
Abstract
Access to Hepatitis C (HCV) treatment requires a specialist referral in Manitoba, Canada, with specialist availability posing barriers to HCV care. This work assessed the impact of eConsult, an electronic platform that enables Primary Care Providers (PCPs) to access specialist advice, potentially reducing face-to-face patient visits. This single case study was conducted at Nine Circles Community Health Centre in Winnipeg. Charts of individuals referred via traditional pathways (Dec. 2016-Dec. 2017) and eConsult (Dec. 2017 - Dec. 2019) were reviewed, and stakeholder interviews were conducted with PCPs and an HCV specialist. Compared to traditional referrals, eConsult patients were more likely to link to specialist care (100% vs. 69%, P = 0.026) and complete HCV treatment (79% vs. 36%, P = 0.049). The use of eConsult may improve access to HCV care in Manitoba, with outcomes shaped by system agility, adaptability across contexts, and the altruism of healthcare providers who support its use.
Introduction
Canadian guidelines recommend that all individuals living with Hepatitis C (HCV) be considered for HCV treatment. 1 Despite treatment advances, uptake remains limited.2,3 In Manitoba, HCV treatment must be prescribed by a hepatologist, gastroenterologist, or infectious disease specialist. 4 Given that access to HCV treatment in Manitoba requires a specialist referral, the availability of specialists may serve as a barrier to treatment in the province.
A potential solution to improving access to specialist HCV care and treatment in Manitoba is through the use of a novel electronic consultation platform (eConsult). Using eConsults, Primary Care Providers (PCPs) can link to HCV specialists through electronic means and receive specialist advice directly, often in less than 1 week and potentially avoiding face-to-face patient visits. The eConsult platform now used in Manitoba was initially developed by clinicians and researchers in the Champlain Local Health Integration Network in Ottawa, Ontario, Canada. 5 The platform launched in Manitoba in December 2017 via a partnership with the Champlain eConsult group. 6
Upon launching, Nine Circles Community Centre (Nine Circles) was the main clinic utilizing eConsults in the province, including eConsults for HCV specialist referrals. Prior to December 2017, PCPs at Nine Circles connected their clients to HCV specialists via a traditional referral pathway. The HCV specialist that Nine Circles referred to for HCV eConsults had already established a long relationship with Nine Circles; providers at Nine Circles typically referred to this specialist prior to the rollout of eConsult. The study reported here aimed to characterize the impact of the eConsult platform on access to and outcomes for HCV treatment in the context of referrals from Nine Circles and to explore potential facilitators and barriers to its iterative rollout in Manitoba with regards to HCV treatment.
Methods
Nine Circles is a community-based primary care clinic in downtown Winnipeg, Canada, which delivers comprehensive primary care, social support, and prevention services, led by primary care physicians, with a focus on the care of people living with HIV, HCV, and other sexually transmitted infections.
This study utilized a mixed methods embedded case study design, combining a retrospective chart review with healthcare provider interviews. 7 Retrospective clinical chart reviews were performed using the electronic patient charting system used at Nine Circles. Inclusion criteria were HCV-positive serology and age ≥18. Individuals were included in the traditional HCV referral cohort if they had been referred for HCV treatment between December 1, 2016, and December 1, 2017, and in the eConsult HCV referral cohort if they were referred for HCV treatment using eConsult between December 2, 2017, and December 31, 2019.
Variables of interest included demographics, and steps along the HCV cascade of care, including “referred to care” (consult initiated to an HCV specialist); “linked to care” (a scheduled appointment with an HCV specialist, or an HCV specialist agreeing to begin an assessment via eConsult); “treatment evaluation” (chart documentation of HCV viral load, HCV genotype, and a fibrosis staging assessment); “treatment recommended” (benefits investigation with documentation of a completed Exception Drug Status (EDS) Form, or an inquiry for federal treatment coverage to Health Canada’s Non-Insured Health Benefits (NIHB) for First Nations and Inuit Program); “treatment approved” (treatment approval from EDS or NIHB, or a prescription generated for HCV treatment); “initiated treatment” (fulfilment of a prescription); “completed treatment” (documentation of completing HCV treatment course); and “successful treatment” (undetectable HCV RNA ≥12 weeks after completing treatment). 8
Participants were right-censored if they died; if they spontaneously cleared their HCV and no longer needed HCV treatment; if they were incarcerated in a federal prison and could no longer be followed by Nine Circles; if they became pregnant and were no longer eligible to start HCV treatment; if they moved out of province; or if it was documented the patient was unreachable with no known address or working phone number, and did not return to clinic within the predetermined 2 year follow-up period.
Descriptive statistics were used to summarize demographic and clinical characteristics. Kaplan-Meier survival curves were used to model the time taken from initial HCV referral to achieve each step of the HCV care cascade, compared by referral type (traditional or eConsult), and the time taken between achieving steps of the HCV care cascade, compared by referral type. The log-rank test was used to compare the Kaplan-Meier survival curves stratified by referral type. Restricted Mean Survival Time (RMST) was used as a complementary comparison method to account for several cascade steps which had less than half of individuals achieving the step of interest, making a Kaplan-Meier median incalculable. 9 A restricted mean follow-up time of 2 years was chosen for both methods. All analyses were conducted using RStudio with a significance level set at 0.05. 10
Interview questions were developed after preliminary chart review data collection and focused on how eConsults impact access to HCV specialist care, exploring where along the HCV care cascade eConsults may offer particular advantages or disadvantages, as compared to the traditional referral pathway. Stakeholder interviews were completed with two PCPs at Nine Circles, as well as the sole HCV specialist who received HCV treatment referrals. Each interview was approximately 30 minutes duration. Interviews were audio recorded and transcribed. The modified Penchansky and Thomas framework of access to care was used to guide analysis, which conceptualizes access to healthcare across six domains: availability; accessibility; accommodation; affordability; acceptability; and awareness.11,12 Access to care is deemed greatest when all six dimensions maximally “fit” the needs of an individual. Transcripts were sentence-coded into the six domains. If a sentence did not satisfy one of the six domains, a new domain code was created.
Results
Between December 1, 2016 and December 1, 2017 at Nine Circles, a total of 14 individuals were referred for HCV treatment using the traditional referral pathway. Between December 1, 2017, and December 31, 2019, a total of 17 individuals were referred for HCV treatment using eConsult.
Select sociodemographic characteristics among case study cohort participants referred for Hepatitis C treatment at Nine Circles Community Health Centre (N = 31).
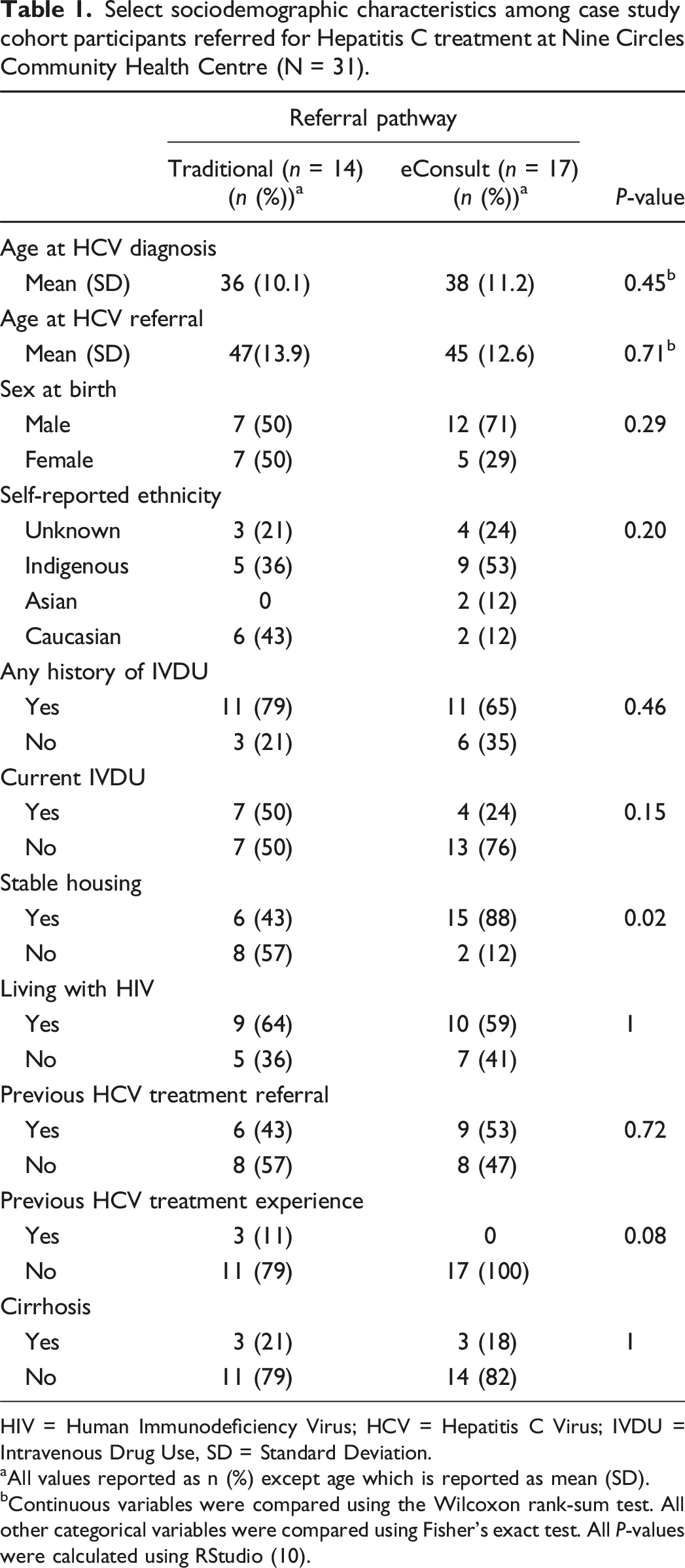
HIV = Human Immunodeficiency Virus; HCV = Hepatitis C Virus; IVDU = Intravenous Drug Use, SD = Standard Deviation.
aAll values reported as n (%) except age which is reported as mean (SD).
bContinuous variables were compared using the Wilcoxon rank-sum test. All other categorical variables were compared using Fisher’s exact test. All P-values were calculated using RStudio (10).
Hepatitis C cascade of care for case study cohort participants referred for HCV treatment at Nine Circles Community Health Centre (N = 31).
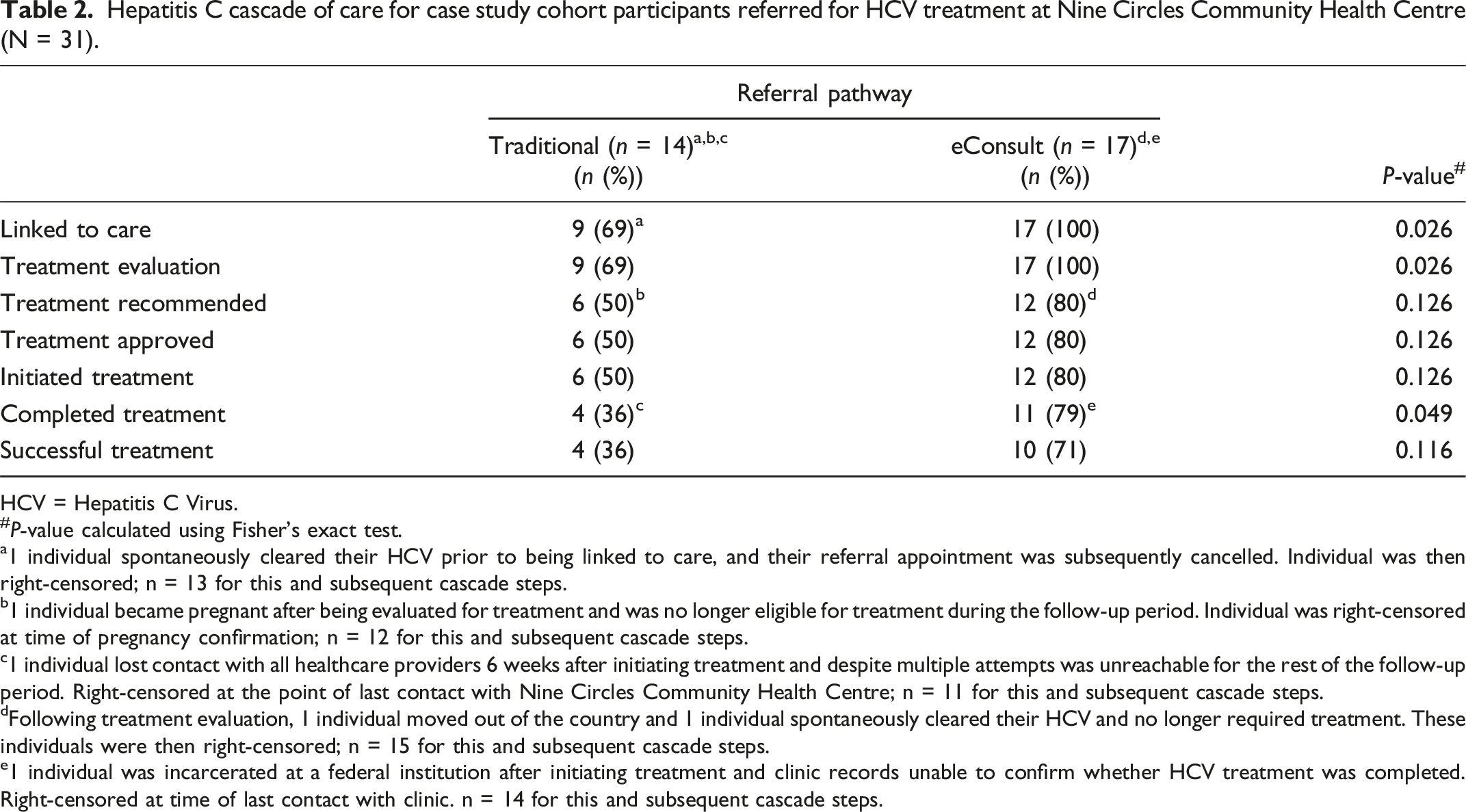
HCV = Hepatitis C Virus.
#P-value calculated using Fisher’s exact test.
a1 individual spontaneously cleared their HCV prior to being linked to care, and their referral appointment was subsequently cancelled. Individual was then right-censored; n = 13 for this and subsequent cascade steps.
b1 individual became pregnant after being evaluated for treatment and was no longer eligible for treatment during the follow-up period. Individual was right-censored at time of pregnancy confirmation; n = 12 for this and subsequent cascade steps.
c1 individual lost contact with all healthcare providers 6 weeks after initiating treatment and despite multiple attempts was unreachable for the rest of the follow-up period. Right-censored at the point of last contact with Nine Circles Community Health Centre; n = 11 for this and subsequent cascade steps.
dFollowing treatment evaluation, 1 individual moved out of the country and 1 individual spontaneously cleared their HCV and no longer required treatment. These individuals were then right-censored; n = 15 for this and subsequent cascade steps.
e1 individual was incarcerated at a federal institution after initiating treatment and clinic records unable to confirm whether HCV treatment was completed. Right-censored at time of last contact with clinic. n = 14 for this and subsequent cascade steps.
From the time of their initial referral, individuals referred via eConsult went on to achieve each step along the HCV cascade of care significantly faster than individuals referred via a traditional referral. Perhaps of most clinical significance, over 2 years, individuals referred for HCV treatment via eConsult initiated treatment, on average, in 261 days (95% CI [120, 402]). This was 316 days shorter (95% CI [138, 494] than those referred via traditional referral, who initiated treatment, on average, in 577 days (95% CI [469, 685]) (P < 0.001; see Figure 1). Probability of not achieving the Hepatitis C (HCV) cascade step of “Treatment Initiation” among patients at Nine Circles Community Health Centre referred for HCV treatment, stratified by referral pathway. (A) Overall Kaplan-Meier curve comparing eConsults to the traditional referral pathway. Individuals referred for HCV treatment via eConsult initiated treatment after a median of 106 days (95% Confidence Interval (CI) [46, NA]). A median could not be calculated for individuals referred via a traditional referral pathway (95% CI [400, NA]) (P = 0.014). (B) Restricted Mean Survival Time (RMST) over 2 years (731 days). Over 2 years, individuals referred for HCV treatment via eConsult initiated treatment, on average, in 261 days (95% CI [120, 402]). This was 316 days shorter than those referred via a traditional referral, who initiated treatment, on average, in 577 days (95% CI [469, 685]) (P < 0.001).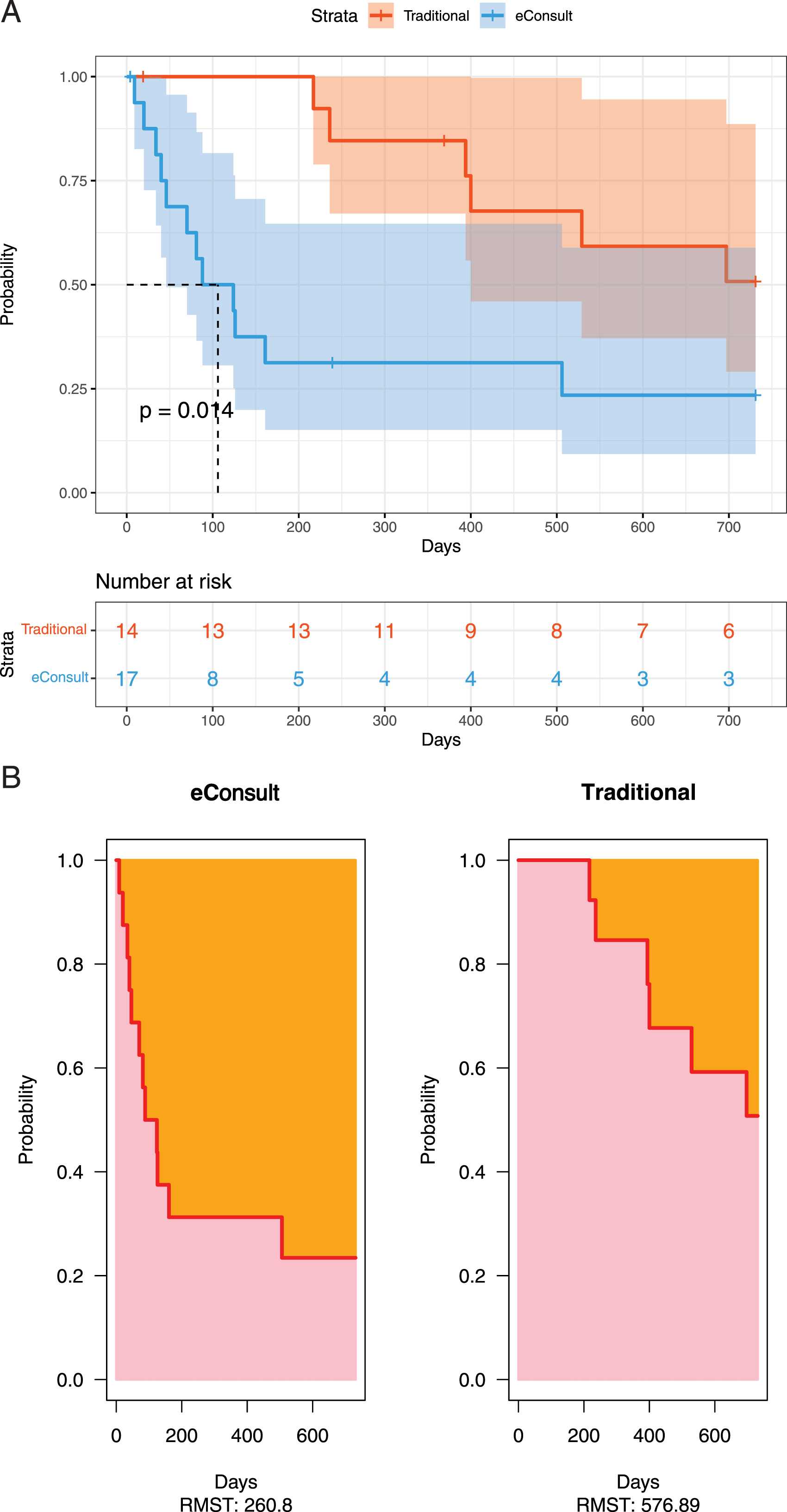
When examining the time between each step of the cascade of care, eConsult referrals were significantly faster in the time between referral and being linked to specialist care—a median of 0 days (95% CI [0, 2])—while individuals referred for HCV treatment via a traditional referral were linked to care after a median of 444 days (95% CI [90, NA]) (P < 0.0001). Individuals linked to care via eConsult were evaluated for treatment after a median of 0 days (95% CI [0,0]), while individuals linked to care via a traditional referral were evaluated for treatment after a median of 11 days (95% CI [0, NA]) (P = 0.0059). While there was a trend towards a shorter time between being “evaluated for treatment” and then having “treatment recommended” for individuals referred via eConsult, it was not significant (P = 0.053). Similarly, there was a non-significant trend towards a shorter time between having “Treatment Recommended” and “Treatment Approved” (P = 0.078). The median time between having “Treatment Approved” and “Initiating Treatment” was similar when comparing individuals in each referral cohort (P = 0.20).
Overall, utilizing eConsults rather than traditional referrals for HCV treatment increased the “degree of fit” between an individual and the dimensions of care described by the modified Penchansky and Thomas framework. All providers interviewed emphasized how eConsults decreased the wait time for individuals referred for HCV treatment, improving the “availability” of and wait time for specialist advice. Notably, the hepatologist interviewed was the only hepatologist in the province fielding HCV eConsults, which did place a high demand on a sole provider. One area where eConsults seemed to hold a major advantage over traditional referrals was “accessibility.” All providers spoke about the benefit of being able to avoid an in-person appointment, where appropriate, with a specialist. PCPs appreciated that eConsults allowed asynchronous advice, enabling them to postpone HCV treatment if more urgent care needs arose. All providers appreciated that eConsults still allowed for more traditional in-person appointments to be arranged if felt to be necessary. Providers felt that eConsult was perceived by patients at Nine Circles to be an “acceptable” alternative to a traditional in-person appointment, in part due to the advances in HCV treatment with the advent of all-oral treatment regimens that had now remained fairly consistent for the last few years. One PCP felt that if HCV treatment guidelines were changing rather than static, eConsults may not suitably “accommodate” HCV treatment; there may be more benefit to a traditional referral and in-person visit. The hepatologist also posited that eConsult advice may not be as feasible for patients at clinics that did not have the support and expertise of the providers at Nine Circles.
In addition to the six dimensions of care captured by the modified Penchansky and Thomas framework, three additional dimensions were added during interview analysis. The first dimension of “agility” related partly to the speed of communication from specialist to PCP which was motivating for PCPs: “it’s very rewarding; you get a response, usually the same date from our specialist that does HCV treatment recommendations.” All providers spoke about how easy the eConsult platform was to use; there was not felt to be an added administrative burden, though the consultant did suggest ways to improve agility, such as integrating direct access to lab results from the provincial database within the eConsult platform. One theme that came up repeatedly was contextual elements unique to Nine Circles and the relationship between the consultant interviewed and Nine Circles PCPs. These ideas were grouped together under the theme “adaptability” to reflect that the successful rollout of eConsult at Nine Circles may be at least in part context dependent: the familiarity of PCPs with HCV treatment; the wealth of allied health resources at Nine Circles including pharmacist support; and a strong working relationship between the referring providers and the specialist. Both PCPs and the specialist commented on the sense of trust that had been established between them over many years of previous communication. The final theme was the extent to which the “altruism” of providers contributed to the success of eConsults for HCV treatment. eConsults rely on the PCP making the referral to include sufficient information enabling a specialist to answer the clinical question, requiring the PCP to take more time than may be typical for a referral. At the time of this study, there was no additional compensation for this extra work, making PCP participation effectively voluntary. Despite this, the PCPs interviewed were still in favour of using eConsult: “we don’t want to become the barriers ourselves to our patient getting treatment.” The specialist spoke in appreciation of the perceived time that PCPs put in to creating an HCV eConsult. Similarly, the specialist was very aware that most Nine Circles providers and their patients relied on them for HCV treatment advice, and reported responding to eConsults even when on vacation “because there’s nobody else doing [HCV eConsults] in Manitoba.”
Discussion
From the time of initial referral, individuals referred via eConsult went on to achieve each step along the HCV cascade of care significantly faster than individuals referred via a traditional referral. The biggest time benefit with eConsult referrals was seen in rapidly linking individuals to specialist care, with over a year in median difference between the two referral cohorts, and then in having individuals quickly evaluated for HCV treatment.
To our knowledge, this is the first published HCV cascade of care to describe individuals living in Manitoba, and the first in Manitoba to compare the achievement of HCV cascade steps via two different referral modalities. Notably, this is the first study to evaluate the use of an eConsult platform for HCV care in a Canadian context. While one previously published study examined the use of eConsult for improving access to gastroenterology consults in Ottawa, only two of these consults were regarding HCV treatment. 13 This is particularly relevant given the geographic challenges faced by Canada’s rural and remote population. In Manitoba, there is one major city, Winnipeg, which serves as the main referral hub for the rest of the province. Some communities are extremely remote, with many being fly-in, fly-out communities with no feasible road access to transport patients to Winnipeg. Exploring non-traditional referral modalities is imperative to improving access to medical care for people in rural and remote communities.
Importantly, the sample size of participants eligible for the study was fairly small. This was not surprising given the case study focused on participants within a single health centre. Because of this small sample, and because participants were all from a single centre, the results may not be generalizable. The observed benefit may be context-specific, shaped by factors such as the familiarity of Nine Circles PCPs with HCV treatment; the presence of allied health supports (e.g., pharmacists); and a longstanding relationship with the HCV specialist. Future research should prioritize evaluating eConsults across diverse clinical settings and with multiple specialists to assess the generalizability of these results. As well, only two of four PCPs who worked at Nine Circles during the study inclusion period were interviewed. However, thematic saturation was felt to have been achieved; it was notable how perceptive and aligned the PCPs were in accurately recognizing perspectives of the specialist, and vice versa. The study did not include the perspectives of patient stakeholders. Without this essential component, a holistic understanding of access to HCV care cannot be achieved. Future studies examining access to care should aim to include patient perspectives where possible.
While eConsult shows great potential in helping expand access to specialist advice, successes seen with HCV care at Nine Circles may be partly context dependent. Creative solutions to overcome barriers to HCV care will be needed to reach the federally-endorsed goal of connecting 80% of eligible people to HCV treatment by 2030. 14 These solutions must also address socioeconomic and syndemic factors that prevent people from accessing HCV treatment, including houselessness, injection drug use, and mental health comorbidities. Policy-makers should be aware that the success of eConsult, or other novel modalities aiming to improve access to care, may depend on their perceived agility; adaptability to a variety of clinical contexts; and the extent to which they rely on the altruism of healthcare providers to implement them.
Footnotes
Acknowledgements
The authors would like to thank Dr. Robert Balshaw from the George & Fay Yee Centre for Healthcare Innovation, University of Manitoba, for statistical consultation regarding the appropriate methods for time-to-event data analysis with small sample size; and the team at Nine Circles Community Health Centre who were instrumental in supporting and facilitating data collection. The authors would like to acknowledge people living with Hepatitis C in Manitoba, particularly those whose experiences informed this work. We hope this research can contribute to our collective understanding about how to best improve access to Hepatitis C care.
The authors acknowledge with gratitude the late Dr. Luis Oppenheimer, who passed away prior to publication. His enthusiasm for improving access to care, thoughtful feedback, and generous investment of time greatly enriched this work. His insight and mentorship are deeply appreciated and will be fondly remembered.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LJM gratefully acknowledges PhD funding support received from the University of Manitoba Faculty Development Committee, as well as the University of Manitoba Institute for Global Public Health.
Ethical approval
Ethics approval was obtained from the University of Manitoba’s Health Research Ethics Board (UM-HREB) (HS23325 (H2019:416)); the Winnipeg Regional Health Authority & Shared Health Approval Committee for Privacy, Impact, and Access in Research (WRHA & SH ACPIAR) (RAAC2020:011); and the Nine Circles Community Health Centre Research Committee.
Informed consent
Written and verbal informed consent was obtained for qualitative interviews.
Data availability statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.