on caregivers in a qualitative study. Physicians recognized that they need to adapt appointment communication strategies to include caregivers, engage caregivers in patient care, and find ways to care for the caregiver in tandem with the care recipient (Semere et al., 2022). One physician participant in the study by Semere et al. (2022) stated, “If we care for our patients’ caregivers, that's an indirect way of taking care of our patients” (p. 7).
Policy
Specific findings from this study can offer implications for policy. Leveraging informal care in place of institutional long term care has become a key strategy in maintaining healthcare system sustainability worldwide (Carstairs & Keon, 2009; Khayatzadeh-Mahani & Leslie, 2018). In a brief review of existing Canadian literature and policy, there was found to be a paucity of current policies that enhance caregiver support at both provincial and federal levels. Currently, most governmental supports focus on providing assistance to those with care recipients in care homes, rather than positive aging in the community. This focus is contradictory to previous governmental efforts in the 2000s (Carstairs & Keon, 2009) that sought to enhance caregiver support. Findings from this study can be used to adapt policies to improve the support that caregivers to older adults receive in the community.
Strengths & limitations
Due to the breadth of this study, a variety of strengths and limitations exist at different points, which are described in this section. Regarding study design, strengths and limitations of qualitative description (Sandelowski, 2000, 2010) and the online delivery of the survey are explored. We also describe oversights that occurred in the collection of data.
Qualitative description offers a straight description of the data that is typically organized chronologically by topic or relevance (Neergaard et al., 2009; Sandelowski, 2000), which was ideal for the Saskatchewan Caregiver Experience Study since one of the main objectives was to determine what Saskatchewan caregivers prioritized for support in their roles. However, qualitative description is regarded as one of the least theoretical qualitative approaches to qualitative research (Neergaard et al., 2009). Despite not being based in theory, qualitative description should be the method of choice when a description of a phenomenon is desired (Neergaard et al., 2009), as was the case in this study. Therefore, the overall employment of the qualitative descriptive approach is a strength to this study's design. With that being said, limitations to the use of qualitative description still persist. For example, there is no clearly defined approach to qualitative description (Milne & Oberle, 2005). As such, there could have potentially been some issues with rigor in the analysis process. These issues were mitigated by regular meetings occurring between the first two authors, as well as a review of the results and progress in analysis by the entire research team at near-monthly time points.
The online delivery of this study is a somewhat unconventional method of interaction in qualitative research but its use has been emerging in recent years (Carter et al., 2021; Horrell et al., 2015). Qualitative researchers have been increasingly turning to online platforms for data collection (Carter et al., 2021). Specifically for caregivers, online participation can be inviting because they do not need to arrange accommodations for the care recipient or respite time, which can often stand in the way of in-person research (Hewson, 2014; Horrell et al., 2015). Ethical challenges exist with online data collection, such as with ensuring informed consent is understood and the potential for participants to become distressed (Carter et al., 2021). These challenges were addressed in this study by providing the participants a consent form as the entry page to the survey and contact information for supportive services was provided at the beginning and end of the survey.
Other limitations regarding the collection of caregiver demographic data exist. The first is that caregiver gender was not collected. This omission was an oversight. Although assessing differences in caregiver gender was not the specific aim of the study, the data would have allowed for additional interesting analysis. Not collecting caregiver ethnicity also proved to be a limitation and oversight in the context of Saskatchewan's high population of Indigenous Peoples. It has been recognized that previous research has largely ignored the experiences, unique challenges, and perspectives of Indigenous caregivers in Canada (Jewell et al., 2022). Lastly, the fourth survey question, “Is there anything else you would like to add about the experiences, perspectives, and priority support needs of caregivers in Saskatchewan?” was determined to be confusing and/or overwhelming to survey respondents and subsequently did not collect data that was helpful to answering the specific research questions of this study. Regardless, responses to the fourth survey question have been retained for potential secondary analyses of the Saskatchewan Caregiver Experience Study's data set.
Conclusion
This study has the potential to have an impact on future research, practice, education, and policy in Saskatchewan and beyond. Considering the essential role that caregivers play in providing care to older adults in the community, focused attention should be directed toward supporting these individuals in their caregiving role. In this study, Saskatchewan caregivers were given the opportunity to share the challenges and positive aspects of their caregiving role in addition to reporting their support needs. The methods used in this study, specifically related to recruitment, was found to be successful in reaching a wide variety of participants in different geographical settings across Saskatchewan. There was much gratitude expressed by participants in their survey responses, as they were appreciative of the opportunity to share their stories. By gathering the full spectrum of the caregiver experience in Saskatchewan, we hope that our findings from the Saskatchewan Caregiver Experience Study will help to inform how communities, governments, and our healthcare system can best support caregivers in their roles. Carers Canada (2021) states on their website that the question is not ‘if you will become a caregiver,’ but rather ‘when will you become a caregiver?’ As such, it is critical that systems move towards functioning in a manner that enhances the caregiver experience.
Footnotes
Acknowledgment
We would like to thank the Saskatoon Council on Aging and their Caregiver Committee for their support in the development and launch of the Saskatchewan Caregiver Experience Study. As well, thank you to the caregivers of Saskatchewan for their interest and participation in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was received from the Saskatoon Council on Aging, a not-for-profit organization in Saskatchewan that provides support to older adults and their caregivers.
Ethical approval
Ethical approval was received for this study from the University of Saskatchewan's Behavioural Research Ethics Board (Beh ID #3377).