
Abstract
Increasingly, health leaders recognize climate change as a crucial issue for healthcare operations, requiring a whole-of-system approach to mobilizing governance, leadership, and resources to respond appropriately. Granular-level guidance is needed to guide the operationalization of adaptation, resiliency, and mitigation strategies specific to acute-care clinical operations within Canadian health facilities. We present the Climate-Resilient Acute Care Clinical Operations Framework to guide the development, implementation, and evaluation of strategies within clinical operations to build more climate-resilient acute care systems. The experience of Alberta Health Services, which is currently the largest provider responsible for the delivery of acute care within Alberta, is highlighted as a case study to demonstrate the practical adoption of this framework. As more health systems adopt similar strategies, sharing data and insights generated will contribute to ongoing iterations and adaptations, ensuring the framework evolves to meet the dynamic needs of healthcare sustainability.
Introduction: Climate change as a threat for human health and health systems
Increasingly, health leaders recognize climate change as a crucial issue for healthcare operations, requiring a whole-of-system approach to mobilizing governance, leadership, and resources. 1 These challenges are now a permanent part of health system operations; these systems must be reshaped to encompass adequate, equitable responses while providing safe and quality care. 1 Recently, it has been argued that the Quintuple Aim’s five goals for optimizing health system performance—(1) quality and experience of patient care, (2) population health, (3) quality of work and satisfaction of healthcare providers, (4) equity and inclusion, and (5) cost reduction—must be reframed into a Sextuple Aim integrating environmental sustainability. 2 This is because equitable, high-value care for patients, populations, and providers cannot be accomplished without also caring for the planetary systems that sustain us.
The Sextuple Aim represents a substantive change in approaching policy and practice decisions. Building climate-resilient and low-carbon health systems requires action in three categories: (1) adaptation: adapting to intensifying climate change impacts such as extreme weather events, disasters like wildfires, and air pollution; (2) building resiliency: the ability to cope, respond, and reorganize to increasing demands on the healthcare system while still maintaining its essential function, identity, and structure, as well as the capacity for adaptation, learning, and transformation; and (3) mitigation: reducing the healthcare sector’s contribution to ecological degradation, such as reducing Greenhouse Gas Emissions (GHGEs) and plastic waste. 3 We present the Climate-Resilient Acute Care Clinical Operations Framework (henceforth referred to as the Acute Care Framework) as granular-level guidance to guide the development, implementation, and evaluation of climate-resilience and decarbonization strategies within clinical operations. The experience of Alberta Health Services (AHS), currently the largest provider of acute care within Alberta, will be highlighted as a case study to demonstrate the practical adoption of this framework.
The importance of climate-resilient and low-carbon acute care delivery
Acute care is a major component of healthcare delivery, encompassing a range of functions including emergency medicine, trauma care, pre-hospital and emergency care, acute care surgery, critical care, urgent care, and short-term inpatient stabilization.
4
Hospital care is the largest category of health spending in Canada, most recently estimated at $81 billion per year.
5
All aspects of acute care affect, and are affected by, climate change. Extreme weather events are straining capacity and demands in an already fragile health system.
6
Well-coordinated efforts to address a changing burden of health impacts across system levels will support an agile, sustainable organization that can withstand climate shocks while minimizing carbon emissions waste. Figure 1 illustrates a simplified diagram of the relationship between climate change and acute care impacts in Alberta.7-14 Climate change also affects the infrastructure supporting acute care delivery, exposing critical areas requiring extensive preparedness, often in coordination with other sectors and geographic regions. For example, during the Slave Lake (2011) and Wood Buffalo (2016) wildfires, AHS staff members’ responsibilities relevant to acute care included deploying emergency management plans to manage evacuation of patients from healthcare facilities and ensuring ongoing provision of health services to evacuees and first responders.15,16 This work occurred in coordination with organizations such as the Alberta Emergency Management Agency and the provincial ministry of health.15,16 In 2023, hospitals in Alberta and British Columbia accommodated, at short notice, numerous patients evacuated from a wildfire in Yellowknife.
17
Relationship of greenhouse gas emissions with acute care impacts in Alberta, Canada.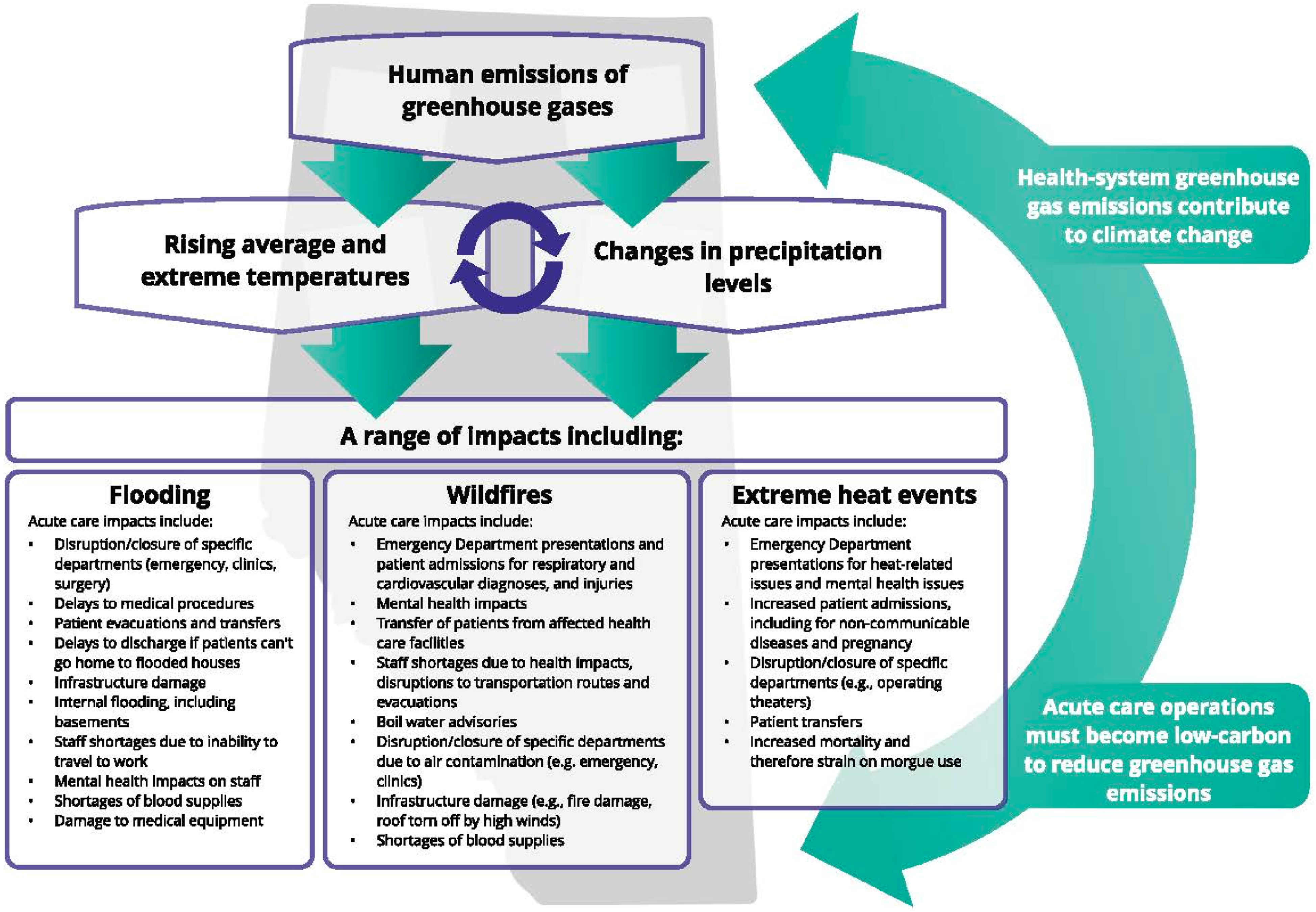
There is also an urgent need to reduce carbon emissions from healthcare services. Acute care, and the infrastructure required to support it, is the largest carbon hotspot for emissions within a health system; 62% of overall healthcare emissions comes from the supply chain for the production, transport, and disposal of goods and services, such as pharmaceuticals and other chemicals, food and agricultural products, medical devices, hospital equipment, and instruments. 12 The GHGEs from medical care not only draw down the national carbon budget but are also directly costly to the health system, as evident by the UK National Health Service’s estimated savings of £180 million by reducing its carbon emissions. 18
To support the necessary awareness-building and action, physician leaders working within AHS developed the Acute Care Framework specifically tailored for Canadian acute care settings. It is based on the World Health Organization’s Operational Framework for Climate-Resilient and Low-Carbon Health Systems, stakeholder insights, and lessons learned from pilot projects within AHS.
1
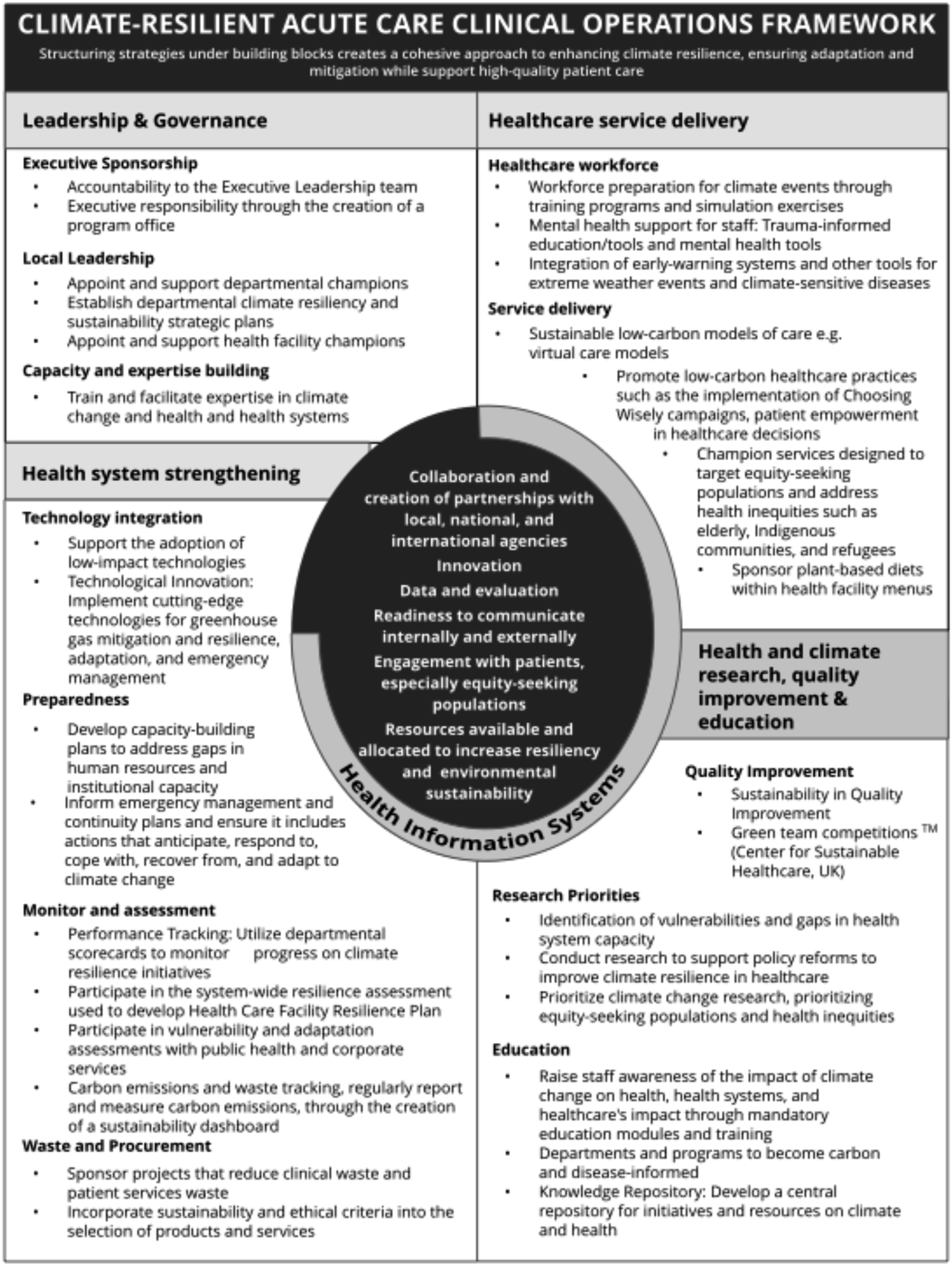
The Acute Care Framework incorporates building blocks of (1) leadership and governance; (2) health system strengthening; (3) health service delivery; and (4) health and climate research, quality improvement (QI), and education. Seven facilitators underpin the building blocks: (1) collaboration and creation of partnerships with local, national, and international agencies; (2) innovation; (3) data and evaluation; (4) readiness to communicate internally and externally; (5) engagement with patients, especially equity-seeking populations; (6) resources available and allocated to increase resiliency and environmental sustainability; and (7) health information systems. A knowledge mobilization expert was recruited to develop two versions of the framework: a simplified graphic suitable for purposes such as meeting presentations (Figure 2) and a more detailed table showing key deliverables necessary to achieve climate-resilient acute care, which is useful for supporting conversations about planning and implementation (Figure 3). Simplified form of the Climate-Resilient Acute Care Clinical Operations Framework. Table form of the Climate-Resilient Acute Care Clinical Operations Framework.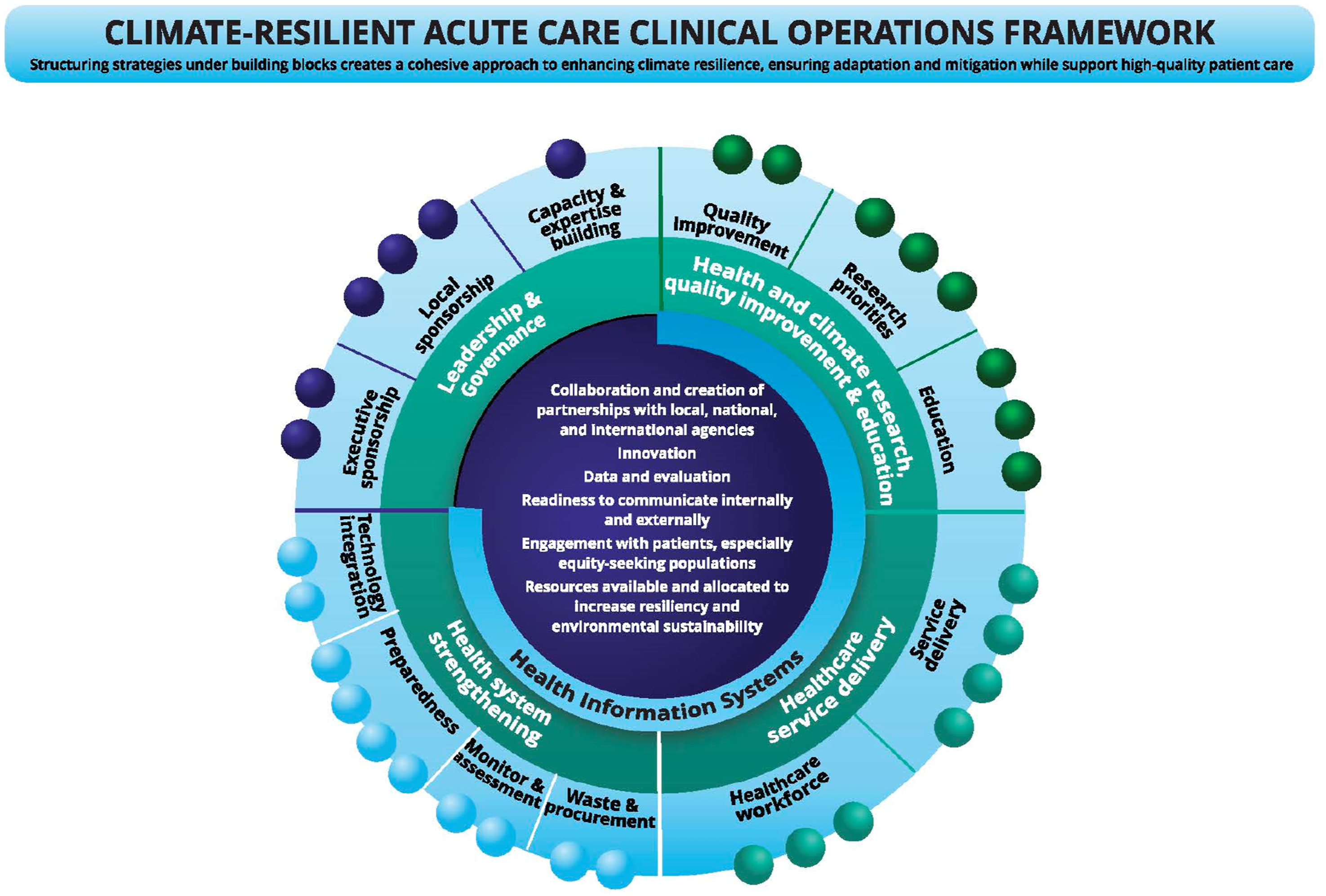
The framework is designed for use by health leaders and teams responsible for embedding resiliency in acute care operations. Anticipated benefits to organizations include: (a) agile operations/departments that can withstand the shocks of the climate crisis; (b) overall cost savings, as many initiatives that reduce the drawdown of the carbon budget also offer financial benefits; (c) increased awareness among staff and patients about participating in sustainable healthcare; (d) increased staff engagement, creating social unity, increasing staff morale, and reducing burnout;
19
and (e) improved health and reduction of harm for the populations served.
Operationalizing the framework: A case study of Alberta Health Services
As noted above, AHS is currently the largest and primary provider of acute care services within Alberta. AHS operates 106 acute care facilities, manages the workforce of all healthcare professionals except physicians, and sets clinical and operational priorities. 20 AHS is divided into five Zones supporting localized decision-making while working with province-wide services such as emergency medical services, diagnostic imaging, and quality and safety. 21 Individual health facilities are managed by a dyad of administrative and physician co-leads reporting to the Chief Zone Officer. 22 In this structure, the necessary whole-of-system response to implementing and sustaining climate-resilient and low-carbon acute care requires provincial-, Zonal and facility-level action. AHS has begun implementing various strategies from the framework within each of the building blocks outlined above. While the implementation process is still in its early stages, we will highlight some initial strategies and quick wins, categorized by the framework’s four building blocks (see Figures 2 and 3).
Building block: Leadership and governance
AHS has a provincial-level Office of Sustainability and Energy Management, which supports health facilities in reducing GHGEs, environmental footprint, and costs. 23 The office coordinates a provincial sustainability committee, which supports the spread and scale of initiatives such as a partnership with Stryker for recycling certain single-use medical devices which originated at Rockyview General Hospital and has now spread to sites in Calgary, Edmonton, Red Deer, and Grande Prairie. 24 Another remarkable site-level initiative fostered by local leadership is the 2023 certification of South Health Campus (SHC) as a Beacon site by the UK’s Centre for Sustainable Healthcare (CSH), as part of the facility’s drive to embed sustainability into QI work. 25 The Calgary Zone’s Internal Medicine department recently appointed a Vice Chair for Planetary Health to cultivate local leadership and expertise. While these grassroots initiatives are important, there is a need for a structure that will coordinate these efforts at a high level and lead the strategic planning necessary to turn AHS into a truly climate-resilient organization.
Building block: Health system strengthening
Sustainable waste management and procurement are being addressed through several program- and site-level initiatives. The Alberta Surgery Initiative has supported operating room staff in finding innovative ways to extend the lifecycle of medical supplies, including sending white disposable towels to veterinarians for reuse and donating spare drapes and gowns to dog shelters or veterinary clinics. Additionally, blue disposable instrument set wrappers find new purpose as paint drop cloths, while unused drapes serve multiple functions, from supporting educational simulation days to aiding in cast cart preparation and painting projects. Procurement staff at individual sites are having conversations with suppliers to investigate lower-carbon options. As noted above, AHS has emergency preparedness plans and has successfully supported the evacuation of patients and the transfer of acute care services during extreme weather events and wildfires. Overall, however, we recognize the opportunity to develop more robust resiliency plans that extend to the frontlines and, importantly, develop provincial- and regional-level vulnerability and adaptation assessments.
Building block: Healthcare service delivery
AHS has explored several low-carbon models of care, with a strong emphasis on virtual care solutions including the virtual home hospital programs in Edmonton and Calgary and virtual outpatient neurology clinics. Although these initiatives were not introduced for sustainability reasons, they have co-benefits for reducing the carbon footprint associated with inpatient care—a particularly resource-intensive aspect of healthcare delivery—and for patients by minimizing complications often linked to hospitalization.26,27 Aligned with Choosing Wisely Canada’s climate-conscious campaign, which aims to reduce unnecessary tests and treatments in Canada in order to reduce patient harm, use of valuable resources, and GHGEs, AHS has embraced numerous low-carbon practices across various areas of care, with a particular focus on surgical services. 28 Significant strides have been made through initiatives including the introduction of the CASCADES Sustainable Perioperative Care Scorecard. 29 This tool prioritizes actions like eliminating desflurane and nitrous oxide, reducing low-value care, promoting the use of reusables, and minimizing surgical waste.
Building block: Health and climate research, QI, and education
The Calgary Zone has started adopting the Sustainable QI (SusQI) approach, amplifying AHS’ existing QI framework by embedding the triple bottom line—encompassing environmental, financial, and social impacts—into QI projects. 30 Staff across the organization are being trained by the Calgary Zone QI consultant to incorporate these outcomes, fostering a more holistic perspective. The adoption of SusQI has been rapid and well-received across the Zone and provincially, significantly boosting engagement in QI initiatives.
The initial consultative process with AHS clinical operations’ Zonal leads established the priority of establishing climate change and health as a core part of organizational knowledge. Awareness-raising initiatives have included departmental grand rounds, AHS-led conferences, leveraging local and provincial networks, and engaging staff through health facility site meetings. In addition, a dedicated course on climate change and health has been embedded into the AHS education platform, MyLearningLink, and advocacy efforts are underway to mandate this course for all staff working within AHS facilities. These initiatives drive a sustainability culture and empower staff to address climate-related challenges in healthcare.
Facilitators for implementing the framework
Our reflections on the role of the facilitators at the heart of the Acute Care Framework (Figures 2 and 3) include the following.
Facilitator: Collaboration and creation of partnerships with local, national, and international agencies
Strong collaboration across AHS levels with key national organizations—for example, between the provincial surgery program and CASCADES, Calgary Zone and the Canadian Coalition for Green Health Care, and SHC and the CSH—has provided valuable guidance and support for moving forward with environmentally conscious healthcare practices.
Facilitator: Innovation
A focus on climate resilience is a new demand on health systems, requiring support for innovative thinking. The Acute Care Framework is itself an innovation that will support the integration of environmental sustainability and resiliency into everyday patient care and research practices, coordinating local-level innovations described elsewhere in this manuscript and drawing on the passion of individual AHS staff members for incorporating sustainability in their day-to-day work.
Facilitator: Data and evaluation
AHS is in the early stages of defining key data and evaluation metrics to assess the overall success of its sustainability framework and strategies. However, some important performance metrics are already being collected under the SusQI approach, including carbon emissions, financial savings (e.g., through bed days and supply reductions), and social indicators such as nursing time saved. These metrics have been used to engage diverse stakeholders at all levels and build a strong case for continued support of these initiatives. To measure the Acute Care Framework’s short- and long-term success, a comprehensive evaluation system will be necessary, ensuring progress is effectively monitored and refined.
Facilitator: Readiness to communicate internally and externally
The role of partnerships, knowledge mobilization, and champions at all organizational levels has been crucial for crafting and disseminating messages suited to AHS’ context. Each site’s organizational culture and physical infrastructure vary greatly, influencing the feasibility of specific initiatives and strategies; the involvement of staff members with this contextual knowledge is essential for implementation success. An example of how AHS’ province-wide scope enables sustainability work is the creation of the role of Surgery Sustainability Lead; the incumbent’s role, connection to, and support of site teams creates a support and knowledge mobilization pathway for teams, including the systems change and cross portfolio work necessary to bring new and known projects to site.
Facilitator: Engagement with patients, especially equity-seeking populations
AHS has long recognized the importance of patient engagement and collaboration to inform the organization’s decisions, actions, and priorities. 31 Alberta patients are excited about and supportive of initiatives to reduce carbon footprint and waste. For example, the “Bring Your Own Bag” initiative in the Peter Lougheed Centre’s day-surgery program, in which patients store their clothing and shoes in their own bags rather than single-use plastic bags provided by the hospital, has been so well-received that its first month saw a reduction of plastic bag use by 42%. Colleagues across Canada have shared that patients in their regions are similarly supportive; further work to incorporate the patient voice in climate change policy-making is essential.
Facilitator: Resources available and allocated to increase resiliency and environmental sustainability
Health systems worldwide are increasingly focused on delivering value-based healthcare, and sustainability efforts naturally align with this goal. For example, AHS’ Office of Sustainability and Energy Management advances initiatives that jointly reduce costs as well as GHGEs and environmental footprint. 23 SHC’s Green Team Competition has brought AHS anticipated annual savings of $221,627 and 30,981 kgCO2e at this site as well as creating awareness and bolstering staff members’ enthusiasm for environmental initiatives. 25 When these initiatives are spread provincially, there will be additional cost savings.
Facilitator: Health information systems
Robust and integrated health information systems are vital to facilitating resiliency, sustainability, data, and evaluation. 1 The recent implementation of the Epic EMR system (called Connect Care) across the province’s hospitals, continuing care facilities, community health centres, and laboratories is an important foundational element in this work, reducing waste by avoiding duplication of investigations and tests and allowing access to multidisciplinary notes to streamline care. 20 For example, AHS staff have developed tools in Connect Care supporting improved provincial surveillance processes for infectious diseases through rapidly identifying patients with recent abnormal lab results and tracking those patients between sites. 32 These early detection tools can help identify changing incidence of specific climate-sensitive diseases. 1
Conclusion
The current pace of climate change, to which the global response has so far been woefully inadequate, will shape human health and health systems for decades and indeed centuries to come. 33 Every aspect of acute-care clinical operations in Canada must be reshaped in light of this threat. The Acute Care Framework is designed to guide the implementation of sustainable, high-quality, and high-value acute care across Canada. Early adoption efforts in AHS have shown the framework’s value for supporting a structured yet flexible approach to embedding sustainability and resilience within the health system, and for coordinating numerous initiatives driven by the creativity, passion, and operational knowledge of staff at all levels—from frontline professionals to senior leadership. 25 While the framework’s core strategies are adaptable, successful implementation in other systems will require customization based on governance structures, resources, and policy environments, and we look forward to the continuous improvement of the Acute Care Framework based on these experiences.
The response of health systems must be proportionate to the magnitude of the threat from our changing climate. Alberta’s experience, similar to other provinces, is that climate-resiliency and low-carbon ideas are often initiated from the passion and commitment of health system staff; however, over time work done “off the side of the desk” is subject to staff turnover and burnout. 34 Therefore AHS, and all acute care operations across Canada, must support this work with (a) leadership commitment across all system levels; (b) adequate resourcing and prioritization; (c) dedicated positions employing people with subject-matter expertise, system knowledge, and credibility with their peers; (d) processes for learning from the practical expertise of frontline staff and patients about opportunities to reduce waste; and (e) formalized learning health cycles to rapidly integrate data into policy and practice.34-37 These steps, supported by the Acute Care Framework, are urgently needed to reduce current and future impacts for Canadian patients, communities, and health systems. 3
Footnotes
Acknowledgements
We acknowledge with thanks the input from Pedro Reis and Tara Klassen, and Kristie L. Ebi’s review of ![]() . Denise Thomson, Gabrielle Zimmermann, and Candace Ramjohn (who designed the versions of the framework reproduced here) are supported by the Alberta SPOR SUPPORT Unit (AbSPORU), which is co-funded by the Strategy for Patient-Oriented Research program of the Canadian Institute for Health Research (CIHR), Alberta Innovates, and the University Hospital Foundation. AbSPORU also acknowledges its implementation partners: the University of Alberta, the University of Calgary, the University of Lethbridge, Alberta Health Services, Athabasca University, the Women and Children’s Health Research Institute, the Alberta Children’s Hospital Research Institute, and Alberta Health.
. Denise Thomson, Gabrielle Zimmermann, and Candace Ramjohn (who designed the versions of the framework reproduced here) are supported by the Alberta SPOR SUPPORT Unit (AbSPORU), which is co-funded by the Strategy for Patient-Oriented Research program of the Canadian Institute for Health Research (CIHR), Alberta Innovates, and the University Hospital Foundation. AbSPORU also acknowledges its implementation partners: the University of Alberta, the University of Calgary, the University of Lethbridge, Alberta Health Services, Athabasca University, the Women and Children’s Health Research Institute, the Alberta Children’s Hospital Research Institute, and Alberta Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Denise Thomson, Gabrielle Zimmermann, and Candace Ramjohn (who designed the versions of the framework reproduced here) are supported by the Alberta SPOR SUPPORT Unit (AbSPORU).
Ethical approval
Institutional review board approval was not required.
Data availability statement
Data sharing is not applicable as no datasets were generated or analyzed during the current study.