
Abstract
The wealth of personal information recorded in the admissions books of Greenwich Hospital offers one of the most detailed portraits available of Britain's essential naval workforce. This article uses a quinquennial sample of the men admitted to Greenwich Hospital between 1764 and 1864 to reconstruct the evolving composition of the Greenwich pensioners across this pivotal period of British naval ascendancy. Over this time, the prevailing features of the different cohorts of pensioners varied significantly, with differences between years of peace and war a driving factor. The characteristics of the admitted pensioners reflected the shifting fortunes and challenges encountered by the Royal Navy, and thereby offer a new perspective on important debates, such as the naval manning problem and the overall composition of naval manpower across this long period. The Greenwich Hospital population was far from static and its residents – experienced seamen – were among the decisive sinews of British power.
Keywords
Thrice honoured be his manes! Supremely blest, Who found for England's Tars a place of rest. This neuclus of their hopes, a rich award, From storm, from tempest free, here snugly moor’d A haven for the guardians of our coast. A nation's gratitude long be our boast This noble pile let foreign powers behold And hear the tale its annals will unfold When dire privation has its withering rage Exausted, and decrepitude and age Creeps o’er the frame; the hardy tar will veer And shape his future course for Greenwich Tier
1
In these few lines of poetry, George Hewens, a Greenwich pensioner, 2 conjures up the multiple different functions of the Royal Hospital for Seamen at Greenwich. This was not a hospital in the modern sense of a place to heal the sick, but a vast almshouse – a retirement home for men who had served in the Royal Navy. There, the ‘guardians’ of Britain's security and wealth could find their ‘haven’ and live out their days ‘snugly moored’ and free from poverty. At the same time, Greenwich Hospital was a powerful and multifaceted statement. With its palatial buildings and symbolic location on the banks of the Thames, this ‘stately pile’ represented an unambiguous assertion of British maritime hegemony to ‘foreign powers’. For the British public, the institution communicated the beneficence of an enlightened state – ‘a nation's gratitude’ to its loyal servants expressed in bricks and mortar. As Hewens suggests, this was also a place of ‘tales’ and ‘annals’, where the old sailors provided a living link to past naval victories and seemed to hold out the promise of future glories.
Designed by the greatest architects of the day, including Christopher Wren, John Vanbrugh and Nicholas Hawksmoor, Greenwich Hospital was intended to show that Protestant Britain, with its ‘balanced constitution’ of monarch and parliament, could match the wealth, power and munificence of Louis XIV's absolutist France. In particular, the Sun King's foundation for wounded soldiers, the Hôtel des Invalides in Paris, served as a rival model for Greenwich and earlier soldiers’ hospitals at Chelsea and Kilmainham in Dublin. 3 The grandeur of Greenwich Hospital represented a strong assertion of Britain's naval exceptionalism and a clear recognition that the nation's fate was tied to the sea. Some of the imagery was less than subtle, and the centrepiece of the magnificent Painted Hall's ceiling shows King William III and Queen Mary crushing Louis XIV of France and his aspirations of universal monarchy underfoot.
The Greenwich pensioners held a curious and contradictory identity. Dependent on state charity, these men were effectively paupers, but they lived among princely splendour. 4 They were naval veterans and national heroes, 5 celebrated for their martial masculinity, but were frequently portrayed as amputees with broken bodies incapable of supporting themselves. 6 As such, the distinctive uniform of a Greenwich pensioner – a dark-blue coat and black cocked hat – was simultaneously both a stigma and a prestige symbol. 7 The Greenwich pensioners were lauded for embodying supposedly distinctly national virtues, yet the hospital's population was multinational and multi-ethnic, reflecting the full reach of Britain's global maritime interests. These men were the subject of enduring curiosity in British society, but they have been little studied. This omission is especially surprising as the level of personal detail provided by the three sets of Greenwich Hospital admissions records makes the resident Greenwich pensioners some of the best-documented members of Britain's essential maritime labour force. 8
Greenwich Hospital has been the subject of several histories, such as the work of Philip Newell, Pieter van der Merwe and C. M. Dawson, 9 but these are narrowly institutional in scope and reveal little about the thousands of men who called that organization home. 10 So far, the only work to use a quantitative approach to identify the contours and composition of the Greenwich Hospital population has been Martin Wilcox's study of resident Greenwich pensioners between 1705 and 1763. 11
Wilcox compiled a database on the 8,112 pensioners admitted to Greenwich Hospital between 1705 and 1763, using information from two sets of admissions books. Of these, comprehensive biographical information was available for the 3,316 men admitted after 1749. 12 The cut-off point of 1763 was chosen because it marked a caesura in Greenwich's operation, as demobilization at the end of the Seven Years War brought significant expansion. 13 Crucially, until 1763, all Greenwich pensioners had been resident in the hospital buildings. The introduction that year of ‘out-pensions’, whereby men continued to live in their own home community and received a regular cash pension, created a distinction between these new ‘out-pensioners’ and the resident ‘in-pensioners’. As with Wilcox's article, the ‘in-pensioners’ are the focus here.
Wilcox provided an unrivalled portrait of the Greenwich Hospital population in its first six decades. This also represented an unusually detailed profile of Britain's vast maritime labour force, of which the Greenwich pensioners were a small but significant sample. He concluded that a typical Greenwich pensioner likely ‘came from a poor background’, often from the coastal counties of England, the city of London or the Celtic fringe; generally went to sea at a young age; was ‘at considerable risk of injury and disablement’; and was ‘more likely than average to be unmarried and childless’ at the end of his career. 14 Wilcox's work broke new ground in using the empirical statistical features of the Greenwich Hospital population to move beyond previously impressionistic perceptions of the men who manned Britain's warships. However, because extensive biographical details were only available for the last 15 years of Wilcox's sample, his was necessarily a snapshot view of the Greenwich pensioners and Britain's seagoing workforce, and could not assess how these pivotal populations changed over time.
This article builds on Wilcox's work in order to address the question of change over time. It is argued that the men admitted to Greenwich Hospital varied considerably between 1764 and 1864, and that this variation was especially pronounced between years of war and years of peace. The successive conflicts, chiefly between Britain and France, which comprised what Anthony Page has called the ‘Seventy Years War’ (1744–1815), 15 find clear reflection in the attributes of the men admitted as Greenwich pensioners. In turn, this sheds new light on long-running debates in maritime history, including the composition of Royal Navy manpower during the Age of Sail and the perennial naval manning problem.
Greenwich Hospital offers a uniquely detailed insight into the lives of an important subset of Britain's naval manpower from the perspective of the end of their career. As such, this case study is able to capture a more summative view of the experiences of these men than comparable sources, such as ships’ muster books. Between 1705 and 1869, approximately 35,000 men were admitted to Greenwich Hospital as resident in-pensioners. 16 For the vast majority, a wealth of personal data survives, with categories including age, birthplace, last place of residence, length of naval service, height, occupational background, marital status, number of children, and details of wounds and illnesses suffered during or due to naval service. These sources also record the date and manner of discharge until 1844. 17 Other information can be calculated, including the tenure of residence and approximate birth year.
Greenwich Hospital required detailed information on its residents, and so the admissions records are well suited to this article's objective of charting the changing contours of that population. For example, the age and wound profile of the pensioners would affect care requirements; details of long naval service or wounds were recorded to justify a man's admission; and information on birthplace, family and residence allowed coordination with local authorities about welfare responsibilities and, coupled with details of physical appearance, could also be useful in cases where men ‘deserted’ from the hospital. It is striking that the hospital records mark these men with an ‘R’ for ‘Run’, exactly like in naval muster books to designate men who absconded from active service. 18 The population of resident pensioners was not intended to be representative of naval manpower as a whole, and Greenwich Hospital's entry criteria favoured long service, which makes the sample especially revealing when it comes to career sailors. At the same time, however, illnesses, accidents or wounds inflicted by the enemy could affect anyone. Therefore, while the sample is skewed towards more experienced sailors, practically the full range of lower-deck society is represented. 19
The period covered by the Greenwich Hospital admissions books (1705–1865) and this article (1764–1869) encompasses an era of astonishing upheaval, including the ‘classical’ era of the Industrial Revolution and the socio-economic dislocations that this entailed. 20 Critically for the Greenwich pensioners, these years witnessed the climax of the global conflicts between Britain and France and the twilight years of the generation of men who served during the French Revolutionary and Napoleonic Wars. It was also within this period that Britain's welfare system was overhauled, with the Old Poor Law, characterized by parish-based ‘outdoor relief’, increasingly replaced by ‘indoor relief’ centred on the workhouse. 21 The reforms of 1834 were traditionally viewed as the key pivot point in this process, although any impression of a rapid or universal shift in practice has been challenged from multiple angles. 22 As such, Greenwich Hospital’s admissions records have the potential to contribute to a range of wider debates, including the underlying purposes of eighteenth-century charity, the nature and impact of welfare reforms centred on the New Poor Law of 1834, and the use of height data as a proxy for standards of living during the Industrial Revolution.
This article is more limited in scope and is intended to demonstrate that the Greenwich Hospital population was not static or unchanging but, on the contrary, mirrored the needs and fortunes of the Royal Navy and the challenges that it faced. Consequently, the focus here is on those fields of data that exhibited the greatest variation over time, including age at admission, tenure of residence, place of origin and wound profile. Its findings rest on a database containing the complete information provided by the three sets of admissions books on all men admitted as Greenwich in-pensioners in every fifth year from 1764 to 1864. This has resulted in a total sample of 6,045 admissions, including readmissions, although some categories of information are only available until 1844 or 1859 due to changes in how the admissions books were compiled. Although Greenwich Hospital closed in 1869, the final admissions were in 1865, and these were only half as numerous as in 1864. Consequently, although this sample ends in 1864, it captures the make-up of the population until the hospital's closure in 1869. As a quinquennial sample, the results of this study are preliminary. Nevertheless, the current data set offers a sufficiently robust basis for initial analysis due to its large sample size, even distribution of sample years, and inclusion of years of peace, war, mobilization and demobilization. The remainder of this article presents the results of this analysis and applies them to ongoing debates in maritime history regarding workforce composition and the naval manning problem.
Admissions Trends
Before turning to the successive fields of data, it is important to recognize that the number of men admitted to Greenwich Hospital each year was itself subject to broad variation. Years of war, and particularly demobilization, came to stand out clearly from years of peace, but the strength of this contrast developed in tandem with the growing intensity of warfare across this period. Linda Colley has argued that the expanding scale of late eighteenth-century warfare led states to make ever-increasing demands on their population for manpower and resources, while granting constitutional concessions in return. 23 This article suggests that military welfare provision was also required to expand and adapt to reflect the greater number of men eligible for such support.
As Figure 1 demonstrates, admissions to Greenwich Hospital proceeded at a steady rate throughout the second half of the eighteenth century. Demobilization after the American War of Independence was mostly completed in 1783, so the figures for 1784 register only a modest increase in admissions, likely representing the tail end of the demobilization process. Periods of mobilization are associated with lower rates of admission, and so Britain's entry into the French Revolutionary War in February 1793 had little immediate effect on admissions in 1794, while remobilization after the short Peace of Amiens (March 1802 to May 1803) resulted in a strikingly low number of admissions in 1804 compared to the surrounding years of war. A peak associated with demobilization is observed for 1814, as the Royal Navy contracted following the first defeat and exile of Napoleon. 24
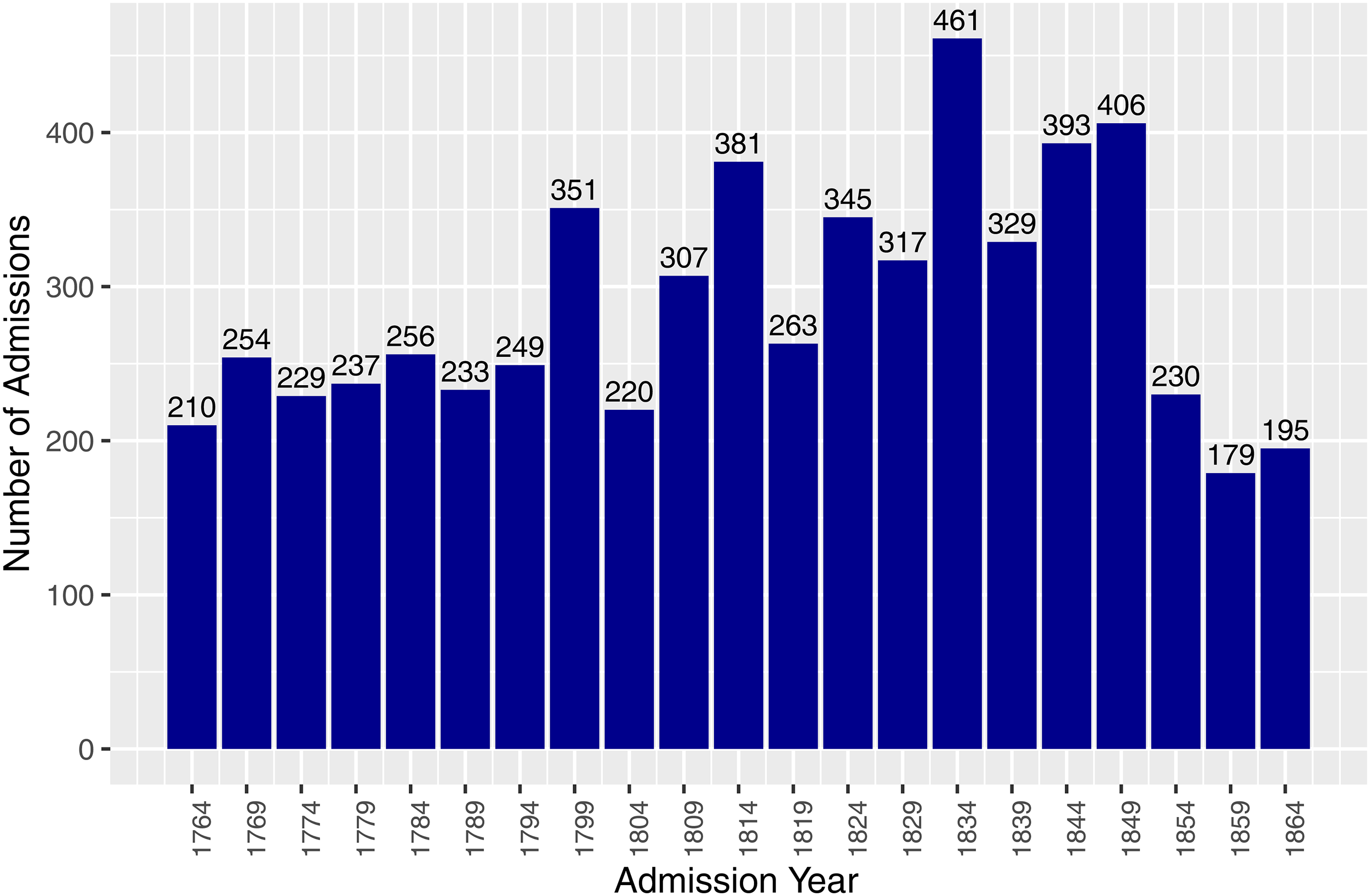
Quinquennial admissions to Greenwich Hospital, 1764–1864.
From 1824 to 1849, the number of admitted men fluctuated but remained high by earlier standards, corresponding to the autumn years of the vast pool of naval manpower from the wars of 1793–1815. Due to the central position that the reforms of 1834 have traditionally occupied in British welfare history, 25 it is curious to note that this was the sample year with the highest number of admissions. The hypothesis might be that the increasing severity of the civil poor relief and the spectre of the workhouses (‘Poor Law Bastilles’) made entry into Greenwich Hospital a more attractive prospect, 26 but this requires further enquiry. The total population of resident Greenwich pensioners between 1705 and 1869 did not grow evenly but in a set of successive jumps as new blocks and wards were completed, and peaked at circa 2,700 in the years immediately following the Napoleonic Wars. 27
The observed pattern of admissions appears well attuned to both the individual needs of the sailors and the institutional interests of the Royal Navy. The comparatively small number of admissions during years of mobilization corresponds to the period of greatest demand for sailors during the initial rush to man the fleet as ships were commissioned from reserve, when large bounties were paid to men joining the navy. 28 Increased numbers of men were admitted in wartime, likely reflecting the larger size of the active navy and the higher instance of injuries. It was in wartime that Greenwich Hospital's function as an indirect incentive to naval recruitment was most important, encouraging the young to serve, in the confidence that they would be cared for if wounded. 29 High numbers of admissions during years of demobilization align with Evan Wilson's recent work on the hardships that peace brought to soldiers and sailors, with the marketable skills of seamen not fully protecting them from the sudden competition for employment. 30
These admissions practices also complemented trends in Greenwich Hospital's income, which was higher in wartime than in peacetime. The hospital received sixpence per month deducted from the wages of every sailor in the Royal Navy and merchant fleet. 31 This scheme resembles a form of proto-National Insurance, demonstrating one respect in which Greenwich Hospital can be considered a pioneer of welfare policy. 32 Wartime swelled the number of Royal Navy sailors while the merchant fleet did its best to maintain its scale of operations. 33 Ultimately, more seamen translated into more sixpences. Furthermore, while payments from merchant sailors were gathered through paid assessors in the major ports, with one-third of this income sometimes swallowed up by collection costs, naval sixpences were paid directly by the Admiralty based on the number of naval personnel on its books. 34 In 1707, Greenwich Hospital was granted all unclaimed and forfeited naval prize money and, in 1806, an additional five-per-cent share of all naval prize money – a valuable revenue stream in wartime but negligible in peacetime. 35 Consequently, unlike most welfare organizations in Britain, Greenwich Hospital found wartime more lucrative than peacetime.
Just as cycles of war and peace exerted a strong influence on the number of pensioners admitted to Greenwich Hospital each year, they also affected the average age of the admission cohorts, with knock-on ramifications for the average length of naval service and average tenure of residence at the hospital. As shown in Table 1, the general trend was an increasing age at admission, and this is especially evident in the decades after the end of the Napoleonic Wars. The exception is a reduction in average age at admission during war years, most clearly observable for 1799 and 1809. These years saw the highest proportion of admitted men aged 30 or younger, at 13.7% and 14.3%, respectively. 36 A similar but smaller dip in average age at admission is also observable during and just after the American War of Independence (1779 and 1784). These declines likely reflect younger men falling victim to illness or injury during wartime and being admitted to Greenwich Hospital straight from naval service.
Mean age of men admitted to Greenwich Hospital (rounded to the nearest integer).
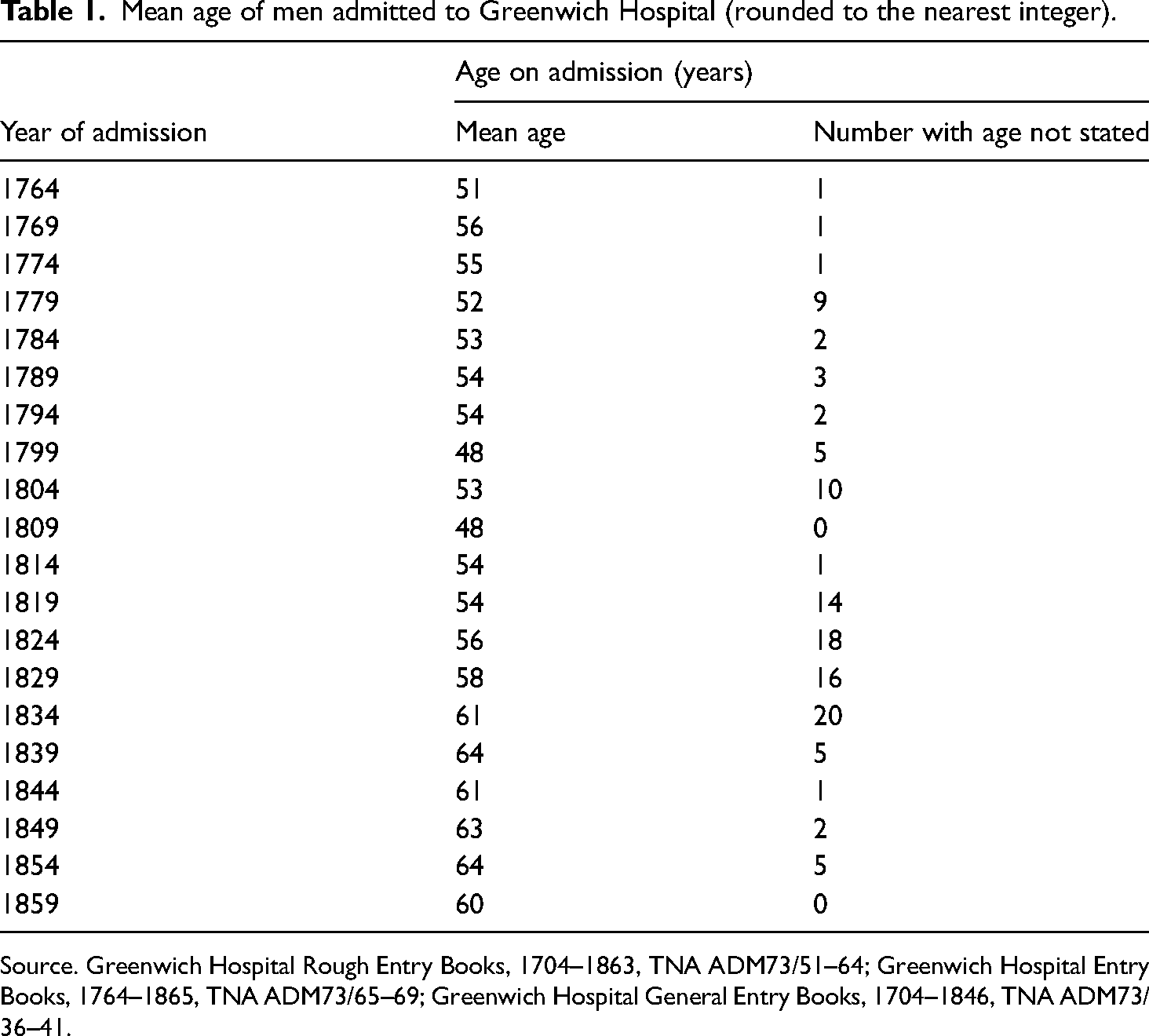
Source. Greenwich Hospital Rough Entry Books, 1704–1863, TNA ADM73/51–64; Greenwich Hospital Entry Books, 1764–1865, TNA ADM73/65–69; Greenwich Hospital General Entry Books, 1704–1846, TNA ADM73/36–41.
Contrastingly, the long period of relative peace after the final defeat of Napoleon in 1815 resulted in an increasing average age at admission, and the mean age of men admitted in 1844 was nine and a half years older than in 1764. Unsurprisingly, as shown in Figure 2, when the average age at admission increased, the mean tenure of residence fell, as older entrants had fewer years left to live. Consequently, the mean tenure of residence in 1844 was close to half that of 1764. 37
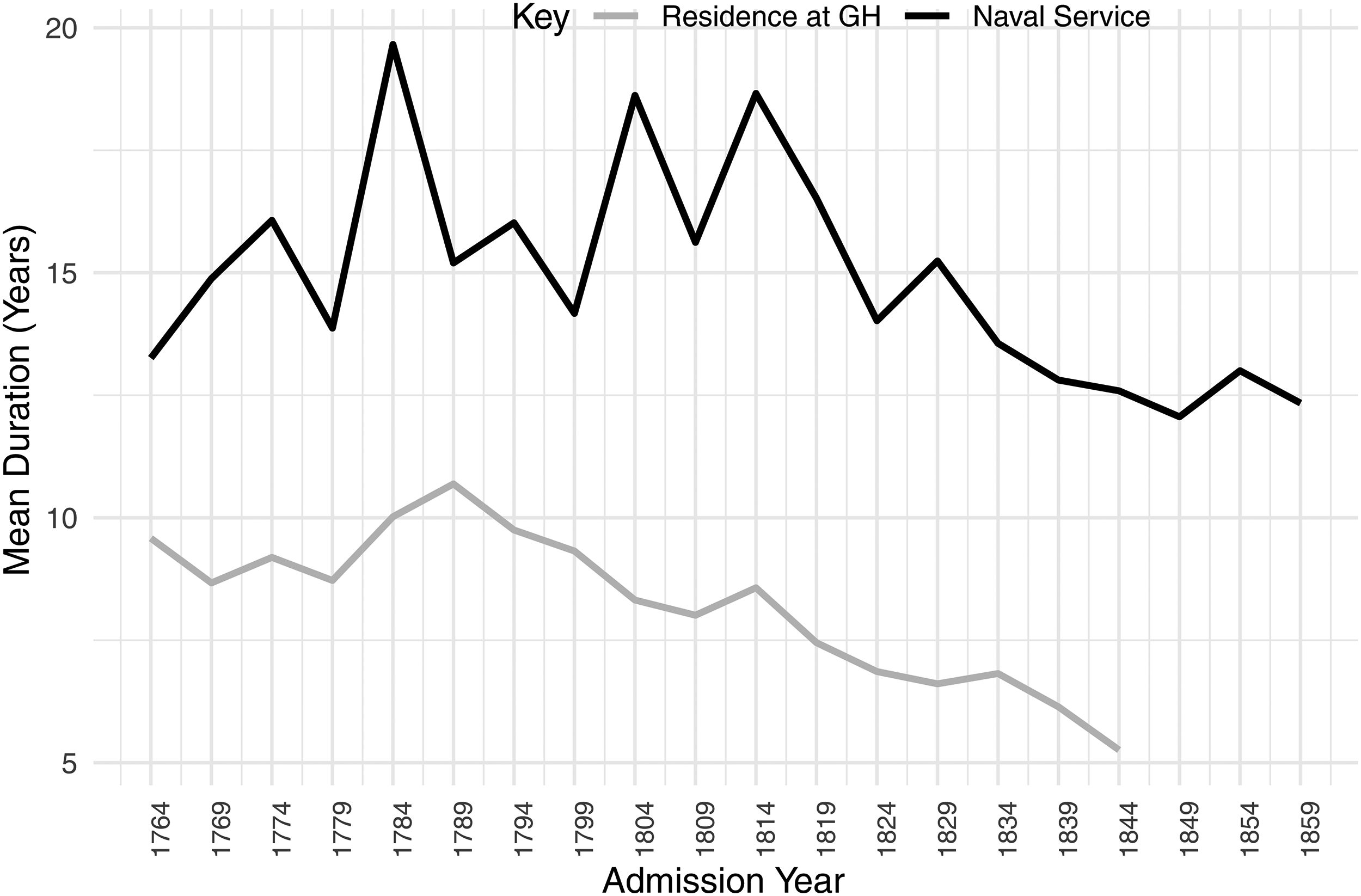
Mean duration of residence and length of naval service of men admitted to Greenwich Hospital (rounded to the nearest integer).
This ageing population helps to reconcile a surprising feature about the admissions rates shown in Figure 1. In 1860, a Parliamentary Commission reported that there was insufficient demand for residential places at Greenwich Hospital and that the institution was unsustainable. 38 It was understood that the number of occupants had been declining for some time: vacancies had increased from 3 in January 1849 to 835 by January 1857, and continued to grow. By the start of February 1860, there were 1,124 unoccupied places. 39 No further admissions to Greenwich Hospital were allowed after 1865 and all remaining residents were required to leave in 1869. The report identified a number of convergent causes for the declining demand for admissions, including ‘the gradual removal, by death, of the survivors of the last war; the long subsequent peace; the decreased naval armament since 1815’; strong demand for sailors in the merchant service; higher pay provided by foreign English-speaking navies; and the attractiveness of emigration to Britain's settler colonies. A final suggested cause was the extended eligibility and improved rates of out-pension offered, implying that this was increasingly preferred to residential in-pensions. 40
Figure 1 shows that the decline in admissions occurred surprisingly late (between 1849 and 1854), and that the number of entrants to Greenwich Hospital even then continued at a similar rate to that seen across the second half of the eighteenth century. This would appear to raise questions about why this reduced rate of admission was considered a threat to the future of Greenwich Hospital in the 1850s and 1860s, but not a century earlier. However, the increased average age at admission helps to reconcile this quandary because, even though large numbers of men continued to be admitted, they were older and so the duration of their stay was shorter, resulting in a higher turnover of residents and increasing vacancies.
Unlike the previous two measures, Figure 2 shows that the average length of naval service for men admitted to Greenwich Hospital did not display a changing overall trend: the average period of service in 1859 was little different to that of 1764. That being said, this measure was subject to significant fluctuation within this long period, driven largely by war and peace. On the whole, the average length of naval service of admitted men was lower in years of war (for example, 1779, 1799 and 1809), which, in conjunction with the lower average age on admission for these years, likely reflects the admission of younger men with fewer years of service who had been injured during the current war.
Contrastingly, there were sharp peaks in the average length of service for men admitted during periods of demobilization (1784, 1804, 1814 and 1819). This suggests that some of the most experienced naval sailors took the opportunity afforded by the return of peace to bring their sailing career to an end, and that those with long service were seen as especially deserving of admission. In the context of the intense competition for work on merchant ships at the end of a war, 41 it appears likely that the long-serving men admitted to Greenwich Hospital were at or beyond the threshold, where their experience ceased to be a competitive advantage for gaining employment and their age and infirmities counted to their detriment.
Two caveats are important here. First, several years of demobilization also have elevated numbers of men whose length of service is not stated (for example, 1784, 1814 and 1819). 42 The proportion of entrants with no stated length of service peaked at 31 per cent in 1819, compared to an average of just 8 per cent across the period from 1764 to 1859. 43 Second, the years 1804 and, to a lesser extent, 1814 can be considered years of both demobilization and remobilization due to the short duration of the Peace of Amiens and the surprise of Napoleon's Hundred Days campaign. 44 Nevertheless, these patterns reinforce the extent to which trends among the men admitted as Greenwich pensioners changed over time and the dominant role of cycles of war and peace in defining that process.
One limitation of the Greenwich Hospital admissions records is that they do not specify which, if any, wars a man served in. 45 This is less of a problem for the period between 1764 and 1815 because the repeated bouts of warfare and the hospital preference for men with long service meant that the vast majority would have seen wartime service, although not necessarily combat. For men admitted in the decades after 1815, however, it would be desirable to determine how many were veterans of the Great Wars up to 1815, and how many had served purely post 1815. It is possible to provide a tentative estimate on this matter by using the available data on year of admission, age at admission and length of naval service.
Looking specifically at the 2,315 men admitted in the years 1829, 1834, 1839, 1844, 1849, 1854 and 1859, these were divided into four categories. Those who would have been aged 25 or older in 1815, or whose total length of naval service was greater than the span of time between 1815 and the year of their admission, were recorded as ‘highly likely’ to have served in the Great Wars of 1793–1815. Those aged 16 to 24 in 1815 were designated ‘possible’ veterans of those conflicts, while anyone younger than 16 in 1815 was listed as ‘highly unlikely’. Finally, the two per cent of men whose age was not recorded on admission formed an ‘insufficient data’ category. While the findings of this exercise are tentative, it is hoped that they will serve as a starting point for future study. Under these criteria, the proportion of men ‘highly likely’ to have served during the wars prior to 1815 remains remarkably high for decades: over 90 per cent in 1829, 1834 and 1839; 83 per cent in 1844; and 76 per cent in 1849. Thereafter, there is a sharp decline to 57 per cent in 1854 and then 31 per cent in 1859. The ‘possible’ category grows slowly from a negligible 2 per cent up until 1839 to peak at 27 per cent in 1859, while the ‘highly unlikely’ category does not reach 10 per cent until 1849 but then increases rapidly to reach 42 per cent in 1859. 46 This demonstrates the numerical dominance of veterans of the French Revolutionary and Napoleonic Wars among resident Greenwich pensioners, and the gradual disappearance of that generation was central to the decline and eventual closure of Greenwich Hospital.
Place of Origin
The Greenwich pensioners who make up the sample of 6,045 men admitted between 1764 and 1864 were a diverse group from over 40 modern countries and territories, but there are evident patterns in the rates of admission. 47 As shown in Table 2, between 1764 and 1859, at least 60 per cent of the admissions in the sample were English. 48 If admissions with no identifiable place of birth are excluded from the calculation, the proportion of English admissions rises to 66 per cent across the period. 49 By either measure, it was rare for English-born men to comprise less than half of the admissions. Again, it is years of warfare and demobilization that stand out, this time for their lower proportion of English admissions. After 1819, the English majority became even more pronounced. The Irish were almost always the second most-represented group, followed by the Scottish. These, as well as the Welsh and foreign-born men, were most clearly in evidence during years of wartime and demobilization.
Birthplace of admissions to Greenwich Hospital, 1764–1859 (5,850 observations as place of birth not recorded for 195 men admitted in 1864).
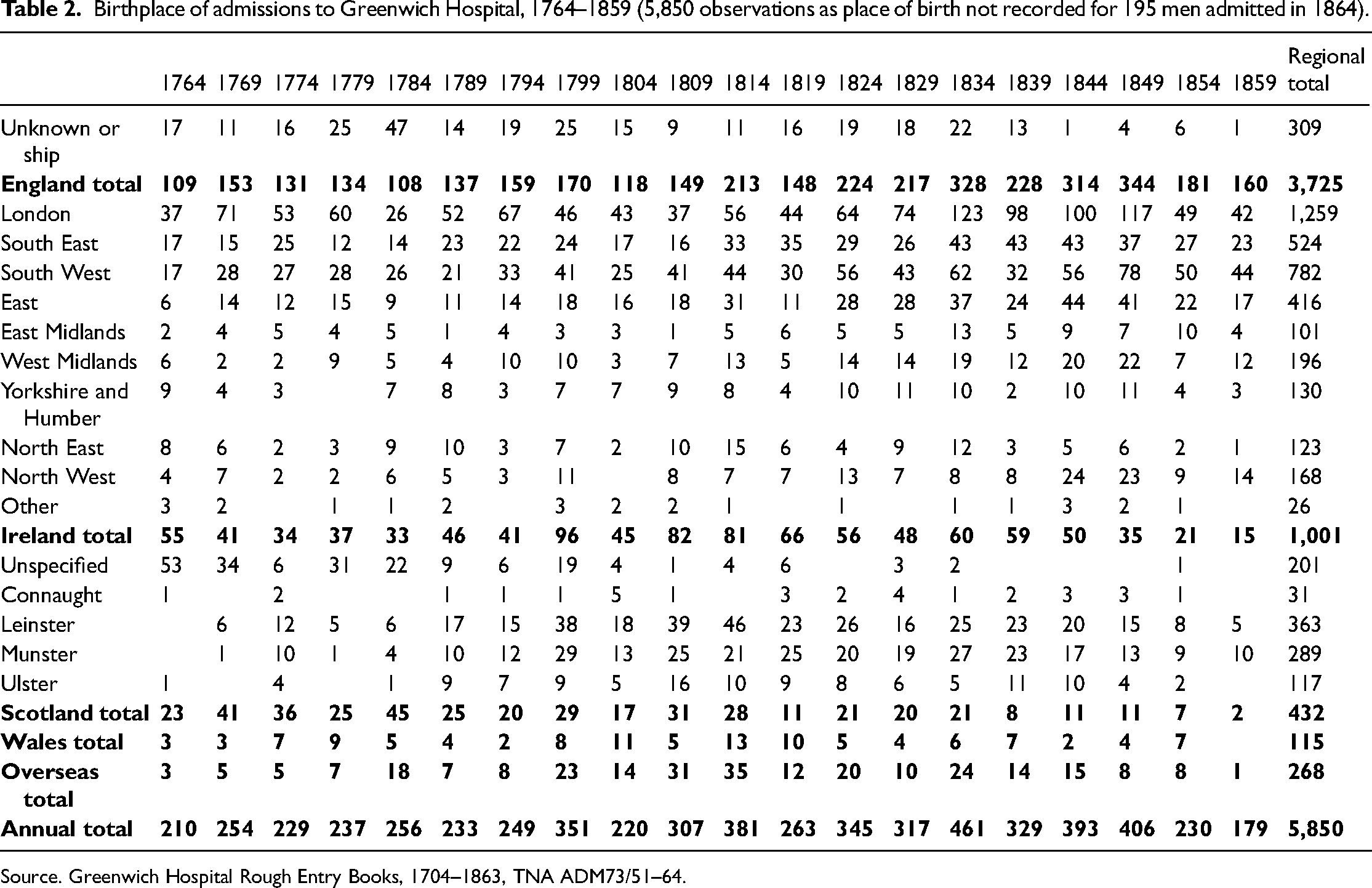
Source. Greenwich Hospital Rough Entry Books, 1704–1863, TNA ADM73/51–64.
The reason for this pattern is not clear. One possibility would be that the peacetime navy had a higher proportion of Englishmen and that manpower from Scotland, Ireland and Wales was increasingly called on during wartime. This might conform to the perennial problem of wartime naval manning, 50 but does not seem overly convincing. Another possibility would be that men from Wales, Scotland and Ireland were more likely to apply for admission during periods of wartime and demobilization because that was when they would be more likely to be located closer to London (with the naval establishment based in Plymouth, Portsmouth and Chatham), and so better positioned to apply for admission, which had to be done in person at the Admiralty in London.
Whereas recent studies of the naval manning problem have paid significant attention to the national identity of Royal Navy sailors, 51 the Greenwich Hospital data also facilitates analysis of regional identity. Among the Englishmen, London was nearly always the modal place of birth, with the French Revolutionary and Napoleonic Wars (1799, 1809 and 1814) marking one nadir of this dominance and a second, more surprising, dip at the end of this period (1854 and 1859). Unsurprisingly, the traditionally maritime South West of England ranks comfortably second among English birth regions, with South East and East England also prominent. Contrastingly, the North East and Yorkshire and Humber regions were the origin of shockingly few of the Greenwich pensioners in this sample, considering their centrality to the coastal coal trade and fishing fleets, both conventionally viewed as ‘nurseries for seamen’. 52 One possible explanation for the comparative lack of men from these regions would be that the economic opportunities associated with rapid industrialization in these areas made it easier for even the elderly or infirm to find employment and earn their own subsistence through labour. In her studies of ageing in eighteenth-century England, Susannah Ottaway found that the elderly ‘in the north were less likely to turn to the Old Poor Law (and received less support from it when they did)’ because the greater availability of casual employment in industrializing northern regions enabled ‘the old in the north to help themselves’. 53
For Ireland, Leinster (particularly Dublin) and Munster (especially County Cork) are most prominent, although many entrants were recorded simply as ‘Irish’. Connaught and the west of Ireland are conspicuous by their relative absence. Scotland suffers a similar problem, with place of birth often recorded merely as ‘Scotland’ or ‘North Britain’, but the modal regions of Central and South East Scotland correlate well with population distribution, although the Shetland and Orkney Isles are disproportionately well represented. 54 Of those specified, South Wales provided more than twice as many Greenwich pensioners as North Wales, although this, too, likely reflects population levels. 55 Noted surprises aside, most of these findings tally well with previous estimates. 56
Table 3 shows the fluctuating proportion of foreign-born admissions to Greenwich Hospital. The second column gives foreign-born men as a percentage of the total admissions in that year, which represents a reliable minimum value. The third column shows the foreign-born proportion only of those admissions where a birthplace was reported. For the purposes of this study, ‘foreign-born’ is defined as anyone who was not born in England, Scotland, Wales, Ireland, the Channel Islands, Isle of Man, the Shetlands, the Orkneys or the Hebrides. As such, some of these men would have been British subjects by birth – those born in Gibraltar, Jamaica and Canada, for example. Others would have become naturalized subjects due to the length of their service in the Royal Navy. 57
Proportion of admissions to Greenwich Hospital who were foreign-born, 1764–1859.
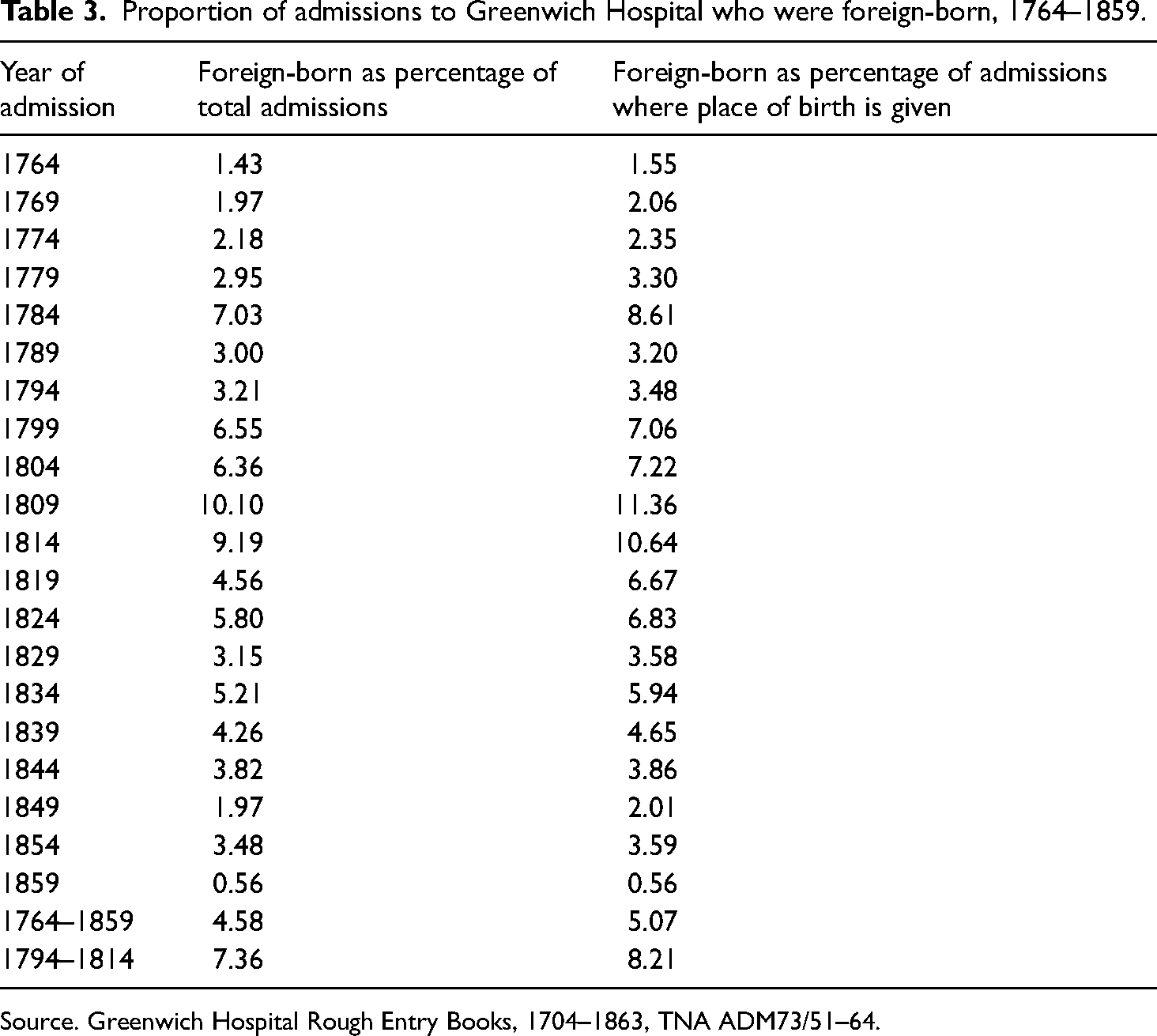
Source. Greenwich Hospital Rough Entry Books, 1704–1863, TNA ADM73/51–64.
Sara Caputo has outlined many of the problems that face historians using British naval documents of this period to identify foreign seamen. Notably, these record birthplace (usually parish and county) rather than nationality. The details of foreign-born men did not fit this template and their self-identification might anyway be mistaken, simplified or generalized by the clerk, as was perhaps the case for the four men in this sample whose birthplace was recorded only as ‘Africa’. ‘Birthplace’ was not necessarily the same as legal or cultural identity, while this period also saw frequent changes to territorial control, as in the case of many Caribbean islands and the partitions of Poland, so the jurisdiction at time of birth might have been different by the time of entry to Greenwich Hospital. 58
In Table 3, the highest proportion of foreign-born admissions occurred during wartime and around demobilization – for example, 1784 and 1799–1814. Whereas foreign-born men comprised approximately five per cent of total admissions between 1764 and 1859, their proportion during the period of the French Revolutionary and Napoleonic Wars was circa seven to eight per cent. This figure matches Jeremiah Dancy's estimate of the proportion of foreign-born sailors among Royal Navy crews during the French Revolutionary Wars and also corresponds to the lower end of Caputo's estimate for the period 1793–1815. Both of these studies were based on quantitative analysis of ships’ muster books. Dancy's sample was drawn from ships serving in British home waters, while Caputo's came from ships on the most distant naval stations, so it is unsurprising that the figures for foreign-born Greenwich pensioners tally with the lower bound of her estimate. 59
This would suggest that the proportion of foreign-born men admitted to Greenwich Hospital roughly kept pace with the ratio of foreigners serving in the navy at that time. This is itself surprising as, even in wartime, one would expect an appreciable, though indeterminate, time delay between service and admission. Intriguingly, a final wartime peak at 3.5% of admissions recording a foreign birthplace in 1854 coincides with the Crimean War and matches almost exactly Caputo's findings on the proportion of foreign-born sailors in the British Baltic Fleet during that conflict. 60
The average age and length of naval service reported by the foreign-born Greenwich pensioners was practically identical to that of the rest of the pensioners, further suggesting that they were admitted on equal terms. The mean age of foreign-born men on admission was 55, compared to 56 both for the entire sample of admissions and for those specifically who reported a non-foreign birthplace. For length of naval service, the mean reported by foreign-born men was 14 years, compared to 15 for the entire sample of admissions and for British and Irishmen. 61 Nor were foreign-born Greenwich pensioners more likely to report a wound than their native-born peers. 62 In summation, foreign-born men were admitted as resident Greenwich pensioners at a rate and on terms that reflected both their proportion of Royal Navy manpower and the service history of native-born admissions.
The sample contains a total of 268 admissions with a foreign birthplace. Of these, 16 were born in Africa and 114 in the Americas (67 from the Thirteen Colonies/United States, 11 from Canada, 2 unspecified and the remaining 34 from the Caribbean). There were 9 men born in Asia, with 6 of them from India. Of the 129 men born in Europe, the main contributing regions were Germany (40), Sweden (22), the Netherlands (15) and Italy (8). As a proportion of foreign-born pensioners in the sample, Europe accounted for 48 per cent, the Americas 43 per cent and the other regions 9 per cent. It has been shown that the admission of foreign-born men was highest in wartime years, but the regions that contributed the most pensioners (such as the United States, Germany, Sweden and the Netherlands) were present among almost all admission cohorts, albeit in smaller numbers in peacetime years. For other regions, there was a marked cluster of admissions towards the end of the time frame, as, for example, with Poland and Canada. 63 Only 2 of the 16 men born in Africa were admitted before 1804 and only 5 before 1829. 64
With over 40 modern countries and territories represented, the geographical variety of birthplace is striking, as is the continued admission of men in years when their country of birth was at war with Britain, as with men from the United States, the Netherlands, Denmark and France for specific years between 1794 and 1814. The number of Greenwich pensioners born in Portugal (6) is perhaps oddly low for a famous seafaring country and Britain's oldest ally, whereas the small number of men from India (6) is also surprising, considering the large literature on lascar sailors living in Britain, although lascar service was usually concentrated in the Indian Ocean. 65
The presence of so many foreign-born Greenwich pensioners would seem to contrast with the form of overt, theatrical patriotism communicated, for example, by the ceiling of the Painted Hall and many of the artistic representations of Greenwich Hospital. 66 From this wide diversity, it might tentatively be suggested that Greenwich Hospital took a more contractual approach to matters of belonging and entitlement. Through serving in the Royal Navy, men automatically contributed to the income of Greenwich Hospital through compulsory monthly wage deductions, regardless of where they happened to have been born. As such, it would have been difficult to deny their reciprocal right to support from the hospital, including admission. For foreign-born Greenwich pensioners, their service in the ranks of the Jack Tars could effectively constitute an honorary or earned Britishness, whether or not they had formerly become British subjects. In the context of the perennial wartime naval manning problem, the navy benefited from this pragmatic approach. 67 This pliability of identity among seafarers is comparable to the transient, liminal space occupied by American sailors during the early decades of the United States’ independence, identified by Nathan Perl-Rosenthal, where social status, occupation and individual skill could mean more than subjective ideas of nationality. 68
Wound Profile
Turning to the wound profile of the admission cohorts, this also displayed considerable variation between years of war and peace, as shown in Table 4. Understandably, the proportion of admissions with wounds was significantly higher during wartime. As observed in Wilcox's study, wounds to limbs were especially frequent, 69 but sensory wounds like loss or impairment of sight or hearing also stand out. The ‘other wounds’ category is large and varied, but mostly consists of injuries to hands and feet without loss of digits, skull fractures and ruptures. Men admitted with less than five years of naval service were much more likely to report a wound – 80 per cent compared to an overall average of 48 per cent – so it is clear that length of service and injuries were both pivotal criteria in admission decisions. 70
Wound profile of admissions to Greenwich Hospital, 1764–1859 (percentage of men admitted each year).
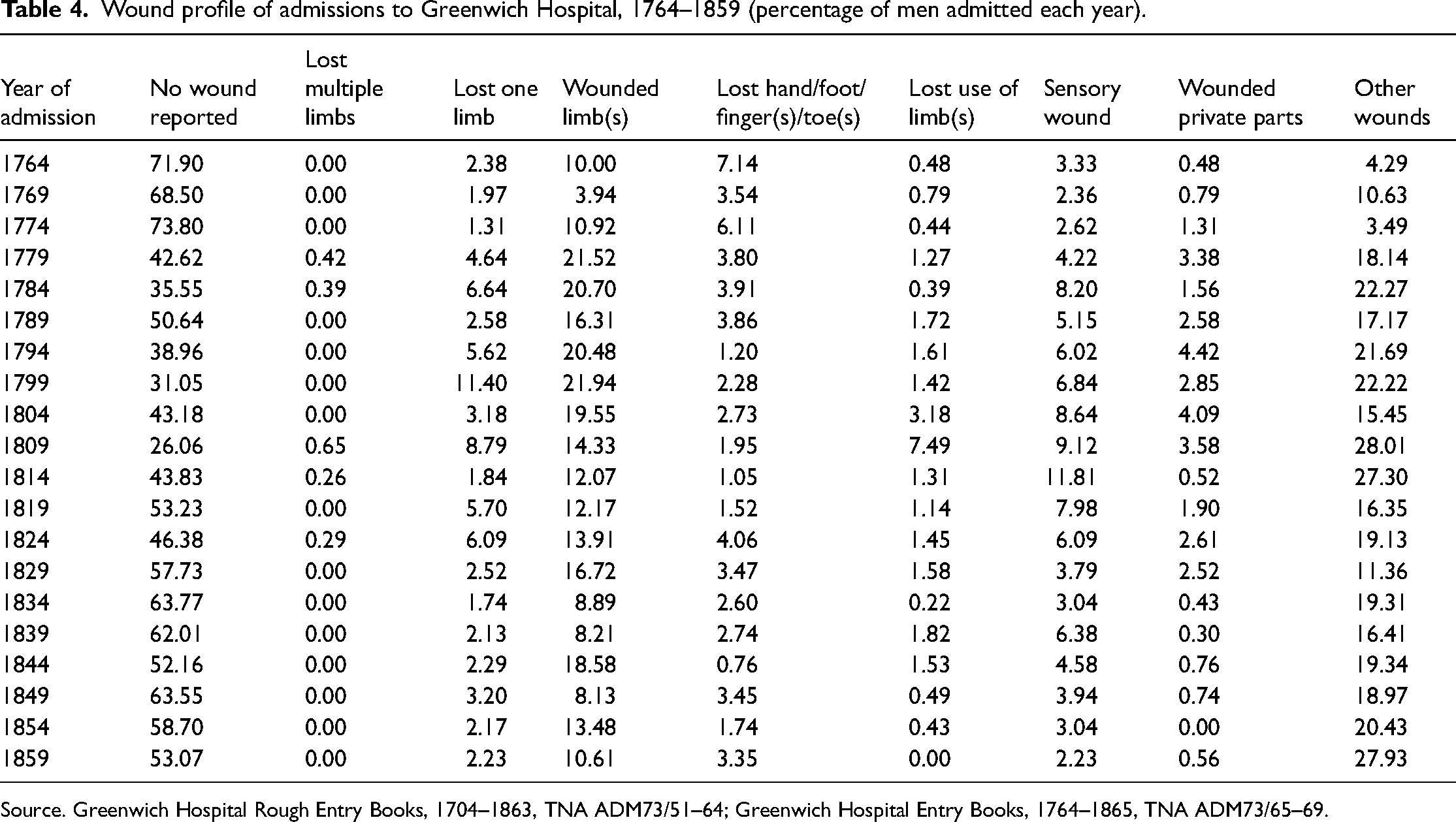
Source. Greenwich Hospital Rough Entry Books, 1704–1863, TNA ADM73/51–64; Greenwich Hospital Entry Books, 1764–1865, TNA ADM73/65–69.
Unsurprisingly, the proportion of admissions reporting no wound was smallest in mid-war years (1799 and 1809), whereas these same years saw the highest proportion of admissions who had lost a limb. The wounded-limb category shows a remarkably consistent wartime rate of circa one-fifth of admissions during the American War of Independence, French Revolutionary Wars and Napoleonic Wars (1779, 1784, 1794, 1799 and 1804), but is significantly lower in 1809 and 1814. In the case of 1809, the lower instance of wounded limbs is more than compensated for by a sharp spike in those reporting the loss of the use of a limb. In contrast to the more visceral wounds, peaks in the proportion of admissions reporting sensory wounds occurred in the years around demobilization, such as 1784 and 1814, and were likely linked to the older average age of the men admitted in those years.
There was a sharp increase in the proportion of admissions reporting a wound between 1774 and 1779, and it appears that this was due to a change in how that information was compiled. Up to 1774, recorded wounds were either permanent or current at the time of admission. By 1779 and thereafter, any wound suffered during naval service (and sometimes afterwards) was recorded. For example, many temporary wounds, such as a broken arm, were reported as having taken place on ships that were not the last vessel on which the individual had served. As such, these must have been historical wounds, which would presumably have healed by the time of admission. The most extreme case was William Stocker, admitted on 20 June 1834, whose entry in the wounds column reads ‘Struck by lightning’. 71 It seems safe to assume that this did not take place that day on his way to be assessed for admission, but related to a traumatic occurrence during his naval career. Other entries make clear that wounds were suffered ‘in the packet service’, ‘while a prisoner in France’ or in the ‘merchant service’, or that an amputation took place ‘a month after his admission’. 72
Mental health is difficult to assess from these sources, but some elements were recorded. Six men were reported to be ‘insane’, while a further four were discharged to asylums, including the famous Bethlem Hospital. In some cases, euphemisms make it hard to interpret individual circumstances. For example, 48-year-old James Topham was described as ‘quite childish and unable to give any account of himself’, while George Davey was said to be suffering from ‘Melancholia’. Thirty men admitted in 1814 were all described simply as ‘worn out’. 73 Occasional details recording premature deaths, including a small number of murders and others that could have been suicide, might also relate to mental health problems. As one example, Michael Carnady was reportedly ‘Killed by a fall from a Window in King William Square’ on 17 July 1766, but whether it was by accident or suicide is unclear. 74 The current quinquennial sample includes only one explicit case of suicide – that of John Jones, who ‘Hanged himself in his Cabin’ on 1 August 1777. 75 The mental scars of witnessing the horrors of naval warfare at close hand have been highlighted by Roland Pietsch. 76 It is possible that these find some reflection in the frequency of punishments for drunkenness in Greenwich Hospital's disciplinary records, 77 as well as the institution's consistent problem with desertion. 78 George Williams, for example, deserted at least four times and was repeatedly readmitted, which might suggest mental health difficulties or a feeling that the institution was failing him in some way, although one wonders why he requested (and was granted) readmission. 79 Clearly, in keeping with the attitudes of the time, Greenwich Hospital recorded physical injuries more systematically than mental ones.
The impression of the Greenwich pensioners presented in Table 4 diverges markedly from popular portrayals of these men in visual sources, where the loss of one or more limbs appears to be almost as integral to the uniform of a Greenwich pensioner as the famous blue coat. 80 Generally, these wounds were presented in scenes that were either jovial (showing that they did not prevent the pensioners from enjoying themselves) or reverential, where the empty sleeve or wooden leg emphasized the nobility of the men. 81 It is striking, therefore, that from this sample of 6,045 men, only six had lost two limbs – in each case, both legs – and that the proportion of admissions who had lost one limb never exceeded 11.4%, and averaged just four per cent across this period. 82 This conforms to the findings of a study of 97 skeletons from the Greenwich Hospital cemetery, of which only five showed signs of likely amputation – in all cases, the loss of one leg. 83 Unlike the ubiquity of wooden ‘peg legs’ in the popular images, analysis of the bones showed no signs of the use of these prostheses and instead suggested ‘under arm crutch use’. 84
Nevertheless, the Greenwich Hospital admissions data makes clear that only a small proportion of pensioners were amputees. This necessarily raises questions about the reasons for this artistic licence. There were several likely purposes for this disconnect between the visual portrayal of Greenwich pensioners and the statistical reality of that population. 85 First, the presence of serious wounds like amputated limbs served to place these men unambiguously in the category of the ‘deserving poor’. 86 This helped to sidestep some of the possible contradictions of their identity, such as the contrast between their martial masculinity and their inability to support themselves through their own labour. Second, as David Turner has argued, the portrayal of amputation as representing no barrier to the pensioners having the time of their lives acted to ‘disarm the horrors of war’ and so sterilize and downplay the risks of military service, while celebrating the courage of wounded servicemen. 87
In the case of the Georgian militia, disability was grounds for exemption from service, and vague categories like ‘infirm’ allowed for significant discretion. 88 Contrastingly, for Greenwich pensioners, a visible disability could provide tangible proof of their service and show their sacrifice for their country. In this way, as Joanne Begiato has argued, the visible wounds and disabilities of veteran soldiers and sailors were seen as proof of ‘personal valour and national glory’, which could exempt these men from the ‘moralisation of aesthetics’ that associated deformity with degeneracy. 89
In her study of military welfare during the Seven Years War, Erica Charters has shown that military success was contingent on ‘the state caring about the wellbeing of its troops, as well as being perceived to care’. Commanders and statesmen drew direct and long-term connections between the well-being of servicemen and the ability to recruit volunteers. 90 Like its counterpart at Chelsea, Greenwich Hospital held out the promise that veterans’ welfare could be protected by the state long after their military service, and even for life. In this respect, Greenwich Hospital is emblematic of the relationship between military welfare and military recruitment.
This theme of encouraging naval service connects Greenwich Hospital to debates regarding the overarching purpose of welfare provision in eighteenth-century Britain. Joanna Innes and Helen Berry have argued that some welfare policies were, in part, intended to increase Britain's preparedness for the next bout of warfare. 91 Berry's work concerns the charitable care of foundling children, many of whom were encouraged towards careers in the army and navy. 92 This is not directly comparable to the care of naval veterans at Greenwich Hospital, but it is suggestive of an attitude to welfare as a potential means to achieve practical ends – in this case, military recruitment. The sentiment that the lives of these children were saved for the nation links to Michel Foucault's concepts of biopower and biopolitics, which he dates to the eighteenth century, where states took an increasing interest in the bodily health of their populations as a resource to be shepherded and managed. 93 The vast majority of Greenwich pensioners were no longer fit for active service but the hospital's founding charter made clear that the institution was both for ‘the relief and support’ of veteran sailors and ‘for the encouragement of seaman’. 94 Admiral Sir George Rodney, governor of the hospital from 1765 to 1770, made the connection explicit when he asked: ‘Who would not be a sailor to live as happy as a prince in his old age?’ 95 Consequently, Greenwich Hospital served the state's purpose of incentivizing naval service at one remove by reassuring men that, after their service, they would be cared for by their grateful country. Intriguingly, this was one purpose of Greenwich Hospital absent from the lines of George Hewens' poem, with which this article began.
Conclusion
To conclude, despite Greenwich Hospital's superficially unchanging appearance, its population was far from static. The evolving features of successive admission cohorts offer a reflection of the prevailing and recent status of British naval manpower, the fortunes of the navy and the difficulties of naval manning. Above all, the admissions data reveal the impact of recurring and intensifying cycles of war and peace on Britain's seagoing workforce. As the tabulation of these admissions records continues towards completion, there will be further opportunities for quantitative analysis of this crucial population, using fields such as marital status, height and occupational background. What can be said with confidence is that the level of detail contained in the Greenwich Hospital records offers a valuable and underutilized window into Britain's seagoing workforce from the holistic perspective of the end of their careers, and reveals the crucial human components of Britain's naval strength in a way that is collectively quantifiable while still sensitive to the individual. Furthermore, Greenwich Hospital sits at the point of convergence of many of the contradictions and socio-economic negotiations that lie at the heart of Britain's stormy path through the ‘Age of Revolutions’, and is a desirable avenue for extensive future study.
Footnotes
Acknowledgements
I would like to thank Martin Wilcox for generously sharing his earlier work on the Greenwich pensioners from 1705 to 1763 and acting as an invaluable guide as I grappled with the Greenwich Hospital admissions records. Elaine Galloway and the members of the Greenwich Hospital Research Group provided a kind and supportive sounding board for these ideas and made many excellent suggestions. I thank the two anonymous peer reviewers, whose comments on the initial draft have made this article far better than it would otherwise have been. This article is dedicated to Dr Robert Blyth, Senior Curator in World History at Royal Museums Greenwich, without whom this work would not have been possible.
Funding
This work was supported by a 12-month Caird Research Fellowship at Royal Museums Greenwich.