
Abstract
Equitable and effective service and policy decisions require reliable evidence-based information; interRAI assessments offer objective data across broad health determinants for multiple purposes. This article aims to highlight selected embedded scales and algorithms and illustrate their prevalence across settings using Canadian data. Ten measures are described along with examples of subsequent use in predicting outcomes, adverse events, and resource utilization across diverse populations and jurisdictions. Prevalence rates for nine scales and algorithms were available across home and community care, Long Term Care (LTC), and inpatient settings. Higher rates of disability in function and cognition were seen in LTC and CCC, whereas palliative care has highest prevalence of health instability. Overlaps in key areas suggest the need to provide targeted services irrespective of setting. Overall, this article highlights the potential of scales and algorithms to capture key clinical information across the broader health determinants while minimizing assessment burden.
Introduction
Health executives, policy-makers, clinicians, and researchers are responsible for caring for populations that include persons with complex health needs, older adults, and persons with disabilities. Clients have diverse health characteristics that span health dimensions (i.e., physical, cognitive, psychoemotional, and social) and provide information beyond diagnoses. It is important that the severity and intensity of their needs are captured in a standardized way to inform care planning, care quality, risk of rehospitalization, funding, and resource utilization. interRAI, an international group of clinicians, researchers, and policy-makers, supports a diverse suite of interoperable clinical assessment tools that cover all ages, and many diverse health domains, all with the goal of improving individual health outcomes across a continuum of healthcare settings and services.1-7
Scales, derived from combinations of items within the assessment, help summarize key aspects of health status. 1 Scores on these scales are automatically calculated at the point of care through computerization. Whenever possible, interRAI scales have been validated against other well-known assessments or scales8-11 and have been designed to be used both at the individual- and population level to monitor changes and trends11-13 At an individual level, the interRAI scales can be used to summarize a person’s status (e.g., physical function, pain, and mood) on admission or across time and service settings, as well as to identify the person’s risk of adverse outcomes (e.g., hospitalization, death, and placement in long-term care) or to help inform the care plan. At a population level, scales can be used to compare across different populations, for risk adjustment in modelling, and to facilitate comparisons across programs, jurisdictions, and nations.14-28
The utility of these scales has been strengthened through extensive use and communication across settings, countries, and populations.1,5 Over time, large assessment datasets have accumulated and been made available for research and quality monitoring, permitting evaluation of scales’ performance and evolution in various situations and for diverse populations. Furthermore, there is evidence of strong validity and reliability of these assessments across multiple healthcare settings and countries.1,26,29-34
Despite the extensive literature on the development and utility of these scales, they are often underutilized and underreported. Thus, this article aims to provide a narrative overview of commonly used interRAI scales and algorithms for adults and to illustrate their prevalence rates in a variety of healthcare settings using Canadian data as an exemplar.
Measurement Overview
Scales and Algorithms
Description of Commonly Used interRAI Scales and Algorithms
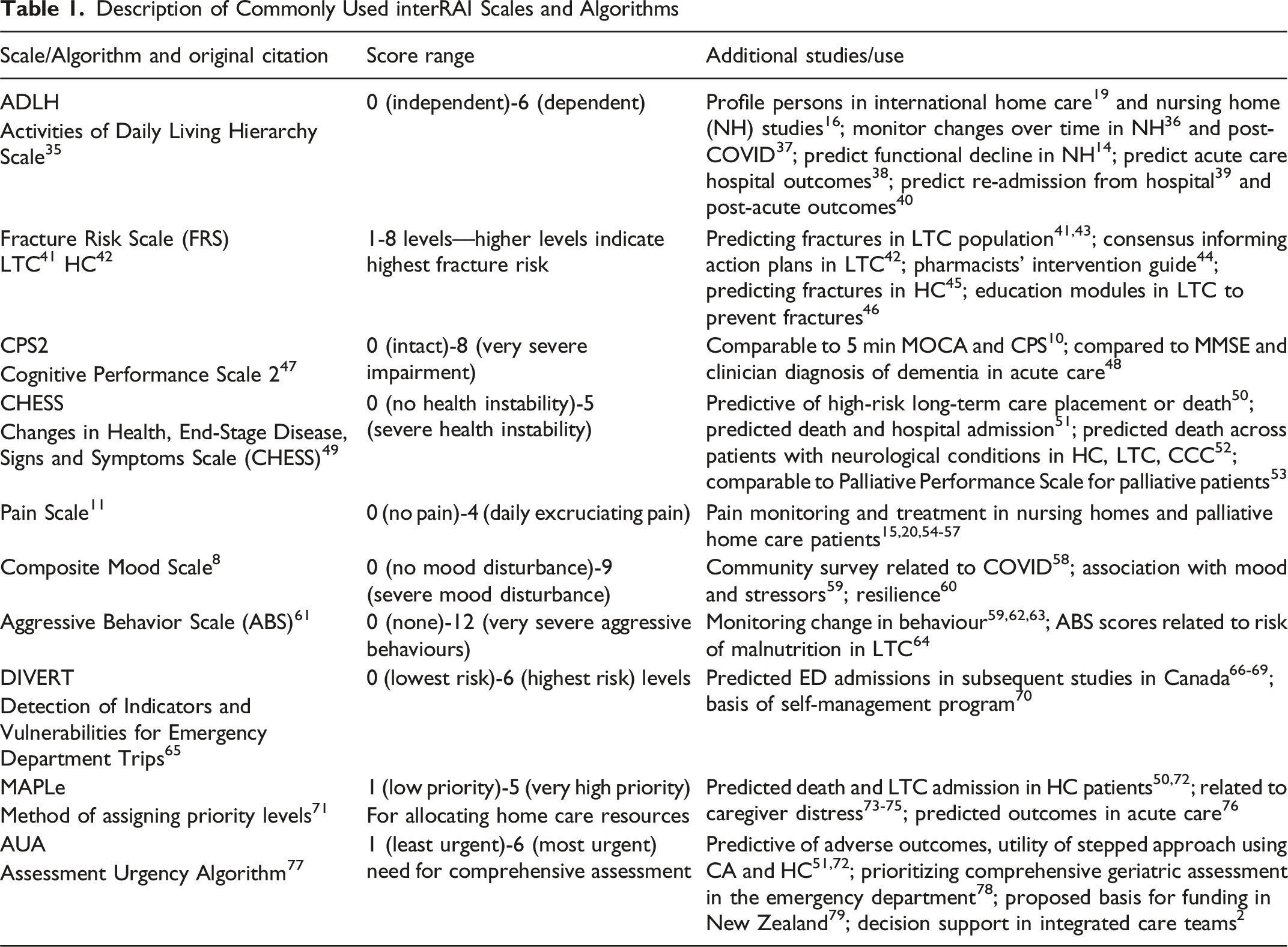
Various functional and cognitive outcome measures address daily clinical decisions but also work together to identify risk and prognosis regarding length of stay, re-admissions, and need for alternate level of care placements.38,39,80
Scales and risk scores are valuable communication measures in primary care for targeting appropriate interventions.2,81 Scores on Fracture Risk Scale 42 in home care or long-term care 41 signal the need for a review on admission whether appropriate interventions are in place. Similarly, newly admitted patients to long-term care experienced increased odds in both positive (i.e., discharged home and improved health) and adverse outcomes (i.e., greater health instability, hospitalization, and mortality). 82 These findings demonstrate a need to either explore interventions for improvement and medical stabilization, or a review of advance directives.
Certain scales such as the Detection of Indicators and Vulnerabilities for Emergency Department Trips (DIVERT) 65 were explicitly developed to address service utilization such as Emergency Department prevention. The utility of the DIVERT scale was highlighted in a study where earlier intervention identification was captured and a complex self-management intervention including resources and capacity building was delivered to community adults. 70 The Method for Assigning Priority Levels (MAPLe) algorithm scores 71 were intended for service-level decision support in home care or long-term care. They were subsequently key in identifying adults at a high risk of LTC placement or mortality, and therefore in need of higher intensity home services. MAPLe scores can also help prioritize adults in need of geriatric consultation, a very limited resource. 83
interRAI regularly reviews the performance of scales across populations and modifies or develops new versions when appropriate and as new evidence emerges, including evidence collected using interRAI tools across the care continuum. Examples include revision of the Cognitive Performance Scale (CPS) to CPS247,48 and the Depression Rating Scale (DRS) to the Composite Mood Scale. 8
It is important to underscore that the scales and algorithms discussed in Table 1 are purposely designed to work together to provide an interoperable and comprehensive biopsychosocial health profile of an individual. This profile uses a common language that is compatible within, and across, healthcare settings. These measures are important at an individual level for care planning, and at a population- and system level, can be, and are, aggregated for use by policy-makers and researchers.
Canadian Scale Distributions Across Healthcare Settings
Scale Distribution for Each Healthcare Setting (N = 622,387). Column Percentages Reported.
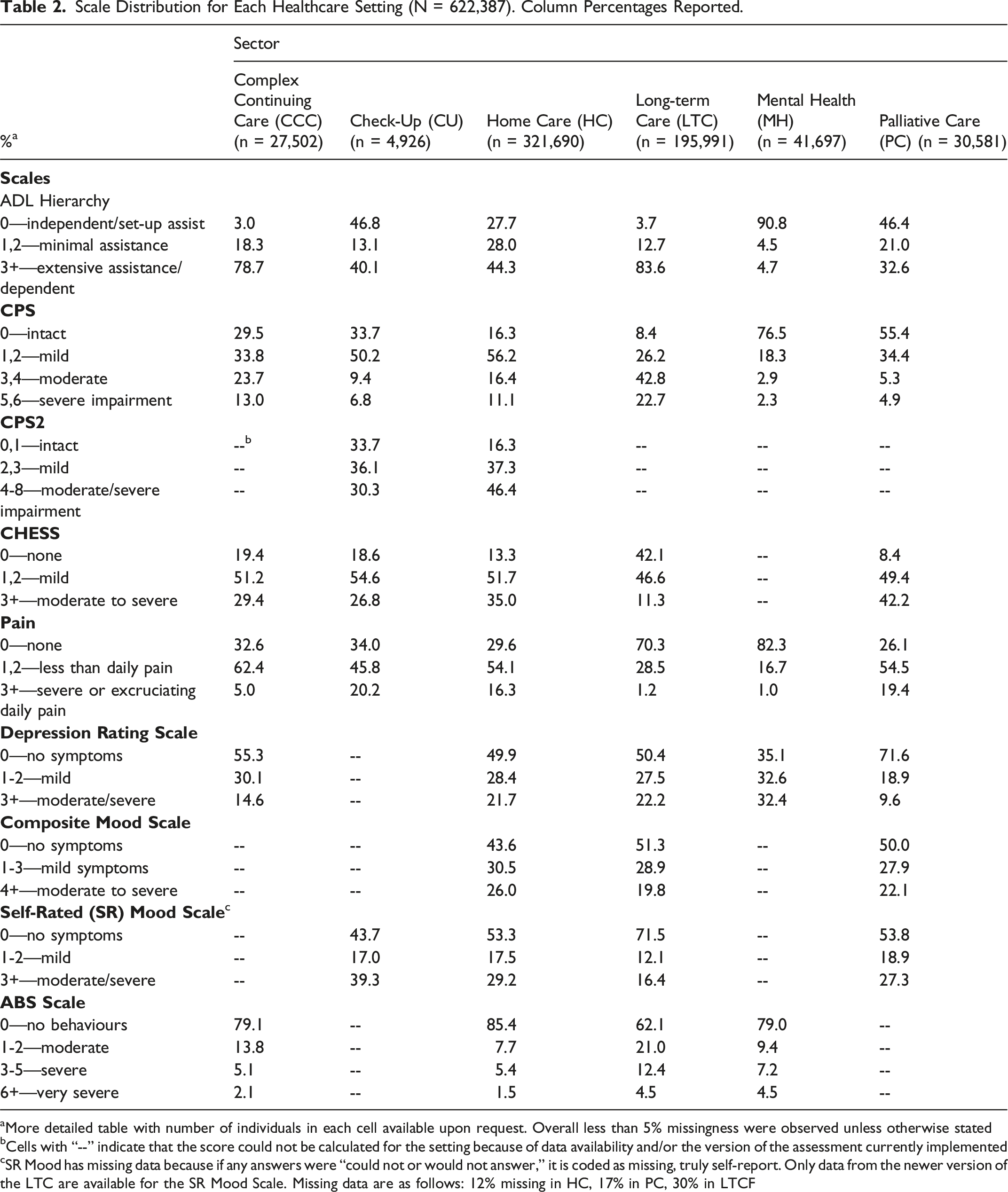
aMore detailed table with number of individuals in each cell available upon request. Overall less than 5% missingness were observed unless otherwise stated
bCells with “--” indicate that the score could not be calculated for the setting because of data availability and/or the version of the assessment currently implemented
cSR Mood has missing data because if any answers were “could not or would not answer,” it is coded as missing, truly self-report. Only data from the newer version of the LTC are available for the SR Mood Scale. Missing data are as follows: 12% missing in HC, 17% in PC, 30% in LTCF
These cross-sectional analyses derived scale scores across the following care settings: complex continuing care (CCC) (January, 2023-March, 2024), home care (HC) (January, 2023-December, 2024), long-term care facilities (LTCFs) (January, 2023-March, 2024), inpatient mental health (MH) (January, 2023-March, 2024), and palliative home care (PC) (January, 2023-September, 2024). Data were deduplicated and the first available assessment was reported within the selected timeframe. Additionally, we also used a limited sample of Check-Up assessments from November 2020 to April 2021. Check-Up assessments capture data on persons living in the community and those receiving primary care. 33 All assessments were housed in the interRAI repository held at the University of Waterloo, Ontario, Canada and ethics approval was received to conduct this work (ORE# 30173 and ORE #30372).
The distribution of the scales by sector is outlined in Table 2. A high proportion of persons with cognitive impairment in long-term care facilities (65.5%) have a score indicative of moderate to severe cognitive impairment (3+). In contrast, in complex continuing care settings and home care, the proportion of persons with moderate to severe cognitive impairment is 36.7% and 27.5%, respectively. For persons receiving care in inpatient mental health and palliative care settings, 76.5% and 55.4% showed no signs of cognitive impairment (i.e., CPS score of 0). Half of the community Check-Up assessment sample showed mild signs of cognitive impairment (CPS score 1, 2).
The Activities of Daily Living (ADL) Hierarchy distribution showed that 90.8% of persons in inpatient mental health settings were independent or required only set-up assistance. In CCC and LTCF settings, most persons experienced moderate to high levels of ADL dependence (78.7% and 83.6%, respectively). The proportion of persons with a score of 0 (independent) in the ADL Hierarchy scale was 46.8% among those in community and primary care settings, compared to the home care sample (27.7%).
With respect to the Changes in Health, End-Stage Disease, Signs and Symptoms Scale (CHESS) scale, persons receiving palliative care had a high proportion (42.2%) with scores of 3 or greater. In home care, 13.3% of patients had no CHESS symptoms, and the majority (51.7%) had scores of 1 or 2. The Check-Up sample and the home care sample show relatively similar distributions across CHESS. In LTCF settings, 46.6% had a score of 1 or 2 with mild signs and symptoms; similarly, those in CCC settings also had the highest proportion of clients in the mild signs and symptoms category (51.2%).
Mood was explored in multiple ways, considering both the DRS and the newly developed Composite Mood Scale (CMS). With respect to the DRS, the highest proportion (32.4%) of those experiencing moderate to severe symptoms of depression were in the inpatient mental health group. Approximately 20% experienced these symptoms in home care and LTC settings. When looking at the Composite Mood Scale across the LTCF, and the home care settings, there is a range of 19.8% to 26% of persons experiencing moderate to severe mood symptoms.
Similar distributions were observed in LTCF and inpatient mental health settings across the pain and ABS scales. A high prevalence of persons in LTCF and inpatient mental health settings reported no pain (70.3% and 82.3%, respectively); rates of severe aggressive behaviours were highest in these sectors (16.9% and 11.7%).
The distribution of scores illustrates the overlap of many functional, cognitive, social, and psychoemotional characteristics as well as the range in severity across the settings along the care continuum. The data offer a bridge from clinical information to policy and health system planning. Comparisons can identify populations and subpopulations of clients in one setting with characteristics that align with those in other sectors, which can prompt an examination of resource use and possible redistribution. Specifically, this could help ensure that the client is receiving the right care within the setting that best supports their care needs.
Discussion
This overview identified commonly used interRAI scales, algorithms, and indices and used data from Canada to show how they can be derived across different healthcare settings. Additionally, this paper outlined how these scales measure broad health determinants among different clinical populations. Health system executives, policy-makers, clinicians, and researchers can use these commonly captured scales and algorithms as measures to aid in making equitable and efficient clinical and resource distribution decisions. These data can inform care from the individual level to the population level. The interRAI assessments captured these measures in a valid, reliable, and standardized way across multiple healthcare settings with no additional assessment or assessment burden to synthesize and provide insight about the clients’ functional performance or capacity.
The prevalence rates across these scales are consistent with what would be expected, based on existing literature and the populations served, in each healthcare setting. It is common to observe high rates of functional impairment in long-term care, complex continuing care, and home care,84-87 as well as higher rates of moderate to severe mood symptoms in the inpatient mental health setting. 8 Interestingly, these data also highlight significant rates of mild impairment as well, suggesting areas where remediation may be possible. This is important as it draws a link between the scales and interRAI’s Collaborative Action Plans (CAPs), evidence-informed tools that can be used to prioritize and guide individual care planning efforts. Different ranges across various scales act as a trigger for CAPs, which indicate areas where maintenance or improvement could occur when developing the care plan.
Summarizing health across these domains facilitates a common language among clinicians, health executives, policy-makers, and researchers which builds a bridge from practice to evidence-based decisions. Common language and common tools are essential in creating and maintaining an interoperable system across all levels of healthcare and healthcare services. Standardized communication within and between teams2,81,88 allows for consistent intra- and inter-organizational comparisons, as well as national and international comparisons.5,15,16,19 Thus, decisions within and between organizations, nationally and internationally, are evidence-based and from a consistent source. The interRAI systems are inherently designed to be interoperable and this is an important feature that has played a critical role in the use of these data in further research aimed at addressing clinically relevant questions.
There has been broad implementation of interRAI systems and as such, broad and unique applications of these scales and algorithms. For example, Turcotte and associates 23 used prior interRAI home care assessments to develop a measure of clinical frailty on admission to ICU. They used this frailty measure to compare survival in Intensive Care Unit (ICU settings) for those with and without mechanical ventilation. The findings of this work provide an example of the utility within, and between, healthcare settings using linked healthcare databases and demonstrate the implications with respect to triaging, care decisions, and care planning. Similarly, Sinn et al. 50 examined the application and use of the CHESS and MAPLe together (i.e., those with higher scores in both the CHESS and MAPLe) to predict one-year mortality and LTC placement among home care clients. This is an innovative and clinically relevant way to use these two outputs together to identify a higher needs population.
Care planning was also a critical application for the work conducted by Egbujie et al., 89 wherein trajectories of functional decline, as measured by ADLH scale scores, were observed over 36 months. The authors found that baseline ADLH scores were the strongest predictor of further decline and identified positive factors that could indicate the potential for functional recovery. This is an important clinical finding with respect to care planning, resource allocation, and prevention.
Routinely collected scales and algorithms provide an opportunity to examine effects of a policy change or event across multiple health domains and status. Notably multiple international studies were able to evaluate effects of consequential and rapidly evolving changes in the healthcare landscape due to COVID-19 pandemic functional performance,24,89,90 cognition,59,90,91 and mental health indicators59,92 as well as trends in service provision at the system level. 93
Interoperable comprehensive assessments provide an opportunity to identify and understand the unique needs and outcomes of smaller subpopulations across the care continuum measured in a consistent way. A large Canadian study examined eight neurological conditions including amyotrophic lateral sclerosis 94 across LTC, CCC, psychiatric hospitals, and home care settings. Additionally, there are multiple studies that have considered various subpopulations with broader neurological conditions as well as other specific conditions such as multiple sclerosis and brain injuries.52,73,95-99
The scales and algorithms can be used across the lifespan and across diverse populations. There are other scales available for mental health 8 and child and youth 100 populations. Many of the child and youth scales parallel the adult instruments to facilitate following individuals across the lifespan. Further, national-level organizations can, and do, use, and report on these scales at a population level (e.g., Canadian Institute for Health Information). The interRAI assessments and scales have also adapted well to different countries and Indigenous groups. 101 In part, the flexibility of administering the assessments facilitates cultural adaptation. Assessors are trained on scoring the response categories, but they are free to elicit information in a conversation. They are not obliged to read exact wording or maintain the order of questions. Assessors may be guided by person’s circumstances and expressed concerns. The interaction can help build rapport and encourage sharing of concerns.
Overall, this article provides insight into the utility of these scales and highlights how they minimize assessment burden while capturing key clinical information across the broader determinants of health. Further, examples of research pertaining to implementation and clinical applications were briefly discussed with their corresponding references. Canada was used as an exemplar to highlight how these scales can be used at a population level to better understand the biopsychosocial clinical profile of the clientele served in each healthcare setting, and to monitor changes over time and during periods of healthcare reform. We can use, in real time, relevant and country specific data, derived from evidence-informed standardized assessments, to guide practice, inform policy, and aid in resource allocation.
Footnotes
Acknowledgements
The authors gratefully acknowledge Gabrielle Stent, RCPN for her contributions in the early development of this work. The authors also express their gratitude to the following colleagues for critical insights and review of the manuscript: Drs. John Morris, George Heckman, Caitlin McArthur, Reem Mulla, and Johanna de Almeida Mello.
Ethical Approval
The project was reviewed and approved by the Research Ethics Board at the University of Waterloo, ORE# 30173 and ORE #30372, and it involved secondary data analysis of information collected using interRAI instruments and secondary analyses of anonymized interRAI data from the data sharing agreement with the Canadian Institute for Health Information.
Consent to Participate
All methods were performed in accordance with the relevant guidelines and regulations. The research team is not involved in data collection, and we do not know the details of what participants are told at the time about how their data might be used in the future (e.g., research purposes). We do not know the actual process involved in obtaining informed consent because each province has their own protocols in place for client consent as the assessments are completed as part of normal clinical practice. These assessments are mandated or recommended for use by the province/territory and those collecting the data would have to follow the policies laid out by their respective ministry of health. All identifying client information is de-identified prior to being shared with the research team. The need for individual-level consent for this cross-sectional study involving secondary data analyses was therefore waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available, but they are directly available to interRAI fellows and their staff and students. Other researchers can access the data from the Canadian Institute for Health Information for researchers who meet the criteria for access to confidential data. These data represent third party data that are not owned nor collected by the study authors. A data request form can be found here: ![]() .
.