
Abstract
Background
The rising rates of anti-Asian sentiments has recently been called into question by several community activists and scholars. While this collective work has heightened awareness to address anti-Asian racism, the experiences of Asian healthcare workers in particular remains limited.
Purpose
To map the existing literature on anti-Asian racism experienced by Asian healthcare workers in North American healthcare settings, identify gaps in the current literature base, and inform future areas of anti-Asian racism research.
Methods
A scoping review following Arksey and O'Malley’s (2005) methodology with updated guidance by Levac et al. (2010) and Peters et al. (2020) was undertaken.
Findings
A total of 3565 articles from database searches were identified from eight databases, with 64 full text articles screened and 15 articles included in this review. Anti-Asian racism amongst healthcare workers has been conceptualized, studied, and understood in three broad categories: levels of racism, descriptions of anti-Asian racism, and the impact of racism. In 60% of the included articles, interpersonal level of racism was solely studied, while 40% articles simultaneously studied interpersonal and institutional levels of racism. Anti-Asian racism was described through three key perspectives: otherness, inferior professional status, and general racial discrimination. Lastly, the impact of Asian healthcare workers’ experiences of anti-Asian racism was studied by exploring the impact on mental health and barriers to career advancement.
Conclusion
Despite the presence of anti-Asian racism, the limited literature examining the complexities of the experiences of anti-Asian racism for Asian healthcare workers is concerning. Future scholarship requires further investigation that comprehensively explores the multiple pathways of anti-Asian racism, the contestation of monolithic stereotypes, and how Asian healthcare workers negotiate both hypervisibility and invisibility within healthcare spaces.
Recognized as a determinant of health, racism is significantly related to both poorer mental and physical health due to a variety of factors such as economic and social deprivation, inadequate or degraded medical care, and socially-inflicted trauma (Canadian Public Health Association, 2015; Paradies et al., 2015). Crises reinforce deeply rooted sociopolitical and cultural fractures in society. Shedding light on the COVID-19 pandemic illuminates how existing structures of racism produce inequitable access to healthcare and social services and disproportionately impact the health and wellbeing of racialized communities. Within the North American context, the racialization of COVID-19 continue to unduly affect Asian diasporas; an experience reminiscent of the social marginalization, stigmatization, and discrimination experienced by Asian communities during the 2003 SARS outbreak (Person et al., 2004). Over the course of the pandemic, news outlets, elected officials, and citizens have used polarizing tactics to blame China and Chinese people for COVID-19 (Chae et al., 2021; Cheah et al., 2020). Racializing COVID-19 as the “China virus”, has manufactured insurmountable conditions not only for Chinese diasporas, but for Asian communities across North America (Chae et al., 2021; Cheah et al., 2020; Hswen et al., 2021). Particularly, rising rates of anti-Asian sentiments have escalated racial violence on Asian diasporas. Anti-Asian hate incidences and hate crimes have been reported at exponential rates across Canada and the United States of America since the racialization of COVID-19 (Chae et al., 2021), including verbal harassment, avoidance and shunning, coughed at or spat on, physical assault, and workplace discrimination (Chinese Canadian National Council Toronto Chapter, 2022; Stop AAPI Hate, 2022).
These overwhelming acts of racism in the wake of COVID-19, however, represents only the resurgence of state sanctioned anti-Asian racism within the underbelly of North America. Recent scholarship suggests that the COVID-19 pandemic amplified anti-Asian sentiments and exposed existing racial biases against Asian people (Chae et al., 2021; Hswen et al., 2021). This rise in anti-Asian racism has recently been called into question by several community activists, organizations, and scholars in response to COVID-19-related anti-Asian racism. Activists and non-profit organizations from coast to coast have actively addressed the rise in anti-Asian violence. For example, StopAsianHate (https://stopaapihate.org/) is collecting and reporting anti-Asian incidences across the United States, Elimin8Hate (https://www.elimin8hate.org) is working to eliminate anti-Asian racism through arts, film, and media, while Act2EndRacism (https://act2endracism.ca/) is creating campaigns and educational resources addressing COVID-19-related racism. Coupled with social media trends such as #StopAsianHate and #HateIsAVirus, unearthing the insidiousness of anti-Asian racism across North America is gradually emerging from the shadows.
While this collective work has heightened awareness and efforts to address anti-Asian racism, we, as two Asian Canadian registered nurses (SLP, PC), have observed that the experiences of Asian healthcare workers in particular, have received far less attention in comparison. Shang et al.'s (2021) recent study documented that Asian healthcare workers across North America are experiencing heightened COVID-19-related racial violence in the workplace. Therefore, it is of critical importance to protect the safety and wellbeing of Asian healthcare workers as they will continue to play a crucial role in delivering the health and social care services that the public society depends on.
While all health care professionals have a role to play in addressing anti-Asian racism, we suggest that significant opportunities exist within nursing given that nurses comprise of the largest portion of the healthcare workforce across North America and play a critical role in leading interprofessional teams to deliver quality healthcare services. In recent years, some nursing organizations across North America have publicly recognized the importance of actively embedding anti-racism into practice, education, research, and policy (American Nurses Association, 2022; Canadian Nurses Association, 2022). Some have also explicitly called out the need to address anti-Asian racism (American Academy of Nursing, 2021). As a result, this is an opportune time for nurses to lead much-needed change within health systems across North America to improve the experiences of Asian healthcare workers, which ultimately influence patient care, population health, and costs within the health system. Although the need to address racial violence experienced by Asian health workers is non-debatable, a thorough investigation into the nature and foci of the existing literature base is first warranted to inform potential areas of research and inquiry that may inform policy and practice. As a result, we conducted a scoping review for three purposes. First, to map the existing literature on anti-Asian racism experienced by Asian healthcare workers in North American healthcare settings. Second, to identify gaps in the current literature base. Third, to inform future areas of research. The overarching research question that guided our review was: What is the nature, extent, and range of literature focused on Asian healthcare workers’ experiences of racism in North America?
Methods
We conducted a scoping review following Arksey and O’Malley's (2005) methodology with updated guidance by Levac et al. (2010) and Peters et al. (2020). This review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) statement (Tricco et al., 2018) and registered in Open Science Framework on January 31, 2022. Due to the limited evidence with how to integrate community stakeholders (i.e., patients, policymakers) throughout the scoping review process, we did not conduct the optional sixth stage (consulting with relevant stakeholders) proposed by the original Arksey and O’Malley (2005) framework. We consulted with a health sciences librarian (JYK) throughout the review.
Data sources and search strategy
An experienced medical librarian (JYK) conducted a comprehensive search strategy and relevant records were retrieved by systematically searching electronic library databases including Ovid MEDLINE, Ovid EMBASE, Ovid HealthSTAR, APA PsycInfo, CINAHL Plus with Full Text, Sociological Abstracts, ProQuest Dissertations & Theses Global, and Scopus on February 7, 2022 (Supplemental file A). The search was peer reviewed by a second research librarian using the Peer Review of Electronic Search Strategies (PRESS) guideline. To capture all relevant literature pertaining to the lived experiences of racism by Asian healthcare workers, we carefully selected relevant keywords and controlled vocabulary from the combination of search terms in three main categories: 1) Asian people, 2) healthcare workers, and 3) racism. The Asian origin groups were adapted from the list by the Pew Research Center (Budiman & Ruiz, 2021) and the diverse range of health occupations was adapted from a ‘health professionals and students’ search filter (Campbell, 2018).
In order to capture data on the historical context of anti-Asian racism experienced by healthcare workers, we did not place delimitations on the year of publication. We restricted the search strategy to studies available in English due to the feasibility of this review, and restricted geographical locations to Canada and the United States of America due to our focus on the North American context. In addition to subscription databases, we reviewed the first 200 Google Scholar results to supplement the bibliographic databases. The research team supplemented the electronic database search by backwards and forwards citation mining all reference lists of included studies. We directly imported all studies retrieved from the search into Endnote, a reference citation management program. Following the removal of duplicate records in Endnote, we exported the remaining records into a Microsoft Excel (2019) spreadsheet in tabular format for data management.
Study selection
We included articles if they met the following inclusion criteria:
available in the English language, within the North American context (Canada or the United States of America), focused on Asian healthcare workers, addressed racism (i.e., internalized racism, interpersonal racism, institutional racism) within the healthcare setting, and primary research articles and grey literature sources.
Articles were excluded if they were a) focused on the academic setting, b) editorials and conference proceedings given the limited data of the experiences of Asian healthcare workers in these source types, or c) books and novels due to the lack of methodological guidance for synthesizing this data within a scoping review methodology.
We defined healthcare workers broadly to include regulated professionals across all health professions and unregulated care providers who work to provide care to individuals, families, communities, and populations (Canadian Nurses Association, 2017). The term Asian is used to reflect peoples with ancestry to Asian countries or who are ethnically Asian (Statistics Canada, 2017b) with diverse ethno-cultural backgrounds (Statistics Canada, 2017a). In this review, racism was defined as the system of oppression and discrimination that unjustly impacts some populations rooted in the historical, social, political, and cultural exclusionary ideology of racialization (Cobbinah & Lewis, 2018; Racine, 2021). Internalized racism reflects the process whereby individuals accept unjust treatment and discrimination inflicted on them (Jones, 2000). While interpersonal, or personally mediated, racism is the intentional or unintentional discriminatory attitudes and behaviors between individuals, and institutional racism is the manifestation of racist ideologies through power and material conditions across institutions such as government, education, and healthcare (Jones, 2000). The healthcare setting in this review included any space where Asian healthcare workers provide direct patient and/or client care (e.g., hospitals, clinics, community centers).
Before study selection, two reviewers (SLP, PC) screened a random sample of the same 50 records and discussed discrepancies to increase reviewer consistency and understanding (Arksey & O'Malley, 2005; Levac et al., 2010; Peters et al., 2020). Study selection followed a two-level screening process. First, two reviewers (SLP, PC) independently screened all retrieved titles and abstracts against the a-priori inclusion criteria. The reviewers then classified these articles as either “include”, “unclear”, or “exclude”. Any records classified as “include” or “unclear” by one or both reviewers were included for secondary screening. Second, the same independent reviewers (SLP, PC) screened all full-text articles against the a-priori inclusion criteria. Disagreements arising from primary or secondary screening were resolved through a discussion until full consensus was achieved. Records excluded during secondary screening were recorded to ensure review transparency and reproducibility (Figure 1).
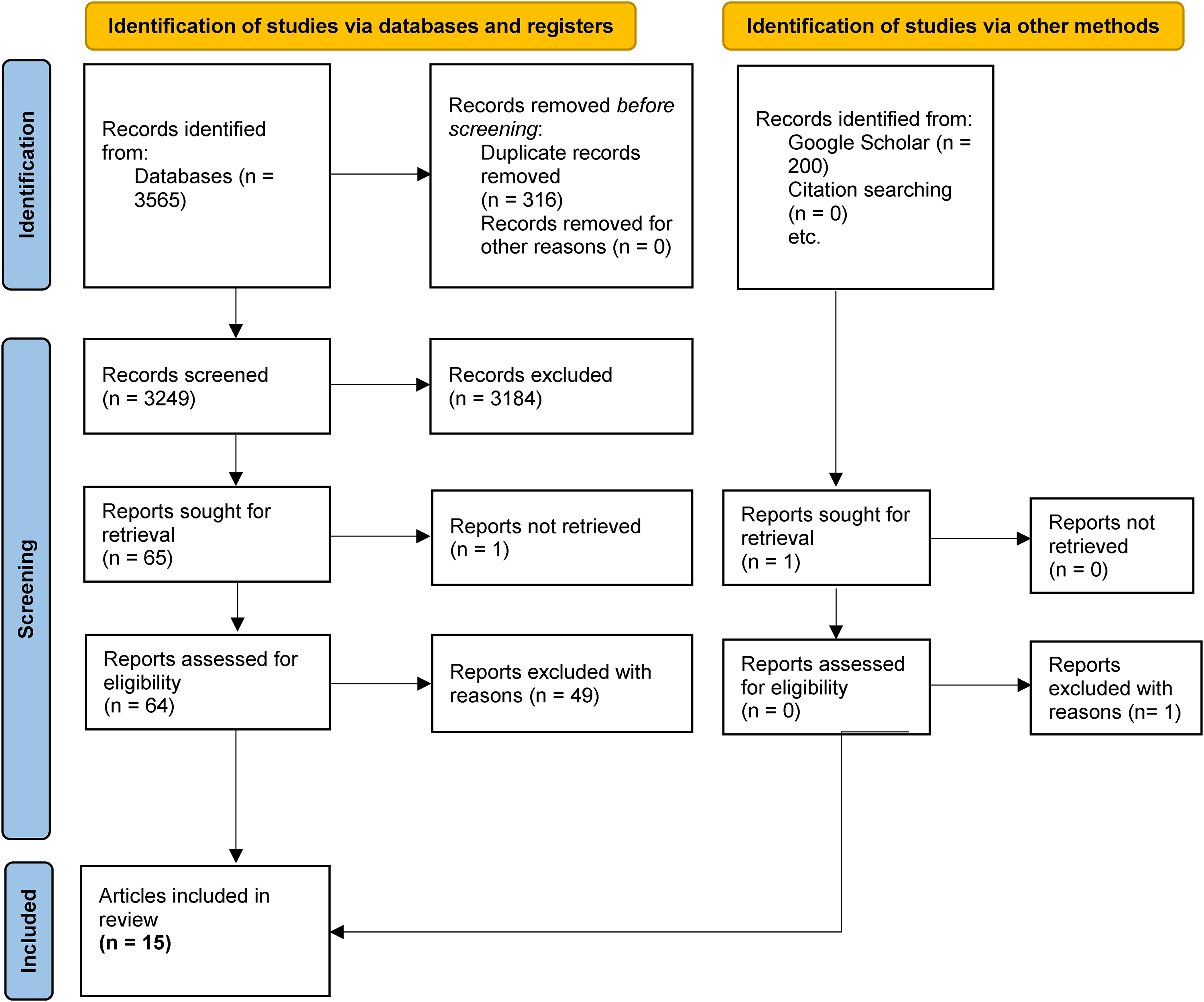
PRISMA Flow Diagram adapted from Page et al. (2021)
Data extraction, analysis and synthesis
We extracted data using a data extraction tool adapted from Arksey and O’Malley's (2005) recommended data charting items and piloted them independently using five records. The data extraction process was conducted independently by two reviewers (SLP, PC), and discrepancies were resolved through a discussion and consensus. Given that the primary objective of this scoping review was to map nature and extent of evidence and not to propose recommendations based on the effectiveness of findings (Arksey & O'Malley, 2005; Levac et al., 2010; Pollock et al., 2021), we aggregated findings regardless of research quality and did not perform critical appraisals of primary research studies. We used conventional content analysis to analyze data by classifying the coded data into broader categories representing similar meanings (Hsieh & Shannon, 2005). We also used descriptive statistics (frequency counts) to capture study characteristics.
Results
Study characteristics
We retrieved a total of 3565 articles from database searches in February 2022, with no additional articles identified through other sources. After removing 316 duplicates, 3249 unique articles remained for the initial title and abstract screening and 64 full text articles were screened (Figure 1). During our full text article screening, the majority of the articles were excluded based on two main reasons: a) not focusing on Asian healthcare workers, and b) focusing on other types of discrimination, such as disability, which did not include mentions of racism. We included a total of 15 articles in this review based on our a-priori inclusion criteria.
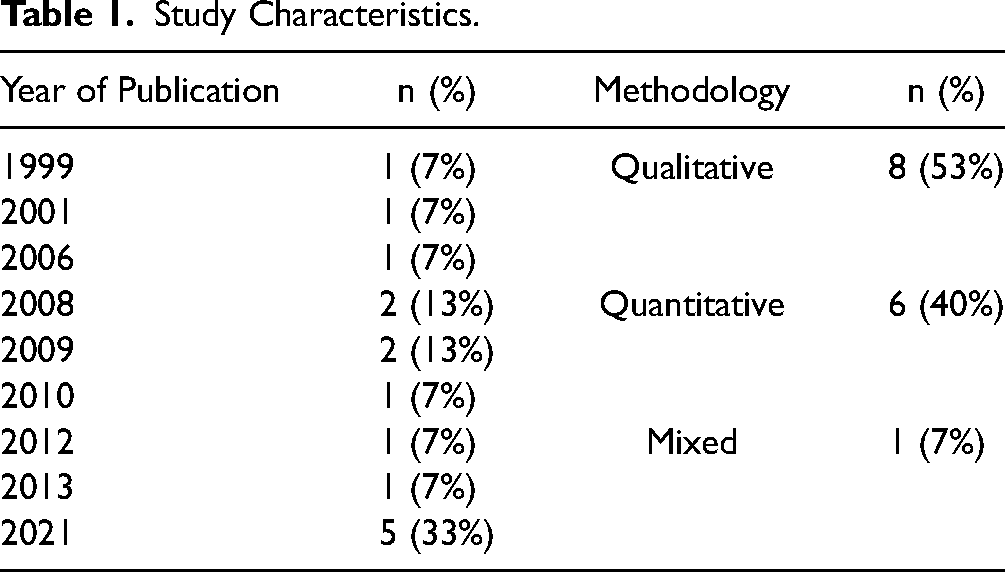
Of the included articles, the year of publication ranged from 1999 to 2021. Only one (7%) article was published prior to 2000 (Corbie-Smith et al., 1999), with seven (47%) articles published between 2001 to 2020 (Andal, 2006; George, 2001; Leung, 2008; Murti, 2010; Nunez-Smith et al., 2009a; Nunez-Smith et al., 2009b; Xu et al., 2008) and seven (47%) articles published between 2011 to 2021 (Bakken et al., 2021; Bhatt, 2013; Filut et al., 2021; Fujiwara, 2012; Hennein et al., 2021, 2022; Shang et al., 2021). See Table 1 for year of publication breakdown and study methodology.
Study Characteristics.
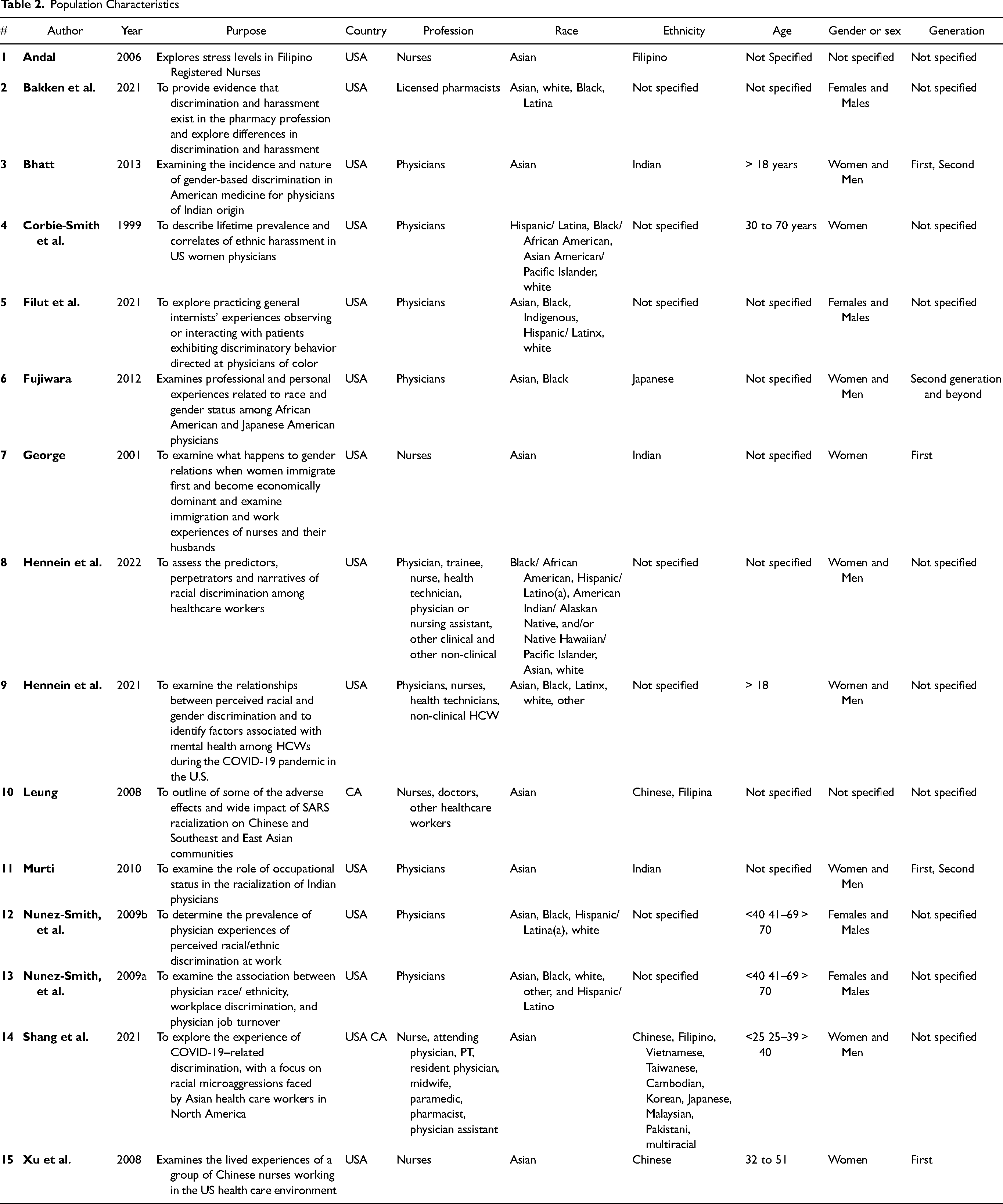
Population description
Population Characteristics
How anti-Asian racism is conceptualized and studied within literature
Through our analysis of extracted data, we sorted the content into three categories to illustrate how anti-Asian racism amongst healthcare workers has been conceptualized, studied, and understood. These categories include: levels of racism, descriptions of anti-Asian racism, and the impact of racism.
Second, anti-Asian racism was examined through notions of inferior professional status of Asian healthcare workers. In some cases, articles examined how Asian physicians were not perceived as doctors, such as white doctors not referring patients to Asian physicians (Filut et al., 2021; Murti, 2010). For other healthcare workers, some articles explored how Asian nurses had their professional capacity and competence questioned in the workplace (George, 2001; Xu et al., 2008).
Third, anti-Asian racism was described in the current literature through Asian healthcare workers reporting experiences of general racial discrimination. Specifically, racial discrimination was studied in the workplace and during training including hearing demeaning comments related to their race and/or ethnicity (Bakken et al., 2021; Bhatt, 2013; Corbie-Smith et al., 1999; Hennein et al., 2021; Murti, 2010; Nunez-Smith et al., 2009a; Nunez-Smith et al., 2009b; Xu et al., 2008) and experiencing microaggressions from colleagues (Hennein et al., 2022). Acts of discrimination were examined across multiple populations including Asian healthcare workers experiencing racism from patients, colleagues, and supervisors simultaneously (Bakken et al., 2021; Bhatt, 2013; Fujiwara, 2012; George, 2001; Hennein et al., 2021, 2022; Leung, 2008; Murti, 2010; Nunez-Smith et al., 2009b). Less commonly, general incidences of racial discrimination were explored from the sole perspective of patients discriminating Asian healthcare workers (Filut et al., 2021; Xu et al., 2008).
The impact of Asian healthcare workers’ experiences was also studied by exploring barriers of anti-Asian racism on career advancement (Bhatt, 2013; Filut et al., 2021; Murti, 2010). For example, the idea of ‘Asianness’ was examined in relation to impacting professional advancements in leadership or administration positions and access to fellowships for physicians (Bhatt, 2013; Fujiwara, 2012; Murti, 2010). Similarly, scholars documented Asian healthcare workers leaving their practice or position in relation to experiences of anti-Asian racism in the workplace (Filut et al., 2021; Nunez-Smith et al., 2009a). The concept of proving or earning their rights within the healthcare system was also explored from Asian healthcare workers’ perspectives (Bhatt, 2013).
Discussion
During a time of heightened anti-Asian racism, these findings add to the small but growing literature on the experiences of Asian healthcare workers. Not only have Asian healthcare workers across North America experienced racism, our findings suggest that anti-Asian racism continues to exist. As a result, further research is warranted to adequately document these experiences, to strengthen our collective understanding of the nuances and complexities across different Asian ethnicities, and to inform action-oriented solutions at the individual, organizational, and system level. In the sections below, we use a critical lens to discuss the implications of the findings and identify further areas of inquiry within the area of anti-Asian racism. Our primary focus on anti-Asian racism intentionally highlights the distinct experiences and challenges of Asian diasporic communities in North American scholarship, which often inadvertently contributes to the erasure of the Asian experience. While these areas of inquiry are relevant to all health professions, we suggest that nursing can play a leadership role in developing knowledge to advance anti-Asian racism policy and practice given the many contexts in which nurses are situated alongside other health care professionals.
Historical and contemporary existence of anti-Asian racism
The recurrent concept of othering of Asian healthcare workers serves as a reminder that anti-Asian racism has historically rendered Asian diasporas in North America as foreigners (Cheah et al., 2020; Shang et al., 2021). In the nineteenth century, xenophobic perceptions of Asian diasporas in North America produced the foundation of the ‘yellow peril’ rhetoric. The ‘yellow peril’ trope vilifies Asian diasporas as ‘foreigners’ and as a threat to the free-market ideologies in North America (Darling-Hammond et al., 2020; Litam, 2020; Tessler et al., 2020). Eventually, the perpetual foreigner stereotype was used to legalize racist North American policies including, but not limited to, the Chinese Exclusion Act in the United States, the Chinese head tax and Chinese Immigration Act in Canada, and the internment of Japanese people across North America (Government of Canada, 2021; Litam, 2020).
Similar to the historical use of the ‘yellow peril’ within immigration and legal institutions, the concepts of otherness, foreignness, and hypervigilance around Asian healthcare workers were prominent in this review. By acknowledging that the ‘yellow peril’ narrative has been legalized across North American institutions, it helps to explain why ‘perpetual foreigner' tropes materialized within the healthcare system such as patients and co-workers being hypervigilant around Asian healthcare workers (Leung, 2008). While we acknowledge the historical presence of anti-Asian racism through ‘perpetual foreigner' stereotypes, it is critical to note that anti-Asian racism continues to thrive presently. These ‘yellow peril’ tropes are used to justify the racialization of global pandemics, such as SARS and COVID-19, and are used as the foundation for the xenophobia and othering of the Asian diasporas in North America (Darling-Hammond et al., 2020; Leung, 2008). Many of the articles in this review are focused on the contemporary existence of anti-Asian racism (Bakken et al., 2021; Filut et al., 2021; Hennein et al., 2021, 2022; Shang et al., 2021), demonstrating how the history of anti-Asian racism continues to manifest in the present-day healthcare system. While the amount of literature we identified in this review was relatively small, the continued existence of such racism warrants further investigation to inform anti-racist behaviors, practices, and policies within the healthcare context.
Building the knowledge base on anti-Asian racism
While this review reflects the existence of anti-Asian racism from past to present, there remains a resounding discrepancy with the importance of addressing anti-Asian racism and the lack of an evidence base attempting to challenge it. Despite not having delimitations on the years and geographic locations within our search where Asian healthcare workers are considerably represented (Shang et al., 2021), this review identified a small sample of articles and even fewer from the Canadian context. Anti-Asian racism has indeed surged in recent years due to the racialization of COVID-19; however, the presence of discrimination against the Asian diasporas has existed since the conception of Canada and the United States of America as colonial nations (Litam, 2020; Tessler et al., 2020). Given this legacy of anti-Asian racism within and beyond the healthcare system, the lack of awareness for this type of oppression is concerning.
The impact of the ‘model minority’ myth within academic and healthcare spaces work to discredit the reality and impact of racism experienced by Asian peoples in the North America context (Pon, 2000). Despite centuries of violence against Asian diasporas, the ‘model minority’ myth allows anti-Asian racism to be strategically and structurally silenced, forming yet another manifestation of how anti-Asian racism is produced and reproduced within the current healthcare system. This, in part, explains the limited literature identified in this review and why Asian healthcare workers may internalize these stereotypes to silence their own unjust experiences. The lack of recognition on matters of anti-Asian racism only serve to solidify the systemic erasure of the Asian experience within North America particularly during a critical moment of widespread suffering and violence. We suggest that the erasure of the Asian experience supports the need to continue documenting and building the knowledge base on Asian healthcare workers’ complex experiences of anti-Asian racism in the three key areas: the pathways of anti-Asian racism, the contestation of monolithic stereotypes, and the negotiation of hypervisibility and invisibility.
Nursing and other healthcare disciplines are often developed on a care ethic that holds a strong mandate for promoting justice across all communities. Accordingly, the egalitarian perception of nursing and health disciplines allows covert racism to remain unchecked by promoting social justice in other areas while maintaining the structural violence of white supremacy (Louie-Poon et al., 2022). The limited literature exposing Asian healthcare workers’ experiences of covert racism provides support to how the existing evidence base strategically neglects covert racism to fulfil health professionals’ outwards appearance of our ethical mandate. In addition to this population under study (i.e., Asian healthcare workers) being linked with the caring roots of healthcare providers, the added complexity of being Asian diasporas is critical. Integral to the ‘model minority’ stereotype is the inaccurate myth and perception that the Asian diasporas living in North America are a token of success among academic and healthcare spaces by upholding a few successful Asian doctors and researchers. Unfortunately, this inaccurate portrayal creates the narrative that Asian healthcare workers are not impacted by racialization (Pon, 2000; Tessler et al., 2020). With this understanding, we assert that this silencing of the Asian experience through the ‘model minority’ stereotype is one mechanism of how covert racism manifests for Asian healthcare workers. It is only until Asian diasporas are used as scapegoats during global pandemics (i.e., SARS, COVID-19) that more outwards violence towards this population is highlighted in the media and the otherness of Asian healthcare workers are studied, as documented in several articles in this review (Hennein et al., 2022; Leung, 2008; Shang et al., 2021). Taken together, there may be a societal perception associating overt racism with ‘perpetual foreigner’ narratives and covert racism with ‘model minority’ narratives, which may further explain the limited attention on covert racism for Asian healthcare workers.
The exclusion of covert forms of racism within our review add to the existing evidence base documenting that subtle pathways of racism are often strategically overlooked within nursing and other healthcare disciplines (Louie-Poon et al., 2022). We contend that this continues to be concerning given that both overt and covert pathways of racism work in tandem to legitimize and support white supremacy (McKay, 2019; Racine, 2021). We require more scholarship that moves beyond reactive analyses of overt racism, to proactively studying all pathways of racism in order to capture the complexities of anti-Asian racism and its impacts on Asian healthcare workers.
On the basis of these findings, potential direction for our future research, policies, and education may seek to understand the shared and distinct experiences of various Asian ethnicities, the differences between Canadian and American healthcare contexts, and how different healthcare workers of Asian origin negotiate spaces within the healthcare system. In doing so, scholars in this area can begin contesting the monolithic stereotypes enforced on Asian diasporas, while creating a collective voice for the pan-Asian experience.
Importantly, academic and healthcare spaces require investing in tangible actions that allow Asian healthcare workers to resist the ‘model minority’ myth and begin taking up space in the pursuit towards racial justice, while working in solidarity with Black and Indigenous communities. In the absence of discourses on the Asian experience and the limited scholarship exploring the nuanced pathways of anti-Asian racism, commitments that promote the safety and racial justice of Asian healthcare workers will remain unheard and undervalued. Therefore, achieving the awareness and commitment toward dismantling anti-Asian racism within the healthcare sector necessitates a responsibility for anti-racism action.
Engaging in action-oriented anti-racism
Despite the need for tangible, action-oriented anti-racism, our review of the literature suggests that significant progress towards disrupting anti-Asian racism is still warranted. While we focused primarily on the experiences of anti-Asian racism, anti-racism recommendations remain a gap within this extant literature. Although, some articles highlighted strategies to counteract anti-Asian racism in the healthcare system including the need to support the retention and representation of Asian healthcare workers (Hennein et al., 2021), providing psychological services to Asian healthcare workers (Shang et al., 2021), and strengthening the efforts to enforce existing policies against racism (Xu et al., 2008), drawing explicit attention to dismantling racial power hierarchies was nearly absent across all included articles.
In some cases, scholars focused on the integration and adaptation of Asian healthcare workers into their workplace as a solution to anti-Asian racism. It is important to note that while the inclusion of systematically oppressed populations has been widely adopted by institutions (e.g., professional organizations, academia, health service organizations) as the standard response within the ‘equity, diversity, and inclusion’ movement, representation and inclusion insufficiently reflect anti-racism practices, which fundamentally require addressing institutional power structures rooted in whiteness to amplify systemically marginalized voices (Toraif et al., 2021). Such narratives which opt for changing how Asian populations exist within institutions constructed on whiteness may become a harmful tactic that covertly protects and reinforces white supremacy. Future direction in the area of anti-Asian racism scholarship must focus on dismantling the systemic oppression rooted in a long history of anti-Asian violence, rather than relying on Asian healthcare workers to build resilience within the spaces they occupy. Specifically, recommendations must move beyond reactionary and performative actions that focus on the adaptability of historically oppressed individuals to proactive solutions that are targeted, measurable, and designed to challenge the systemic and institutionalized practices and policies built on white supremacy.
Limitations
The articles included in this review do not represent all of the extant literature focused on anti-Asian racism and healthcare workers given the exclusion of editorials, commentaries, books, and conference proceedings. However, with the sample of articles included in this review, we have a sufficient starting point to understand the current gaps within the literature and the multiple areas requiring further inquiry.
Conclusion
The current study presented a timely review that outlines the nature, extent, and range of literature on Asian healthcare workers’ experiences within the Canadian and American contexts. These findings suggest that contemporary scholarship on the experiences of anti-Asian racism within the healthcare system are reminiscent of the historical legalization of racial discrimination and stigmatization of Asian diasporas. Despite the presence of anti-Asian racism, the limited literature examining the complexities and nuances of the experiences of anti-Asian racism for Asian healthcare workers is concerning. Future scholarship requires further investigation that comprehensively explores the multiple pathways of anti-Asian racism, the contestation of monolithic stereotypes, and how Asian healthcare workers negotiate both hypervisibility and invisibility within healthcare spaces. Investing in and engaging in action oriented anti-racism strategies that targets systemic racial power hierarchies is required to address this long history of anti-Asian racism and to move beyond reactionary and performative action. Undoubtedly, we are at a critical crossroads that demands us to re-examine the existing narratives and actions used to justify assimilating Asian healthcare workers into spaces without challenging or changing the violent systems that often preclude Asian healthcare workers from full participation.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621231166101 - Supplemental material for Asian Healthcare Workers and Their Experiences of Racism in North America: A Scoping Review
Supplemental material, sj-docx-1-cjn-10.1177_08445621231166101 for Asian Healthcare Workers and Their Experiences of Racism in North America: A Scoping Review by Samantha Louie-Poon, Patrick Chiu and Janice Y. Kung in Canadian Journal of Nursing Research
Footnotes
Disclosure statement
The authors reported no potential conflicts of interest.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.