
Abstract
Background
Migraine is a neurobiological condition characterized by a constellation of unpredictable symptoms and is the second cause of disability worldwide. Migraine is prevalent among nurses. However, literature exploring nurses’ experience of living with migraine is scarce which has important individual and systems implications for health and wellness and patient safety. Self-management is essential in chronic disease management as the patient engages in various strategies to be able to live with their condition.
Purpose
This study explored the experiences of living and working with migraine among female nurses in Ontario, with particular attention to their priorities and strategies for self-management.
Methods
Interpretive description methodology was employed to guide this study and informed a thematic analysis approach to examine the self-management experiences of nurses living with migraine.
Results
Nurses engaged in various self-management strategies including pharmacological and non-pharmacological strategies and highlighted the role of technology in migraine self-management. Participants described experiences of living with migraine as an invisible condition including feelings of not being understood, stigmatization, and the absence of formal support at the workplace.
Conclusion
The implications of these findings support the incorporation of a critical approach to relational engagement that is person-centred including nonjudgemental, strength-based care as a practice approach when caring for persons living with migraines and the need to include experiential learning in educational curriculums as a strategy to reduce stigma against migraines.
Background and purpose
Migraine is a prevalent neurobiological and potentially incapacitating disorder and is a leading cause of disability worldwide, with a global prevalence of 12% and is more common in females than males (Steiner et al., 2018). Migraine is also a prevalent illness reported by nurses (Shields & Wilkins, 2006; Smyth et al., 2016; Wang et al., 2015). Migraine can be classified based on the severity and frequency of headaches into episodic and chronic migraine. Episodic migraine is defined as episodes that occur less than 15 days per month for three months. Chronic migraine, a severe form of migraine, is defined as headaches that occur for at least 15 days per month, with migraine features on at least eight days per month for at least three months (Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition,” 2018). In two national surveys conducted on the work and health of nurses in Canada and Australia, migraine ranked as the third most common chronic condition among female nurses and nurses and midwives respectively (Shields & Wilkins, 2006; Smyth et al., 2016).
Migraine attacks are characterized by episodic pulsating unilateral headaches of moderate to severe intensity, with acute episodes lasting for a few hours up to two to three days that are often associated with nausea or vomiting, photophobia or phonophobia (Dayapogu & Yildiz, 2017; Landy et al., 2011; WHO, 2011). There are two significant subtypes of migraine; migraine without aura and migraine with aura which includes migraine symptoms that are preceded by completely reversible visual, sensory, speech, language, or motor symptoms (International Headache Society (IHS), 2018).
Migraine is responsible for 5.6% of all years lived with disability (YLDs) and ranks as the second most disabling condition in the Global burden of disease study in 2016 (Schroeder et al., 2018; Steiner et al., 2018; Steiner et al., 2020). Persons living with migraine have reported decreased efficiency at work, during their studies, and performing family roles such as caring for their children (Ruiz de Velasco et al., 2003; Rutberg & Öhrling, 2012). In addition, stigma and stereotyping are issues that have been raised by migraine patients and remain a significant determinant of health for persons with migraine (Aydemir et al., 2011; Parikh & Young, 2019; Young et al., 2013). Stigma against migraine began around the 18th to nineteenth century and was rooted in the absence of objective manifestation of pain or headaches and lack of tangible anatomical and pathological features (Parikh & Young, 2019). Recently, Raffaelli et al. (2021) used photos of people with migraine to explore migraine patients and healthcare workers’ perception of these images. Both groups rated photos with male and older models as more realistic than photos with females and younger models. The authors, argued from a feminist perspective, that pain expressions of females are often taken less seriously and the reality of pain among women is often questioned. The stereotypic representation of migraine has persisted to current times (Raffaelli et al., 2021).
Dayapogu and Yildiz (2017) highlighted that 70% of migraine patients experience moderate to severe pain that affects their ability to perform activities of daily living. According to the WHO (2011) about 50% of persons living with migraine self-manage their symptoms. In the United States, only about 40% of individuals with chronic migraine sought consultation and about 10% of this sample received a diagnosis, while only half of those who were diagnosed received evidence-based treatment (Schroeder et al., 2018). These data indicate a gap in the medical management of migraines and underscores the importance of self-management as an approach to caring for individuals with migraine.
Enabling patient self-management is a core element in the chronic disease care model and self-management support has been linked to improved disease outcomes (Grady and Gough, 2014). Effective self-management encompasses the ability to monitor one's condition and the cognitive, behavioural, and emotional responses necessary to maintain a good life and includes recognizing and responding to symptoms, managing acute episodes, managing relations, obtaining support from significant others, and using medications or other activities towards living with a chronic illness (Lorig & Holman, 2003; Munir et al., 2005). Nurses play a critical role in maintaining the wellbeing of others through engaging in the treatment, and promoting the health of, individuals, families, and communities (College of Nurses of Ontario, 2022). Moreover, the health and wellbeing of nurses and their ability to meet their expectations within the workplace has important implications for patient care and safety (Forstag and Cuff, 2020). As such, nurses with migraine are likely to engage in self-management to continue with their daily activities and fulfill their workplace obligations.
Unfortunately, research and medical care for migraine patients have been overlooked in the women's health agenda; arguably because migraine symptoms are episodic, not contagious, and migraine is not listed as one of the significant causes of adult mortality (Rutberg & Öhrling, 2012; WHO, 2011). For example, research on migraine receives minimal funding from the National Institute of Health (NIH) a major US research organisation (Schroeder et al., 2018). Also, literature exploring the experiences of migraine among nurses is limited to indicators of prevalence, leaving a gap in potential health and wellness approaches for nurses (Shields and Wilkins, 2006; Smyth et al., 2016; Wang et al., 2015; Xie et al., 2020). Scholarly attention is needed to explore nurses’ migraine experiences inclusive of the multiple contextual factors that may influence migraine self-management. Thus, the purpose of this research was to explore the experiences of living with migraines among female nurses in Ontario with attention to their strategies and priorities for self-management.
Methods and procedure
Design
Interpretive description methodology was used to guide this study. The goal of interpretive description research is not to generate theory but rather to inductively explore a phenomenon of interest to gain new ways of understanding that can inform health care practice(s) and/or advance understanding (Thorne, 2016). Understanding migraine management remains a challenge as migraine experiences are unique and require a person-centred approach to care (Andreou and Edvinsson, 2019). In this research, interpretive description provided an orientation towards inquiry that sought to better understand the complex nature of nurses’ migraine self-management experiences (Teodoro et al., 2018). Interpretive description affirms the importance of understanding the time and context within which human expressions and behaviours are enacted in the analysis process (Thorne, 2016). In this study, temporality helped to analyse how the length of time living with migraine has shaped nurses’ self-management experiences while context incorporated the various social, political, and ecological factors and how these elements relate and are expressed within participants’ experiences.
Interpretive description acknowledges the researcher - participant interaction as a process of co-constructing the meaning of the phenomenon (Thorne, 2016). Therefore, engaging in active self-reflection was an essential part of this research process. Reflective journaling was used to track initial observations, decision points and for testing various conceptualisations from the data (Thorne, 2016). Ethical approval for this study was obtained from the university Research Ethics Board (project ID 116511).
Sampling and recruitment
Purposive and theoretical sampling techniques were used to recruit study participants. Purposive sampling allowed for the selection of participants with the potential of answering the research question of this study (Thorne, 2016). The inclusion of theoretical sampling (Thorne, 2016; Sandelowski, 2000) informed further recruitment of participants with additional attributes such as participants multiple symptoms of migraine and living with migraine for a longer period which further informed data collection. Study advertisements were shared on social media platforms such as Facebook, Instagram, Twitter and Kijiji. Potential participants contacted the researcher via email or telephone number listed on the study advert. Nurses were included in this study if they met the following criteria: 1) employed full time, part-time or casual in a clinical environment, 2) identified as women, 3) were fluent in spoken English and 4) had either had a medical diagnosis or self- report migraine or migraine-like symptoms.
Data collection
Data were collected through semi-structured interviews via a video call at a scheduled date and time of mutual agreement between each participant and the researcher. Virtual interviews were conducted to respect the health of participants/researcher and to align with the Public Health Agency of Canada's (PHAC) mandate of maintaining physical distancing at the time the data was collected. Demographic and occupational characteristics such as type of workplace, number of hours of work, and questions in relation to migraine symptoms such as type of symptoms, frequency and severity of symptoms were collected using an online questionnaire. A semi structured interview guide was used to conduct the interviews which lasted between 45 to 60 min. A conversational approach was employed using the following open-ended questions that guided the interview with participants: Please, describe your experience of living with migraine? How does migraine influence your daily activities? What does having migraine mean to you? How do you manage your migraine? Tell me how you manage your migraines in different settings. Tell me about the conversations you have with others about your migraine. Have you ever had any experience with discrimination at work? Can you talk about any technology platforms you have used specifically for your migraines? A $5 coffee or tea e-gift card was offered to participants at the end of each interview as a gesture of gratitude, acknowledging their time.
Data analysis
Consistent with the interpretive description methodology, a thematic analysis of the interview data, as described by Braun and Clarke (2006), was conducted. This analysis process extends analytical insight beyond the semantic content of data to identify underlying assumptions and conceptualizations within data (Braun & Clarke, 2006; Thorne et al., 2004; Thorne, 2016). NVivo (QSR International Pty Ltd., 2020) a qualitative software program was used for data organization. The thematic analysis process consisted of a set of non-linear six steps which included familiarising oneself with the data, generating initial codes, searching for themes, reviewing themes, defining themes and reporting findings (Braun & Clarke, 2006). Informed by the approach employed by Thorne (2016), the first author (MND) transcribed each interview verbatim which helped facilitate the initial appreciation of underlying concepts from each interview. All names of individuals were changed to pseudonyms and quotes were edited for readability. Each transcript was read multiple times and attention was directed to strategically identifying patterns, test, explore, and expand on conceptualizations observed in relation to contextual and social factors reflected in the self-management experiences of nurses (Sandelowski, 2000; Thorne et al., 2004; Thorne, 2016).
The criteria used to facilitate trustworthiness of this study included credibility, dependability, confirmability, and transferability (Nowell et al., 2017; Sandelowski, 1993; Thorne, 2016). Using an iterative approach to analysis (Sandelowski, 1993), all authors with diverse backgrounds collaborated through data analysis discussing and exploring commonalities and variances within participants’ experiences thereby creating a memo audit of the analysis process.
Findings
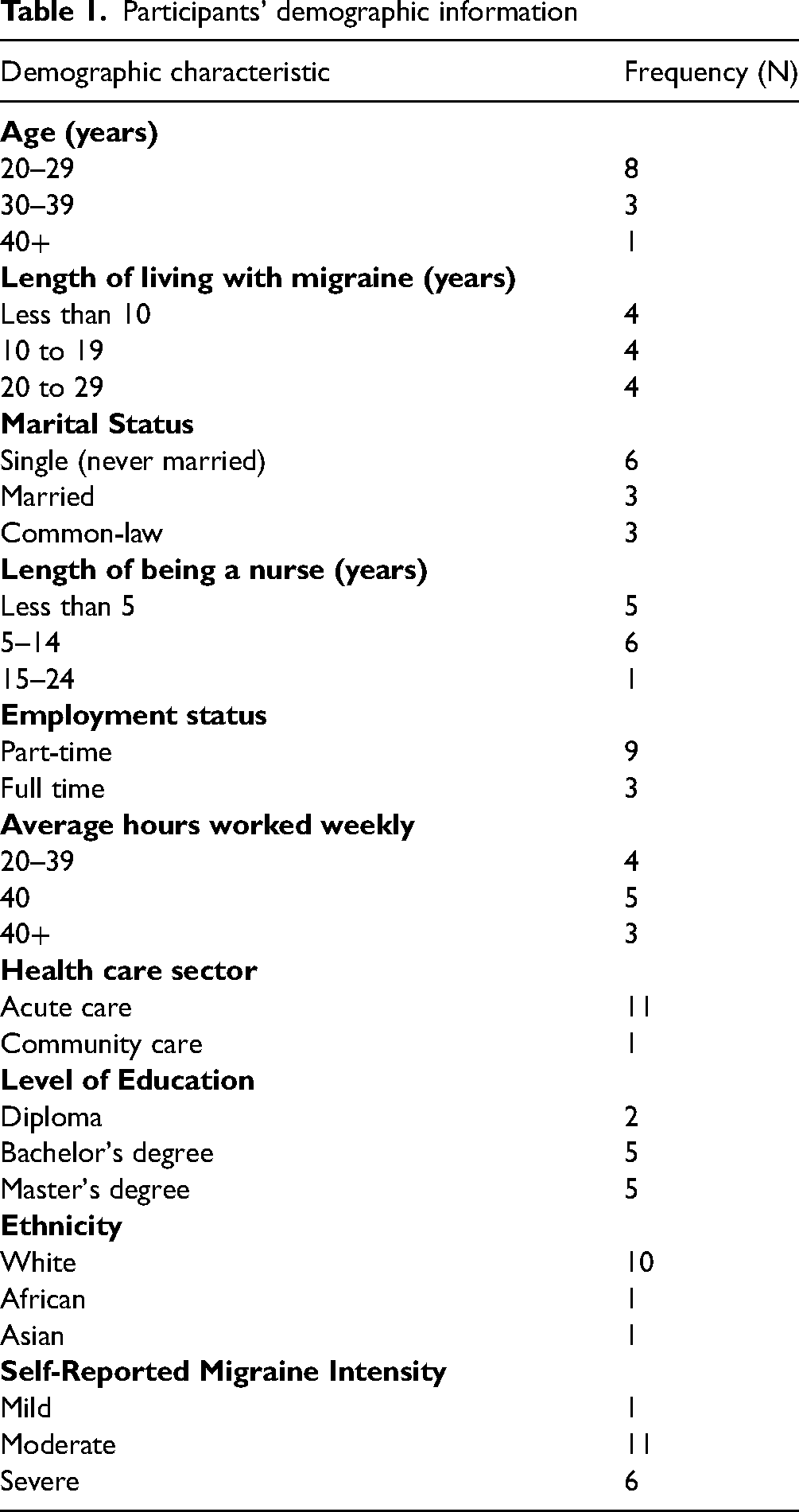
Twelve semi-structured interviews were conducted with nurses from Ontario who met the inclusion criteria for this study. Participants were recruited from clinical practice areas of community and acute care. Participants included both registered nurses (RN) and registered practical nurses (RPN). Most participants were single females, aged between 20 years and 29 years and identified as white. Majority of the participants rated their migraine headaches to be moderate to severe and had lived with migraine for at least ten years. (See Table 1).
Participants’ demographic information
Physical manifestation of migraines
All but one participant had received a medical diagnosis for their migraine. Participants described their headaches as throbbing or pulsating, located on one side of the head ranging from moderate to severe intensity. Symptoms accompanying migraine headaches included photosensitivity, visual disturbances, phonophobia, nausea or vomiting, sensations of pins and needles or numbness, muscle weakness. Other symptoms included generalized fatigue, alterations in thought process such as slowness in expressing themselves, loss of appetite and difficulty sleeping.
Furthermore, participants shared their experiences in relation to living and working while experiencing migraines and how they engaged in self-management. The following three themes and associated subthemes were constructed from participant's reported experiences: 1) Self-management strategies with four subthemes: pharmacological strategies, non-pharmacological strategies, learning as you go and technology as a tool for self-management; 2) Living with an invisible condition with two subthemes: feelings of not being understood and “It [Migraine] is very debilitating”; and 3) Negotiating the workplace with three sub-themes: stigma, developing resilience through suffering and lack of formal workplace supports.
Theme 1: self-management strategies
Participants described various self-management strategies that they employed to manage their migraines. Overall, participants described engaging in multiple strategies to help provide symptom relief and to prevent worsening of symptoms. These strategies are reflected in the following four subthemes: Pharmacological strategies, non-pharmacological strategies, learning as you go, and technology as a tool for self-management
Subtheme 1: pharmacological strategies
The use of either prescription or over-the-counter medications to manage migraines was described by all participants. Ethel
1
explained If I start taking Tylenol (acetaminophen) and Advil (ibuprofen) like right away when I first start having a headache, I can catch it [headache] and it [headache] will go away in a couple of hours. But if I am busy doing things or I don’t have access to the [medications], it can last up to two days.
Subtheme 2: non-pharmacological strategies
Participants described using non-pharmacological strategies to either prevent migraine symptoms, provide symptom relief or maintain their overall wellbeing. Ella explained: so, when I have a migraine, sometimes I just like to lay on the couch and turn out the lights because I find I don’t like being in bright spaces, or looking at phones or computers aggravates it [migraines]… Sometimes, I would put a cold cloth on my head, and put some peppermint oil, its cooling effect helps.
Participants also described managing acute migraine episodes by seeking social isolation as they manage their symptoms as Kathy explained: I think like the worst part about them for me is like having to like to seclude myself. You know, because I just like, can't function with anything around me you know, so I'm going to lock myself away and even like shut off my communication.
Subtheme 3: learning as you go
Improved understanding of self, migraine symptoms, and management techniques was revealed through the participants’ years of living with migraines. Participants described their ability to better identify and prevent migraine triggers and engage in activities that promote general health such as staying hydrated, and sleep hygiene that also helps prevent migraines. Establishing and building supportive relationships was at the centre of their learning experience. Ethel described her experience with her family physician below: Having a family doctor that understands how debilitating the migraines and the headaches kind of changed the management. Because she was the one who was like let's try prescriptions. Let's try physio, let's try massage and …the fact that she's willing to try different regimens and it did help. One of my old employers, she was a migraine sufferer, so when I started experiencing the auras, I did reach out to her and asked her what her experience was when she has migraines and what helped her, and she is the one who told me about peppermint rollers…
Subtheme 4: technology as a tool for self-management
Most participants described searching online for information about migraine. A participant Katie, explained: […] I didn’t know there was a migraine with an aura. No one has ever spoken to me that could happen. So I searched on google “zig pattern”, “left peripheral vision” and the result was migraines with auras explaining the symptoms[…]I would search for images of migraines with auras and what the visual field would look like and there were many that came up that was exactly what I experienced[… ] I would read all of it and then just make an informed decision about what I was experiencing […]I was just looking for that reassurance for myself more than anything else[…]
Theme 2: living with an invisible condition
Participants described their experience as difficult to share with others or difficult to be understood by others because their condition was not always visible to others. These experiences are reflected in two themes: a) Feelings of not being understood b) It [Migraine] is very debilitating
Subtheme 1: feelings of not being understood
Participants were hesitant to share their migraine experience with others. Participants perceived others to have a limited comprehension of the depth of their experience and suffering. Sonia explained: I find it's usually men who don’t get migraines are the ones that believe you the least and not very empathetic towards your experience. However, I find older women who have suffered migraines their whole life are usually the ones that are very empathetic of your experience which makes you feel validated because you can’t ever prove to someone that I have a really bad headache right?
Subtheme 2: “it [migraine] is very debilitating”
A common theme described feelings of frustration towards the unpredictability of living with migraines. This is reflected in Eunice's experience: So, to me what it (migraines) means is…that it's very debilitating. I know that I've cancelled so many plans in the past that sometimes I feel bad […] I honestly hate having migraines because there's a lot of things that I kind of feel I missed out on…I have to think ahead like am I going to get a migraine? I always have to pack extra things to manage my migraine if it were to come on. So, it's like I'm planning my life around having migraines as well. [A] couple [of] times recently within the last two months I've like thought about shaving my hair off because that even feels painful and I'm like I just don't wanna live in pain like this. So that I think would be the most distressing thing to me[…]
Sheila's experience was reflected in all other participants as they described pain or migraine headaches as the most significant and challenging symptom that impedes their ability to carry on their activities. Participants expressed navigating past migraine headaches as a priority outcome to their self-management strategies. The quality of pain was not only in its characteristic discomfort associated with the experience but also its unpredictability.
Theme 3: negotiating the workplace
Participants described having to work while having an acute migraine episode. During this experience participants described how they go through a mental self-assessment process which includes assessing the severity of their symptoms, the availability of resources or supports at the time, and their ability to manage these symptoms and go on with work. Participants’ experiences are reflected in three subthemes: stigma, developing resilience through suffering, and lack of formal workplace supports.
Subtheme 1: stigma
Some participants described receiving negative stereotypic responses from others regarding their migraine experience. As Ella explained: So, I remember leaving work one time early. I remember coworkers saying, “well if you have vision problems you shouldn't be driving” […] I remember that co-worker said, “as long as you're not just using that as an excuse to leave early”, and she said, “I remember one nurse who said they were having a migraine and said they couldn't see, then they drove home” overall, speculating whether they were even having a migraine or not. … people just think well, she's just making it up or something, right? […] I think it would be a problem if I called in sick as often as I need to. So, I work with severe migraines more often because I've seen it happen to other people. I've heard a conversation of, you know, this person oh they have migraines again. I think I function so much with mine being as bad as they are sometimes because I don't want to be the topic of conversation, I don't want to have the attendance management letters sent to me. It's a lived experience that I've seen other people go through.
Subtheme 2: developing resilience through suffering
While at work participants managed their migraines by living through the experience while finding strategies to improve their symptoms so they could continue to work. As Sonia explained: At work, it's a lot of different variables depending on the severity of the headache, the staffing, the ability of how acute my patients are, depending on how able I am to go leave my patients for 20 min but sometimes you can't always do that. I'll go sit in the break room and just close my eyes.
However, the goal of these strategies was not to completely relieve symptoms but to make symptoms tolerable so that the nurses could continue working. Participants found that at work it was not always possible to fully avoid their migraine triggers, or they did not always have the opportunity to engage in multiple strategies to prevent or improve their migraine symptoms. Participants described what considerations they made to return home or continue to work during a migraine episode. Thora explained: I did have to go home sick I remember, and it was because my vision started to change. So, I started to see black spots and was really foggy, I couldn't focus on anything and obviously you have to be able to think critically, so that made me quite nervous. So, that was part of the reason that I did go home. Because I had a pretty sick patient, and I didn't want anything to happen to them.
Subtheme 3: lack of formal workplace supports
Participants described supports at work to come from coworkers or colleagues and identified limited formal supports in place to assist them specifically with their migraine. As Rowe explained: And I don't feel like I have any support at work for sure. It's just I don't have any other choice and so I just keep doing my job like my co-worker will need help with a boost or I need to give that next medication, or I need to go talk to the family. Like it's Tylenol, Advil, drink some water and just keep going and that's it.
Discussion
This study explored the experiences of Ontario-based nurses living with migraines with attention to their self-management experiences. Participants shared common experiences reflected in three overarching themes including, self-management strategies, living with an invisible condition, and negotiating the workplace. These themes illuminated the need for a more relational and person-centred approach to the treatment and support for nurses living with migraines.
Symptom management
Nurses in this study primarily relied on their own ability, skills, and knowledge to self-manage their migraines to cope with the debilitating nature of the condition. This concept of self-reliance reinforces the importance of self-management as an essential concept in chronic pain and chronic disease management and highlights the challenges of under-treatment of migraines. Similar to what has been described elsewhere (Heidari et al., 2022; Schroeder et al., 2018; Steiner et al., 2020), all nurses in this study described the importance of self-reliance and the ‘trial and error’ process they used to determine the most effective composition of self-management strategies including both pharmacological and non-pharmacological strategies. What remains a challenge for people with migraines is the persistent focus on management and treatments reflecting a mainly biomedical understanding of migraine (Lui et al., 2020).
Pain relief was the most significant outcome described by nurses, which possibly contributed to their use of multiple self-management strategies during acute episodes to provide pain relief. Consistent with the findings of Peters et al. (2004) nurses in this study would decide on management options and engage in self-management behaviour to achieve relief from pain. They described improvement of their acute symptoms with over-the-counter medications, but not complete relief. Similar findings were described by Chang et al. (2021) who reported that most participants relied on multiple self-management strategies, including alternative therapies for migraine relief. The use of multiple self-management strategies to relieve migraine symptoms may indicate synergistic effects between pharmacological and non-pharmacological strategies in migraine management.
Information seeking
The experiences of nurses also highlighted the role of digital health literacy in the self-management of migraine. Nurses in this study described using the internet and Google to search for information about their migraines or to inform their self-management strategies. According to Lorig and Holman (2003), individuals require knowledge to be able to make decisions in response to the changes in their disease condition. Self-management interventions for chronic conditions incorporating educational resources for persons living with migraines have shown increased engagement and successful self-management outcomes (Patel et al., 2019; Probyn et al., 2017). Although nurses in this study accessed the internet for information, few nurses described using technology such as online apps to track their migraines or seek social support or collaborate with their health care provider. However, the use of digital technology such as mobile applications or web pages to track headache patterns, and migraine triggers to facilitate migraine diagnosis has been described in the literature as helpful (Mosadeghi-Nik et al., 2016; Pearson et al., 2019). Although, there is evidence that screen time exposure with digital device use can be a contributing trigger to individuals with migraine thereby prohibiting online access to information and / or support networks (Montagni et al., 2016). Further research is needed to understand the impact of digital health apps and social networks among nurses experiencing migraine or chronic pain.
Similar to the findings of this study, Befus et al. (2019) and Matthews and Kneipp (2020) reported that women experiencing migraines relied on their physician, trusted family member or close friend from whom they learned their self-management strategies. These findings specifically highlight the importance of the development of trust in professional healthcare provider-patient relationships fostering self-management abilities for those living with migraines. Also, previous studies on persons living with migraines have identified the presence of social support as an important strategy in the successful management of migraine symptoms and improved quality of life (Lui et al., 2020).
Negotiating the workplace
The workplace as a context that shapes migraine experience was consistent among all participants. Participants described how they negotiated the workplace to continue to function through migraine episodes. From our findings the potential factors that may have influenced participants’ decision whether to stay at work during migraine symptoms included personal factors (i.e., perceived severity of migraine, perceived ability to manage symptoms and feelings of guilt or perceived stigma), and workplace factors (i.e., available supports, workload, and concerns about the ability to provide safe care). Our findings echo the results from Onwuekwe et al., (2014) who reported minimal disability, work absenteeism and loss of productivity time despite the high prevalence of migraine among healthcare workers in Nigeria. Similarly, Landy et al. (2011) reported low absenteeism related to migraine among persons living with migraine who work in healthcare settings in the United States.
The concept of presenteeism where individuals continue to work despite being sick and/or a primary caregiver (e.g., caregiver of older adult) and distracted from the duties of their occupational role has been given lesser attention than absenteeism (Malmberg-Ceder et al., 2020). Presenteeism is associated with decreased health status and lower workplace productivity (Malmberg-Ceder et al., 2020; Shimizu et al., 2021). Similar to nurses’ experiences in this study, barriers for persons continuing to work when sick has been associated to workload and difficulty finding replacement staff (Martinez & Ferreira, 2012). This current study contributes to the existing literature on the prevalence of presenteeism among persons living with migraine and the need to provide organizational work support for persons living with migraines.
The experience of stigma was mostly described within the context of the workplace. In this study, we found that disclosure of migraine symptoms was influenced by the context. At work most participants described only disclosing their migraines to immediate colleagues to receive supports from them. Participants experienced negative connotations and reactions from their colleagues questioning the authenticity of their symptoms. These findings add to the literature on stigma toward migraine patients (Parikh et al., 2021; Shapiro et al.; 2014; Young et al., 2013). Studies also have described stigmatising attitudes toward persons living with migraines by healthcare professionals (Belam et al., 2005; Palacios-Ceña et al., 2017; Varkey et al., 2013). Participants described internalizing stigma and as a result, did not disclose their migraines at the workplace or continued to work despite having an acute migraine episode. Research suggests that internalized stigma negatively correlates with the ability to work and increases with absenteeism (Shapiro et al., 2014; Young et al., 2013). As such, a migraine patient with higher functional ability might feel less stigmatized than someone with lesser functional ability (Young et al., 2013).
Most nurses in this study did not feel the need to disclose their migraine symptoms to their supervisors or to organizational human resources as they felt they were able to manage their migraine without influence on their work. At the same time, nurses also reported a lack of awareness of organizational supports regarding their migraine condition. It is possible among participants that there is a bidirectional relationship between disclosure of their symptoms and their perceived lack of organizational support. Access to work compensation for time lost due to the debilitating nature of migraines continues to be a challenge for many persons living with migraines (Schroeder et al., 2018; Steiner et al., 2018). These findings highlight the ripple effect of the absence of migraines in global policy debates, i.e., migraine is not recognised as a debilitating condition and thus it is not included in some social compensation policies (Schroeder et al., 2018). Although participants highlighted there are other supports at the workplace such as wellness programs that promote overall health, they were not aware of any resources directly for migraines. However, most participants described not disclosing their migraines to their managers or organizational human resources. As such more research exploring healthcare work environments and organisational supports for persons living with migraines can reveal greater insights into some structural implications for migraine management.
Living with an invisible condition
Nurses in this study found that the nature of their migraine condition was often not understood by others. Similarly, Younas (2020) described the concept of individual suffering as a personalized negative experience that can threaten a person's physical, emotional, and psychological well-being. As well, the strategies of self-managing migraines such as withdrawing from social activities may also enhance individuals’ social isolation or feelings of ‘aloneness’ (Kneipp & Beeber, 2015).
Nurses also described feelings of frustration surrounding the unpredictability of migraines and having to plan their lives around their migraines. Nichols et al. (2017) reported similar findings in their systematic review where participants described headaches as a driver of their behaviour including medication overuse or avoidance to plan events. Additionally, nurses in this study described their experiences of living with migraines using words such as scary, frustration, and debilitating, reflecting the emotional suffering associated with having migraines. Reinforcing the need for a biopsychosocial approach to migraine management that includes a relational practise approach to healthcare delivery for persons living with migraines. Relational practice creates a milieu that facilitates communication, compassionate care, and person-centred exploration of the patient's needs (Younas, 2020). A relational approach requires healthcare providers to gain a deeper understanding of patients’ experiences beyond assessment of their physical suffering to understanding their emotional and psychological suffering (Younas). In addition, relational inquiry requires the healthcare provider to critically examine intrapersonal factors (i.e., factors within the patient and within the healthcare provider such as their beliefs or personal experiences), interpersonal factors (i.e., between and among the healthcare provider, the patient, and their environment), situational contexts and knowledge to inform their care models (Doane and Varcoe, 2021).
Limitations
A limitation of this study is the nature of the sample of this study. The participants in this study included female nurses from urban areas, who are English speaking, and majority worked in an acute care setting. As such the influences of various situational contextual factors such as geographic locations (i.e., urban areas or rural areas) or type of workplace environment (i.e., exploring acute care, community care, long-term care, and virtual care settings) on the experiences of living and working with migraines could not be explored this study. More research exploring the experiences of nurses living with migraines across a diverse demographic is needed.
Conclusion
This study has highlighted information technology as tool for self-management of migraine and suggested ways in which technology can be employed. Nurses’ experience of self-management strategies and stigma are consistent with findings in the existing literature. Nurses’ experience of living with this invisible condition also contributes to the literature; emphasizing participants’ experiences of not being understood. This study also has provided more context to previous quantitative reports on the importance of workplace as a context when exploring migraine management approaches. The implications from this study have the potential to inform new approaches to caring for persons living with migraines and have potential to influence new areas of research in this domain.
Footnotes
Acknowledgements
We thank and value the insight of the nurses who participated in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.