
Abstract
In Canada, the provision of Paediatric Palliative Care (PPC) services faces unique barriers due to a large geography and dispersed service population. This review identifies global challenges and strategies to inform efforts in strengthening Canadian PPC access and delivery. Utilizing a rapid review methodology, two databases were searched for publications between 2014 and 2024. Five hundred and ninety-five studies were imported, and 31 retained. Challenges identified in the literature included (i) uncertainty with team roles and responsibilities, (ii) lack of PPC familiarity, and (iii) navigating fragmented health systems. Recommendations included (i) enhancing education, (ii) streamlining access, and (iii) increasing awareness. Concerted effort between health leaders is essential to implement solutions towards a more integrated care system–one that considers the needs of all children. Prioritizing nationwide awareness, access, and capacity-building will ensure PPC meets the needs of all children and families, regardless of location.
Introduction
Paediatric Palliative Care (PPC) encompasses an active and total approach to the care of children with life-limiting illnesses and their families. These conditions are likely to lead to death before the age of adulthood. 1 Children and their families may wish to pursue curative treatment, to prolong life, or to provide comfort measures. The philosophy of palliative care embodies compassion, care, and support for children and families no matter their decision, from the moment of diagnosis, until the time of death and beyond. PPC differs from adult palliative care in that it requires expertise, resources, and approaches tailored to the unique needs of children and their families.
Globally, an estimated 21 million 2 children could be in need of palliative care, with approximately 9.8 out of every 10,000 Canadian children needing access to these services. 3 For Canada’s population of over 10 million children, this could translate to over 10,000 children in need of PPC annually. 4 However, Canada faces distinct challenges to providing these services. 5 The country’s vast geography and dispersed population of children with palliative needs requires innovative service delivery models. Currently, PPC expertise is concentrated in a few urban tertiary centres, 6 forcing many families to travel long distances to access care. This also means that many children die at these institutions, often in critical care units, away from home and those who matter to them. Although Canada has made strides in PPC research, policy, and service development over the past three decades, 7 barriers remain in ensuring that children and families can receive the care they need, particularly in their location of choice. Health Canada 8 has recently identified palliative and end-of-life care as a national priority area for research and program development. This includes identifying and supporting the unique needs of children with life-limiting illnesses across the country. 9
This article offers a rapid review aimed at synthesizing current literature on international PPC programs and services, focusing on shared challenges and successful strategies to inform system change in Canada. This review uniquely takes a Canadian systems-focused approach, offering actionable recommendations for PPC delivery.10,11
Methods
This research is based on a rapid review methodology as outlined by the World Health Organization. 12 This method strategically streamlines the systematic review process. Considering the immediate need to develop accessible PPC services, this approach was chosen to provide actionable evidence and swiftly support program strategy, policy development, and system improvement.
In collaboration with a health sciences research librarian, a search strategy was developed for Medline (Ovid) and CINAHL (EBSCO) using combinations of the concepts “pediatrics,” “palliative care,” and “programs” (and their variations). Databases were searched on May 6, 2024, limited to the past 10 years (2014-2024) and to empirical research in English or French. Articles were included if they served paediatric or perinatal populations with life-limiting conditions. Studies focusing exclusively on oncology were excluded, as cancer represents a distinct and narrower subset of PPC. Programs considering cancer alongside other life-limiting conditions were included. Studies focusing solely on clinical practice, teaching, or non-programmatic aspects of care were excluded, as these were beyond system-level scope.
Results
Study selection
A total of 595 studies were imported into Covidence© and a final 31 articles retained through a triage process conducted by the first and second author (see Figure 1).13-43 Each article was independently assessed against the eligibility criteria. Conflicts were resolved through discussion until unanimous agreement. Data were manually extracted into an Excel© spreadsheet, detailing country, perspective, population, purpose, methods, findings, and challenges and recommendations for PPC. Challenges and recommendations were narratively synthesized and grouped into salient themes by the authors.12,44 Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart.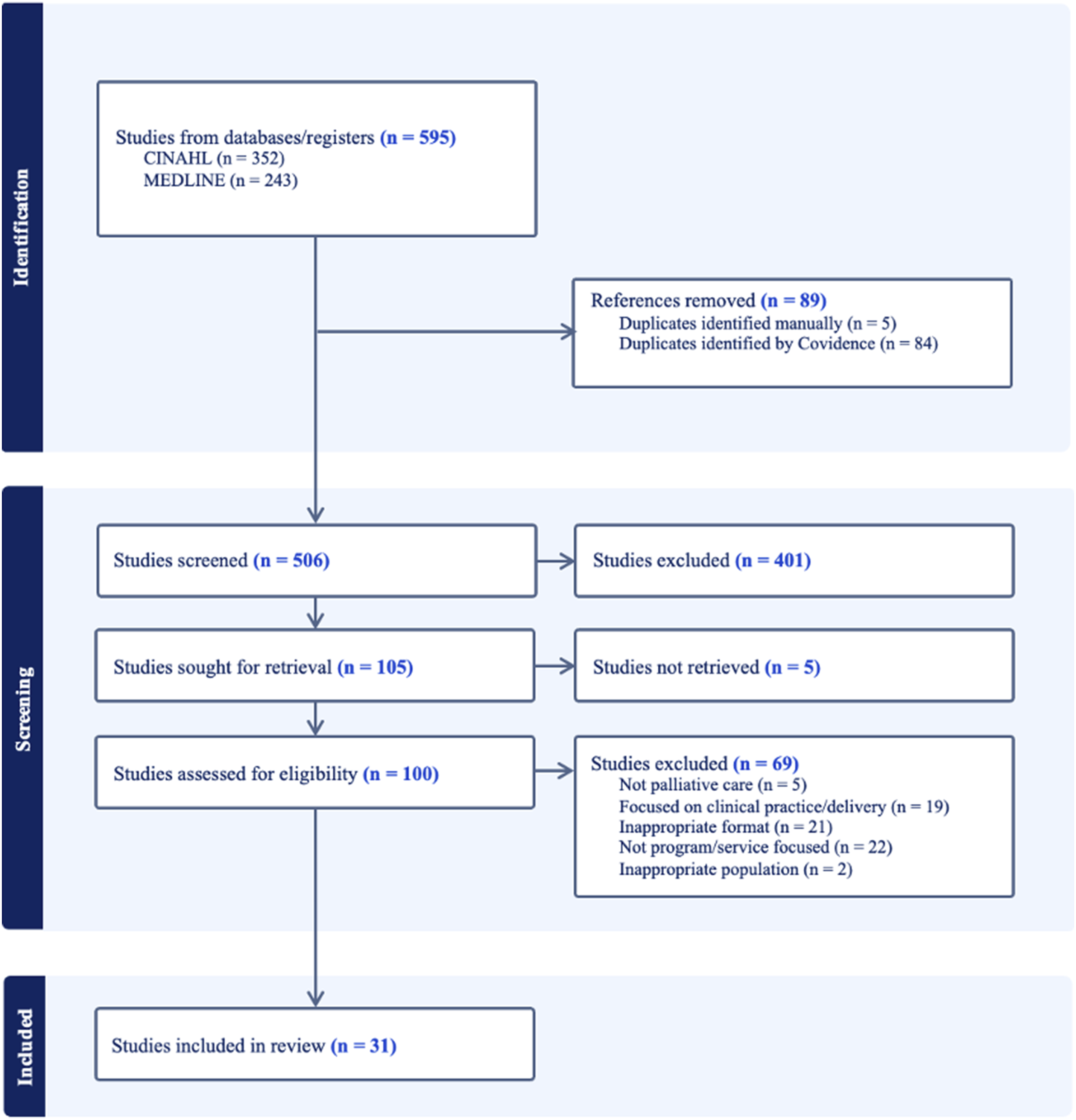
Study characteristics
All retained articles were in English. Nineteen were qualitative,13,15-17,20,21,23-25,29,31-35,37-40 9 were mixed-methods,19,22,27,28,30,36,41-43 and 3 were quantitative.14,18,26 PPC populations mostly consisted of children of all ages.13-15,18,21,22,24,26,28-39,42 Seven articles focused on perinatal populations.16,20,25,27,40,41,43 Two articles highlighted considerations for the transition from paediatric to adult palliative care.19,23
Geographic areas varied, with the vast majority situated in western countries. Ten articles stemmed from the United States,14,16,17,20,21,35-37,41,43 6 from the United Kingdom,13,15,29,31,32,34 3 from Canada,19,24,25 3 from Australia,26,33,40 2 from the Netherlands,22,39 2 from Italy,28,42 1 from Columbia, 18 1 from Ireland, 23 1 from India, 27 1 from Denmark, 30 and 1 from Malaysia. 38 Perspectives sought in these studies included administrators,17,28,29,41 parents and families,23,24,31-35,37-39,42,43 healthcare providers,13-16,19-22,25-27,30,35,36,40 and varied stakeholders.21,34 No articles focused on the perspectives of children themselves.
Challenges to paediatric palliative care
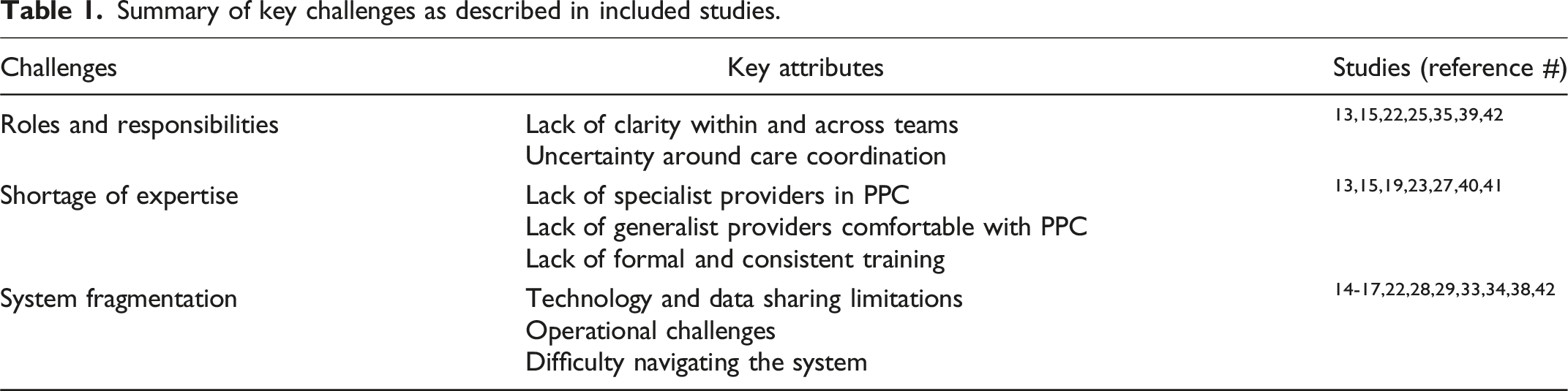
Summary of key challenges as described in included studies.
Unclear roles and responsibilities
A recurring challenge identified in the literature was the lack of clarity around roles and responsibilities between care teams. Typically, many teams work together to care for children with complex and/or life-limiting illnesses (e.g., community nurses, generalists, and specialists). Several studies identified that multiple referrals across different speciality services contributed to a fragmentation of care. 15 In other words, different “specialized” components of care would often operate in siloes, leading to a marked difficulty in delineating responsibilities with shared patients.13,25 The lack of clarity around roles and responsibilities amongst teams was also attributed to uncertainty around care coordination (i.e., knowing the “who, what, and where” of a child’s care). In one study that explored parents’ and providers’ experiences with PPC in non-metropolitan areas, 35 almost all participants named care coordination as a challenge. Consequently, any transitions between care settings or treatment needs were met with difficulty by families. Without a consistent point of contact, parents often ended up taking on additional responsibility to ensure that their child was getting the care they needed.39,42
Shortage of expertise
Throughout the literature, there was a stark lack of PPC expertise available. In part, this stemmed from a lack of specialized providers in PPC. This was especially prevalent for children who needed to rely on adult providers in rural communities or children that “aged out” of paediatric supports.19,23,40 There was also an identified lack of generalist providers comfortable providing PPC. This latter issue stemmed both from a small number of children with palliative needs encountered by generalists and from a broader discomfort with delivering palliative care to children. 13 In some areas, the concept of PPC was still relatively unknown. 27 Other times, PPC as a whole remained a “blind spot” in children’s care since conversations of the possibility of dying were avoided. 15
Some articles proposed that a lack of formal and consistent training was largely to blame for the lack of expertise. Existing educational initiatives were often made accessible only at the expense of substantial time and financial burden. In this way, operational barriers, such as funding and staffing, contributed to a scarcity of opportunities available to providers.13,40
A complex and fragmented system
A significant barrier to PPC access was people’s experiences navigating the health system. This issue was reinforced throughout challenges in individual care coordination and again on a macro-level through system-wide fragmentation and siloing of operations. This was made visible through a ripple effect. In themselves, siloed speciality teams struggled with collaboration and communication. At an institutional level, increased patient volumes accompanied by a lack of synergized resources contributed to many operational challenges around staffing, funding, and cohesive practice.17,23,28,29 At a systems level, technological barriers prevented collaboration due to varied documentation systems that made data sharing difficult.14,29,34 This cumulation deterred families already overwhelmed by their child’s complex healthcare needs15,16,33,38,42 and contributed to diverse barriers to care.
Recommendations for paediatric palliative care
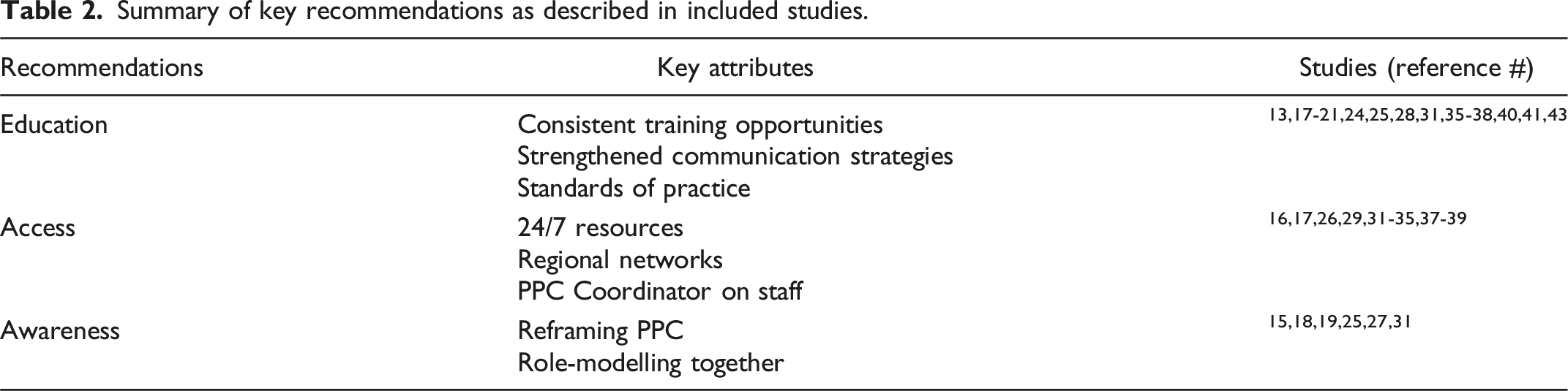
Summary of key recommendations as described in included studies.
Consistent education and standards
Considering barriers in expertise and training, education came as a strong recommendation throughout the literature. In general, research advocated for better and consistent training opportunities for providers,13,18,21,25,28,35,40,41 specifically in areas of pain and symptom management, 21 communication, 18 perinatal care,20,43 and bereavement support.24,31 Given the discomfort providers expressed with having difficult conversations, knowing how to deliver bad news (e.g., terminal diagnosis or declining health status) was consistently highlighted as an educational imperative.18-21,32,38,41 Similarly, education for providers around grief and bereavement support was often neglected and in need.24,31 Recommendations around bedside care focused on the implementation of best clinical standards. To do so, many studies urged for the development and/or integration of standards of practice or quality guidelines for PPC.17,21,36,37,40,43
Streamlining access to speciality services
Many recommendations were made to support better access to PPC services. Multiple papers advocated for staffing a PPC Coordinator to support families in navigating the health system.16,38,39 The creation of care networks was also identified as a valuable support, including regional networks between professionals and organizations26,29; networks of peers, mentors, and “champions” 17 ; as well as peer-support networks for families.32,35 Having specialized PPC providers available in person 37 or by phone 24/7 was essential when families had questions about their child’s care, particularly outside of metropolitan areas, to provide reassurance, options, support, and advice.31,33 According to one study, 34 knowing that specialist PPC was available by phone 24/7 reduced the need to access in-person care out of hours. Telephone lines were also recommended for generalist providers to be able to access expert consultations when needed. 29 Together, combining regional networks and available clinical expertise by phone was identified as a strong strategy.26,29 Additionally, creating a centralized on-line space for PPC resources could also contribute to extending the reach of expertise to more remote areas.26,32,35
Increasing awareness of palliative care
Enhancing the perception of palliative care as a global approach to care focused on quality of life and compassion, was identified as a necessary shift.26,33,39 Palliative care was often described by others as being exclusive to end-of-life care rather than as a comprehensive approach that could be integrated early, even alongside curative and life-prolonging treatments. This misunderstanding could prevent early integration and utilization of key PPC services. For generalist providers and families new to palliative care, this domain was often mentioned as an intimidating idea,15,25,27,31 especially when concerned with neonates or youth transitioning outside of paediatric care.19,23,27 One recurring recommendation was to work towards a deeper awareness of PPC across different spaces to support more timely access.18,25 This would involve debunking myths and increasing awareness of PPC as focused on quality of life rather than solely end of life. Reframing PPC as an approach to care would require all levels and specialities to collaborate in legitimizing and role-modelling this practice. 15
Discussion: Learning from each other’s experiences
This review underscores that many challenges and recommendations for PPC are shared globally. In Canada, their impact is shaped by unique geographic and population-related factors. Canadian families continue to face significant barriers to accessing care, especially in rural and remote regions. A lack of specialized expertise, unclear pathways, and fragmented systems contribute to inequitable access. These challenges are further amplified for underserved populations, such as Indigenous communities, who face additional barriers rooted in geographic isolation and the legacies of historical mistreatment. Addressing these issues demands a coordinated, system-wide approach that prioritizes both equity and accessibility, beginning with early and meaningful partnerships with families, children, and youth from underserved communities.
Large gaps persist in PPC provision across provinces like Saskatchewan, Manitoba, the Territories, and Atlantic Canada, where speciality teams and children’s hospices are few or absent. Recommendations to streamline communication through regional care networks linking urban specialists with rural providers offer a scalable solution. International models like Australia’s state-wide PPC service 26 demonstrate feasibility, while 24/7 virtual care and telephone support 34 could provide timely PPC guidance. National quality standards and care guidelines, like those in the United Kingdom 31 and the United States, 17 which Canada does not currently maintain, could further establish consistent expectations for high-quality PPC and enhance families’ experiences. However, these strategies depend on inter-jurisdictional collaboration and sustainable funding. With Canadian healthcare services funded and managed variably at federal and provincial levels, coordinated government support, policy advocacy, and grassroots fundraising are critical to ensure the long-term viability of these initiatives.
Building capacity among clinicians and organizations is equally critical. Digital tools, such as telehealth platforms and centralized databases,26,29 present opportunities to enhance generalist providers’ competencies and reduce travel burdens for families. In areas where establishing PPC hospices may not be feasible, these technologies can enable local providers to deliver high-quality PPC. Additionally, other innovative models, such as Australia’s “pop-up palliative care” approach 45 —where specialist teams collaborate with local services to meet the needs of families—offer promising alternatives for Canada’s remote and resource-constrained regions. Future efforts should prioritize improved reporting on the availability and quality of PPC programs, as well as research into their growth and evolving needs; including the voices of children themselves in research and decision-making, helping to inform the state and progress of PPC for the very people it aims to serve; and longitudinal studies on system initiatives paired with specific program quality metrics such as access, satisfaction and care outcomes to drive continued learning and improvement.
This rapid review has three main limitations. First, only Medline and CINAHL were searched, which, while strategically selected for their healthcare focus and interdisciplinarity, may have limited the yield. Second, grey literature was excluded to maintain feasibility within the review’s timeline and scope, though such sources might have provided valuable anecdotal insights. Finally, no critical appraisals (optional) were conducted, as the aim was to scope available literature rather than assess effects.
Conclusions
Paediatric Palliative Care is more than a service—it is a commitment to enhancing the quality of life for children with life-limiting illnesses and their families. This review has outlined key areas to strengthen PPC and offered actionable recommendations aligned with Canadian priorities, such as those expressed in its Guiding Principles and Norms of Practice for Paediatric Hospice Palliative Care 46 and Health Canada’s Action Plan on Palliative Care. 8
Despite Canada’s relatively small population and vast geography, it demonstrates leadership in PPC. Organizations like Canada’s Paediatric Palliative Care Alliance, the Canadian Network of Palliative Care for Children, and Children’s Healthcare Canada are spearheading initiatives to improve and develop standards, peer networks, and centralized resources. By addressing system barriers and fostering innovative solutions, Canada can build a more equitable and integrated PPC system—one that supports all children and families at every step of their journey, no matter how short.
Footnotes
Acknowledgements
The authors would like to thank the health sciences librarian at the University of Ottawa for her help developing the search strategy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Health Canada grant (# 2324-HQ-000113).
Ethical approval
Institutional review board approval was not required.