
Abstract
Older adults living with frailty and multimorbidity interact with multiple care providers and health settings, resulting in fragmented care and information discontinuity. Standardized assessments potentiate integrated care by communicating consistent measures of health information between sectors and providers. We use a pragmatic case example of a theoretical medically complex older adult to illustrate use of interRAI standardized assessments throughout the health journey. The case example represents the assessment findings of a patient accessing care through primary care, the emergency department, home/community care and long-term care. A suite of assessment instruments embedded with decision support algorithms guides nursing care decisions, while a common language and standardized assessment items support effective communication and collaboration among the health team. Successful adoption of integrated and comprehensive assessment tools requires training, engagement, and time to embed processes into practice. interRAI assessments enable integration through a common language, aligning successive assessments across the care continuum.
Introduction
Older adults with multimorbidity have complex health and social support needs, often requiring care across multiple settings.1,2 This population has high rates of health instability, frailty, functional and cognitive impairment. 3 Older adults also interact with multiple providers across care sectors, creating challenges for care continuity.4,5 Health information sharing across clinical settings is essential to support care integration, health system performance and improved patient outcomes.6,7 However, the typical organization and housing of health records within physical locations (e.g., hospitals, primary care offices) and health sectors (e.g., acute care) are fragmented, inhibiting accessibility and timely information transfer.8,9 Even when health information is shared, use of different assessment, documentation, and care planning tools creates barriers to interpretation and application by providers. 10 Inaccessible historical information results in workforce inefficiencies, including duplication of assessments and diagnostic tests. 11
Standardized assessments are designed to facilitate care integration, reduce assessment duplication, and support continuity of care. Informational continuity is enhanced when the chronological nature of patient information, interprofessional workforce use of information, digital and nomenclature language consistency, and interoperability of information are considered.9,12,13 Standardized health assessments have the potential to ensure access to pertinent clinical history, including pre-morbid syndromes, diagnostic investigations, social needs, patient care goals and tailored care plans,6,14 so that providers can see temporal changes in assessment data.
This article aims to provide an overview of how a standardized approach to assessment, documentation, and care planning, when championed by effective leadership, can benefit clinical decision-making, enhance interprofessional collaboration, and facilitate shared decision-making with persons across health settings from a Canadian nursing perspective.
Description of Care Practice: Intersectoral Approach to Assessment
These assessments can be completed by health professionals (e.g., nurses, social workers, therapists), making them ideal for interprofessional communication across health settings. The interRAI suite of instruments spans the age continuum, from pediatrics to geriatrics, and is designed to be used across diverse care settings. 15 A common core set of approximately 70 items shared between all instruments ensures compatibility across care settings. 15 The suite of instruments support identification of patient needs, strengths, and preferences, to facilitate proactive development of individualized care plans and referrals or consultations. 16
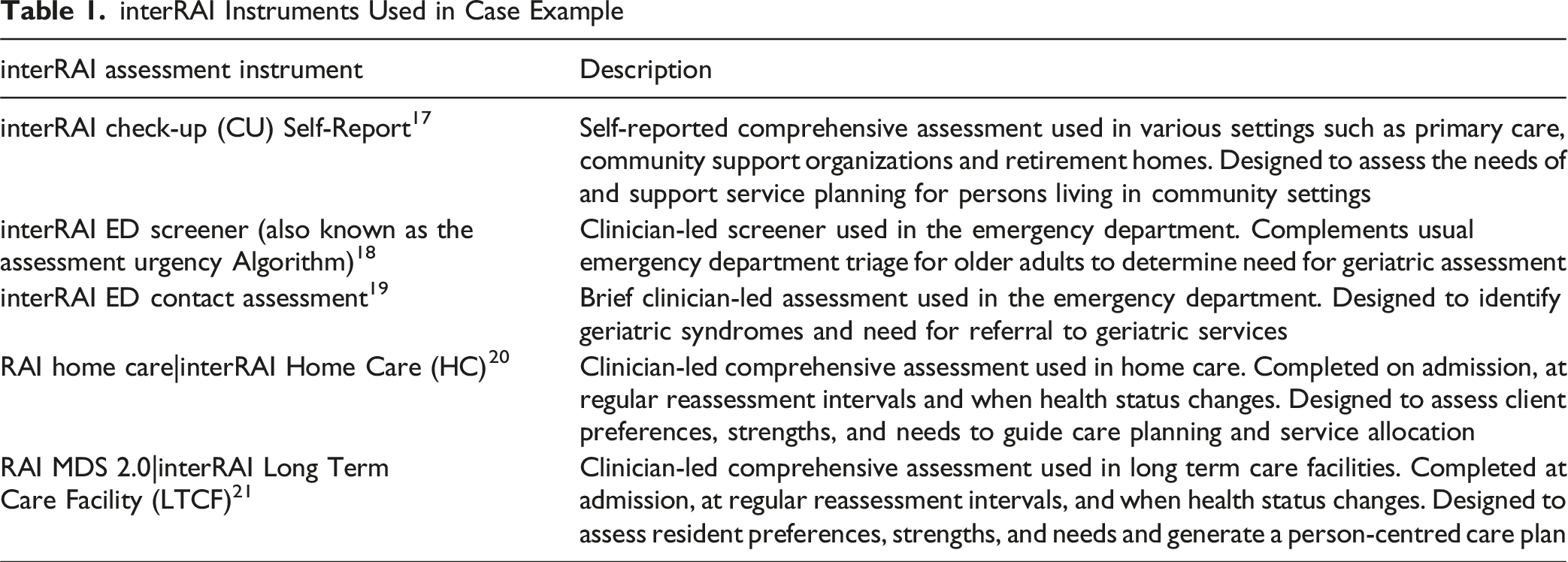
interRAI Instruments Used in Case Example
interRAI Outputs Used in Case Example
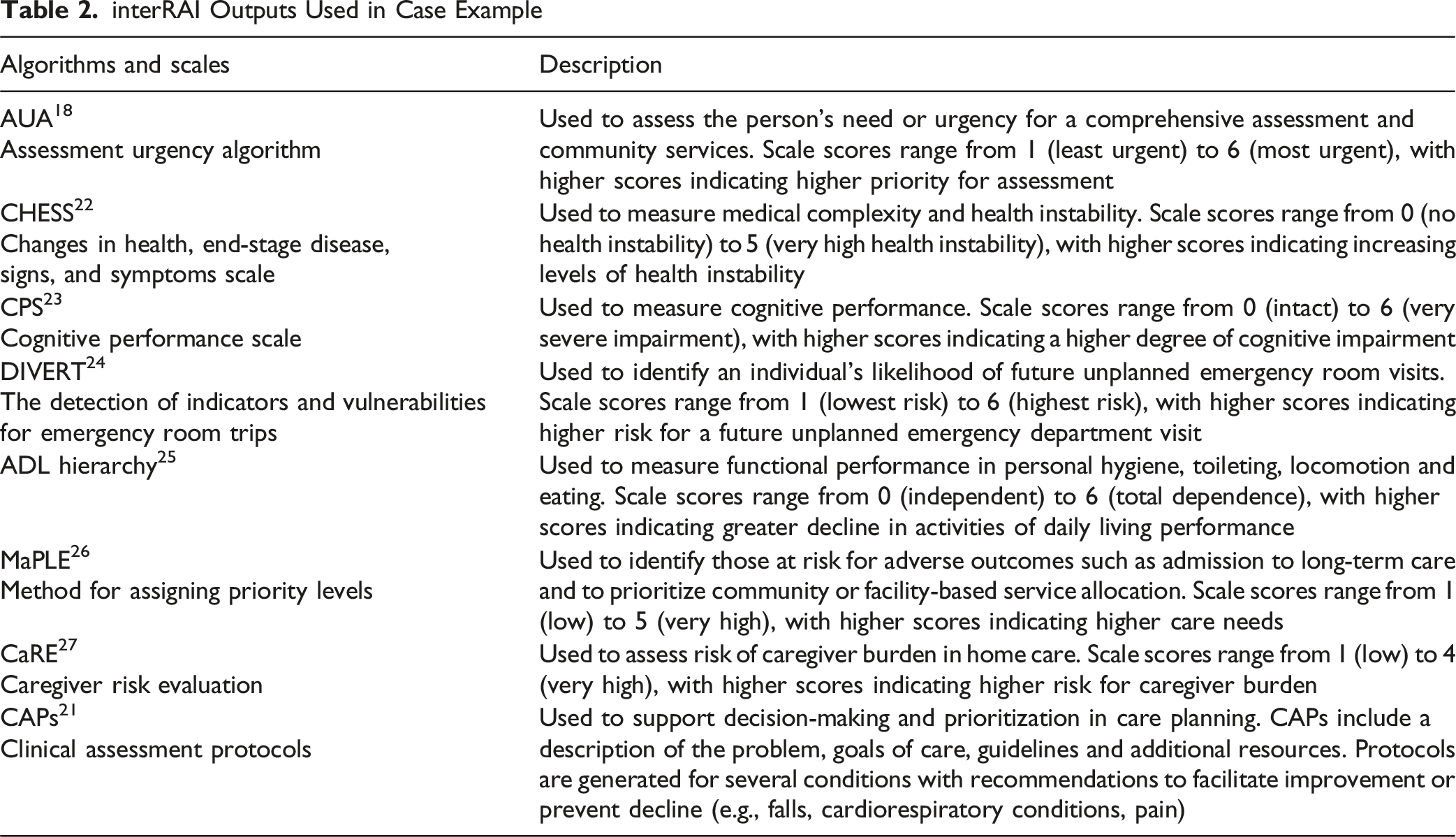
A narrative review of the literature with a theoretical case example is used to describe the health journey of an older adult (Robert) with medical complexity, where nurses leverage interRAI standardized assessments to support continuity of care (Figure 1). Robert’s Story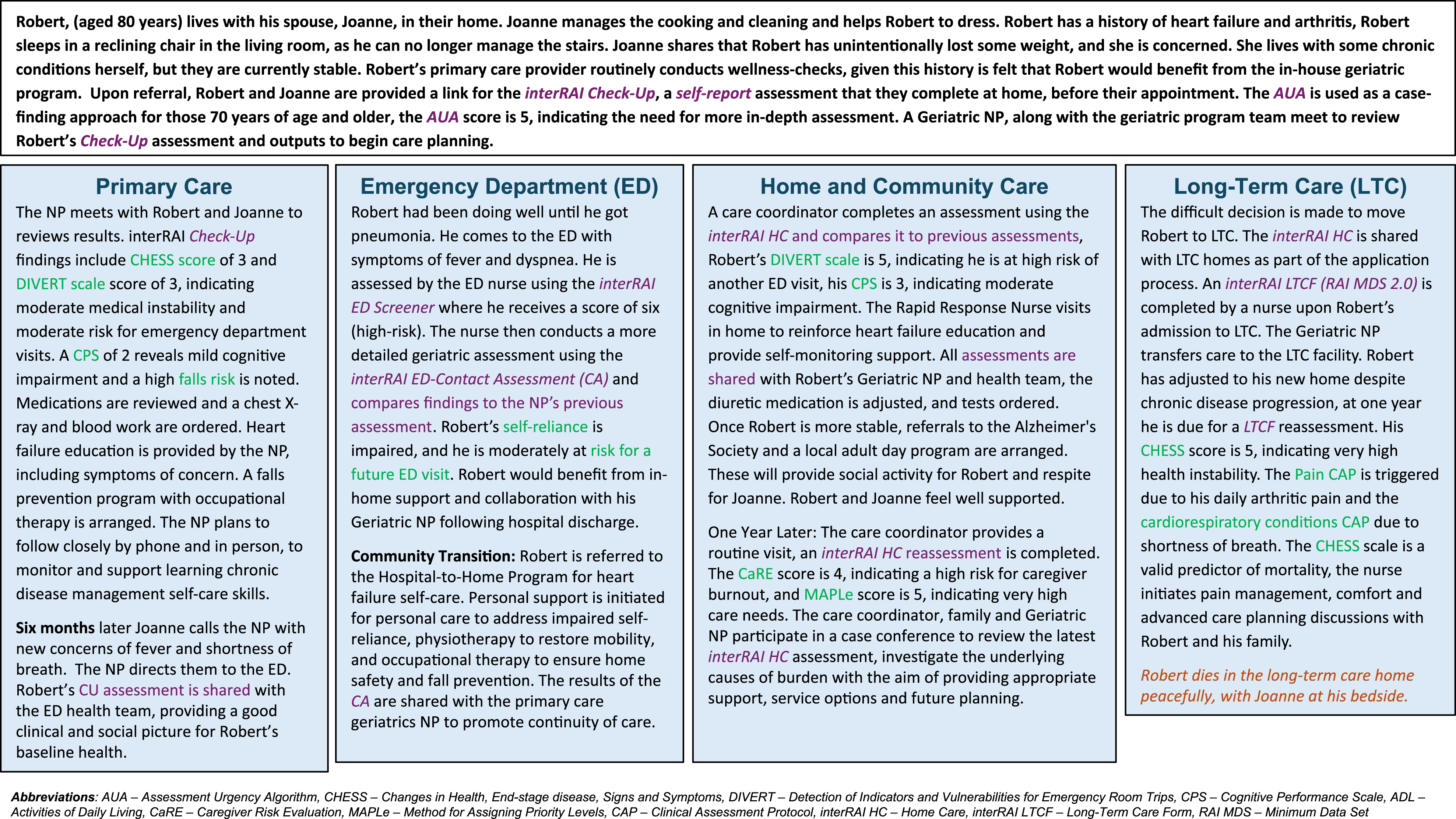
interRAI Check-Up Self-Report: Robert is Seen in Primary Care
Primary care supports older adults with multiple chronic conditions by coordinating their care with various specialists. 28 However, primary care providers report feeling overwhelmed by the complex needs of these patients and lack time and resources to help them navigate the health system effectively. 28 Using the interRAI Check-Up Self-Report (CU), older adults and their care partners can document health concerns before their appointments, increasing autonomy and engagement in care, while allowing more time to address concerns during in-person appointments.29,30 The CU outputs act as a problem list identifying which issues to focus on, thus saving time.
An example of how the CU can be used to support primary care practice is seen in the Complex Care Program of a Family Health Team in Ontario, Canada, where the interRAI Check-Up was implemented to improve care of older adults living with complex needs related to frailty. 31 This shared care interprofessional Nurse Practitioner (NP) led model includes a geriatrician embedded within the primary care team. The Assessment Urgency Algorithm (AUA) is used to screen all rostered older adults and identify those requiring comprehensive assessment. For patients with high AUA scores (5 or 6) the CU is completed with the caregiver, assessment findings inform team interventions and/or referrals for further management. Patients with the highest scores are prioritized to see the team and approximately 2/3 of these patients will see the Geriatrician. For example, a high CHESS score and diagnosis of an unstable chronic condition, such as heart failure, the plan may include medication review, diagnostic tests, and regular follow-up until the exacerbation is resolved. For those who do not require an urgent clinician assessment but are experiencing other concerns, such as loneliness, the NP shares information and facilitates access to socialization programs and community resources.
Emergency Department Assessment System: Robert Visits the Emergency Department
Older adults commonly present with complex medical diagnoses and psychosocial histories, which can be challenging for Emergency Departments (EDs) to manage when care needs change.32-35 Older adults and those receiving home or Long-Term Care (LTC) are known to have greater ED visitation rates, hospital admissions, and worse health outcomes, both in the ED and post-discharge.36,37 The interRAI ED Assessment System is a clinical decision support tool which is prognostic of important outcomes, including mortality, length of hospital stay, and the need for new or additional support services following discharge.18,38,39 The system includes two elements: the AUA screener and a rapid geriatric assessment - the interRAI ED Contact Assessment (interRAI ED-CA). Together, they support identification of geriatric syndromes and the need for geriatrician referral, thereby allowing for interventions to improve outcomes.40-43
The AUA adds approximately 1 minute to usual triage times. 18 As seen in the case, the AUA score of 6 is used to determine that Robert required a rapid geriatric assessment with the interRAI ED-CA. 44 This instrument supports evaluation of a series of health domains, including physical function, cognitive performance, comprehension, mood, falls, nutritional status and symptomology (e.g., pain, dyspnea). 18 Nurses can use information to identify geriatric syndromes (e.g., falls or urinary incontinence) or other health concerns, supporting appropriate support services referrals (e.g., memory or falls clinic) as part of the discharge plan.39,40
Home Care Assessment System: Robert Receives Home Care Supports
In Canada, a small but growing proportion of care has been provided by hospital-to-home transitional care programs, which utilize interRAI tools.45-47 Hospital-to-home programs offer short-term intensive care to help patients with complex conditions transition home, with an aim to reduce readmissions and ED visits.48,49 Older adults receiving home care services are more likely to have cognitive impairment and functional dependency. 33 Therefore, routine assessments, after hospitalization or with treatment changes, are crucial to support successful aging in place.
In the hospital, the interRAI Contact Assessment (CA) is completed by the transitional care nurse to determine the patient’s discharge plan of care. 38 Once at home, the interRAI Home Care (HC) is completed, outputs from the assessment (see Table 2), and clinical judgement are used to develop the care plan and service needs. Decision support tools are used to prompt advanced care planning, including the DIVERT scale, Method for Assessing Priority Levels (MAPLe) and CaRE algorithms.24,26,27 The DIVERT scale identifies the likelihood of future unplanned ED visits and can be used to target nursing interventions. 49 For example, a DIVERT score of 5 and heart failure symptoms suggest Robert would benefit from self-care support and education. A pilot project using the DIVERT Scale and nurse-led intervention for cardiorespiratory symptoms reduced emergency visits by 20% over the 7-month, prompting broader adoption in home care.49,50 Other decision support tools such as the MAPLe and CaRE score assess caregiver burden, prompting discussions about future planning and need for long-term care. Identification of caregiver burden enables clinicians to investigate its underlying causes and initiate appropriate resources and services, including respite care and adult day programs.
Long-Term Care Transitioning Robert to Ensure Well-Being and Comfort
While most older adults prefer to age at home, the proportion of people living in collective dwellings, such as LTC homes, increases from 1 in 5 among the 85-89 age group to more than half of centenarians. 51 Care provided in LTC requires careful and tailored assessment and care planning to adapt to the changing care needs of the individual. 52 Within LTC, the interRAI Long Term Care Facilities or its legacy instrument, the Resident Assessment Instrument-Minimum Data Set (RAI-MDS 2.0), are used to conduct assessments. 53 Upon completion, CAPs are generated (e.g., pain, pressure ulcers, and cardiorespiratory conditions). CAPs provide potential underlying causes of the issue and guidance for problem resolution to reduce risk for further decline.20,54
The assessment is completed by a nurse upon admission to LTC, repeated quarterly, and as needed with clinical status changes. 55 Assessment information is used by nursing staff to identify resident risk factors, support decision making and care planning. 56 Over successive assessments, nurses note changes in scores and CAPs and respond with appropriate care planning adjustments. For Robert, a high CHESS score along with Pain and Cardiorespiratory Conditions CAPs prompts end-of-life discussions that include comfort and pain management strategies. From a quality perspective, the data support home and system quality improvement initiatives, such as benchmarking and monitoring inappropriate use of antipsychotic medications.21,57
Discussion
Standardized and comprehensive interRAI assessment tools offer interoperability and improve care efficiencies at the person and system levels. This case example highlights for health leaders the feasibility and practicality of interRAI instruments for case finding, care planning, collaboration, and continuity of communication. Workflow efficiencies and individual health patterns are demonstrated through the comparison of pre-morbid and standardized health data tracked over time.
Patient-Level Efficiencies
In our illustration, we demonstrate the benefits of using a standardized assessment instrument, including identifying cognitive, cardiorespiratory, and functional changes over time, along with caregiver needs. When interRAI instruments are used, patients and families report feeling connected in their care, 58 confident that their needs are communicated to and between providers 59 and incorporated into goal-oriented plans of care. 60 Changes in risk scores and associated health states enable clinicians to take proactive measures and systematically allocate time and resources. 53 Reliable assessment tools and shared language of critical findings, such as deterioration, can support clinician collaboration and shared understanding of the severity of conditions or concerns. 43 Decision support features can aid in managing and monitoring chronic conditions in real-time, thus improving patient-specific interventions and case management. 61 Our clinical illustration of interRAI risk algorithms and their use demonstrates their utility and timely decision-support.
Optimal clinical use of interRAI instruments has not yet been realized across care settings.61,62 With appropriate education and practice support, interRAI assessments can reduce duplication of assessment and allow more time to discuss patient and caregiver concerns.11,62-64 However, negative provider perceptions of the tool as an “administrative task”, taking time from direct clinical care, can prevail in settings where clinical utility of the instrument is not emphasized and feedback regarding assessment data is not shared with clinical staff.62,65 For some clinicians, moving from discipline-specific assessments to a shared assessment results in uncertainty regarding professional responsibility and role, however the impact on patient care potentially outweighs this adjustment.66,67 The benefit at the patient level must be realized by clinicians, to support implementation of standardized assessments such as interRAI. Improved patient outcomes have been demonstrated post-implementation, including reduced hospital admissions and improved functional outcomes.14,68,69
Optimizing Interprofessional and Sectoral Integration
The case demonstrates standardized assessment tools that function cohesively as a system of intersectoral communication. 10 This ensures that the continuance of care is consistently measured using a shared language. 43 Workforce collaboration can further support positive patient outcomes,61,70 through referrals and the transfer of assessment information across health sectors. interRAI standardized assessments can support multidisciplinary models of care in home care,26,27 and palliative care 59 settings. For example, a novel project of an interprofessional model of care, led by a primary care NP, used the Check-Up with patients awaiting geriatrician consultation to prioritize those at the greatest risk for poor outcomes. This approach expedited geriatric-sensitive interventions by the NP, such as medication reconciliation, referral to community support services and resulted in a 50% reduction in ED visits. 71
interRAI assessments used in community-dwelling and LTC populations have improved the allocation of health resources, nursing care, and the initiation of referrals to interprofessional team members.14,68,72 To successfully implement a system like interRAI on a large scale, it is essential to have patient, clinician and leadership engagement and system infrastructure for sustainable adoption. 73 Limited interoperability between the electronic health record and software to administer the interRAI instruments in a manner that aligns with the workflow of clinicians can threaten successful adoption. 65 From a health system leadership perspective, using a standardized electronic assessment can improve processes, streamline training and optimize health resources when assessment outcomes are integrated into continuous quality improvement processes.74,75
Nursing Workforce and Impact
Our case example demonstrates how nurses can enhance daily care, assessment, and documentation by fully utilizing the interRAI assessment suite. This approach reduces the risk of duplicated documentation and supports efficient and effective use of information, adhering to the principle of ‘collect once, use many times’.76,77
Healthcare settings can evaluate care policies using nurse-sensitive outcomes like preventable hospitalizations and preventable complications (delirium, pressure injuries, urinary tract infections, pneumonia).78-80 However, accessing and utilizing data for secondary analysis has been challenging.81,82 The absence of nursing care components in population health work has hindered adoption.83,84 interRAI instruments, which focus on function, cognition and activities of daily living (the core targets of nursing practice), offer a comprehensive framework for continuous quality improvement and research on nursing care impact. Utilizing aspects of the interRAI assessment suite can enhance person-centered care and provide valuable feedback for the nursing workforce and health services.
Limitations
We present evidence supporting the practical and clinical use of interRAI instruments from the perspective of the nurse. However, these instruments are not exclusive to nursing and are used by other healthcare professionals where clinical assessments fall within their scope of practice. While the home care, community and LTC sectors have been robustly using interRAI instruments in Canada, they have yet to be adopted as standard practice in emergency and acute care sectors, indicating areas for future development and integration. 85 Collecting sector-specific data for evaluation of real-world clinical applications of interRAI assessments and their impact on practice patterns (e.g., referral rates) and patient outcomes (e.g., health decline) can be used to drive health system transformation.
Conclusion
In conclusion, interRAI instruments can be utilized across various healthcare settings to provide a standardized language for supporting care of older adults. 31 Their practical clinical use enhances point-of-care decisions, care processes and workflow for patients, clinicians and the health system. The educational and practice needs of the clinician and patients in the setting should be considered when adopting new instruments. Informational continuity is crucial for building collaborative capacity and interprofessional practice, this can be achieved by integration of interRAI assessments into existing electronic health records. Nursing and interprofessional teams can use the standardized assessment items and scales within interRAI instruments across sectors to better capture patient care trajectories, improve integration and reduce fragmentation.
Footnotes
Acknowledgements
The authors wish to extend their sincere thanks to those who contributed to the scientific review of this manuscript, with particular appreciation to George Heckman, Anja Declercq, Julie Weir, and John Morris.
Ethical Approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.