
Abstract
This article presents how the Registered Nurses' Association of Ontario developed the People-Centred Care, 3rd edition best practice guideline and describes its use in advancing patient advocacy by implementing the three guiding principles, two evidence-based recommendations and five good practice statements. Furthermore, the guideline equips leaders and organizations with implementation tips to promote patient autonomy, address systemic barriers, and foster inclusive, advocacy-driven care. We emphasize leadership’s role in fostering cultures of engagement, collaboration, and empowerment. This is a critical tool for organizations, leaders, and providers seeking to embed patient advocacy within practice and policy. It underscores the transformative potential of leadership-driven advocacy in advancing people-centred care and ensuring health systems prioritize the voices, needs, and experiences of those they serve.
Introduction
Over the past 20 years, there has been significant work to focus health and social services on people, including the relationship between providers and the people receiving care. 1 From this groundbreaking work, the concept of people-centred care emerged, urging health and social service providers to follow a person-led approach that considers the needs, preferences, and values of the person receiving care and the influence that family, the community, and society all have on health. 2
People-centred care recognizes people, families and communities as “participants in, and beneficiaries of, trusted health systems that respond to their needs and preferences in humane and holistic ways.” 3 The inclusion of families and communities, in addition to the person seeking care, necessitates a shift away from the terms “patient-centred care” and “person-centred care” which assumes a focus on individuals. 4 A people-centred approach to care dissolves the paternalistic assumption associated with the biomedical model and the relegation of people to passive receivers of care. 5 Instead, health and social service providers advocate for those accessing care to be treated as people who are capable of making informed decisions aligned with their preferences, needs, and values. 6
People seeking health and social services have the right to and deserve a safe and positive experience. Indeed, the World Health Organization’s (WHO) position is that high-quality health and social care should be effective, safe, timely, efficient, equitable, integrated, and centred around the needs of people. 2 People-centred care is seen as foundational to quality health and social care around the globe.1,7 When care aligns with a person’s needs, values, and preferences, it becomes more effective and leads to better outcomes for the people receiving care, and for health and social service providers and organizations.1,7,8 When people feel respected and genuinely heard (and their health situation allows), they are more likely to actively participate in their care journey, follow treatment plans, advocate for themselves, make informed choices, and report higher satisfaction with their healthcare experiences. 1 This is why people’s experiences with the health system is one of the pillars of the Quintuple Aim and of evidence uptake and sustainability of social movements.9,10 Based on a concept analysis, patient advocacy in health and social care is defined as the professional and ethical act of safeguarding, apprising, mediating, and valuing the people receiving care. In turn, people are empowered through support, representation, and action to uphold their rights, preferences, and safety. 11 Providers are in a unique position to support individuals in advocating for greater control over their affairs.
The Registered Nurses’ Association of Ontario (RNAO) recently published the 3rd edition of the People-Centred Care Best Practice Guideline (BPG) that includes guiding principles, evidence-based recommendations, and good practice statements that promote cultural and equitable practices associated with people-centred care. 12 The purpose of this article is to describe how the BPG can be used to advance and strengthen patient advocacy and drive organizational culture change across the continuum of care. This article is divided into four core sections. First, we briefly highlight the rigorous methodology used to develop the guideline. Second, we discuss how the guiding principles can be embedded into organizational structures to support advocacy at both the organization and provider level. Third, we consider how the recommendations and good practice statements can be adopted to support advocacy at the provider level. Finally, we provide examples of implementation tips for both organizations and providers that can be used to operationalize advocacy. 12
In alignment with the WHO and the People-Centred Care, 3 rd edition BPG, the terms “people” and “people-centred care” are used. Further, the term “leader(s)” is intentionally defined to encompass both formal and informal leadership roles within health and social settings. Formal leaders may include individuals such as nurse managers or clinical directors who hold designated leadership positions and are responsible for organizational oversight. 13 Informal leaders are those who may not hold “official titles” but exert significant influence through their expertise, mentorship, or advocacy—such as experienced frontline nurses, patient champions, or peer educators. 13
Methods
Between December 2022 and December 2024, a panel of 22 interprofessional experts from practice, research, education, policy, and people with lived experience was convened to update a BPG on person and family-centred care. 14 The expert panel determined priority topic areas that the new edition guideline would address, as well as research questions and outcomes to guide the systematic reviews. Two systematic reviews were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 15 and registered in PROSPERO (CRD42023475962). For a complete description of the rigorous development procedures followed in the development of this guideline, please refer to the “methodology documents” tab at https://rnao.ca/bpg/guidelines/people-centred-care.
Search Strategy and Screening
Together with a health sciences librarian, the guideline development and research team conducted a comprehensive literature search for two recommendation questions. For recommendation question one, “Should decision aids used by health providers and people (to support shared decision-making about treatment and care) be recommended or not?”, a search for relevant quantitative studies published in English between March 2022 and February 2024 was conducted in the following databases: Cumulative Index to Nursing and Allied Health (CINAHL), Medline, Cochrane Central, Cochrane Database of Systematic Reviews, Embase, and Emcare. For recommendation question two, “Should sensory-minimizing strategies that address noise and light (used to facilitate people-centred care) be recommended or not?”, a search for relevant quantitative studies published in English between January 2018 and July 2023 was conducted in the databases, as well as in PsycINFO. In March 2025, the searches were updated using the same databases to retrieve articles published between July 2023 and March 2025. All studies were independently assessed for relevance and eligibility by two guideline development methodologists based on priori inclusion and exclusion criteria. Disagreements were resolved through consensus.
Data Extraction and Quality Appraisal
Two guideline development methodologists independently extracted data using a standardized Excel sheet (Microsoft® Excel® 2019 MSO (Version 2408 Build 16.0.17928.20114) 64-bit, Microsoft Corp., Redmond, WA, USA).
Quality Appraisal of Included Studies

GRADE and Development of Recommendations
To determine the certainty of quantitative evidence for each prioritized outcome across studies and for each recommendation question, two guideline development methodologists applied the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. 19 Following GRADE, five domains are assessed: risk of bias, inconsistency, indirectness, imprecision, and publication bias. 19
For each recommendation question, two guideline development methodologists collated information in an evidence-to-decision framework that was presented to the expert panel for feedback. For each recommendation, the evidence-to-decision framework detailed the magnitude of the problem, the balance of benefits and harms, the certainty of evidence, the values people place on outcomes, preferences for the intervention, and considerations for health equity. Preliminary recommendations based on this information were drafted by the guideline development methodologists and presented to the expert panel. The expert panel reviewed the evidence-to-decision frameworks and draft recommendations, finalizing them through consensus.
For more information about the guideline development process, including the use of GRADE methods and evidence profiles, refer to supplementary materials under the “methodology documents” tab on the BPG web page (https://rnao.ca/bpg/guidelines/people-centred-care).
Good Practice Statements
In addition to the recommendations, the expert panel identified and came to a consensus on good practice statements. Good practice statements are actionable statements that are deemed to be so beneficial that conducting a systematic review would be a poor use of time and resources. 20 These statements are not given a strength or level of certainty, but they are considered to have substantial benefits that far outweigh any harm. 20
Components of the People-Centred Care, 3 rd Edition Best Practice Guideline
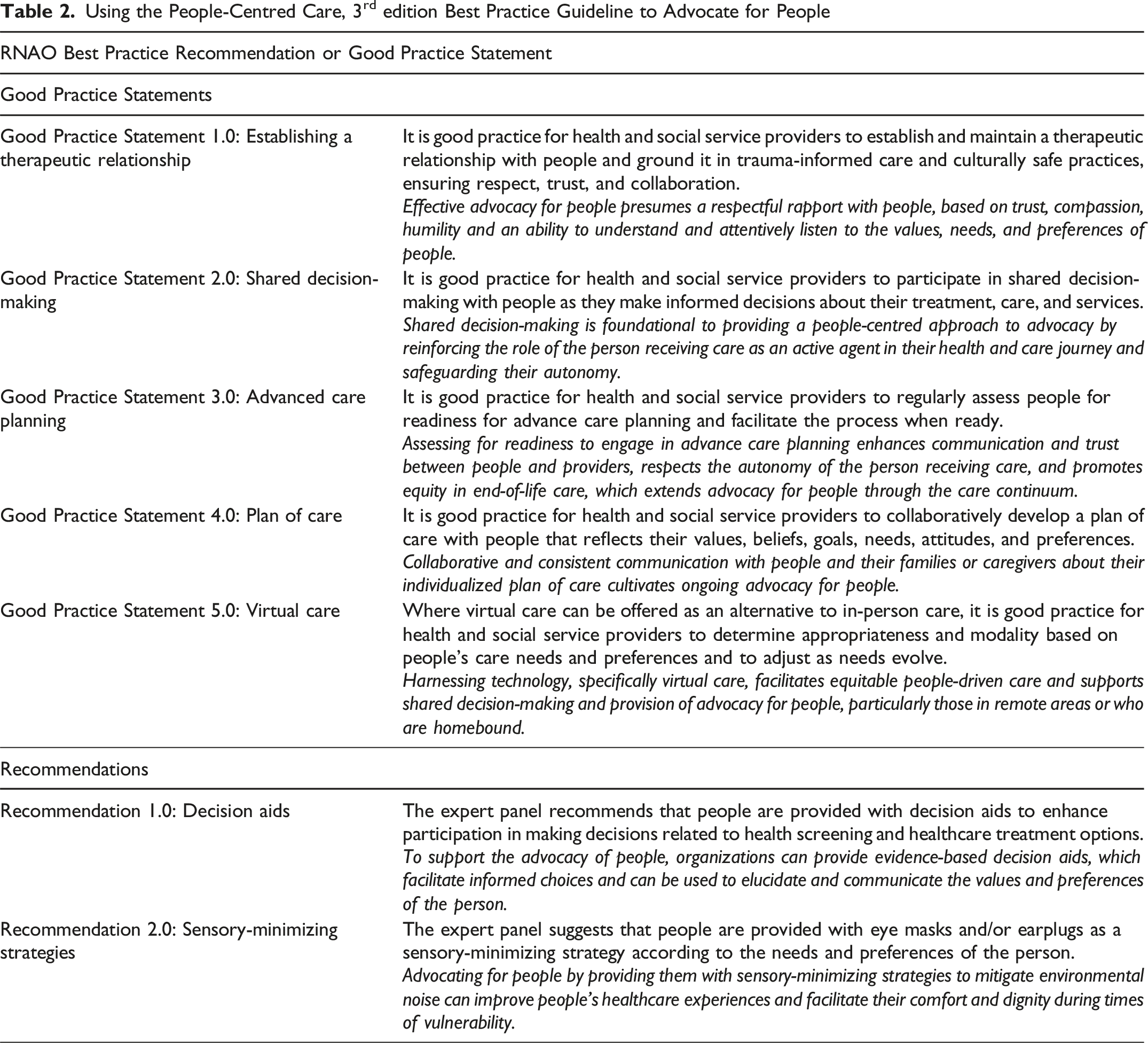
A BPG was systematically developed to inform and enhance the provision of people-centred care across the health and social care continuum. The expert panel identified three guiding principles (i.e., cultural safety, trauma-informed care, and strengths-based nursing and healthcare), two recommendations (i.e., decision aids and sensory-minimizing strategies), and five good practice statements (i.e., therapeutic relationships, shared decision-making, advance care planning, plan of care, and virtual care). Implementation tips, supporting resources, and appendices are also included in the BPG to support implementation in practice.
Discussion
Advocacy is both a clinical skill and a leadership role competency that drives organizational culture re-design. The skills required to practice advocacy centre on an empathetic attitude, being responsible, and using assertive communication to support people with their decision-making. 21 Advocacy is essential to improve a person’s experiences and outcomes of care, and to be effective requires an organizational culture that values and supports the tenets and attributes of people-centred care. Collectively implementing the guiding principles, recommendations, and good practice statements in the People-Centred Care, 3 rd edition BPG can drive a shift in organizational culture that values people advocating for, and being more in control of, their care.
Embedding Guiding Principles into Organizational Structures
The guiding principles provide an overarching philosophy that sets out a powerful tone for advocacy across the health continuum by shaping the values, priorities, and actions of leaders, health, and social service providers. When explicitly embedded into organizational structures, the guiding principles emphasize commitment to equity and inclusivity, trust and transparency, collaboration and shared decision-making; promoting policies that prioritize safety, empowerment, and cultural responsiveness. When leaders across health and social service organizations embrace these guiding principles and model them through their actions, it creates an environment where advocacy is enacted, not just spoken about or endorsed in statements—shaping decisions, policies, and care at every level. Below are examples of how embedding the guiding principles into organizational structures can cascade through all levels of the system. 1. Culturally safe practices recognize and address power imbalances in health and social care, acknowledging systemic inequities (i.e., racism and discrimination) and creating environments where people feel safe, respected, and heard.
22
By recognizing and addressing power imbalances and systemic discrimination in health and social care, championing culturally safe practices and advocating for inclusive policies, leaders set expectations for behaviours and communications across the organization. This in turn powers health and social service providers to build trusting relationships with the people receiving care and provide holistic care that incorporates their cultural, spiritual, and social preferences, not just clinical needs.
23
2. A trauma-informed approach requires organizations to recognize the widespread impact of trauma and how it shapes people’s health outcomes and behaviours.
24
Policies must prioritize and reflect the value of people’s lived experiences, ensuring they are meaningfully integrated into the procedures and practices of health and social service providers. Only then can systems begin to foster environments that support trust-building and empower people to actively engage in their care. It is the onus of the organization, not only individual providers, to ensure trauma-informed care and advocacy are deeply rooted in the shared goal of promoting healing, empowerment, and dignity for people who have experienced trauma. 3. A strengths-based nursing and healthcare approach calls on organizations to prioritize people’s capabilities, resources, and resilience as opposed to their deficits or illness.
25
By embedding this philosophy into organizational policies and practices (e.g., staff training and education) organizations can foster environments that emphasize empowerment and self-determination. This commitment encourages collaborative partnerships and helps people recognize and build on their strengths. Through organizational efforts to cultivate confidence and self-efficacy, people are better supported in advocating for their own needs, wishes, and preferences.
25
Embedding guiding principles into organizational structures sets the foundation for advocacy by aligning care environments with equity, inclusivity, and empowerment.
Supporting Advocacy Using Evidence-Based Recommendations and Good Practice Statements
Using the People-Centred Care, 3rd edition Best Practice Guideline to Advocate for People
Implementing Advocacy through Tools and Strategies
Advocacy can be operationalized through practical strategies spanning provider, organization, and system levels. The BPG offers implementation tips, supported by evidence from systematic reviews and/or the expert panel, that provide practical information for health and social service organizations and providers to translate the recommendations and good practice statements into practice. For example, good practice statement 4.0 states that health and social service providers collaboratively develop a plan of care with people. At the provider level, it is the onus of individual providers to ensure the plan of care is completed with the person receiving care, their chosen family, and all health and social service providers involved in the circle of care. At the organizational level, it is the onus of the organization to support implementation of collaborative care plans.
To further support implementation, the Leading Change Toolkit offers an evidence-informed methodology, based on the Social Movement Action Framework9,26 and the Knowledge-to-Action Framework,27,28 that leaders can use to effectively implement best practices. The recommendations and good practice statements from the People-Centred Care, 3 rd edition BPG can be operationalized at the provider level (leveraging intrinsic motivation to improve patient outcomes), the organizational level (updating policies to reflect best practice), and the system level (speaking out for changes to improve health inequities) by engaging people first and following an active process to create iterations of change. A powerful provider-level strategy is building capacity through best practice champions—trained peer leaders (e.g., point-of-care nurses)29,30 who raise awareness about evidence-based practice, mobilize peers, and use change management processes and social movement action to influence uptake and sustainability of BPG(s) in their setting. 31 Advocacy is a core competency of champions, 31 enabling them to champion practice change(s) that promote social justice and people-centred care throughout health and social service organizations. 11
Contribution to Practice
This article contributes to the advancement of advocacy in health and social care by reframing people-centred care as an organizational duty, as well as a provider-level responsibility. It highlights the pivotal role of leaders in embedding the guiding principles, recommendations, and good practice statements from the People-Centred Care, 3 rd edition BPG into organizational structures and practices. By doing so, it strengthens system-wide commitment to equity, inclusivity, and empowerment and ultimately advocacy for people. Additionally, this article reflects a paradigm shift in terminology—from “patient” or “person” to “people”—underscoring a broader, more inclusive conceptual framework that is now shaping clinical guidelines and care delivery.
Conclusion
A people-centred approach to care supports and strengthens advocacy by promoting meaningful partnerships, shared decision-making, and respect for peoples’ values and preferences. With committed leadership support people-centred care can be embedded into everyday practice, policies, and structures—transforming organizational and health system cultures, creating care environments where advocacy is both supported and sustained. The People-Centred Care, 3 rd edition BPG’s guiding principles, recommendations, good practice statements, and implementation tips mutually reinforce one another and offer a cohesive foundation for practice that supports advocacy for people and the ability for people to advocate for their own care.
Footnotes
Acknowledgements
The authors would like to thank UHN Health Search for developing the search strategies. The authors are also grateful for the expertise and guidance of the expert panel who assisted in the development of the guideline: Heather Thiessen, Kameel Abdul-Kareem, Sarah Benn Orava, Melissa Bush, Susan Dunn, Susan Gapka, Karen Hunter, Anshumi Joshi, Karima Karmali, Alifa Khan, Rev. Carmen Llanos Acero, Elisa Nigro, Alliah Over, Dr. Marie-Pascale Pomey, Sara Ryan, Dionne Sinclair, Tanya Smith, Susan Steels, Melissa Stevenson, and Jill Sullivan.
Ethical Approval
Institutional review board approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the Government of Ontario. All work produced by RNAO is editorially independent from its funding source.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.