
Abstract
Background
This article reports an evaluative replication study, including a workshop inspired by Paulo Freire's critical pedagogy. Purpose: Assess how the nursing students’ participation in critiquing Canadian empirical evidence on men's health literacy provokes new perceptions; explore students’ intentions of incorporating the aforementioned contents into their professional practice; and test students’ skills to formulate a hypothetical short action plan about men's health literacy.
Methods
A qualitative evaluation study inspired by the qualitative program evaluation approach. The setting was a university-based Canadian undergraduate nursing program located in a major metropolitan city. Seventeen undergraduate students (representing 3.65% of year 4 student population) composed the sample. The educational intervention was two workshops (6 h duration; February 2017) including a lecture about men's health literacy with video presentations, class discussions and group work using Freire's method of reflection and discussion for awareness awakening. Hypothetical health literacy promotion was the key outcome. All interactions were digitally audiorecorded, verbatim transcribed and submitted to thematic analysis having as themes: Perspectives of awareness and knowledge expansion, and New personal-professional assets.
Results
Students were able to relate new knowledge with their own experiences in the classroom or in the practicum. Application of new knowledge was related to students’ social circles and reported familiar health matters. Cultural and community life shaped knowledge expansion and references to men's behaviors.
Conclusions
Mobilization of personal knowledge awoke students’ awareness about gaps in the nursing curriculum and the paucity of experiences in clinical placements relating to men's health literacy.
Background & purpose
This article reports on an evaluative replication study, including a workshop inspired by Paulo Freire's critical pedagogy used previously with health and social services providers in Canada and Brazil (Zanchetta et al., 2014; Zanchetta et al., 2015a,b), but never with undergraduate nursing students. Freire's critical pedagogy enacts liberation and social change in the learner, stimulating a desire for action which addresses inequities and oppression (Freire, 1973) since the learner's dreams are the master guide to the education process. It incorporates social justice, equality, freedom, and democracy into the learner's consciousness (Gibson, 1999).
The immediate workshop evaluation by students equally addressed students’ satisfaction with the learning opportunity and the overall need to address Health Literacy (HL) among male clientele. As a social determinant of health (SDH), HL can be strategically used to reveal disparities in healthcare (Dodson et al., 2015), implying the need for participatory learning initiatives targeting both nursing students and healthcare providers, to improve their skills as agents of change in their communities of practice. HL evolved from a perspective focused on individual skills and competencies to mobilize them to interact with the healthcare system (Liu et al., 2020) toward a more complex, broad conceptual one (Pleasant et al., 2016).
Pleasant et al. (2016) proposed a reconceptualization of HL as a multidimensional concept entailing the idea of exchange between an individual's skills in health matters as well as the demands and complexities of the healthcare system. Moreover this new conceptual framework also considered the context, system of norms, expectations and regulations that influence the use of skills and configure the resources availability. Therefore, HL can exist at different levels, in each there is an inner variation of increased or diminished skills, as well as the interaction with a context and the diminished skills that could impact the process of HL itself. The contextual aspect of HL does involve healthcare organizations’ responsiveness to the individual and community HL (Dodson et al., 2015), as well as HL competent health professionals (Cesar et al., 2022) to ultimately tackle and reduce health inequities (Schillinger, 2021).
HL-specific content in nursing curricula (e.g., use of plain language, visual material, and HL screening) can improve nurses’ abilities to care for patients with low levels of HL, resulting in appropriate assessment skills, intervention planning, and better health outcomes (Mosley & Taylor, 2017). The nursing health promotion (HP) practice to improve men's HL (MHL) levels requires nurses to enact roles for HL understanding, knowledge application and innovation in practice and abilities. It is particularly relevant for men belonging to groups at risk for low HL, demanding nurses to advocate for the clientele's empowerment through HL-based initiatives (Zanchetta et al., 2012).
To enhance men's health indicators, MHL is an epidemiological relevant factor to be addressed. Men in Canada have higher hospitalization rates due to heart attacks, mental illness, and motor vehicle accidents. Hospitalizations due to alcohol use among men were 143 per 100,000 compared to 56 per 100,000 women. Low-income men were 2.5 times more likely to be hospitalized compared to high-income men, and 2.1 times higher for low-income women compared to high-income women (Canadian Institute Health Information ([CIHI], 2015). Canadian Indigenous men's life expectancy is 72.5 years, which is significantly shorter than that of non-Indigenous men (Tjepkema et al., 2019).
Canadian men have high suicide rates, low rates of depression diagnosis, and poor mental health service engagement. The proper use of mental health services can decrease the negative impacts of mental health problems (Ogrodniczuk et al., 2016). Out of 24,607,300 Canadians, 12,713,600 males older than 12 years of age perceive no need for mental healthcare, despite the fact that suffering from depression in the early stages of life leads to manifestations of anger, aggressiveness, and risk-taking behaviors in subsequent years (Statistics Canada, 2019). In addition, higher hospitalization rates due to substance use in men are reported in comparison to women. Furthermore, seven out of 10 hospitalizations for substance use in Canada involve a mental health issue; the use of illicit substances due to mental health is at 12% for men compared to six percent for women (CIHI, 2019).
Men make up 54% of those below 65 years of age who are diagnosed with dementia (CIHI, 2018). Young-onset dementia often leads to longer hospitalizations due to the difficulty of finding appropriate services. Individuals with young-onset dementia face severe levels of cognitive impairment compared to others who develop dementia as older adults. Initiatives targeting men who experience young-onset dementia represent another area in which men require specialized care from healthcare providers. When seeking care for chronic conditions, men face challenges with accessing services, locating health information, and interacting with healthcare providers to overcome the lack of support (Zanchetta et al., 2017).
This research is vital to fill the content gap in nursing education about men's health. Its social relevance relies on the fact that global statistics for risk factors for men's health remain unchanged (Word Health Organization [WHO], 2022). WHO (2022) reported that alcohol consumption by men is almost three times more than for women; smoking remains prevalent among poorest men; and obesity among men aged 15–49 years remains of high prevalence. Obesity in older male children and adolescents remains highest in the Americas (16.6% in 2016). Men's mental health is relevant to tackle the issues of violence against women, who globally have reported (about one in four) as subjected to aggression since the age of 15. Similar to Canadian statistics about men's health (CIHI, 2015, 2019; Statistics Canada, 2019), WHO's (2022) and the Global Action on Men's Health's (n.d.) reports both indicated that boys, and adolescent, adult and older men's health should be a concern for nursing education, research and practice to bring forward the unique contribution of the profession to the growing global action for enhancement of men's health.
The chosen conceptual framework to guide this research was critical education (Freire, 1973). This philosophy guided the structure of this workshop, its content delivery method, the learning objectives, as well as the individual and group activities incorporated within the workshop. This also calls upon the educator to capitalize on a dialectic approach between themselves and the student, stimulating the latter's experiential knowledge via evocative artifacts (i.e., picture, drawing, object, etc.) to recall their individualized realities (Freire, 2001). By recalling their personal experience associated with these objects, the learner is able to self-reflect on their memories and ideas while connecting them to their current realities in their practice settings, but also to critically consider the inequalities and injustices occurring within their sociocultural context.
Three objectives guided this study: (a) To assess how the nursing students’ participation in critiquing Canadian empirical evidence on men's health and MHL provokes new perceptions of these issues; (b) To explore nursing students’ intentions of incorporating the aforementioned contents into their professional practice, resulting from the collective debate of personal values and opinions grounded in their clinical placement experiences; and (c) To test nursing students’ ability to formulate a hypothetical short action plan about men's health and MHL promotion, to be integrated in one's chosen practice setting. Two questions that guided this qualitative evaluation research, related to the educational workshop entitled “Awakening undergraduate nursing students’ critical awareness about men's health, MHL and nursing practice”: (a) How did the workshop expand the nursing students’ visions of men's health and MHL, and how it relates to their future nursing practice? (b) Which nursing students’ attitudes, skills, motivation, or intended behaviors did the workshop influence?
This workshop was innovative because it was the first educational research initiative at the School that was fully created within an intellectual partnership with undergraduate nursing students who played key roles. The workshop was designed to address the students’ self-identified School curriculum gaps on men's health and men's HL both in classroom and scarce experiential learning on these matters in the clinical placement setting as corroborated by students in the study conception phase. Students were co-creators of the workshop contents, co-investigators, co-designers of the study and participated in data collection and co-analysis of the collected evidence with a leading faculty member to respond to students’ interest in extra-curricular learning.
Special gains were also acquired for those undergraduate students enacting the role of a co-investigator and co-author for the first time. Students consolidated their autonomy by being responsible for seeking, selecting and synthesizing Canadian evidence to compile the body of knowledge to be shared with attendees. Another gain was the first-hand opportunity to establish an equitable intellectual collaboration with a senior faculty profiting of freedom to share ideas and opposite argumentation among the team. Students also, for the first time, experienced a scholarly climate of ideas confrontation aiming to reach an inclusive consensus. Moreover, it was an opportunity to learn about a new engaging teaching method of using simple and playful objects. This method allows students to recall experiences, knowledge, and ideas about the way men deal with information about health, taking care of themselves, and looking for medical help.
Methods and procedures
Design: This qualitative evaluation study design was inspired by the qualitative program evaluation approach that proposes utility, feasibility, and propriety evaluation standards of a given program (Greene, 2000; Patton, 2002; Rossi et al., 2004). The aim of such program evaluation is to collect detailed information about a small number of participants to produce an in-depth understanding of the program's outcomes, even if this reduces the generalizability of its results (Greene, 2000; Patton, 2002; Rossi et al., 2004).
Setting and sampling: The setting was an undergraduate nursing program delivered by a Canadian university in a major metropolitan city. The eligible population of this nursing program was approximately 465 undergraduate students enrolled in their last year (4th year). From it, a sample of 17 undergraduate students took part in the study.
Recruitment: An email sent out to the prospective workshops’ attendees by the Student Affairs Coordinators, and short notices were posted on the year four nursing student Facebook page and the personal Facebook page of the student researchers. Criteria for inclusion were: (a) a year four undergraduate nursing student; and (b) accepting to provide the signed informed consent to audio-record one's participation in the discussion groups. Criteria of exclusion were (a) not a year four undergraduate nursing student; and (b) refusal to provide the signed informed consent to audio-record one's participation in the discussion groups.
Method of work: The evaluation research was implemented through two workshops, each six hours in duration, as an educational intervention delivered on February 21 and 22, 2017. All in-class interactions among students and facilitators, as well as their accounts while working in groups, were audio-recorded to allow the appraisal of learning and indicate awareness awakening.
Ethical considerations: This study was approved by the University's Research Ethics Board (REB 2016–444). Some students responded to the invitation to attend the workshop, but did not accept to take part in the study. To ensure that their oral statements would not be audio-recorded, they chose to pause the audio-recorder when they spoke during the session. Moreover, for the students who did consent, they were given the option to also pause the audio-recording of their oral statements at any time during the session. No financial compensation or incentive was offered to students. Students’ free participation was a gesture of goodwill. Refreshments were provided to support their basic nutritional needs.
Data collection procedures: The procedures included intellectual stimulation, provocation of exchange of ideas and opinions, and sharing of thoughts and personal standpoints about the topics presented in the flow of activities as described below. All responses to those interventions and any other spontaneous in-class verbal interactions among facilitators and students as well as among students themselves when working in small groups were audio-recorded.
The intervention: the workshop flow
The detailed information about the workshop flow guides the discovery of recall of inner experiential knowledge that underpins the gradual process of awakening awareness. The students were informed that audio-recording devices were placed in multiple areas in the classroom to register the full dialogue among them and the facilitators. The workshop began with greetings and the presentation of the research, followed by a discussion and gathering of the signed informed consent forms. During the lectures, a co-investigator student was responsible to pause the audio recording when any of the four non-research participants asked a question and shared a comment. The intervention was the workshop as it unfolded by this flow of activities:
1- Brainstorming: We asked questions about preliminary ideas, including : (a) In what ways are inequities in health represented among men?; (b) What are men's perceptions of health and well-being?; and (c) How do men access and use health and social services?
2- As an ice-breaker activity, the video entitled “You’ve Got Male” (https://www.youtube.com/watch?v=L1MJ8lTk-ig) was presented and followed by a short discussion about men's health and SDH. The lecture proposed a discussion and reflection about the current context for boys, youth and men's HP as a concern for nursing practice.
3- Lecture: Presentation of Canadian evidence about: (a) profile of medical consultations throughout life; (b) men's health and SDH; (c) current context for boys, youth and men's HP; and (d) overview of current definitions of HL. This overview of the conceptual definitions of HL served as the main framework for the workshop. HL was introduced as an ability to: (a) access, read or listen to, process, and appraise textual, graphic, and numerical health information; (b) build new meanings from health information; (c) understand health messages and communicate them in users’ social environments; (d) navigate the healthcare system; (e) use textual, numerical, and graphic health information to inform decision making, reduce health risks, and enhance quality of life; (f) use health information to access healthcare in a medical culture that requires self-defense and health vigilance; (g) evaluate and communicate health information to improve one's life and one's family's life; (h) solve health problems by using multiple forms of language (i.e., written, oral, visual, tactile etc.) at multiple levels (i.e., individual, family, community, world) and in multiple contexts (i.e., home, work, school); and (i) use all family, school, social, cultural, and professional assets gathered through continual learning (formal or informal) from regular contact with information, knowledge, attitudes, and health behaviors in all aspects of life (Zanchetta et al., 2012).
4- Video presentation and class discussion: “When the storm hits” (https://www.youtube.com/watch?v=r_-ibxtXO3g) was presented to support the discussion about the neglected aspects of men's affective life as related to fathers’ grief over their unborn and deceased offspring and the resumption of life in the post-partum period.
5- Lecture: The lecture entitled “What do we know vs What we do not know: How to… Then” followed the video presentation with discussion of actions to promote men's health, emphasizing the knowledge gaps in strategies to promote men's health.
6- Video presentation and discussion: Movember 2016: Stop Men Dying Too Young (https://www.youtube.com/user/movembertv). The video was presented as a foundation for a brief discussion on the Canadian scientific evidence about men's health from sub-groups of men and HL dimensions.
7- Lecture: Presentation of evidence regarding children, pre-adolescents and teens (i.e., respiratory diseases and diabetes), youth (i.e., HIV, mental health, sexual health, newcomers and street-involved youth), young adults, adults and seniors (i.e., colorectal, glioblastoma, leukemia, lymphoma, as well as kidney, liver, and prostate cancer), diverse sexual orientation, transgender, sexual abuse, pornography, and new immigrant. The lecture concluded with the proposal of some solutions to organizational health policies, implementing psychosocial screening tools and procedures, and strategies for masculinity campaigns.
8- Exercise applying Freire's method of raising awareness (Freire, 1973) with evocative objects. Instructions provided were: (a) form groups of three-to-four participants; (b) individually reflect (in silence) on the object you have (2 min) (see Image 1); (c) ponder (in silence) on the relationship between the object and the empirical information presented, considering your personal experience and the reality of lived community or your student clinical placements with male clients of any age (2 min); (d) disclose your thoughts about the object and identified area of promoting men's HL (3 min); (e) analyze what dimension of HL is more common in your group's thoughts (20 min); and (f) create a hypothetical plan of action to incorporate that specific dimension of HL to improve your nursing practice. Relevant areas in the plan included: key dimension of HL, target sub-group of men, men's life or clinical context, plan target objectives, priority actions, and major indicators of success (50 min); and (g) present briefly, as a group, their plans of action (20 min). During the group exercises, the non-research participants were tasked with recording the group session and pausing the recorder when the participants spoke.
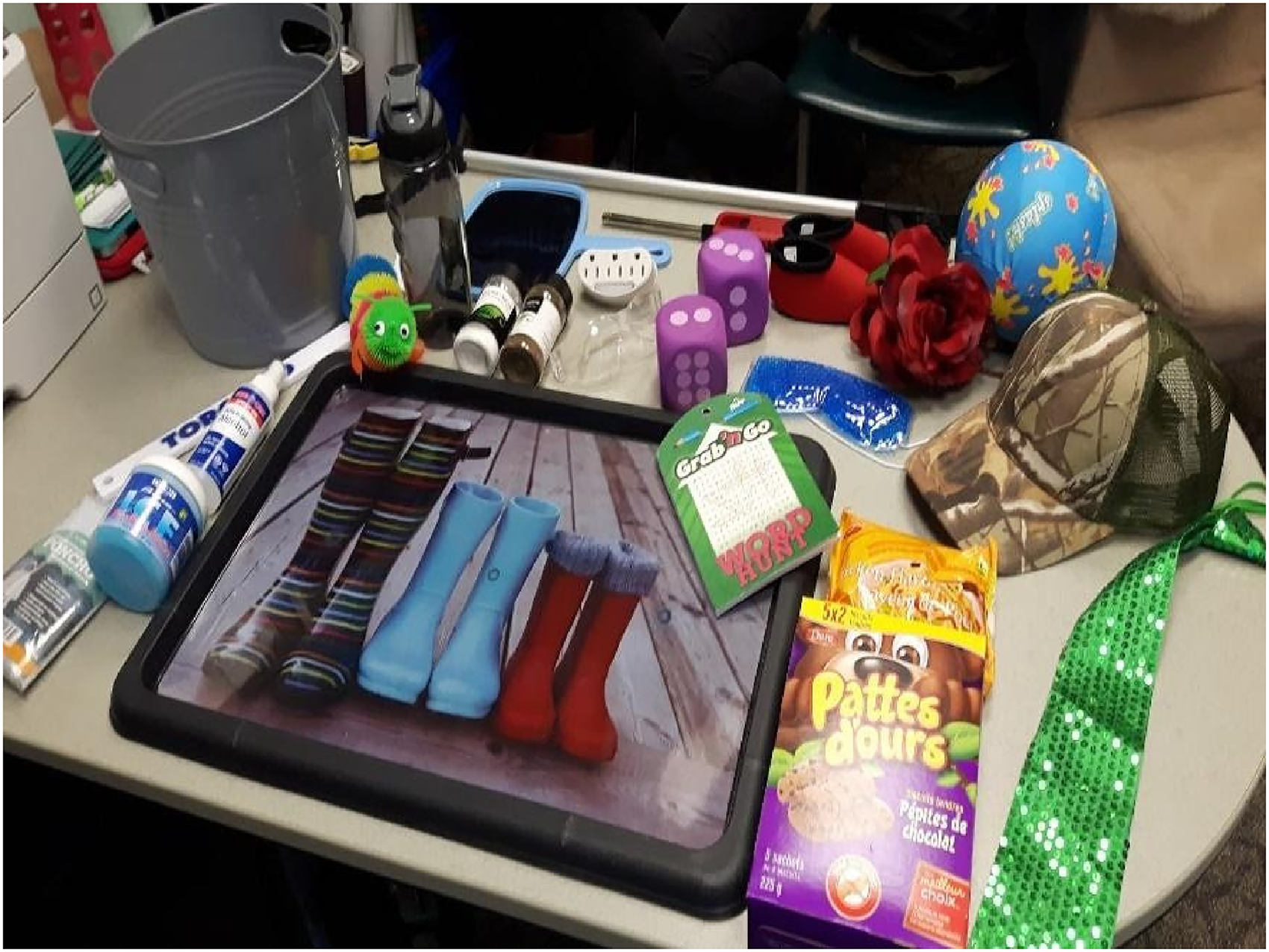
Evocative objects.
9- The class resumed with the presentation and discussion of the hypothetical plans of action, with a general appraisal and feedback of the plans of action.
10-The last step was completion of the workshop's evaluation forms as part of an evaluative study. Anonymously filling out a printed form, participants answered the following questions: (a) How did this workshop help you to learn about men's health issues and MHL?; (b) How did this workshop help you to expand on your ideas about the issues linked to social inequities in men's health?; (c) What ideas do you have now about your work with the community to promote MHL?; and (d) How could this workshop have been more useful for you as a future nursing professional?
Data analysis procedures
All digitally audio-recorded files were transcribed verbatim and coded using ATLAS.ti qualitative software. To support the procedures of thematic analysis, as recommended by Paillé and Mucchielli (2016), the first and fourth authors created an initial list of 15 main codes and their 130 sub-codes as follows: acknowledgment (n = 3), commenting in lectures (n = 5), existing knowledge (n = 5), first reaction regarding MHL (n = 7), intentions (n = 19), knowledge application (n = 3), new vision of MHL (n = 6), objects (n = 12), perception MHL (n = 41), perceptions (knowledge/practice) (n = 4), personal empowerment (n = 1), plans (n = 9), questioning in lectures (n = 9), new motivations (n = 2), and second reaction MHL (n = 4). The final coding output was analyzed using the following procedures: (a) identification of themes after intensive and repeated readings of the coding report; (b) creation of a thematic index with reflections about the content of the discussions and attempts to re-group the themes; and (c) codification of transcribed discussions using two predefined themes (Expansion of the nursing students’ visions of men's health and MHL, and possible application to their future nursing practice; and Workshop's influence on nursing students’ attitudes, skills, motivation, or intended behaviors), refinement of the theme titles (Perspectives of awareness and knowledge expansion
This research responded to criteria of scientificity for qualitative studies (Miles et al., 2020) by using triangulation for data analysis, testing the viability of patterns, incorporating comments from informants, and auditing by an external examiner, as well as incitement to discourse (Creswell, 2007). This was possible since the second and third co-authors, who were not directly involved in the workshops’ delivery, reviewed the digital audio-files verbatim and workshops’ notes. The interpretive validity was reached and endorsed through this research responding to different audiences’ issues of culture, ideology, gender, textual language, relevance, advocacy, and standards of respectability (Miles et al., 2020).
Results
The workshops were attended by 21 students and, despite previously announcing that it would be part of an educational research study, four attendees refused to participate as research subjects (19%), resulting in a participation rate of 81%. The results reported in this section relate only to the narratives recorded by 17 students (representing 3.65% of year 4 student population) as the research subjects, although the other four students remained integrated in the first part of the workshop and in the groups’ practical activities.
The results presented in this section relate to all expressions of understanding, questions, disclosed reflections, and thoughts, as well as the completion of group learning exercises. The initial brainstorming questions about representation of inequities in health among men led to the following answer: … men are historically burdened with caregiver status, they have women … who cares for them … even when I call my dad… I say are you going to the doctor?… It's an innate thing that women are caregivers (an unidentified female student).
A question about men's perceptions of health and well-being was answered as: …the first thing that comes to mind is physical, being strong and being capable of doing stuff by myself… and not going to the doctor until it's severe (an unidentified male student).
Other students discussed men's access and use of health and social services as: For me, I only go to the family doctor if it's needed… I never do a physical check up… (an unidentified male student).
I find after a certain age they don't access health and social services…their perception of self is changing… it goes hand and hand with their masculinity… and after a certain age they do prostate checks and that's emasculating (an unidentified female student).
Some of the attendees, once stimulated by the discussed evidence, shared their personal experiences with men's behaviors, attitudes and decisions as witnessed by the students within their social circles, family and in the context of individuals they interacted with in their clinical placements. During interactions in class among facilitators and attendees, the facilitators assured students that there was no wrong or right answer, as all ideas would contribute to revealing the level of new awareness about men's health that will be the base of new knowledge. Due to the fact that facilitators only met the students on the workshop date, it was not possible to inquire if participants had any previous level of knowledge among them. Therefore, it was not possible to anticipate how much information participants would decide to share with others and its consequent impact on their learning. I actually go to the doctors quite frequently and I feel not ashamed that I'm doing that… my doctor says ”Why are you here so often? You’re a man in your twenties.” (an unidentified male student).
The presentation of the second video, focusing on men's grief, stimulated the disclosure of a surprising reality: I’m used to females… opening up to me when they are upset or grieving … recently I had a male client who was opening up to me … it caught me off guard… I’m not used to it (an unidentified female student).
Then, after lecture resumed, a third video about men's mortality provoked a criticism about Canada's attention to men's health: Ireland and the UK are the only countries who really started to promote men's health… Canada, despite our reputation, we do not have this (an unidentified female student).
The lecture concluded and, once distributed into 7 groups in separate rooms, the students each received an evocative object, followed by the instructions (see picture 1). As the group exercise began and students started sharing their initial thoughts expressing the links among presented empirical evidence, evocated ideas and the represented dimensions of HL, they demonstrated an immediate grasp of the underlying connections: … it has a lot to do with the whole construct of masculinity… the man is supposed to be strong… in the face of all of these hardships… that makes it difficult… for men to fully experience grief (an unidentified female student).
Expansion of students’ visions of men's hl and men's health
The expansion resulted from a group exercise where students created hypothetical plans of action. More than half of the student groups created their plans on adolescents to young adult men (aged 18–30) as their self-selected target group. The most common clinical context in this subgroup was sexual health. It is worth noting that the majority of the students were also in this age range, suggesting that students could be thinking of how these plans of action could help their peers, friends and even themselves. Many of these plans included social media or the internet to promote their tool or receive feedback about it. Thoughts around how to engage the largest number of individuals were central to the decision of using online methods: The prevalence and complication of having… heart complications … We wanted to touch up on social media because there are a great number of men from 20 to 30… we are using plain language (an unidentified male student).
To have politicians work with us to increase these bylaws in making regulations mandatory for sports clubs as well to increase the screening… premature deaths (an unidentified male student).
Groups also demonstrated the importance of using individuals from their target subgroup to develop their tool, in an effort to ensure their tool is effective in achieving their goal. … we want to implement our research information. …on how to navigate the mental health websites… we want to see an increased number of doctor visits… and community centre visits (an unidentified male student).
The plans of action addressed the HL dimensions of: Understanding health messages and communicating them in users’ social environment (n = 3); Navigating the healthcare system (n = 1); Using textual, numerical and graphic health information (n = 1); Using all family, school, social, cultural, and professional assets gathered through continual learning (formal or informal) from regular contact with information, knowledge, attitudes, and health behaviors in all aspects of life (n = 1); and Solving health problems using multiple forms of language at multiple levels and in multiple contexts (n = 1).
An example of a hypothetical action plan follows:
- Dimension of HL: Use all family, school, social, cultural, and professional assets gathered through continual learning (formal or informal) from regular contact with information, knowledge, attitudes, and health behaviors in all aspects of life. - Clinical context: Inability to cope/manage well with chronic health conditions. - Target subgroup: Men aged 40–60 yrs. - Objectives: (a) To recognize available or potential assets through regular contact with HCPs, family members, and social circle/support groups to facilitate continual learning; (b) To reflect on personal feelings (individual and collective), experiences, and values related to the condition; and, (c) To create an individualized plan of exploring and using the identified resources. - Priority actions: (a) Educate clients, family members, and friends on the available resources by providing clients with tangible information or referrals to health services and accompanying clients to referred community services or invite individuals from these services; (b) Encourage self-reflection through various modes of media (e.g., journals, blogging, and artwork) to allow clients to share lived experiences with others by arranging for group sessions for reflection with those having similar experiences/conditions; (c) Work with clients to identify personal goals related to managing their conditions to develop specific activities needed to reach goals by using identified resources; and, (d) create a schedule on what needs to be done and how. - Major indicators of success: 70% of clients asked for more information about a community service; 80% attendance to accompanied trips to health services; 75% of clients were able to share services with clients of similar health conditions; 50% attendance in group sessions; 70% of participation in self-reflection activities, and 80% of clients reported the development/update and implementation of self-care plans.
The conception of the plans of action also uncovered the high difficulty for the students to operationalize the concept of indicators of success. This difficulty was commonly justified by themselves as an existing gap in the curricular courses about knowledge of evaluation of interventions, projects and programs. An example of formulation of indicators of success by the group whose topic was to change the delivery of health information to high school aged students (as per the original written contents in the plan's sheets) included: (a) Adolescents provide us with their ideas (creation of two youth committees, one being tech support while the other in charge of fun, social activities); (b) Able to create a video of their input; (c) Video is well received by the adolescents; (d) An improvement in their understanding of lifestyle behaviors (diet, physical activity); (e) Able to explain obesity; and (f) Expected range of 15–40% success of change in self-image or weight loss .
An area of struggle related to the establishment of priority actions as students asked many questions to the facilitators about this part of the exercise. The related priority actions are presented from the group who chose the clinical context of the inability to cope/manage well with chronic health conditions (as per the original written contents in the plan's sheets):
Educate clients, family members, friends and others on available resources: (a) Provide clients with tangible information or referrals to health services; and (b) Accompany clients to referred community services or invite individuals from these services. Encourage self-reflection through various modes of media (e.g., journals, blogging, artwork): (a) Encourage clients to share lived experiences with others; (b) Arrange for group sessions for reflection with those having similar experiences/conditions; (c) Work with clients to identify personal goals related to managing their conditions; (i) Develop specific activities needed to reach goals by using identified resources; and (ii) Create a schedule on what needs to be done and how. While some faced struggles, the group who decided to work with the HL dimension of understanding health messages and communicate them in the user's social environment, in the clinical context requiring a change in the delivery of health information to high school aged students, adopted a simple approach to deal with the complex idea of priority setting by stating the following (as per the original written contents in the plan's sheets): (a) Collaborate with adolescents (create a committee) to create the video; (b) Interviews, video blogging, video journaling (snapchat), twitter hashtags, anonymous survey, online forms; and, (c) Group discussion form e.g., fun activities like makeovers, fashion shows, celebrating diversity.
Students’ previous knowledge about Bloom's taxonomy of educational objectives (Armstrong, n.d.; Isaacs, 1996) (since this content was taught in the year 3 courses) helped most of the groups to define their plans’ objectives. The group who chose the HL dimension of Navigating the healthcare system targeting the population of young adults and post-secondary students in the clinical context of sexual health stated, as objectives of their action plan (as per the original written contents in the plan's sheets): (a) Recognize the health outcomes associated with risky sexual activities; (b) Explore men's understanding of sexual health; and (c) Acquire skills and navigate resources and healthcare services in the healthcare system. An original handwritten action plan is presented in Image 2.
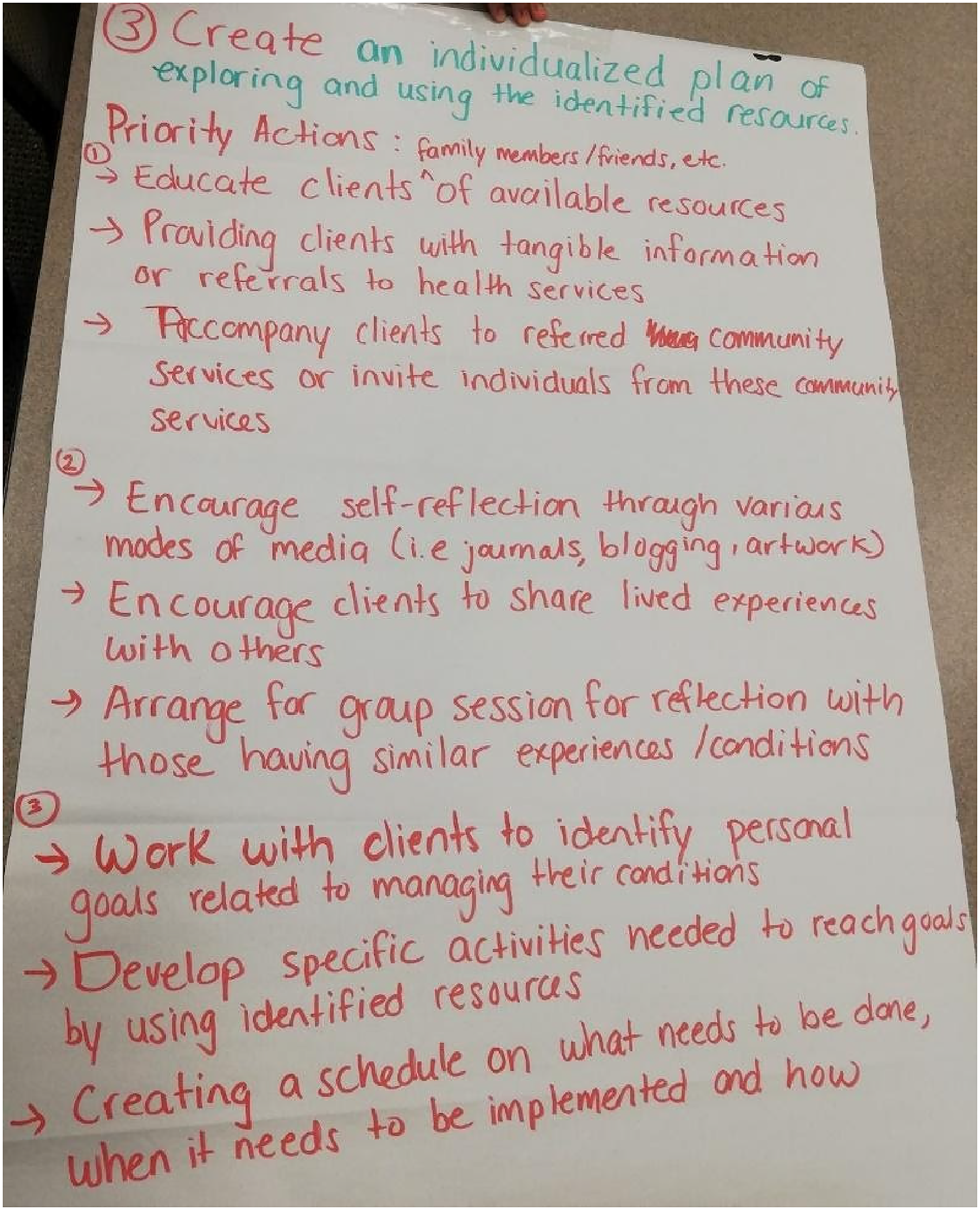
An original action plan.
At the end of the workshop, students provided an immediate, written evaluation of the workshop and documented three major pieces of evidence of such expansion, as inquired by the evaluation questions (see Displays 1 to 3). Students also proposed changes to the workshops to be more useful for future nursing practice. Suggestions included: presenting more strategies to address men's health issues (n = 5); incorporating the workshops into the nursing curriculum (in clinical placements, in community health courses, and throughout four years of the program) (n = 5); presenting more content on men's point of view about their own health (n = 2); and presenting more research content (n = 1). The workshop's immediate evaluation (see Displays 1 to 3) allowed the identification of indicators of new students’ attitudes, skills, motivation, and/or intended behaviors influenced by the workshop regarding working with MHL. Potential benefits of this workshop included: (a) improving students’ problem solving skills, using analysis of the situation as presented by the exercise to create an action plan to resolve a men's health issue: (b) broadening students’ vision of nurses as health educators for men; (c) stimulating students to play a different role as an educator as part of their nursing practice; and (d) feeling motivated to study men's health problems at a graduate level.
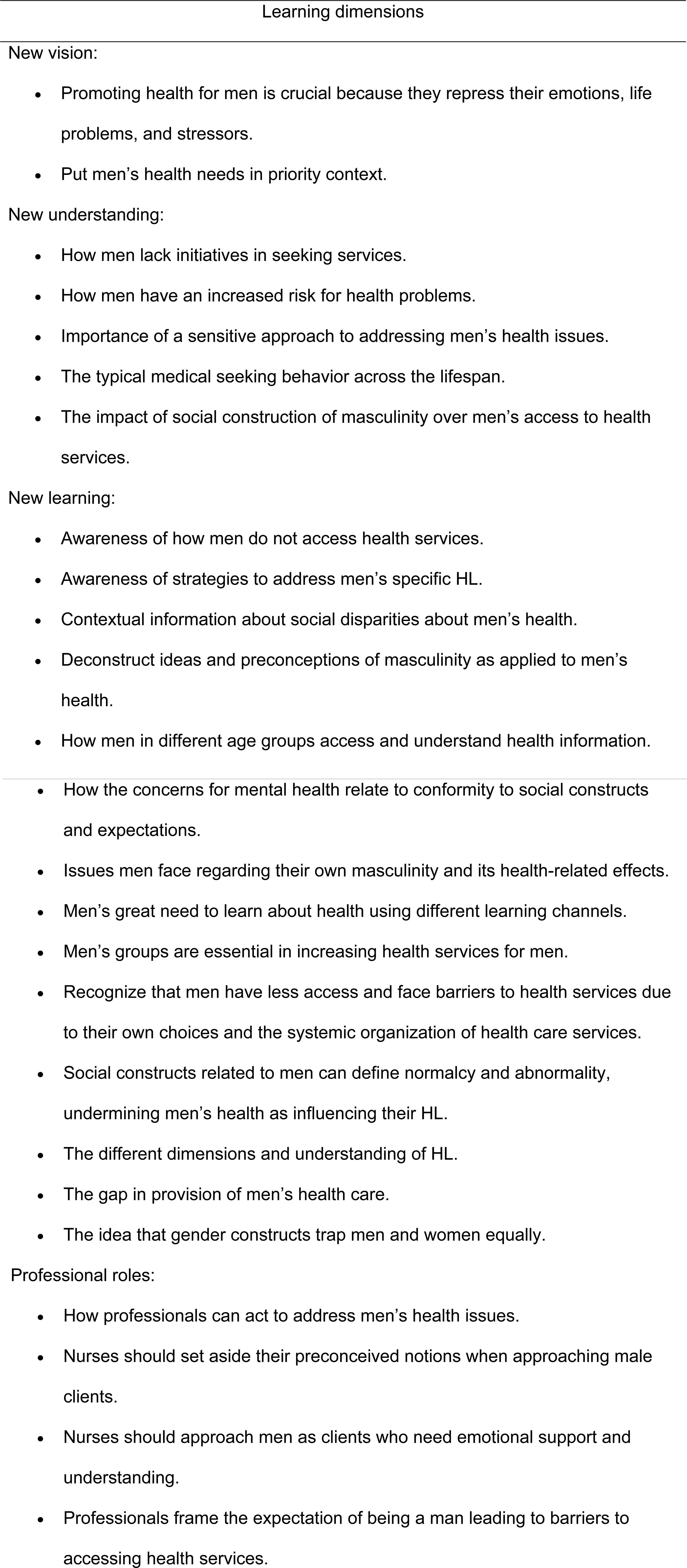
How the Workshop Helped Students to Learn about Men's Health and HL (n = 17 respondents).
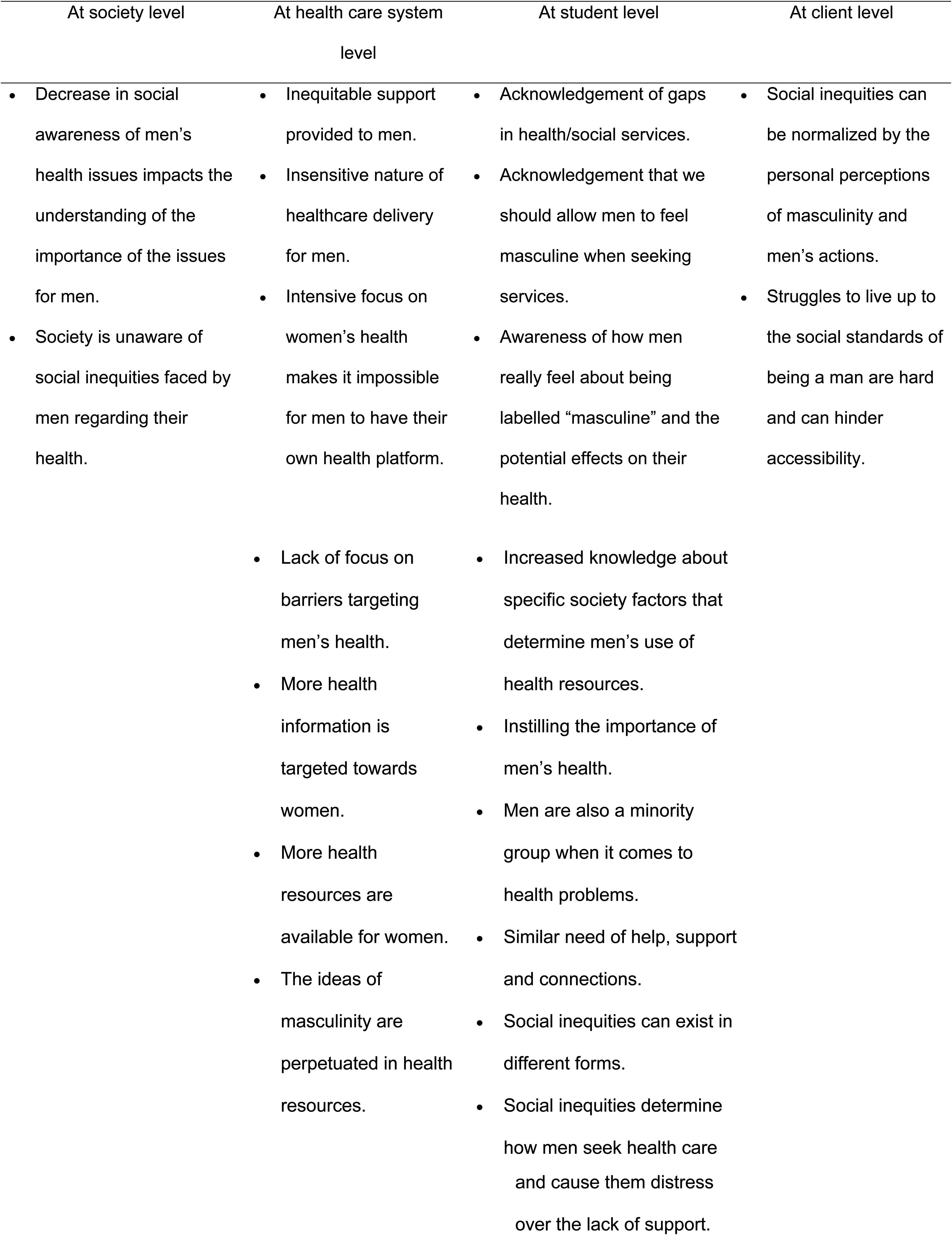
Expansion of Ideas about Social Inequities in Men's Health to Influence Nursing Practice (n = 17 respondents).
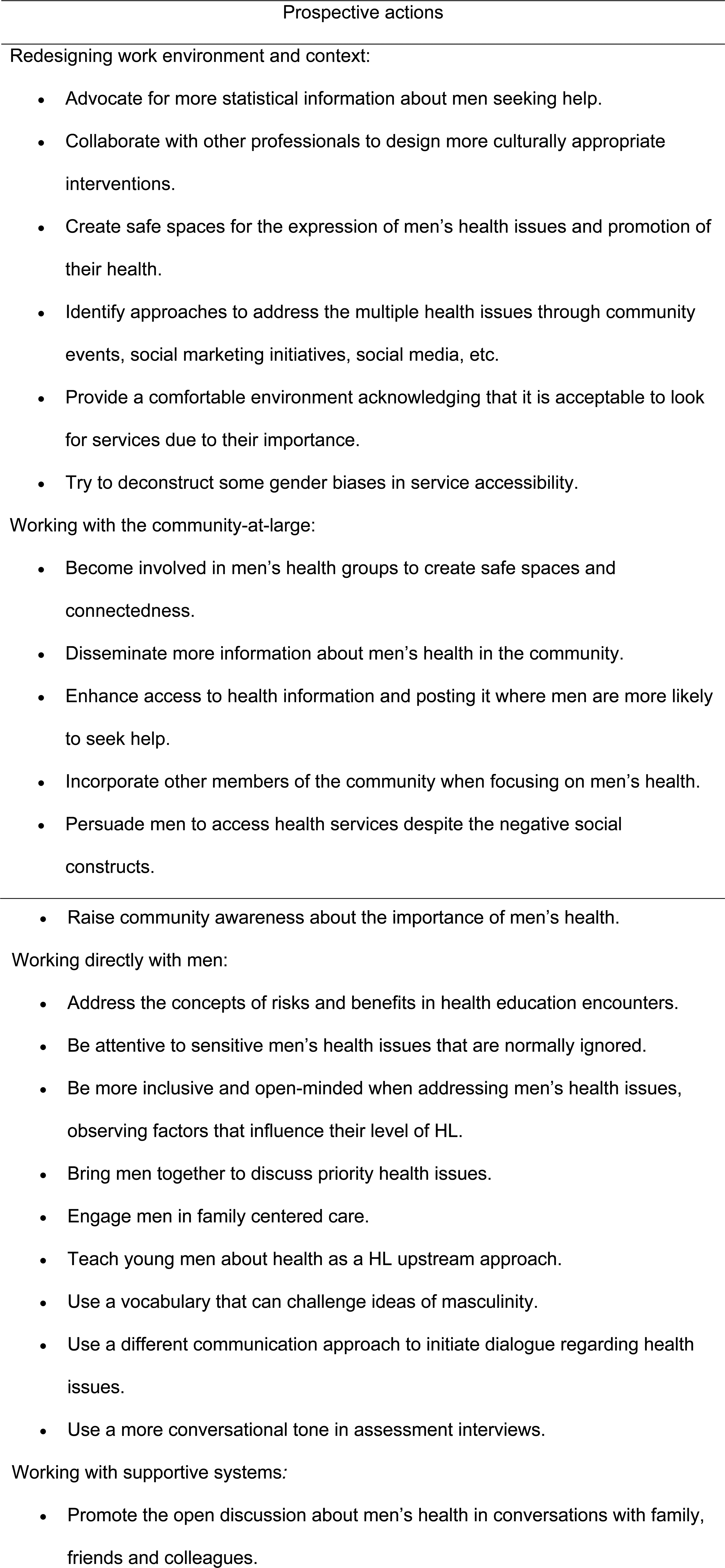
Prospective Actions for Promoting Men's HL (n = 14 respondents).
Thematic analysis
Throughout the workshop, the different activities and discussions expanded the students’ current knowledge of MHL. This analysis unfolded in two main themes, to allow the understanding of the workshop's impact on students’ broad learning.
1-Perspectives of awareness and knowledge expansion
The perspectives of awareness and knowledge expansion concerned the existing lack of knowledge and the recall of the evidence presented in the workshop, making sense of the provided information. When presented with new knowledge on the health inequities experienced by men, students were able to relate this with their own experiences in the classroom or in the practice setting. This relation could be established, as suggested by Weurlander et al. (2018), through drawing on experiences related to students’ social circles, such as family and friends, as commonly reported to other familiar health matters, new knowledge application occurred.
Acknowledgement of inequities in men's health issues and the incipient initiatives addressing MHL inspired students’ formulation of plans of action incorporating the newly acquired knowledge and social media as preferred work strategies. For that, students used affectively appealing subjects to them (De Gagne et al., 2021). Since there were no predominant views expressed by the groups of students, new perspectives were built from students’ acknowledgment of how social constructs may emasculate men's health-related needs, and expectations of masculinity prevent men from caring for themselves. As young individuals, students were aware of the traditional view of men's various societal roles (Courtenay, 1998) that may delay the access to healthcare on both physical and psychosocial levels. Students recognized that men's expectations and roles (as providers for others, while always being emotionally and physically prepared to deal with any hardship) are at stake (Courtenay, 1998). They acknowledged the relevance of support by healthcare providers to shape the way men engage in self-care, since men may feel stigmatization when asking for help, as documented among Quebec men (Montiel et al., 2022). It is particularly relevant in cases of dealing with grief, as students were surprised by their own biases, lack of awareness, and training to approach these cases.
Men's health literacy was only recently analyzed in Canada, based on 2000 data (Oliffe et al., 2020) justifying MHL as a barely incorporated topic in many curricula of healthcare providers’ programs. Students reiterated that their nursing curricula does not provide conceptual and instrumental knowledge to their HL work with compromised MHL. Students’ surprise in relation to their newly acquired and expanded understanding of HL corroborated Akca and Ayaz-Alkaya's (2021) findings that nursing students had inadequate or limited HL knowledge. Students realized that providing men with equitable health begins by educating future nurses on HL. During the discussions in the group exercises, reflection and criticism emerged about the less publicized HL initiatives for men to respond to men's social roles and their related compromises on men's self-care. Students’ analysis about men's health perception as a critical need for men to acknowledge and understand their own level of HL was capital to awareness raising. Students’ awareness about their own lack of skills to deal with men's broad health issues was impressive, as it was experienced during the design of the action plans.
Canadian men's health is influenced by social expectations, surrounding environments, culture, media, and psychological and physiological factors that require specialized interventions to focus on men's health (Zanchetta et al., 2017). However, students’ knowledge about the lack of specific Canadian health policies directed towards making men's health more equitable and accessible was only commented on by one student. As future healthcare providers, these students are expected to recognize that with no public policy, a direct impact exists on resource availability and community knowledge. As an example, Indigenous communities, who are predisposed to diseases due to generational trauma, continue to face barriers that prevent them from accessing the healthcare system. Canadian literature points out that cultural and language differences, long wait times, privacy issues, and a lack of trust are reasons Indigenous men avoided receiving help from their healthcare providers (Zanchetta et al., 2017).
2-New personal-professional assets
New personal-professional assets by participants were immediate gains due to a synergism of attitudes, skills, motivation and intended behaviors. Students’ renewed attitudes were expressed as new ways of thinking about HL and HP, men's health, and even a new perception of men's emotional health. Moreover, their knowledge expansion was embedded with references to men's behaviors (shaped by their cultural and community life) in the students’ close family and friendship circles. It is noteworthy to recall that students identified HL and HP as under-discussed subjects within nursing curricula, which for them are instrumental to their future technical communication skills, and may undermine students’ creativity to address HL in clinical settings (Zanchetta et al., 2012). Such skills are capital for the clientele's well-being and safety in situations like discharge teaching and medication administration, etc (Mosley & Taylor, 2017). New attitudes expressing an emerging critical awareness were due to students’ identification of Canadian men's barriers to harmonize roles and expectations with their own physical, emotional and particularly mental health as influenced by peers (Houle et al., 2017).
Students criticized a lack of exposure to such societal issues, leading to a change in their perspectives on the prioritization of men's health. Nursing programs should have more educational opportunities on this subject matter by incorporating HL and men's health content in lab and live simulations, case studies, problem-based learning, community HP projects, discussion, and concept maps, etc. (Akca & Ayaz-Alkaya, 2021). This pedagogical approach would allow students to expand their upstream critical thinking even within a salutogenic perspective (Roy et al., 2017) regarding compromised Canadian men's health, due to life particularities in rural or urban centers. These common situations emerged from Canadian communities and healthcare systems lacking men's health programs and initiatives (Goldenberg, 2014; Zanchetta et al., 2017).
Students’ reactions to the exercise of designing an action plan, understood as a type of simulation to help undergraduate students mimic the experiences of patients with low HL levels (Weekes & Phillips, 2015), were characterized by the mobilization of their existing knowledge and creativity to practice planning as a new skill. Engaging in self-directed learning and workshop activities has been reported to enhance nursing students’ skills for critical-analysis and problem-solving (Choi et al., 2014), as well as to promote their self-initiative for undertaking independent self-learning and provide opportunities to improve their collaboration and communication skills (Zhang et al., 2012). Such learning unfolded in workshops with a more relaxed and enjoyable environment to learn about the topic, as opposed to more formally-structured lectures (Craft et al., 2017). Workshops as a learning environment influence students’ self-directed learning readiness, which is positively correlated with improved academic performance (Alotaibi, 2016).
Students’ documented intended behaviors suggested a need for more advocacy for men's HP and newly gained knowledge application in clinical placements. Since experiential learning can improve students’ confidence in assessing and communicating with their patients, simulations increase students’ feelings of empathy towards their clientele (Weekes & Phillips, 2015) because students lack the experience to apply their HL knowledge (Williamson & Chopak-Foss, 2015). Through their intentions to advocate for men's HP in clinical and educational settings, students displayed proactive, socially engaged behavior as a key outcome of the workshop.
Discussion
There is a long-lasting acknowledgement among several contexts of nursing education and practice that knowledge of HL is imperative (Speros, 2011) for Canadian nurses, as proposed by Rootman's (2004) seminal conceptual ideas. HL remains an enormous challenge for nurses to address the clientele's increasing complexity and diversity (Wittenberg et al., 2018). As a global issue on the nursing agenda (Zanchetta et al., 2021) and within a complexity perspective for its recent reconceptualization (Pleasant et al., 2016), HL involves mastery of numeracy, scientific, and technological types of knowledge in a social context. Thus, the education of a new generation of nurses to systematically support clientele's autonomy and safe self-care may require an audacious pedagogical approach to instill advanced critical skills that incorporate a refined understanding of complexity. This can be done in close collaboration with students to reconceptualize HL as a meaningful SDH (Schillinger, 2021) to address prevalent social inequities in nursing practice.
Results corroborated that identifying HL levels of nurses and nursing students is important, as this relates to how nurses may potentially improve clients’ health, use advanced communication techniques, and identify their educational needs (Nantsupawat et al., 2020). Incorporating HL in the nursing curriculum is essential to improve nursing students’ teaching skills which will ultimately improve patient care by increasing nurses’ HL (Erunal et al., 2019). Lack of a formal education on skill development to enhance clientele's low levels of HL are at play (Akca & Ayaz-Alkaya, 2021; Nantsupawat et al., 2020).
Such evidence may inform the expansion of educational nursing research agendas to respond to the need for improvement in HL-based undergraduate education. Future studies can explore the social impacts of the mastery of HL, as related to nurses’ and students’ satisfaction with delivered care and their clients’ autonomous decision-making. Inspired by recent analysis (Oliffe et al., 2020), research on nursing education about MHL should also address underlying inequities by exploring the current trend of remote learning and telenursing, as well as live and high fidelity simulations. Nursing practice's current challenges include men's computer literacy, linguistic diversity, scientific literacy with newly arrived refugees and immigrants, vaccine literacy, and e-HL deserve special attention. To enhance undergraduate nursing education on issues of MHL, the following topics can be considered: artificial intelligence and men's health-related decision-making, development of self-assessment/self-monitoring devices, online interactive platforms, and appraisal of health-related websites.
This reported study is an example of an intellectual partnership between nursing faculty and undergraduate students as a highly productive way to inform educational initiatives (e.g., research, knowledge transfer workshops, etc.) in which students are best positioned to advise on the design of meaningful studies/initiatives for their own educational benefit (Bailey et al., 2016).
This study has a main methodological limitation: the lack of confirmation of the findings’ interpretation by the workshops’ participants due to loss of contact with them after graduation. Such confirmation would be an appropriate procedure to demonstrate scientificity through the incitement to discourse (Creswell, 2007). To counteract this limitation, the strategy of having the six alumni co-investigators/co-facilitators/co-authors as internal natural experts (Sandelowski, 1998) was used to help to achieve the required confirmation. Additionally, the study's strength includes the implementation of qualitative methodological procedures that ensured its rigor as reported in the Method section.
Conclusion
The unquestionable mobilization of students’ personal knowledge towards the critical exercises awoke their awareness to gaps in the nursing curriculum and the paucity of experiences in clinical placements concerning MHL. Like other low-, middle- and high-income countries, Canadian responsive nursing education to HL issues remains a barely addressed topic. This is a major recommendation for nursing research in the education realm. Within a HP perspective, HL and sex are complex SDH deserving more attention, with regard to social inclusiveness and social justice. MHL content is paramount for nursing curricula in all program levels and research initiatives.
Future nursing research should explore, within the diverse scope of ethno-cultural dimensions of men as individual and collective entities, how they express, practice and what they believe about their own health and HL. Another relevant topic to advance nursing knowledge on men's HL is to explore how updated and developed the nursing workforce is to effectively respond to current, global interventions for enhancing community HL. This includes the investigation of health care organizations’ readiness to respond to HL as well as the use of nursing researchers to redesign the nursing scientific contribution to this global health promotion action.
Footnotes
Acknowledgements
To the former undergraduate nursing students, Sabaa Samuel, Farha Patel and Betty Wang for their inestimable contributions to the workshop implementation, and Shahilaa Devaraja for the literature review support. To Sam Shelstad for the manuscript technical editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ryerson University- Faculty of Community Services, (grant number 2022- Winter Writing Week).