
Abstract
Background
The Period of PURPLE Crying Program® (PURPLE) is a universal parent education program that is delivered by nurses and health care providers to all parents/caregivers of newborns in British Columbia (B.C.). The aim of the program is to reduce the incidence of Traumatic Head Injury -Child Maltreatment (THI-CM), a form of child physical abuse.
Objective
To determine if the PURPLE program had an impact on the rate of physical abuse hospitalizations for children less than or equal to 24 months of age in B.C. since implementation in 2009.
Methods
The analysis measured physical abuse hospitalization rates for the period January 1, 1999 to December 31, 2019 and excluded any cases of confirmed Traumatic Head Injury-Child Maltreatment. Data were divided into pre-implementation period January, 1999 to December, 2008, and post-implementation period January, 2009 to December, 2019. Data were obtained from the Discharge Abstract Database and B.C. THI-CM Surveillance System to capture information on infant child abuse. Poisson regression and ANCOVA was applied to model the change in rates pre and post program implementation.
Results
Physical abuse hospitalization rates decreased by 30% post-implementation period (95% CI: −14%, 57%, p = 0.1561). The decreasing linear trend in the post-implementation period was significantly different than the increasing linear trend in the pre-implementation period (F1,17 = 4.832, p = 0.042).
Conclusions
Nurses’ role in engaging parents in conversations about PURPLE messages over multiple timepoints within a structured universal program model resulted in a decrease in physical abuse hospitalization rates since the implementation of PURPLE.
Introduction
Child abuse is a major public health concern that places children at an increased risk of injury, short-term or long-term disability, as well as negative social, mental, and behavioural outcomes. The impact of child abuse, whether physical or sexual, is reported to have significantly higher rates of depression, anxiety, suicide, interpersonal challenges, as well as other behavioural and cognitive disorders, among victims compared to non-victims (Poole et al., 2014). Physical abuse is defined as physical harm suffered by a child as a result of a behaviour by a caregiver (Fallon et al., 2021), Harm can range from shaking, pushing, grabbing or throwing, hitting with a hand or object, punching, kicking, biting, choking, poisoning, stabbing and other physical abuse forms (MacLaurin et al., 2011).
One-third of Canadians experienced a form of child maltreatment before age 15 years of which childhood physical abuse was reported by 26% of Canadians (Statistics Canada, 2017). The rate of physical abuse investigations was highest in British Columbia (B.C.), at a rate of 3.68 per 1,000 children (MacLaurin et al., 2011), in comparison to other provinces in Canada; Ontario followed with a rate of 3.33 per 1,000 children, and the lowest rate was in Quebec (1.73 per 1,000) children (Fallon et al., 2015). Of all child maltreatment investigations in B.C., 29% were deemed physical abuse, with 8% of these victims experiencing multiple forms of substantiated maltreatment including neglect and emotional maltreatment.
Bruising is the most common injury resulting from physical abuse among infants, however in pre-mobile infants, it is considered a sentinel injury and a flag for abuse (Feldman et al., 2020; Pierce et al., 2021). A subset of physical abuse is Traumatic Head Injury – Child Maltreatment (THI-CM), the leading cause of inflicted injury deaths among children less than or equal to 24 months of age in B.C. (BC Ministry of Health, 2022).
Most often, infant physical abuse begins with anger and frustration concerning an infant that will not stop crying (Gao et al., 2021; Joyce et al., 2022; Oldbury & Adams, 2015). All babies cry to communicate, with frequency and intensity varying among infants. Infant crying research shows that developmentally the fussy and crying duration is highest in the first 6-weeks of life and reduces rapidly during the following 6-weeks (Barr et al., 2005; Wolke et al., 2017). Medical problems such as chronic colic and feeding difficulties can exacerbate crying, which can increase parental frustration in response to crying. To date, the majority of child physical abuse and neglect prevention interventions are targeted at caregivers with a history of substantiated or suspected physical abuse (Barlow et al., 2006; Vlahovicova et al., 2017).
The Period of PURPLE Crying program® (PURPLE)
Since 2009 Prevent Shaken Baby Syndrome B.C. (PSBSBC) administers PURPLE (https://www.dontshake.ca), a universal free parent education intervention program to reduce the incidence of THI-CM, that is funded by the BC Ministry of Health. The program has undergone extensive evaluation, including randomized controlled trials and uses a multi-exposure delivery model to achieve consistent results that include materials, key messages and delivery timing (National Center on Shaken Baby Syndrome - PURPLE Crying, n.d.). The B.C. program reaches the parents of approximately 43,000 births (BC Vital Statistics Agency, 2022) annually encompassing 68 birthing hospitals, 123 public health & primary care units and numerous service agencies that support pre-natal moms, families and caregivers with infants/young children.
The program key messages emphasize that crying is a normal and healthy way for infants to communicate, and provides parents with tools and strategies for responding to crying in a positive and supportive way. PURPLE implementation online training at no cost is available to all health care and service providers who work with new families. B.C. maternity and public health nurses are required to take training as part of the onboarding process. Before discharge from maternity hospitals and at-home births, maternity nurses and midwives deliver the five-minute PURPLE education to all patients. Public health and primary care nurses engage parents in a three-minute conversation about infant crying and reinforce PURPLE messages during well baby check-ups and first immunization appointments up to four months of age. Community service providers 1 also reinforce messages and capture those that may not be aware of PURPLE during their interactions with families, bridging the health and social service systems. For jurisdictions that do not deliver PURPLE universally, nurses can find relevant infant crying, soothing and coping information to support new parents and caregivers in their practice by accessing PSBSBC's website at https://dontshake.ca.
Study objective
The purpose of this longitudinal study, with a pre-post intervention design, was to determine if physical abuse hospitalization rates decreased in B.C. for children less than or equal to 24 months of age after implementing the PURPLE program, as was seen in THI-CM hospitalization rates post-implementation. An eight-year evaluation of the PURPLE program demonstrated that the intervention was associated with a 35% reduction in infant THI-CM hospitalizations that was significant for children less than or equal to 24 months of age. (Barr et al., 2018).
Methods
Measures
The analysis measured physical abuse hospitalization rates for the period January 1, 1999 to December 31, 2019 among children less than or equal to 24 months of age, and excluded any cases of confirmed THI-CM. Data were divided into pre-implementation period January, 1999 to December, 2008, and post-implementation period January, 2009 to December, 2019.
Data sources
Physical abuse hospitalizations
Physical abuse hospitalizations for admissions to BC Children's Hospital (BCCH) among children less than or equal to 24 months of age occurring between January, 2001 to December, 2019 were obtained from the BC Ministry of Health, Discharge Abstract Database (DAD) (BC Ministry of Health, 2021). The external causes of injury and injury diagnoses were identified in and extracted from the DAD data, using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) codes, implemented in Canada in 2001. In addition to the code for physical abuse (T741), other maltreatment codes were extracted to ensure no cases were missed because of misclassification. The codes included, other maltreatment by parent (Y07.1), other maltreatment by acquaintance or friend (Y07.2), other maltreatment by official authorities (Y07.3), other maltreatment by other specified persons (Y07.8), other maltreatment by unspecified persons (Y07.9), assault by unspecified means, including homicide (Y09).
The coding structure changes from ICD-9 to ICD-10 that occurred January, 2001 were substantive and resulted in completely different structures allowing for more detail, but did not allow for a direct translation between the two (Centers for Disease Control and Prevention, 2022). Thus, ICD-9 coded data between January, 1999 to December, 2000 were estimated using the rolling averages of the subsequent years.
THI-CM hospitalizations
Definite THI-CM hospitalizations between the years 2007 and 2019 were obtained from the BC THI-CM Surveillance System, a reliable longitudinal incidence data surveillance system, created in 2007 to capture information on physical abuse in children less than or equal to 24 months of age in B.C. (Prevent Shaken Baby Syndrome BC, 2022). In the BC THI-CM Surveillance System, referrals to the Child Protection Service Unit (CPSU) at BCCH for physical abuse as a primary or secondary referral and/or diagnosis, were reviewed with a protocolized process by the Suspected Child Abuse and Neglect (SCAN) team (pediatricians, clinical nurses and social workers) and the PURPLE team. Using an adaptation of certainty (Feldman et al., 2001), cases were classified as definite, probable, possible, unknown or definitely not. THI-CM data for the period January, 1999 to December, 2006 were obtained from a retrospective review of relevant (CPSU) case charts.
The physical abuse hospitalization cases for children less than or equal to 24 months of age included in the analysis were obtained from removing the definite THI-CM hospitalization cases from the overall physical abuse hospitalization numbers.
Population data to calculate physical abuse hospitalization rates for children less than or equal to 24 months of age for the period January, 1999 to December, 2019 were obtained from BC Stats (BC Stats, 2022).
Analysis
Hospitalization rates per 100,000 person-years were calculated. The person-years denominator was adjusted accordingly in corresponding rate calculations. Rates were first examined for serial correlation by applying the Durbin-Watson test to a linear regression model for the square root (variance stabilizing) transformation of rates. Poisson regression was then applied to model the change in rates by including an indicator term characterizing observation from 2009 forward as post-implementation. Furthermore, trend lines were plotted to determine the pre and post-implementation period slopes. ANCOVA was used to test the difference between the slopes before and after implementation of the PURPLE program, making time (year) the covariate and the implementation state (PURPLE or no PURPLE) the factor in the analysis. Analyses were calculated with R, version 4.1.2 (R Core Team, 2021).
Results
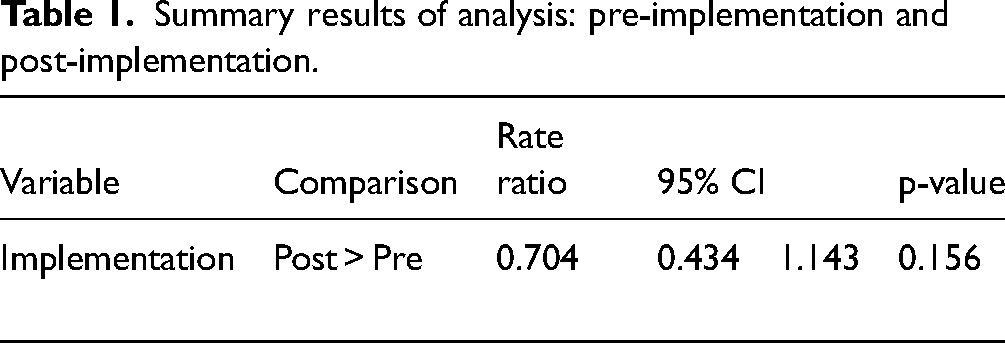
The annual trend for physical abuse hospitalization rates per 100,000 person-years is illustrated in Figure 1. A decreasing trend was observed over time. Physical abuse hospitalization rates prior to implementation averaged 4.6 per 100,000 person-years. Following implementation, physical abuse hospitalization rates decreased to 3.0 per 100,000 person-years. Durbin-Watson test did not reveal evidence of serial correlation and the Poisson regression model was applied. Table 1 shows the rate ratio, with 95% confidence intervals, from the Poisson regression model, which indicated a reduction of 30% (95% CI: −14%, 57%, p = 0.1561) post-implementation. Pre-implementation and post-implementation trend lines are illustrated in Figure 2. Linear trends showed an increase of 0.48 per 100,000 person-years per year for the pre-implementation period and a decrease of −0.73 per 100,000 person-years per year for the post-implementation period. The ANCOVA showed a decreasing linear trend in the post-implementation period which was significantly different than the increasing linear trend in the pre-implementation period (F1,17 = 4.832, p = 0.042).
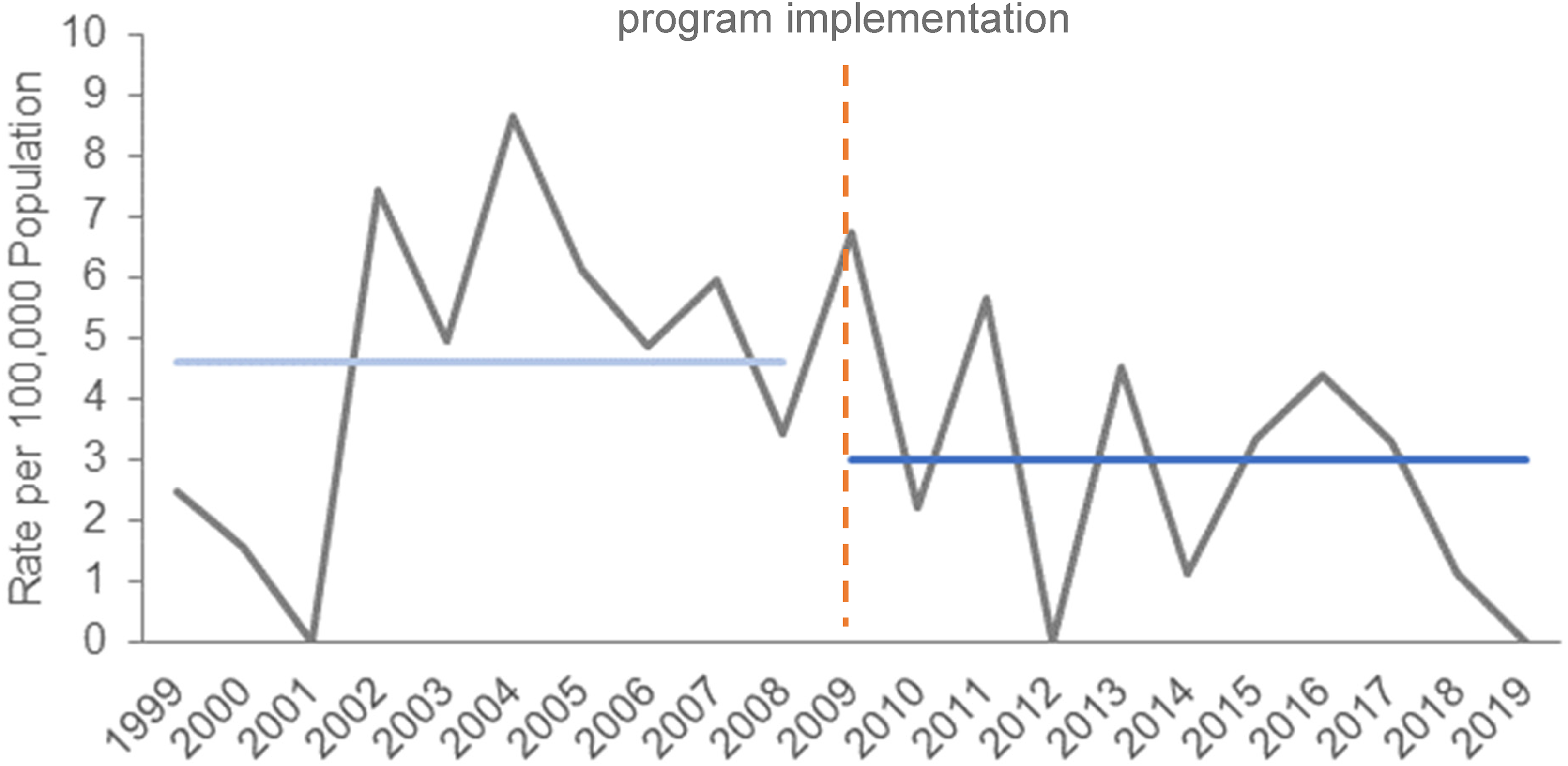
Physical abuse hospitalization rates per 100,000, for children less than or equal to 24 months of age, B.C., Canada.
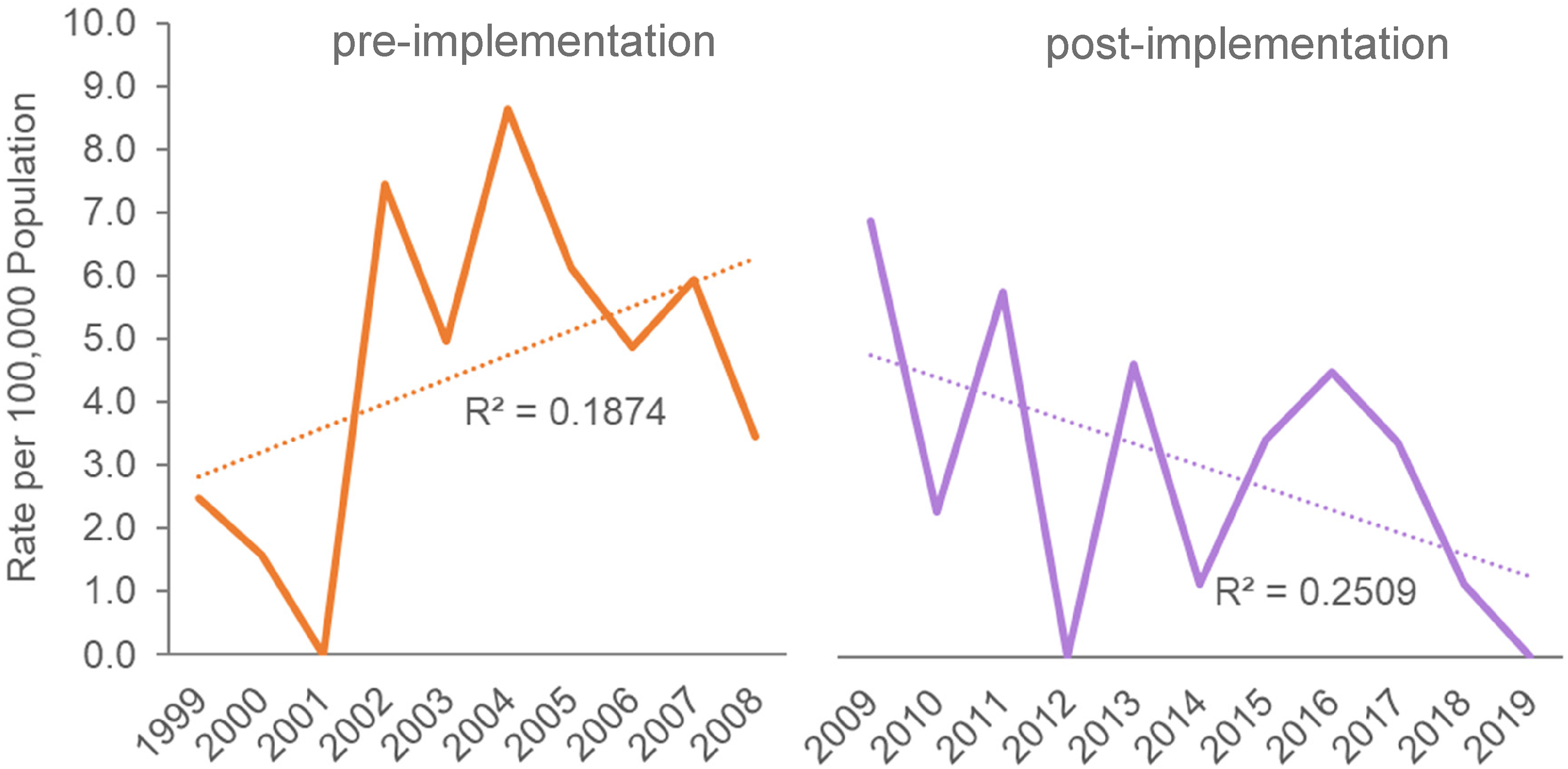
Pre-implementation and post-implementation trend lines for physical abuse hospitalization rates.
Summary results of analysis: pre-implementation and post-implementation.
Discussion
Our study objective was to determine if physical abuse hospitalization rates decreased in B.C. for children less than or equal to 24 months of age after implementing the PURPLE program. This study is the first in B.C., Canada, and results showed a 30% decrease in physical abuse hospitalization rates since the PURPLE program implementation. Although not statistically significant, likely due to the low number of case counts, this reduction was considered to be clinically important in the number of children who did not experience hospitalization resulting from a form of physical abuse, and were meaningful to stakeholders, such as the BC Ministry of Health, who fund PURPLE, the health care and injury prevention community who deliver and support PURPLE, and the families who receive this education (Armijo-Olivo, 2018). Additionally, there was an increasing trend in the pre-implementation period, and a decreasing trend in the post-implementation period. This change in trend was statistically significant. Study results aligned with previously reported outcomes of PURPLE, in a reduction of 29.5% in emergency department visits for crying complaints and a 35% reduction in hospital admissions (Barr et al., 2015, 2018).
Interventions
Interventions to address child physical abuse in Western culture have been directed primarily by an ecological approach. First theorized by Bronfenbrenner, this approach emphasizes that child abuse and neglect are influenced by multiple factors. These can include, the perpetrator's own development, the parent-child interaction, social systems, society, cultural beliefs and values, and interactions across these fields (Belsky, 1980; Bronfenbrenner, 1979; Leventhal, 2003; Sidebotham, 2001). Recognizing the factors and the interplay between them can help move beyond identification toward prediction and prevention of physical abuse. Primary prevention interventions are typically developed to modify known risk and protective factors.
To date, the majority of child physical abuse and neglect prevention interventions are targeted at caregivers with a history of substantiated or suspected physical abuse (Barlow et al., 2006; Vlahovicova et al., 2017). Home visitation programs for selected populations, like new mothers receiving welfare payments, can be effective in targeting high-risk populations and have shown reductions in child physical abuse (Chartier et al., 2017; Poole et al., 2014). These types of intervention programs approach physical abuse prevention by predominately focusing on improving the parent/child relationship through efforts to change parenting attitudes, practices and skills.
A systematic review of parenting education programs identified that although the programs were varied, they had similar goals including: increased parental knowledge about child development; effective parenting practices and skills; promote the use of non-violent parenting behaviours, and promotion of harmonious parent/child relationships (Barlow et al., 2006). Of parenting programs that include an intentional injury prevention component, home visitation programs are more common and more researched than universal programs (Nelson & Caplan, 2014; Poole et al., 2014).
In Canada the Nobody's Perfect Parenting Program, a community-based program for parents of children 0–5 years targets caregivers who face health equity barriers including; young, single, socially or geographically isolated, or have low income or limited formal education, is available in all provinces and territories (Public Health Agency of Canada, 2002). Additionally, in B.C. there are a number of parenting support programs including Parent-Child Mother Goose, Triple P Positive Parenting Program and numerous organization-based programs. Evaluation of these types of programs predominately assesses improvements in parent/child relationship, effective parenting practices, changing child behaviour, and less on specific practices related to violence and maltreatment (Poole et al., 2014). Specific to nursing practice, the Nurse Family Partnership® (NFP) home visitation program is delivered by specifically trained public health nurses (Campbell et al., 2020). The focus is on girls and young women and their children who face socio-economic disadvantages and includes intensive home visits from the prenatal period to when the baby turns two years of age. Research shows that the NFP program has been effective in reducing child maltreatment (Children's Health Policy Centre, n.d.). The challenge is that this type of programming is resource intensive.
Evaluating the cost-effectiveness of universal infant physical abuse prevention programs is challenging. However, analysis of universal versus targeted prevention programs for other health topics concludes that universal behavioural interventions have positive outcomes and resource savings. For example, universal programming for diabetes prevention in relation to the allocation of resources was identified as the best way to retain health benefits for both low and high budgets (Feenstra et al., 2011). Conversely, the cost of intervention of a program to address infant sleep problems could be even lower if more widely distributed (Hiscock et al., 2007).
Universal prevention programs and PURPLE
To be most effective, universal prevention strategies should focus on reducing risk factors that are highly preventable and modifiable (Poole et al., 2014). Research on programs that target selected populations shows that the most effective are those that are highly resourced and require high levels of participant involvement but do not have the same reach as universal programs. Research has identified three advantages of universal programs (Poole et al., 2014; Rose, 2001). First, they focus on the root causes of a problem that are highly prevalent in a population. For example, PURPLE education focuses on increased infant crying as a developmental phase and it is the most common trigger for shaking behaviour. Second, behaviour can be learned and population-level strategies help to enhance the efforts of targeted interventions. For example, PURPLE education message normalizes “It's ok to put your crying baby down in a safe place and take a break”. Third, focusing on highly prevalent risks in a population has the potential to have a large impact on population attributable risk. For example, a key message of PURPLE normalizes that all babies cry, some more than others and it is, how one manages their reaction to the crying that is important.
A working group of representatives from the BC Ministry of Health, Provincial Health Services Authority and B.C. health authorities, identified a combination of universal initiatives, and selected initiatives targeted toward the needs and issues of specific populations as best practices for the prevention of violence, abuse and neglect (BC Ministry of Healthy Living and Sport, 2010). Universal prevention programs such as PURPLE can serve as a complement to other targeted programs for high-risk or selected populations as they are less resource intensive, and can result in substantial return on investment (Masters et al., 2017; Zulman et al., 2008).
Role of nurses
Nurses have been instrumental in the success of PURPLE since its implementation. Although the structural components of delivery are fixed, the nurse/parent interaction allows for nurses’ individual practice to support the unique needs of each family. B.C. health providers follow the Patient as Partners initiative with the goal being that the patient, family and caregiver voices are incorporated at all levels of the healthcare system (BC Ministry of Health, 2020). This model emphasizes the importance of partnership between patients, families, and care providers, and aims to empower patients to make informed decisions about their care. Further, PSBSBC utilizes an iterative review process for delivery which allows for modifications based on best practice, and nurses’ feedback from quality improvement since program implementation.
Limitations
Physical abuse hospitalization cases may have been underestimated, as cases are not always reported to either the police or child protection services (Afifi et al., 2015; Schilling & Christian, 2014). Abuse may not have been disclosed and therefore, may have been diagnosed as unknown or suspected by the investigating physician. Coding of physical abuse in DAD is conducted by professionally trained coders who follow guideline standards defined by the Canadian Institute of Health Information. The coding assignment is influenced by physician's chart documentation and coder interpretation, which may contribute to an underestimation of cases. Perhaps with future introduction of ICD-11, there may be better definitions and tracking of these codes. A lack of knowledge in child abuse and the social implications of misdiagnosing physical abuse (fear of potential legal implications) may have influenced physician charting (Lupariello et al., 2022). Physician documentation could be improved by providing more background detail on circumstances and risk factors (ecological approach) for physical abuse.
The number of definite physical abuse hospitalization cases in B.C. for children less than or equal to 24 months of age during the study period was small and made it challenging to conduct any descriptive or additional analyses. To have obtained numbers that allowed for meaningful analysis in order to achieve significant results would have necessitated the study period to be so long, as to not be feasible.
Finally, this study only looked at the association of physical abuse hospitalization rates decreasing in B.C. for children less than or equal to 24 months of age in relation to pre-implementation and post-implementation of PURPLE. There were other intervention programs for physical abuse prevention in B.C. within the same time period that may have had an impact on the results, however, they were outside of the study scope.
Conclusions
Universal provision and delivery of PURPLE education and resources by nurses and health care providers may have played a role in the reduction of physical abuse hospitalization rates in B.C. for children less than or equal to 24 months of age. Nurses’ role in engaging parents in conversations about PURPLE messages over multiple time points helped reinforce informed choices and decisions in building the skills needed for parenting and infant care. While results failed to reach statistical significance, we regard this reduction in physical abuse hospitalization rates to have clinical importance, resulting in fewer children less than or equal to 24 months who experienced physical abuse.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.