
Abstract
Healthcare is a surprisingly large contributor to climate change, responsible for a significant quantity of global Greenhouse Gas (GHG) emissions. Global commitments to achieve “net zero” health systems, including by the federal government in Canada, suggest a growing need to understand and mobilize capacity for GHG emissions estimation across Canada’s health sector. Our analysis highlights efforts by public sector healthcare organizations in Canada to estimate an increasingly broad scope of GHG emissions, building on longstanding efforts to report or reduce energy-related emissions from facilities. It also identifies why such efforts will not be sufficient. Developing capacity for routine system-wide greenhouse gas emissions estimation can help Canada’s health systems to better understand their progress, including through international comparison. Yet emissions estimation is itself an investment, one that should not displace efforts to reduce the full scope of pollutants from the healthcare enterprise, and to build a truly sustainable health system.
Introduction
As a resource-intensive sector, healthcare is a surprisingly large contributor to climate change, even as growing climate instability threatens health and the safe and effective delivery of health services.1,2 Indeed, healthcare is responsible for approximately 4.6% of Global Greenhouse Gas (GHG) emissions as well as a similar proportion of economy-wide emissions in Canada.3,4
Awareness of these challenges has increased attention to the types of GHG emissions for which healthcare is responsible, alongside growing commitments to drastically reduce the full scope of these emissions. The English National Health Service (NHS) gained international attention with a 2020 commitment to be the world’s first “net zero” national health service, accounting for a comprehensive set of directly and indirectly controlled emissions. 5 Then, as part of the 2021 United Nations Climate Change Conference, COP26, the United Kingdom (the host nation), the World Health Organization (WHO), and other partners introduced the Health Program (now the WHO Alliance for Transformative Action on Climate & Health, ATACH) to seek country commitments to deliver climate resilient and sustainable, low carbon health systems, accounting for emissions from the supply chain. 6 As part of this commitment, countries were to deliver a baseline assessment of the full scope of health system GHG emissions. 6 Ambitious countries were also to define a timeline to “net zero” for these emissions. 7
National commitments to address healthcare emissions have accelerated since. Recent examples include France’s 2023 roadmap, with time-bound objectives to reduce the environmental impact of the healthcare sector. 8 Also in 2023, Australia released the National Health and Climate Strategy, which will establish consistent reporting of healthcare GHG emissions and a reduction trajectory. 9 Other countries have created voluntary commitments to encourage healthcare institutions to reduce their GHG emissions, and more still have decarbonization policies that are not specific to, but still have implications for, healthcare. 10 While high-income countries have particular responsibility for decarbonization, given their elevated per capita emissions, decarbonization efforts are not limited to these countries. Indeed, multiple Low- and Middle-Income Countries (LMIC) participate in the ATACH program, 11 and the Aga Khan Health Services, which manages health operations in several LMIC, was tasked to aim for “net zero” operations as early as 2019. 12
Because of the size and energy intensity of hospitals, there is a common misconception that healthcare’s GHG emissions come principally from the energy required to operate healthcare infrastructure. However, most healthcare emissions are not closely controlled by healthcare organizations. Specifically, under the Greenhouse Gas Protocol that is used to support consistent GHG emissions reporting across sectors,13,14 most healthcare emissions (generally more than 60%) are considered “scope 3.”4,15,16 Scope 3 emissions derive from the products and services that are used to deliver care, including drugs, devices, supplies, equipment, travel, chemicals, and building materials. Thus, the global Health Program commitment from COP26, which included “supply chains,” marked a step-change in decarbonization efforts within healthcare, requiring that healthcare assume responsibility for the full scope of its carbon pollution (Figure 1). Greenhouse gas protocol scopes with healthcare examples.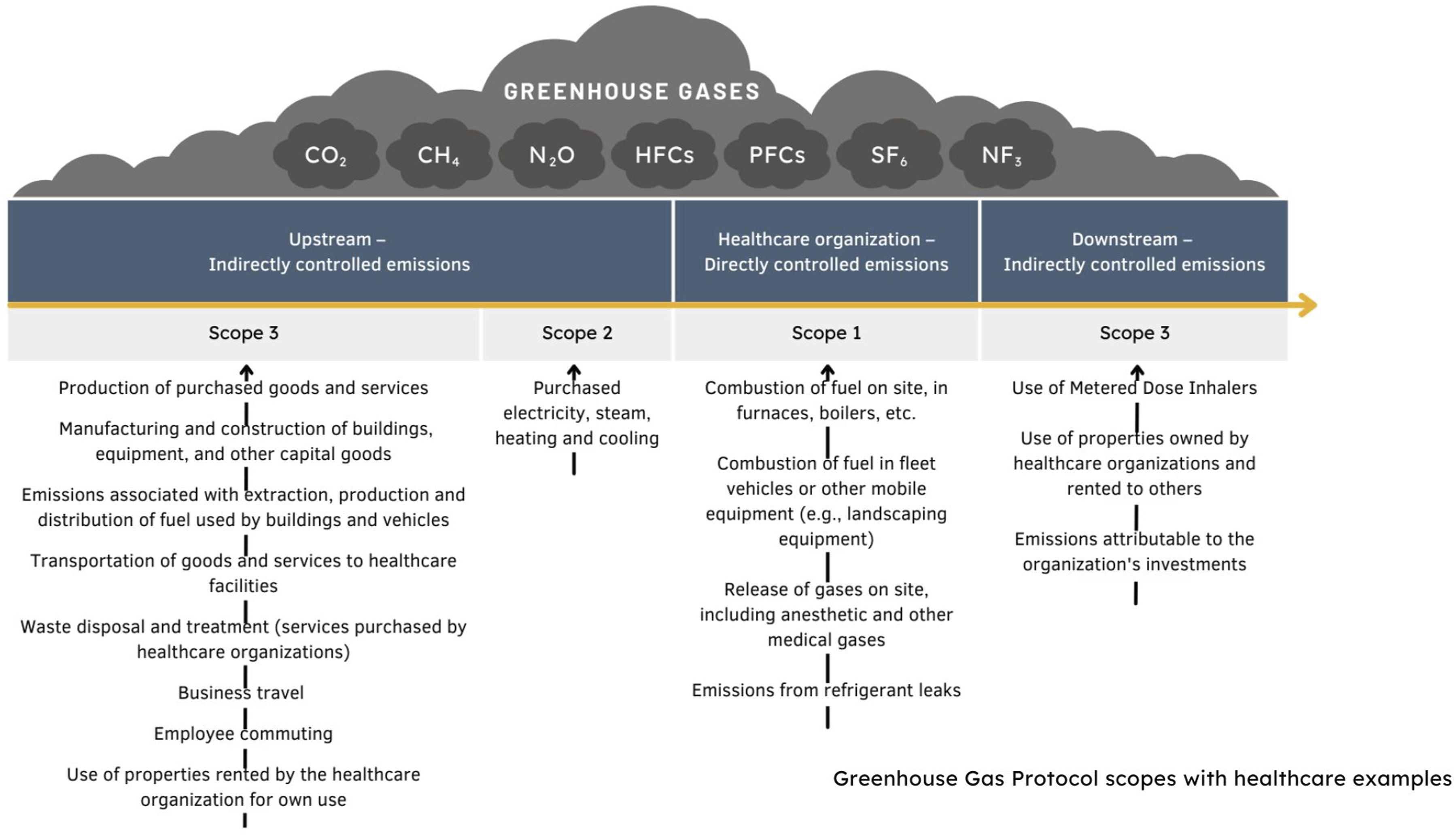
What is the state of health sector emissions estimation in Canada?
In addition to accelerating ambition for healthcare decarbonization, recent global initiatives have brought Canada’s federal government to the table. Indeed, the Canadian government signed on to the COP26 Health Program commitments in the fall of 2021; 17 this commitment was reinforced at subsequent international climate conferences (e.g., COP28). Canada did not originally include a target date for reaching “net zero” health system emissions; 18 however, it appears that a “net zero” target date of 2050 has been recently added to Canada’s ATACH commitments. 11 In a deeply decentralized federation, where federal commitments of this nature do not bind the provinces,19-21 these moves raise important questions about how comprehensive emissions estimation can be achieved across the country.
Our current understanding of Canada’s health sector emissions derives from academic research published in 2018, which identified energy use for public hospital operations, pharmaceutical manufacturing, and the production of medical supplies as the key drivers of emissions. 4 The analysis was based on established models of national economic activity, with emissions estimated from public and private spending on healthcare—an important breadth, as we discuss later.
In countries such as England, which have decarbonization roadmaps for the health sector, such “top down” estimation forms only one component of the total picture. Alongside spend-based estimates that enable whole-system benchmarking and analysis, more granular “bottom up” information about specific activities is also generated, drawing from product, service, or organizational activity information (e.g., litres of anaesthetic gas or fuel used). 16 When combined with data about the GHG emissions associated with each activity, a more detailed picture emerges to guide practice and policy change.
To gain an understanding of the capacity to estimate healthcare emissions in Canada, CASCADES (Creating a Sustainable Canadian Health System in a Climate Crisis)—a knowledge sharing and capacity building initiative funded by Environment and Climate Change Canada—coordinated a pan-Canadian consultative process. Over the course of 2022, CASCADES began consultation with experts responsible for estimating GHG emissions in their healthcare facilities (ranging from single hospitals to multiple facilities owned and operated by health authorities and integrated health and social service centres), eventually leading to discussions and deliberations through a series of workshops with participants from across the country. For information on these workshops and participants, please see the report and implementation-support resource (“playbook”) on the current state of GHG emissions estimation in Canadian healthcare organizations22,23 generated from this work.
In what follows, we briefly synthesize findings from this process, to characterize the current state of GHG emissions estimation in healthcare across Canada, identifying who is positioned to report what emissions. We then review why current efforts will be insufficient to capture the full scope of GHG emissions for all of Canada’s health systems. Finally, we close with suggestions for how these lacunae can be filled, and the importance of looking beyond GHG emissions in the transition toward a more sustainable health system.
Who is reporting what emissions?
A focus on facility-based and energy-related emissions
Most efforts to monitor, report, and mitigate GHG emissions in healthcare have been related to facilities, with responsibility for this work residing in facilities management departments. Indeed, efforts to reduce costs from energy use, as well as regulatory requirements related to GHG emissions and energy, have encouraged large healthcare facilities (and some small ones), to estimate their energy-related emissions. Thus, emissions from purchased energy (e.g., electricity and steam—“scope 2”) and direct emissions from on-site or owned buildings or equipment (e.g., gas boilers or fuel for vehicles—“scope 1”) are routinely estimated across much of the country.
Requirements to report GHG emissions from healthcare play some role in this but are variable across the country and limited in scope. The federal Greenhouse Gas Reporting Program covers scope 1 energy-related emissions and targets high emission facilities—thus, a small number of healthcare facilities report under this program. 24 Provincial GHG reporting programs also target facilities with high scope 1 emissions, with different Carbon Dioxide Equivalent (CO2e) thresholds,25-29 which may have implications for a small number of healthcare facilities. Finally, some provinces require healthcare organizations to report GHG emissions as broader public sector entities, not limited to high emitting facilities. In Ontario, these inventories cover energy-related emissions 30 and in British Columbia, a broader set of emissions are also reported, including those from buildings, purchased energy, vehicles, and the production of purchased paper. 31
Interest in GHG emissions beyond the energy baseline
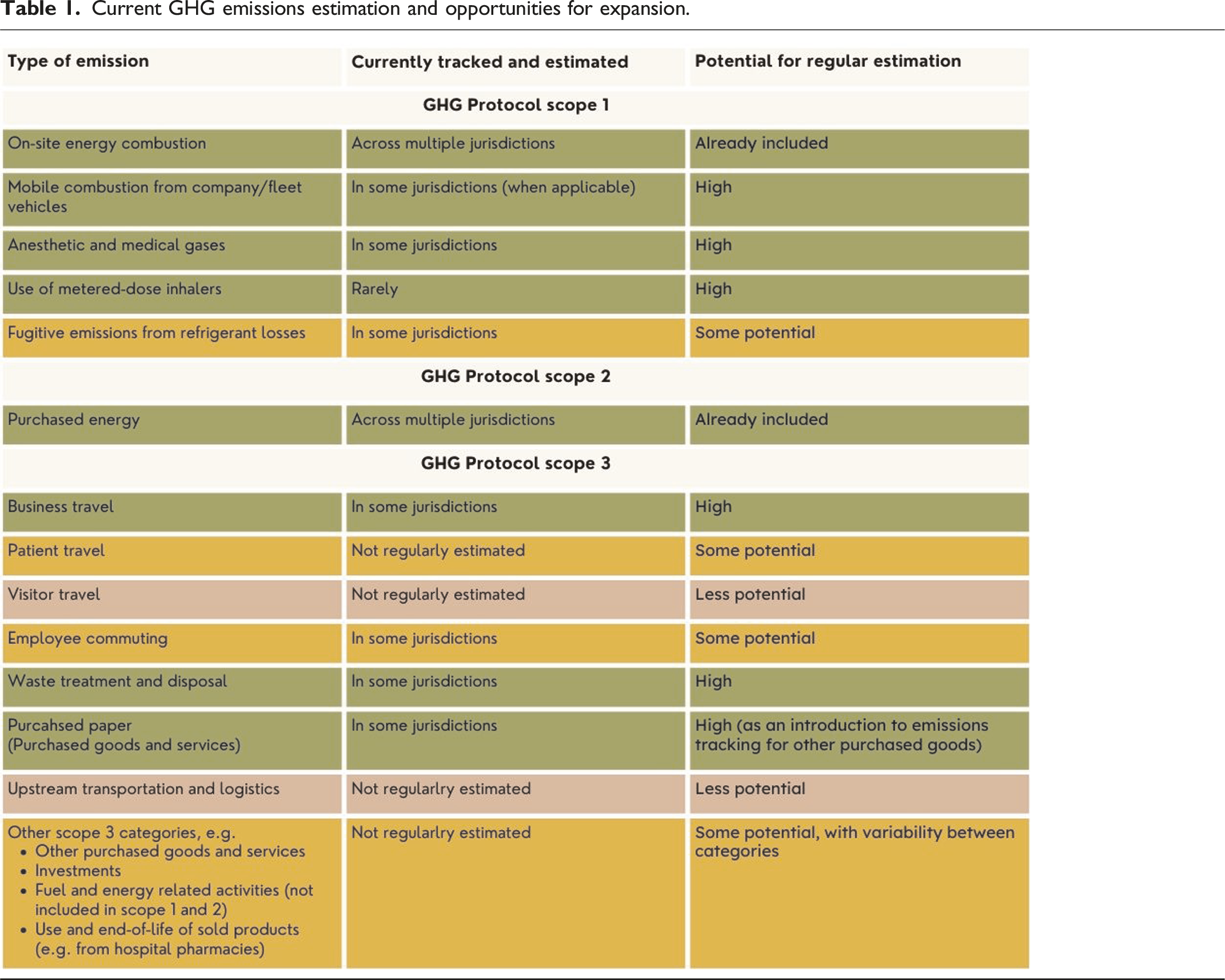
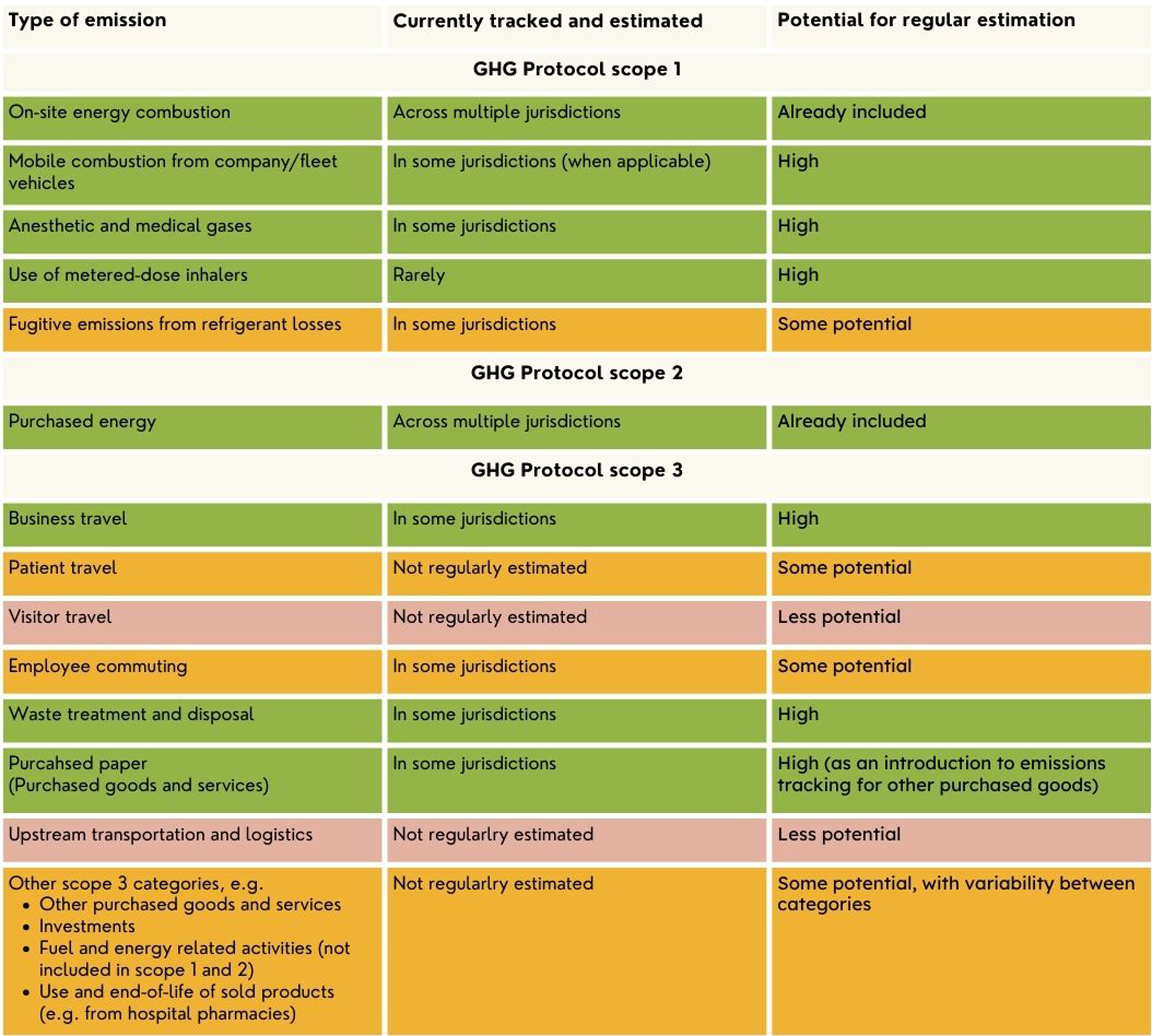
Current GHG emissions estimation and opportunities for expansion.
Extending routine estimation to a wider set of emissions, particularly those in the supply chain, would be challenging and potentially less worthwhile, given limitations in available data, and the time intensity of data gathering. Some organizations have nonetheless completed, or are working toward, more detailed GHG inventories. Reasons for doing so vary, and can include their potential to drive engagement and commitment to change across the organization,34,35 to identify priority areas for reduction,36,37 or as baselines for ongoing monitoring and to guide roadmaps and other plans for GHG emission reduction.38,39
Can current efforts capture the full scope of emissions?
No matter how ambitious different healthcare organizations are becoming about estimating their GHG emissions, no care delivery organization can assess the full scope of health system emissions. This limitation arises for three main reasons: first, because not all facilities are included within emission estimation efforts; second, because not all emissions are facility-based; and third, because not all emissions are under the remit of a public authority (Figure 2). Gap analysis—tracked and reported emissions.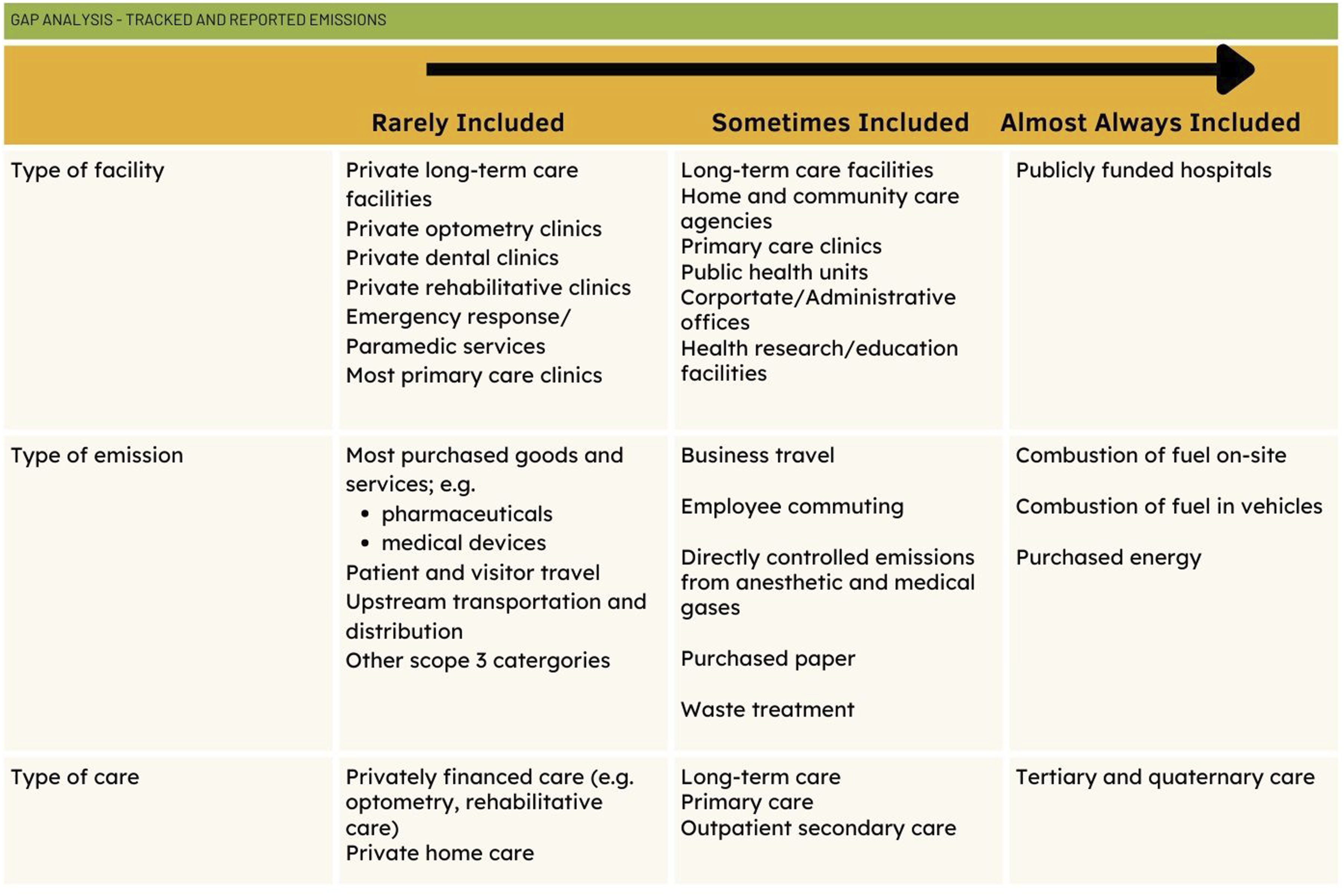
The first challenge arises from differences in healthcare organization across the country, which leads to the routine estimation of emissions from different kinds of facilities. In provinces like Ontario, healthcare’s GHG emissions are estimated by independent hospital corporations, some of whom house non-hospital services such as primary care clinics, long-term care facilities or research institutes. However, many of Ontario’s small facilities and non-hospital healthcare facilities are not captured in these estimates. Outside Ontario, the relevant public authorities are accountable for a wider set of healthcare emissions. In most provinces, health authorities are responsible for estimating emissions, and they typically include public health, community health services, and some long-term care facilities in their remit, and may include some primary care clinics, thus incorporating these facilities within their estimates. In Quebec, the main responsible actors are the integrated health and social service centres (organized as CISSS/CIUSSS), which are responsible for a broad array of health and social service facilities.
The second reason for partial estimation is that a focus on facility-based emissions leaves many emissions unaccounted for. This is so even in provinces with a wider network of facilities covered by the responsible authorities, and even if these public authorities estimate the full scope of emissions for which there are financially accountable. Consider important emissions associated with outpatient drugs, devices and supplies. Pharmaceuticals are estimated to account for approximately 25% of emissions in Canada 4 and 30% in England. 16 While some of these are procured by and administered within hospitals, most are prescribed to people in the community and would not be captured in facility-based emissions estimates, no matter how expansive.
The third reason for partial estimation of healthcare emissions is that not all such emissions are publicly managed or financed. Services that are secured in the community—beyond the remit of facility-based emissions estimation—but publicly financed or managed might be estimated by provincial and territorial drug, device, and home care plans. Yet services for which public authorities are not responsible would remain unaccounted for. This includes privately financed emissions such as most optometry care, dental care, or community-based rehabilitative care as well as private retirement homes and home care. It might be argued that such emissions are not the responsibility of public authorities. Yet privately financed emissions “count” in efforts to deliver a “net zero” health system, both because they manifestly occur, and because privately financed services have the potential to either increase or decrease emissions from publicly financed services. 40 There may be different financial budgets—public and private—but there is only one carbon budget.
Conclusion
For Canada to meet the commitment to create a “sustainable low carbon health system” made at COP26, a baseline assessment of GHG emissions, which includes supply chains, is required. 6 Currently, capacity to routinely estimate healthcare’s GHG emissions in Canada resides primarily within facilities and for energy-related emissions (scope 2 and some scope 1, see Table 1). This capacity can be extended and there are implications for health leaders. Indeed, there is opportunity to learn from organizations that have already started to estimate the full scope of emissions for which they are financially accountable (across scopes 1, 2, and 3). Ultimately, however, there is a need for system-wide emissions estimation, to account for the variable ways that healthcare is organized across the country, the critical emissions that take place outside healthcare facilities, and the many emissions for which public authorities are not financially accountable.
There are many opportunities to close these several gaps. First, healthcare organizations across the country can be supported in their efforts to do this work through standardized and shared approaches to data collection and analysis. No standard approach to estimating GHG emissions in healthcare exists, leading to variation in how emissions get tracked and reported. Health leaders can prioritize increasing methodological consistency to help with benchmarking efforts between organizations and jurisdictions. Efforts to establish an organizational baseline will also support year over year comparisons. Activity and financial data are already collected across jurisdictions in a standardized way through the Canadian Institute of Health Information, 41 and this could support GHG estimation. A majority of GHG emissions are in the supply chain, but limited information on emissions from suppliers makes these estimations difficult. Working with policy-makers to require suppliers to provide standard data on their emissions would increase the availability of information while removing the burden of onerous estimation efforts for healthcare organizations. Existing work to identify targets for suppliers with respect to their GHG emissions 42 can be built upon, and ATACH, through its Supply Chains Working Group could provide additional support. Health leaders can also include emissions criteria in their supplier selection processes, third party risk management programs, and supplier performance/relationship management programs—though data quality and implementation issues warrant careful attention. To capture the activities beyond the financial purview of health authorities, hospitals and other large facilities, provinces, and territories will need to engage. They are well placed to generate estimates of emissions from outpatient and home and community-based care that are publicly financed, supplemented with information about emissions associated with privately paid-for services, so that system-wide estimates can be comprehensive.
While these efforts proceed, it is important to recall that GHG emissions should not be the only environmental metric that healthcare tracks and manages. Attention to GHG emissions does not necessarily reduce other environmental and health harms associated with the healthcare sector. 43 Sustainability metrics should be linked to reporting on healthcare quality and performance and include metrics like quantifying health-damaging pollutants and reducing overuse. 44 Resources on different approaches to embedding sustainability in organizational strategy and performance, including those from CASCADES, 45 can provide direction. Even when GHG emissions cannot be readily estimated, emphasizing reductions in purchasing and consuming, and supporting innovations in care delivery, can lead to decarbonization. Health leaders can create a culture of sustainability in their organizations, set meaningful targets and pursue sustainability in system enablers (like infrastructure and waste) as well as through innovations in care delivery. Ultimately, leaders must prioritize opportunities to pursue mitigation and adaptation in the same action, in efforts to build “a health system that improves, maintains, or restores health, while minimizing negative impacts on the environment and leveraging opportunities to restore and improve it, to the benefit of the health and well-being of current and future generations.” 46
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CASCADES (Creating a Sustainable Canadian Health System in a Climate Crisis) is a multiyear capacity building and knowledge sharing initiative funded by Environment and Climate Change Canada.
Ethical approval
Institutional review board approval was not required.