
Abstract
Study background
Gender-based violence is a global concern. The perinatal period is a crucial time for early identification of the harmful impact of violence on the well-being of both mothers and infants. However, it has been observed that many women choose not to disclose their experiences to their healthcare providers.
Purpose
To gain insight into this issue, a study was conducted to explore the perspectives of both survivors and healthcare providers regarding the barriers to disclosure.
Methods
Through the utilization of a thematic analysis approach, a total of 28 interviews were conducted, involving 12 survivors and 16 healthcare providers.
Results
Data analysis revealed barriers to disclosure at the individual, community, and healthcare system levels.
Conclusion
Health-care providers have a pivotal role in creating an atmosphere where women are encouraged to break the silence and a paradigm shift in the health system approach towards GBV is necessary.
Introduction
Gender-based violence (GBV) is one of the most common problems facing women, girls, and gender-diverse people around the world, including Canada. GBV encompasses any act of abuse or violence that may result in physical, sexual, or psychological harm or suffering perpetrated against someone specifically because of their gender, whether occurring in public or private life (Ali, 2018; Beydoun & Beydoun, 2014; Guillery et al., 2012). According to the World Health Organization (WHO), one in three (35%) women worldwide will experience at least one instance of GBV in their lifetime (Violence against Women, n.d.).
Pregnancy does not offer protection from GBV. It is estimated that one in ten women who have been subjected to intimate partner violence was pregnant at the time (Taillieu et al., 2016). A multi-nation study on violence against women found that between one-quarter and one-half of women who experienced physical abuse during pregnancy were punched or kicked in the abdomen (García-Moreno et al., 2005). Unfortunately, violence during the perinatal period is highly predictive of ongoing violence (Edin et al., 2010). In Canada, the prevalence of physical abuse during pregnancy has been estimated as being between 3.3% and 6.6% (Stewart et al., 2017). The Government of Canada has made a long-term commitment to eradicate GBV in both the public and private spheres (Government of Canada, n.d.). A 2016 study estimated that Canadians collectively spend $7.4 billion annually on the aftermath of intimate partner violence (Canada Still Has Work to Do, 2018) and this is likely an underestimate.
Impact of perinatal GBV on maternal and infant outcomes
Violence experienced during the perinatal period may have severe negative physical and psychological consequences for mother and baby (Alhusen et al., 2015). Women who experience GBV consistently report negative impacts on their physical, mental, and reproductive health (Perrin et al., 2019). Placenta abruption, preterm birth, low birth weight newborns, and antepartum hemorrhage are among the negative consequences of perinatal GBV (Guillery et al., 2012). Experiencing violence during pregnancy has also been strongly associated with postpartum depression, negative parenting practices among mothers, and cognitive and behavioral problems in children. The harmful effects of violence on maternal, fetal, and infant well-being make the perinatal period a critical time for early identification and timely intervention (Velonis et al., 2017).
Disclosure of GBV during perinatal care
Usually, women have more contact with the healthcare system during pregnancy than at any other time in their lives (Devries et al., 2010). As a result, healthcare providers (HCPs) may have sufficient time to build trust and develop a relationship that supports disclosure during perinatal care. However, despite the suspected high prevalence of GBV during the perinatal period, few women disclose their abuse to a healthcare provider (Cherniak et al., 2005; Martin et al., 2001; Pokharel et al., 2020). Underreporting, reluctance to disclose and failure to seek help have been documented worldwide (Palermo et al., 2014). In a secondary analysis, Palermo et al. (2014) explored the determinants of violence disclosure to formal authorities, such as healthcare or legal professionals, police, and nongovernmental organizations. Based on an analysis of demographic and health survey data from 300,000 women from 24 developing countries they identified a vast gap between the prevalence of violence (40%) and the rate of violence disclosure (7%) (Palermo et al., 2014). Similarly, Daruwalla et al. (2019) found that 40% of survivors reported disclosing violence to a friend or relative, but only 7% to a formal source of support such as the health care system or police.
In a study conducted in Ontario, Canada, among 1182 participants, 15% of female patients reported violence, but only 2% disclosed it to a healthcare worker (Catallo et al., 2013). Several reasons have been proposed to explain these low disclosure rates. For example, HCPs may be reluctant to ask direct questions about the history of violence; however, evidence suggests that abused women who have experienced GBV express some support for being asked about violence (Edin et al., 2010). Silence in the face of GBV may be influenced by family beliefs and cultural and religious backgrounds (Kalra & Bhugra, 2013). Moreover, some women do not disclose due to fear of losing custody of their children (Bloom et al., 2020). The community where women are raised and live can either encourage or deter dialogue about GBV and disclosure (Beydoun & Beydoun, 2014).
The barriers to disclosing GBV to HCPs in British Columbia, Canada have not been fully explored. Moreover, women's perspectives on experiences of perinatal GBV regarding disclosure to HCPs have not been explicitly compared with the views of perinatal HCPs themselves. Therefore, this study aimed to explore both survivors and HCPs’ experiences about their perceptions of the barriers to disclosing experiences of violence during the perinatal period.
Methods and design: To investigate the barriers to disclosure among survivors of GBV during perinatal care, we used a qualitative research approach and performed an inductive thematic analysis. All aspects of the methods used were the same for both survivors and HCPs.
Method
Participant recruitment
Participants were selected using a purposive sampling technique in an iterative cycle of data collection and analysis, and recruitment continued until sufficient knowledge regarding the research questions was obtained, and no new themes emerged. Participants were recruited through advertisements on social media (i.e., Facebook and Instagram) and through notices placed in public places such as gyms, shopping malls, shelters, family services, and courts. Printed posters were placed in common areas such as streets around the hospitals and on hospital bulletin boards.
Procedures
After participant recruitment, they were given the option of either face-to-face or telephone interviews. In qualitative research, when face-to-face conversations are not possible, telephone interviews are widely used to conduct in-depth interviews (Saroha & Moulik, 2020). Midway through the study, only telephone interviews were offered due to the onset of the COVID-19 pandemic and limitations on gatherings for research were imposed. In order to consider maximum variation, survivors with diverse identities (including those identifying as Indigenous and immigrants) were recruited.
The UBC C&W Research Ethics Board approved this study (Approval number: H19-02,409).
The researchers ensured that the appropriate procedures were followed regarding informed consent, anonymity, autonomy, and maintaining confidentiality.
HCPs were recruited from different parts of British Columbia. The survivors were from several various metropolitan centres in British Columbia (Tables 1 and 2 show the demographic characteristics of HCPs and survivors).
Demographic characteristics of health care providers.
Demographic characteristics of survivors.
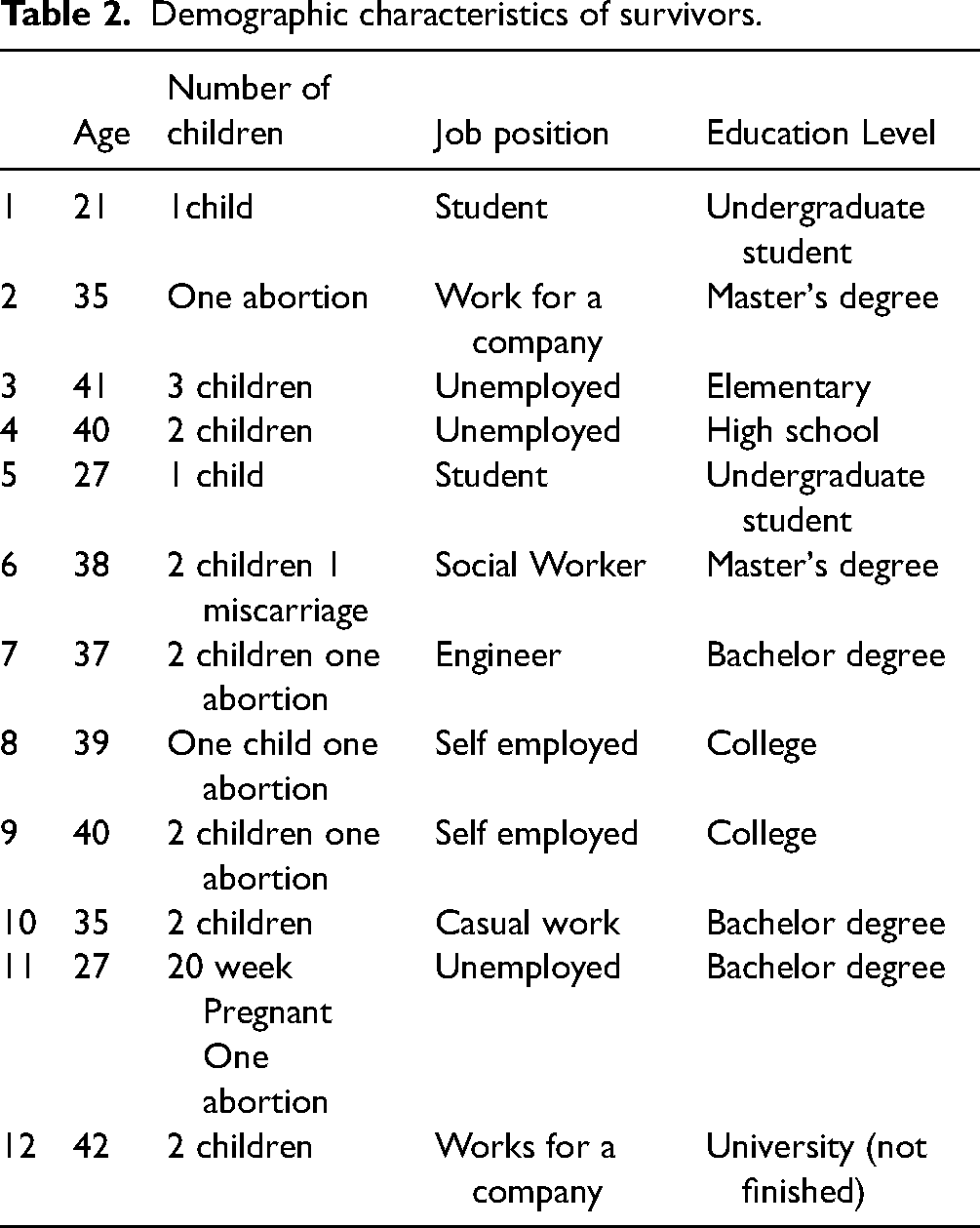
In terms of inclusion and exclusion criteria, the participant had to be between the ages of 18–49, have been pregnant during the last five years, have a self-reported history of gender-based violence in the same period, and be able to speak conversational English. The only inclusion criterion for HCPs was having experience providing perinatal healthcare to women with a history of gender-based violence.
Lincoln and Guba's proposed criteria for rigor in qualitative research were considered (Nowell et al., 2017). Therefore, we addressed the credibility of the findings through prolonged engagement and debriefing among members of the research team. We returned to the raw data to ensure that themes reflected the participants’ voices. To enhance the trustworthiness of the thematic analysis, we repeatedly read the transcripts and undertook prolonged engagement with the data. Themes and subthemes were reviewed and discussed among team members. One of the researchers traced the audit trail using the interview notes and transcripts to establish the inquiry process. We kept a reflective journal to assist with establishing confirmability and prevent insider bias. To increase the transferability of the findings, we generated a complete description of the study participants, the research process, and the study context.
Data analysis
Thematic analysis was used to identify, analyze, and report patterns and themes within data (Braun & Clarke, 2006). Immediately after each interview, the audio files were transcribed verbatim and analyzed (Nowell et al., 2017). Each interview's entire text was read several times; this technique helped us identify meanings and possible patterns in the text. Two of the researchers did an independent analysis. The units were labelled based on their content, and a list of codes was created. The interesting features that were deemed to be relevant to the research aims were highlighted systematically. Codes were organized into meaningful groups according to their similarities and differences. Initial codes were identified, and the various codes were sorted into potential themes and subthemes. The final extracted codebook was discussed, and some themes were modified; finally, researchers came to a consensus about the name of each theme, and then themes and subthemes were discussed with the rest of the research team.
Results
Twenty-eight interviews with two groups of participants were conducted simultaneously (twelve interviews conducted with survivors who had been pregnant within the last five years and 16 interviews with HCPs who provided care for survivors, including five midwives, five nurses, and six physicians. Each interview lasted 30–60 min.
The perspective expressed by survivors were mirrored in the experiences provided by HCPs and thematic analysis suggested that both survivors and HCPs shared a number of similar perspectives, presenting the findings from both groups together.
Overview of main themes
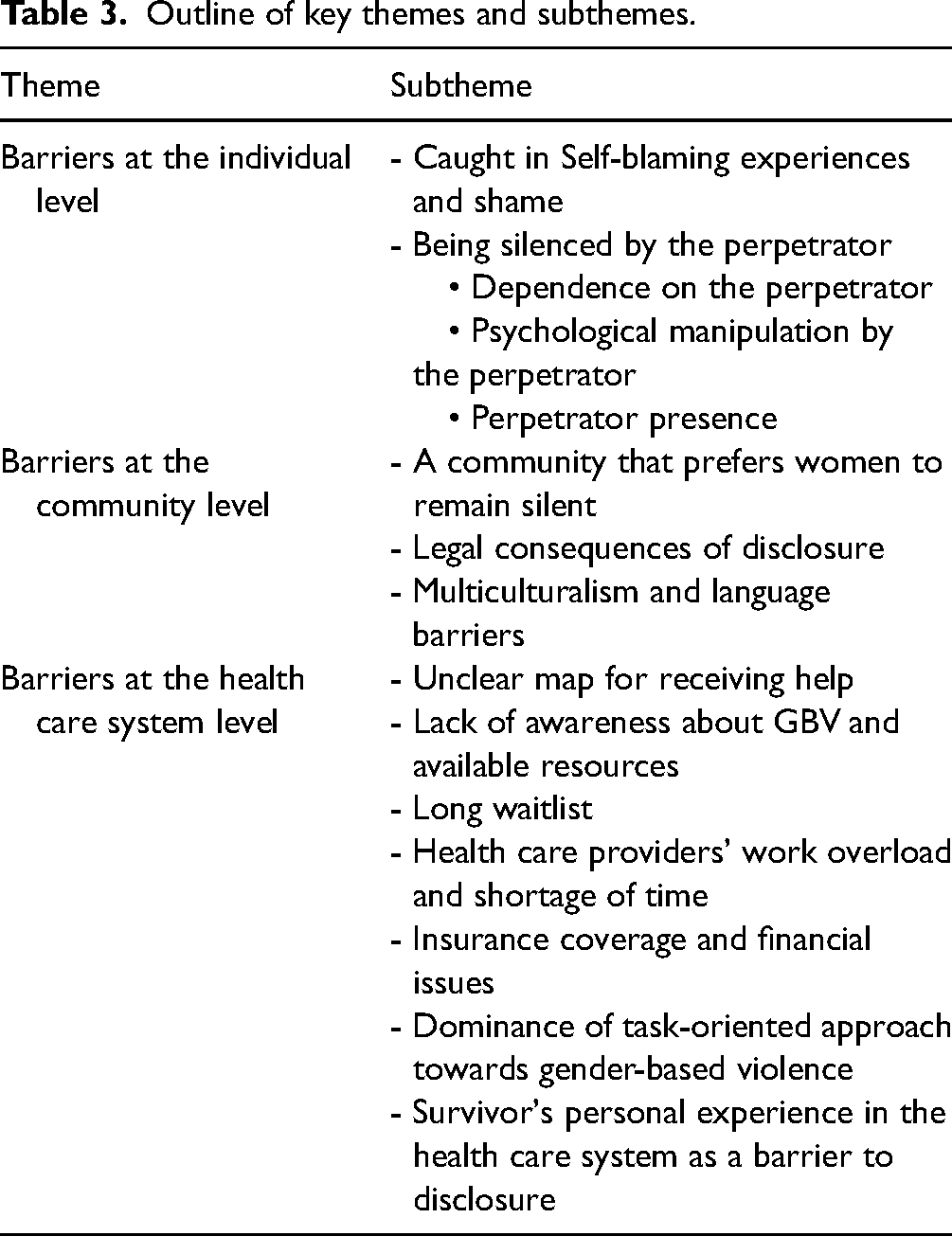
The analysis and research group discussions generated three main themes and 12 subthemes (see Table 3). Barriers at the individual level, barriers at the community level and barriers at the health care system level were the three main themes that emerged from the data analysis, and each of them had its subthemes. We describe these themes with illustrative quotes and identify whether they were from the sample of women with a history of GBV (survivors) or the sample of HCPs (or both).
Outline of key themes and subthemes.
We observed that HCPs and survivors shared the same worldview, which is reflected in their observations and comments regarding perinatal violence. For example, some health professionals expressed their perspectives about the underlying reasons for women not disclosing GBV. Although non-disclosure of violence was the direct experience of women, not HCPs, it was valuable to hear providers’ perspectives on this issue, especially as it was, in most cases, consistent with women's experiences.
Barriers at the individual level
Based on the participants’ reports, some factors that hinder disclosure are rooted in individual factors and factors related to the perpetrator. In many cases, survivors censored themselves, though in some cases, a perpetrator discouraged disclosure.
Caught in self-blaming experiences and shame
Some participants explained that they did not disclose their experiences and had come to believe that violence was their fault and blamed themselves for the situation. Some mentioned that feeling embarrassed and ashamed made them stay silent. Survivors reported that they were under pressure to stay silent. Some also said that they were aware of these pressures and became used to them, considering it something that should be accepted. “A 40 yr old survivor explained: I accepted it; I didn’t understand what was happening. I thought it was my fault. You know, I’m unreasonable. You know, like probably he's working so hard. He's so stressed and makes excuses for him and accepts it all.”
Being silenced by the perpetrator
Survivors also mentioned the perpetrator's presence, dependency, and psychological manipulation as barriers to disclosure. Self-censorship and being censored by others, particularly the perpetrator, were mentioned in their interviews. “Yeah, I just scared. I just felt like, no matter what, he was gonna find out and like he was threatening my life towards the end so. It was, it was just too scary even to say it out loud.” (37 yr old Survivor)
Dependence on the perpetrator
Some participants reported an emotional dichotomy between fear and dependence on the perpetrator. Women reported that the fear of their perpetrator's threats towards them was another contributor to remaining silent. A 35 yr old Midwife mentioned: “They also like to care about the person who's doing it. Maybe rely on them for housing; they might rely on that person (Perpetrator) for child care.”
Some survivors were also worried that their partners would leave them if they disclosed the violence. A 39 yr old Survivor explained: “Fear of him leaving me even though that is not a good thing it did not feel like a good thing to me at that time because I did not want to be alone.”
Psychological manipulation by the perpetrator
Some participants stated that they were manipulated by their partners and were convinced that their experience was not real. In this regard, a 47 years old nurse mentioned: Sometimes, it's hard to change mindset when they are already all their life, they are being overpowered, overruled, and manipulated, and they don't think this is violent. “In my case, I didn't believe it was real. He had me convinced that nothing was wrong. He had me convinced that I was crazy because of my pregnancy hormones, I was a problem, and he was fine; he was normal. Everything was my fault. So, it never even occurred to me to talk about it because I just believed that.” (42 yr old Survivor)
A 39 years old survivor explained that she was emotionally abused and brainwashed by her partner. She expressed: Uh, I felt trapped most times. And I was brainwashed into thinking that he wasn't abusing me, and it was all in my head, making it up.
Perpetrator presence
Survivors mentioned that the presence of their partner during health care was a significant obstacle to disclosure. Cause it was uncomfortable. My partner was always sitting next to me. (39 yr old Survivor)
Another participant explained: “I would never have admitted anything while he was there. I'm still afraid, even calling or sending emails or anything. I feel like he's watching me. Like, I still take precautions. And he hasn't lived with me for a few years.” (40 yr old Survivor)
Healthcare workers also stated that a partner's presence during healthcare visits prevents them from asking women about their history of violence. A 36-year-old midwife echoed the survivors’ perspective and mentioned: A partner who is abusive will make sure that he is at every single appointment to silence someone from telling a health care practitioner.
Barriers at the community level
One of the main themes in the study was the role of context and community in preventing disclosure; it seemed that society was not yet ready to hear the voices of survivors.
A community that prefers women to remain silent
Many women reported perceiving societal pressure to remain silent. They described feeling a sense of social blame for the violence committed against them. Victim blaming and holding women responsible for the situation can prevent women open up a conversation about violence. They were afraid of what others might think of them. Participants felt that GBV was not taken seriously on a societal level and that this contributed to their non-disclosure. This is how one of the survivors described her experience: A 40 yr old Survivor mentioned: “In society, they just don't recognize it as something serious. They just kind of thought well men behave like men. It's just this cultural and social thing about oh ya, you're probably going to be mistreated, and he's not hitting you, so it's okay.”
HCPs reflected that the social context did not respect survivors. A 59 yr old Midwife explained: So I would definitely say society doesn't want to hear about sexual assault and violence. It just like most things with the status quo.
Legal consequences of disclosure
The aftermath of disclosure and the consequences women and their children might face made some survivors stay silent. They worried about entering the dark tunnel of the justice system. In particular, women worried about losing custody of their children, as exemplified in the following excerpts. A 41 yr old survivor mentioned: “I would say because they're like scared. Like from my experience, I was scared like “What if they call the ministry? What if they call, you know?” Yeah, that's probably the most common would be the fear of losing their children, or losing, you know, their home, of losing, you know, their partner. Yeah, it was for me it would be the biggest.”
HCPs recognized this fear among their patients. A 36-year-old midwife stated: They're afraid of having their children taken away from them. I think that it can be difficult for them to seek help because of the repercussions.
Concerns for family status, separation and children's custody were addressed as barriers to disclosure. A 35 yr old Midwife explained: “There could be very complex legal circumstances happening in that situation … A lot of the systems that exist are punishing and remove families or like separate families from their members. If we refer them to social work, they have the potential to be flagged.”
Multiculturalism and language barriers
Participants believed that the issue of violence and perceptions of women about GBV varies among different cultures. In particular, HCPs noted that language barriers likely prevent women from disclosing their experience with violence.
One of the participants noted cultural differences as follows: Disclosing sexual violence is not conventional in our culture, and women keep it hidden from others. The person who sexually assaulted me was a relative, and after that incident, my family tried to ignore the issue. (35 yr old Survivor)
A 48-year-old physician also referred to the language barrier and mentioned: Sometimes, the language barrier is a challenge for women because they have concerns about their safety and the presence of an interpreter.
According to the participants’ experience, cultural norms are different among people with different ethnic backgrounds, and some families may press survivors to remain silent: A 36-year-old midwife said: Different cultures often treat each other differently than our sort of Caucasian Canadian culture. And so, I don't have one thing that fits all families.
Also, an experienced midwife with a long history of taking care of survivors shared her experience as follows: “Well, I think big barriers are certainly very much if one is new to a region or new to a country, one might be worried about all those implications, which may be really important in terms of immigration, in terms of policing, in terms of the court in terms of what it would mean for your partner, if he gets treated worse because of her culture, maybe by the police officer. So there are many layers of violence that aren't just about gender. Like the connections between racism and gender-based violence, and all of you know, in terms of new immigration, or health care, like, I think that's a big thing.”
Barriers at the level of the healthcare system
Both women and HCPs argued that some rules and regulations in the healthcare system could prevent women from disclosing violence. These related to not understanding the procedures for accessing and receiving support as well as an overall lack of knowledge about available supports.
Unclear map for receiving help
It was evident from women's stories that the path to help was not clear. This winding path made some survivors give up seeking help and disclosing their experiences. A survivor who was 38 years old mentioned: “I didn't know what steps I should take. I ended up homeless for six weeks. If I had access to just a couple different resources, I might have taken a few steps differently at the beginning that might have changed the trajectory of this of the whole experience.” “I have been navigating the healthcare system for eight years now. After two years of practicing and six years of being a midwifery student, I still find it difficult to navigate our hospital system. So, someone who is less privileged, has fewer resources, perhaps can't get around, then It's gonna be very difficult for them to access these types of resources.” (36 yr old Midwife)
Another midwife expressed her concerns about the fragmented health care system and mentioned that the dominance of a holistic approach over the existing biomedical one could be a solution. “Each hospital is its own island, and there may be putting you on a waitlist. And we're talking about weeks to months or something that should be dealt with within a day or two. There needs to be a more holistic approach to our healthcare system as well. It's so fragmented.” (35 yr old Midwife)
Lack of awareness about GBV and available resources
Lack of awareness about the available local resources in the healthcare system and being unaware of different types of abuse and violence made some survivors remain silent. A 42-year-old survivor talked about the lack of access to resources. She said: There's not a lot of information out there. So yeah, I would have loved to know more about different assistance programs. In fact, not knowing where to go and whom to talk to prevented women from receiving support was mentioned by the survivors. Lack of awareness was explained by one of the participants as follows: “Yeah, cause a lot of women don't know what it is? And they don't know they're going through it until they actually see a piece of paper on the wall about it. I didn't know about it until like three years ago, and I saw it on a piece of paper.” (40 yr old Survivor)
Long waitlist
Participants in their interviews described the issue of a long waitlist and referred to it as a hurdle for disclosure. A 27-year-old survivor said: I went to a couple of thousand services, and then I was on a waitlist for a trauma program at the hospital. I never got into the program, even though I was on it for a couple of years.
Another survivor had the same concern and talked about her experience as follows: “I'm just in the intake process, so I'm just waiting for it. I went there a few months ago, but then this coronavirus thing started. I couldn't get in to see him, and there was a two-week wait needed to see him immediately, and I had to go to a clinic, and it was terrible.” (37 yr old Survivor)
Health care provider's work overload and shortage of time
Participants believed that physicians did not have enough time and perceived it as an obstacle to disclosure. In her interviews, one of the survivors expressed dissatisfaction with short appointments where there was not enough opportunity to discuss issues like violence and shared her experience as follows: “So if my doctor takes more than 15 min to talk to me, he can't bill for his time, which is why the clinics race through the people so fast. I don't know how to fix the system, but I think that needs change. I think everyone needs to have a doctor, and the doctor should be able to take the time they need to get to the bottom of the problem.” (37 yr old Survivor)
A 35 yr old survivor has mentioned that the person who has been subjected to violence will not disclose her experience if she notices that the care provider is in a hurry. “I think the main thing I found difficult with care providers is that they always seem to want to get you out the door as quickly as possible, and I think that is very difficult for anyone who is dealing with violence because it is difficult to quickly say, ‘This is happening, please help me.”
Insurance coverage and financial issues
Many survivors reported being unable to afford the costs of counselling and psychologist visits as neither is fully covered by most insurance and many survivors of GBV are unable to pay from their own pocket. This causes many survivors to refrain from disclosing and seeking help
Dominance of task-oriented approach towards gender-based violence
According to the HCPs, medical illness dominates their day-to-day work, offering limited opportunity to focus on the psychosocial aspects of health unless these are brought forward by the patient, including gender-based violence questioning. A 45-year-old physician said: So I think yeah, we tend to probably think of things too simplistically and be very task-oriented vs just being relational.
A 41 yr old Physician shared her experiences as follows: I admit that we sometimes neglect it just because we think other medical issues are more important. In the units, talking about social issues usually doesn't happen during rounds. (41 yr old Physician)
Survivor's personal experience in the healthcare system as a barrier to disclosure
Some participants did not hold out much hope of the overarching system being able to change things. Traditionally, the healthcare response to reporting violence has been inconsistent; some women reported this as an obstacle to disclosure. Others mentioned that the healthcare system could not help them anyway. Most participants did not know that identification of GBV is within the scope of HCPs’ practice. One of the participants shared her personal perspective as follows “Oh, I don't think there is anything they could have done that could have helped. Cause it's none of their business. What could they do to help anyway? They only handle medication; why would I talk about it? They don't pay attention.” (37 yr old Survivor)
A 35-year-old midwife expressed mistrust of the healthcare system: “People don't trust health-care providers to be able to hold those complexities. They know that health care providers have the duty to report very serious legal ramifications for their families. So they don't feel health care providers as safe people who actually have any kind of solutions for them. And so why would you report? Maybe if your life was like in imminent danger, and you were going to die, but that's not the case for most ongoing like gender-based violence.”
Both survivors and HCPs recognized that previous experiences with the health care system significantly impacted the extent to which survivors disclosed their experience with violence. Specifically, women shared stories about feeling like the broader health care system may have inadvertently violated them. Thus they experienced this as a major barrier to disclosure about their GBV during the perinatal period. A 35-year -old survivor expressed her negative experience with HCPs and stated: Any kind of Gynecological help I received in the past has been deeply traumatic.
Another participant expressed her experience in the health care setting and mentioned that these experiences made her not disclose her history of violence. “I had the pregnancy test done, and the nurse was beyond the desk at the time, she was asking like very rude to me. She was upset like I wasn't on the proper birth control. And then later she went straight to talk about abortion! She said straightaway to me, I don't think that having another baby is the best decision for you.” (40 yr old Survivor)
A midwife addressed an important issue and explained that previous experience of abuse in a healthcare setting act as a significant barrier to disclosure. “It's a really important conversation that we need to have around people experiencing GBV in the medical system and how in this medical system if they have experienced violence it's going to be harder for them to disclose, and ask for help, because, unfortunately, a lot of the violence happens in the healthcare system to women and trans person bodies when accessing care.”
“It's important to note that overwhelmingly black women, people with color, trans women, all of them are going to experience a higher rate of gender-based violence in the healthcare system. So I think that is a really important thing to discuss.” (36 yr old Midwife)
Finally, the fear of being judged and not being believed made it more difficult for survivors to talk about traumatic and personal experiences. A 40 years old survivor mentioned: Being believed is another issue, the fear that someone won’t believe you. That's really all I can think of, in my particular case. Another survivor (41 yr old) also talked about the judgmental approach of some care providers and said: Because I know a lot a couple times even though what they were saying to me was judgmental.
Discussion
According to our findings, there are a number of barriers that hinder the process of GBV disclosure. These barriers are at the individual level, community level, and the healthcare system level. Personal, interpersonal, organizational, and sociocultural factors influence survivors’ willingness to disclose and their help-seeking behaviours (Overstreet & Quinn, 2013; Parvin et al., 2016).
Self-silencing and being silenced by others was significant finding in this study. A stereotype exists among some people who believe that individuals are responsible for becoming exposed to violence (Overstreet & Quinn, 2013). From this perspective, women subjected to violence possess a deeply stigmatized identity. Therefore, some survivors have concerns about what will happen to them if this stigmatized identity is revealed to others. They blame themselves for what happened to them and prefer to stay silent (Overstreet & Quinn, 2013).
Gender-based violence (GBV) during the perinatal period is a pressing global concern. The discussion section presents compelling evidence from diverse contexts and cultures, shedding light on the widespread nature of this issue. In some communities, there may be tacit acceptance of intimate partner violence, which leads to stigma and shame upon survivors (McCleary-Sills et al., 2016; Murphy et al., 2020; Overstreet & Quinn, 2013; Parvin et al., 2016). For example, in a study conducted in Malaysia, the findings revealed a state of silence or the “unspoken agreement” between women who experience violence and other community members, and disclosure of violence is prohibited in this unspoken agreement. According to the authors of that study, the failure to address these abusive experiences further compounded women's feeling of voicelessness to receive appropriate support and medical care (Othman et al., 2014). In a community that is not prepared to talk about violence, survivors may be reluctant to disclose it because of the fear of bringing shame and embarrassment to their families and communities (Kasturirangan et al., 2004; Parvin et al., 2016). The survivors in our study refer to the sociocultural stigma of the disclosure. They believe that care providers are part of the same society and are under the influence of the same viewpoint; this finding aligns with the findings in other studies (Abavi et al., 2020). It has been demonstrated that a community approach toward supporting or not supporting survivors and disclosure of violence affects women's willingness to disclose their experiences.
We identified a number of contextual factors that may act as barriers to disclosure. In multicultural Canada, women from diverse backgrounds and ethnicities coexist and live together. Women's response to violence and disclosure can vary based on their culture and ethnicity. Specific cultural values can act as barriers to discussing the abuse with HCPs. In this regard, studies on help-seeking behaviors among Asian women have revealed that most women in Asian countries believe that family matters, including domestic violence, should be kept secret (Othman et al., 2014).
Our findings regarding the perpetrator's presence, fear of more threat, and further violence align with the results of other researchers (Othman et al., 2014; Vranda et al., 2018). Also, participants referred to their dependency on their perpetrator as another factor behind their choices to remain silent. This dependency can be emotional or financial. Therefore, some survivors do not feel ready to live a separate life from their partners (Kasturirangan et al., 2004; Othman et al., 2014).
Moreover, our study's lack of awareness about GBV and available resources deter women's help-seeking behavior and disclosure. Researchers emphasize raising awareness and providing information about the available local services and resources. It has been suggested that education about GBV and the available resources could lead to more disclosure and service uptake (Parvin et al., 2016).
In the current study, participants talked about their concerns regarding the aftermath of disclosure and its legal consequences. Some care providers require a police report before providing services, which may hamper disclosure (Murphy et al., 2020). In line with the findings of the current study, in a project conducted in Ontario, Canada, women expressed that they were reluctant to disclose because they were concerned about the possible interference of the legal authorities, particularly the involvement of police and child protection services (Catallo et al., 2013).
The study participants talked about the challenges survivors face on the path to receiving help. They explained that these issues might deter disclosure and help-seeking behavior. Uneasy access to supporting resources can prevent disclosure and help-seeking behaviours (Parvin et al., 2016). Some participants of this study also expressed mistrust of the healthcare system. One possible explanation may be based on their previous negative experience with the health system. Studies show that past experience with HCPs impacts women's perception and trust in the healthcare system. While some women express satisfaction with their healthcare professionals, others are disappointed with their responses, and distrust hinders their willingness to disclose (Othman et al., 2014).
The participants of this study mentioned a fear of being judged and not being believed. Other studies report that many survivors of violence experience adverse reactions like blame and disbelief from formal care providers and criminal justice personnel (Lanthier et al., 2018). Consistent with the findings of this study, in a qualitative study conducted in India, women were concerned about not being believed in the healthcare system, particularly when there was emotional or verbal abuse with no physical symptom to indicate their experience of violence (Vranda et al., 2018).
The experience of violence while receiving healthcare itself was raised in this study as a barrier to disclosure. Vedam et al. (2019) conducted a study on mistreatment during pregnancy and childbirth in maternity care in the United States. They found that one in six women (17.3%) reported experiencing one or more mistreatment. According to their findings, prejudice against certain population groups has been reported. Still, mistreatment has been more frequently experienced by women of colour and those who have social, economic, or health challenges (Vedam et al., 2019). Similar findings have been reported in other studies. Violence in healthcare settings may happen in different forms, such as neglect, verbal violence, rough treatment, threats, physical violence, shouting, intentional humiliation, and denial of pain relief when the patient is suffering (D’Oliveira et al., 2002). In another study conducted by Abavi and colleagues (2020), some of the care providers’ harmful responses disengaged survivors from help-seeking. According to their research, survivors received unsympathetic and blaming responses, invalidating their expressions and burdening them with guilt. These hurtful responses have counterproductive effects in preventing women from disclosing their experiences to health care providers and can re-traumatize survivors (Abavi et al., 2020).
In our study, difficulty accessing services due to a long waitlist and financial obstacles, such as the payment of counselling fees, presented obstacles to survivors’ disclosures. In fact, many insurance companies do not cover the cost of some support services. A recent study by Abavi et al. (2020) also referred to long wait times, the lack of affordability, and being located far away from services as disclosure barriers.
Finally, our findings suggest providers in the healthcare system tend to focus on task-based medical care and hesitate to probe deeply into psychosocial questioning unless a patient provides reason to do so. In a system, which is task-oriented, attention to issues such as GBV is diminished (Byrne et al., 2020; Van Dulmen et al., 2015).
Limitations of the study
Having access to women with pregnancy experiences and gender-based violence was a challenge. Moreover, the COVID-19 pandemic affected the participant recruitment and research process. As a result, instead of a face-to-face interview, some interviews were conducted by phone.
Clinical implications
A paradigm shift in the health system approach towards GBV is necessary (van Dulmen et al., 2015). Paying attention to the social determinants of health should be emphasized during healthcare workers’ training programs (Andermann, 2016). HCPs can intervene and connect women to appropriate resources. By creating a safe and supportive environment, healthcare settings can play a crucial role in encouraging women to disclose their experiences of violence (Beydoun & Beydoun, 2014; Mirlashari et al. 2023).
Future recommendations
Enhancing Education and Policy: In light of the valuable insights gained from both survivors and healthcare providers (HCPs) in our study on the barriers to disclosure of gender-based violence during perinatal care, we propose the following future recommendations for education and policy development. The convergence of perspectives from these distinct participant groups allows for a nuanced approach to addressing the pervasive challenges identified.
1. Curriculum Development for Healthcare Providers: Tailored Training Programs: Develop specialized training programs for care providers that specifically address the nuances of identifying and handling disclosures of gender-based violence during perinatal care. These programs should incorporate insights gained from survivors and focus on building empathy, communication skills, and trauma-informed care.
Interdisciplinary Collaboration: Encourage interdisciplinary collaboration within the healthcare system by incorporating perspectives from various healthcare professionals, including obstetricians, midwives, nurses, and social workers. This collaboration can foster a comprehensive and cohesive approach to addressing gender-based violence.
Cultural Competency Training: Implement cultural competency training within healthcare provider curricula to ensure that professionals are equipped to navigate diverse cultural contexts sensitively. This can enhance their ability to understand and respond effectively to the needs of survivors from various backgrounds.
2. Policy Recommendations: Standardized Protocols: Advocate for the development and implementation of standardized protocols within healthcare settings to guide the identification and management of gender-based violence during perinatal care. These protocols should outline clear procedures for assessment, documentation, and referral, emphasizing survivor-centered and trauma-informed care.
Integrated Support Systems: Work towards the integration of support systems within healthcare institutions, including access to counseling services, legal assistance, and community resources. Policies should encourage collaboration between healthcare providers and external organizations to ensure a holistic and supportive approach for survivors.
Regular Continuing Education: Establish a system of regular continuing education for healthcare providers to stay updated on evolving best practices and research in the field of gender-based violence. This ongoing education can contribute to a dynamic and responsive healthcare system.
Moreover a concern raised by participants regarding the unacceptable waitlist for counselor support underscores a pressing social justice issue that demands attention. To address this challenge, we propose the following community resources and policy developments:
1. Community Resources:
Expand Counseling Services: Allocate resources to expand counseling services within the community, including hiring additional counselors to reduce the backlog and meet the demand for support effectively.
Community Partnerships: Establish partnerships with local mental health organizations, NGOs, and community-based groups to supplement counseling services. Collaboration can enhance the availability of resources and provide timely support to those in need.
Peer Support Programs: Introduce and promote peer support programs within the community, empowering survivors to support each other during the waiting period. These programs can offer a valuable complement to formal counseling services.
2. Policy Development:
Reduced Wait Time Targets: Implement policies that set clear and realistic targets for reducing wait times for counseling services. Regularly assess and adjust these targets to ensure continuous improvement and responsiveness to community needs.
Funding Allocation: Advocate for increased funding allocation to mental health services, specifically targeting resources to address the demand for counseling support. Adequate funding is crucial for the recruitment and retention of qualified counselors.
Streamlined Referral Processes: Develop and implement policies that streamline the referral processes between healthcare providers and counseling services. This can facilitate quicker access to support for survivors during their perinatal care.
By combining community-level resources and strategic policy developments, we aim to not only address the immediate issue of an unacceptable waitlist but also contribute to a more equitable and accessible system of support for individuals experiencing gender-based violence..
These recommendations represent a critical step towards fostering a healthcare environment that empowers survivors and facilitates disclosure, ultimately contributing to improve maternal and child health outcomes.
Footnotes
Acknowledgment
The researchers would like to express their gratitude to all women and health care providers who participated in this research and provided us with their valuable experiences. Also, we appreciate Shahin Dokht Shahin and Shahriar Jahanbani, who helped us as volunteers in this study. We appreciate the Women’s Health Research Institute, Perinatal Services BC, and UBC for their support in the process of doing this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.