
Abstract
Healthcare systems in Canada are under pressure and require change—the status quo is no longer fit for purpose, if it ever was. Innovation is often held up as a cure for what ails us, but shiny new things or novel technologies alone have not been enough. This article will explore the concepts of differentiation and integration as being important drivers in the evolution of living organisms, ecosystems, and complex human organizations. The implications of this deep pattern of systems change are essential to understanding the roles of specialization in medicine, and optionality in primary care. Specifically, overspecialization without attention to the principles of healthcare integration can lead to fragmentation of care and worse patient outcomes. Finally, this article will describe some practical examples of system integration as innovation in the form of better public health and care delivery connections, health homes, and community care coordination centres.
Introduction
Differentiation and integration: Two necessary drives in the evolution of systems
Life has evolved from single cells to multi-cellular organisms to multi-subsystem plants and animals. Similarly, complex human systems (healthcare, education, corporations, global socio-economic systems) have followed a similar pattern; first differentiating unique parts with new and distinct roles which subsequently integrate to create a greater whole that is more fit for purpose.1-3 This article will explore the implication of these deep patterns to the improvement of healthcare systems.
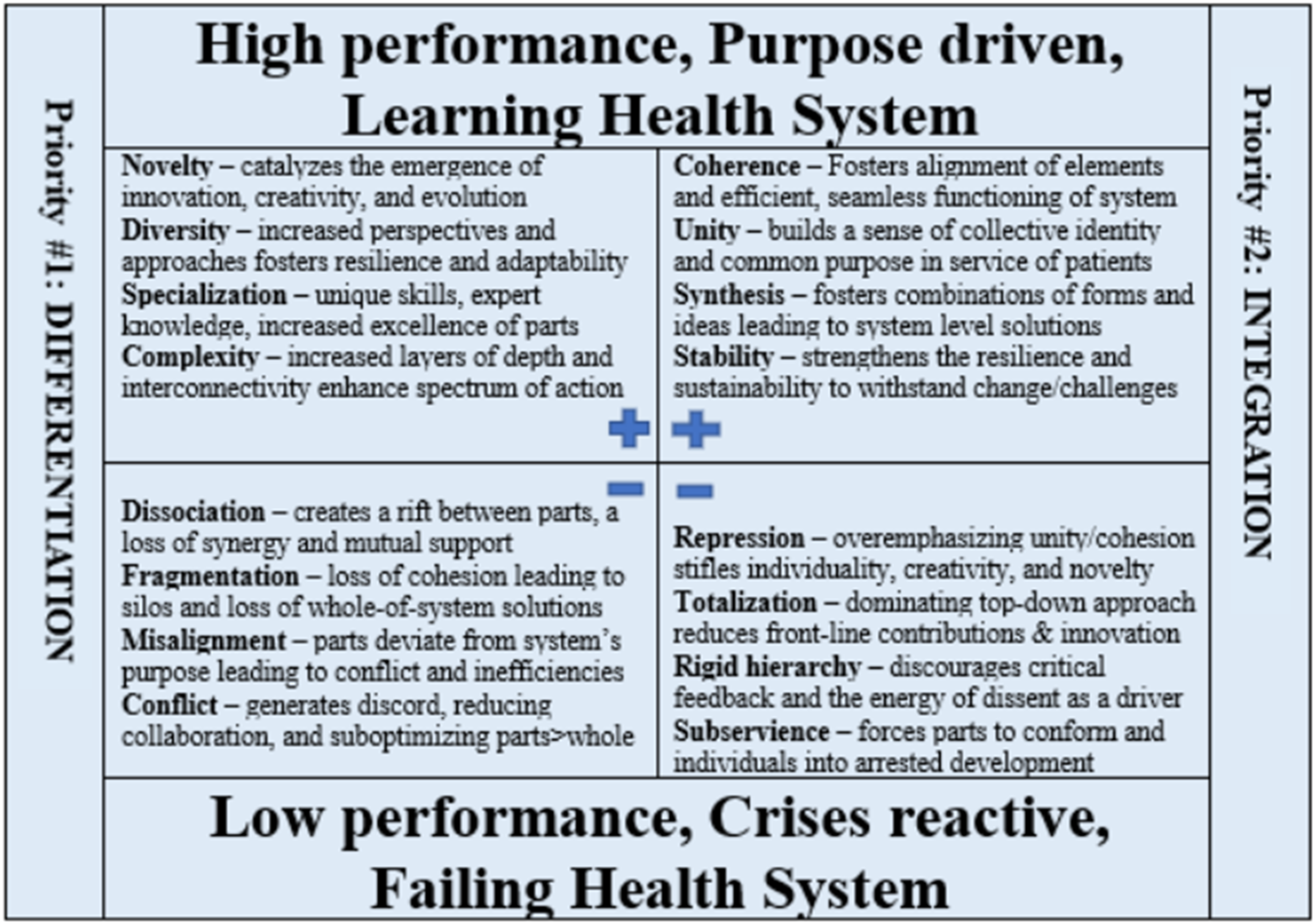
Differentiation is the drive to create novelty and uniqueness, leading to individual parts within a system. Integration is the drive towards synthesis of these diverse elements into a cohesive and functioning whole. Both processes are essential for evolution in systems. Whereas too much of one, at the expense of the other, is problematic. Unbalanced differentiation leads to fragmentation and dys-integration in systems. Unbalanced integration leads to homogeneity and stagnation. 4
20th century: The era of differentiation/specialization in modern medicine
Differentiation and specialization in the sciences over the 18th and 19th centuries contributed to scientific progress in biology, chemistry, biochemistry, pharmacology, and a better understanding of the pathophysiology of disease in humans. 5 This eventually leads to specialization in medicine across the world.6,7 The influential Flexner report from 1910 called for a more scientific underpinning to the advancement or research and education in medicine. 8 Focusing our intellectual energies on narrower aspects of the human body leads to breakthroughs in understanding and eventually to breakthroughs in treatment modalities.
The first speciality recognized in North America was ophthalmology which created its own board and assessment/certification process in 1917 to assure standardization in competencies and skill by its practitioners. By the 1970s, 20 separate specialities were recognized in the United States. In Internal Medicine alone, there were 20 new subspecialities which emerged between 1940 and 2010. 9 As of today in Canada, the Royal College of Physicians and Surgeons recognizes 79 disciplines including 29 specialities, 34 subspecialities, 3 special programs, and 13 areas of focused competence. On top of the speciality of Family Medicine, the CFPC currently also recognizes 8 certificates of added competence.
There are many factors contributing to the perceived need to specialize and subspecialize. Deeper dives into discovery and the creation of knowledge beget an explosion of facts and models for practitioners to keep up with, and we just can’t keep up with everything, so we narrow our interests. Other socio-economic/human motivational factors have also contributed, such as perceived prestige and recognition, the growing relativity gap between specialist and generalists, fee-for-service remuneration models favouring procedure-based specialities, and lifestyle considerations. 10 Humans create structures which then create us.
No doubt, many incredible and life-saving advancements in medicine and public health occurred during the 20th century. No previous era has seen as much evolution in patient care leading to such improvements in population outcomes. Arguably, much of this improvement can be attributed to the trend towards specialization and subspecialisation in medicine during this time, and the impact that had on seeding research and novel approaches to patient treatments and disease prevention.
Too much of a good thing: Does overspecialization contribute to the fragmentation of care?
By the turn of the last century, however, concern was growing that overspecialization was contributing to an overemphasis of the bio-medical model, and an underemphasis of the role that the social determinants of health played. Further, there seemed to be a decline in whole patient care and a fragmentation of our care delivery systems.10-13 Even today, ageing patients with multiple chronic diseases receive suboptimal care overall, and their uncoordinated treatment plans can result in redundancies and inefficiencies.14,15
An oft repeated concern of patients when they are admitted to hospital, especially to a tertiary care teaching hospital, is that they don’t actually know who is looking after them.16,17 One specialist may have admitted a patient, another may have operated, and others still may be managing various issues that arise during their stay: an irregular heartbeat, difficulty urinating, an infected wound, and/or a swollen leg and shortness of breath. After factoring in several layers of learners and multiple handovers to oncoming teams over time, the number of physicians “looking after” a patient can be staggering. Yes, clarity of responsibility and communication through Most Responsible Physician (MRP) polices and validated care transition tools can reduce the chance of error or oversight, but the problem remains. Certainly, the lay literature is filled with thoughtful commentary on this concerning trend.18,19
Unfortunately, with the growing and ageing population, and the increasing pressure on individual programs to manage the capacity of “their own” beds/clinics, the trend towards specialists defining themselves as much by what they don’t do, rather than what they do; fewer complex patients fit nicely into single system (or narrower) speciality and subspeciality parameters. There are more and more obstacles and “gatekeepers” contributing to an increasingly labyrinthine system—further compromising patient care. This recent editorial headline captures the issue succinctly: “The patient who is no one’s problem is society’s nightmare.” 20
At a system design level, the overall lack of coherence and system performance accountability can favour silo (or subsystem) suboptimization over whole-of-system goals, like the Quintuple Aim. There is a risk that one program will show “efficiencies” and balance its budget by deferring its own queue to downstream programs.21-23 Governance and leadership hierarchies and financial incentives and budgets arise to support specialized departments, divisions, and programs which, in turn, reinforce these increasingly siloed structures. Humans create structures which then create us.
Unintended consequences: Does primary care optionality contribute to compromised continuity of care?
A more recent phenomenon, potentially related to overspecialization in healthcare, is the decline and fall of family medicine in Canada.24,25 Accessing primary care is increasingly challenging for large segments of the population. As a response to this many jurisdictions have created multiple “primary care” options. From walk-in clinics to mobile clinics, to transactional retail virtual care, to expanding the scope of many clinicians in other “unattached” environments, primary care is advertised to be more available than ever.
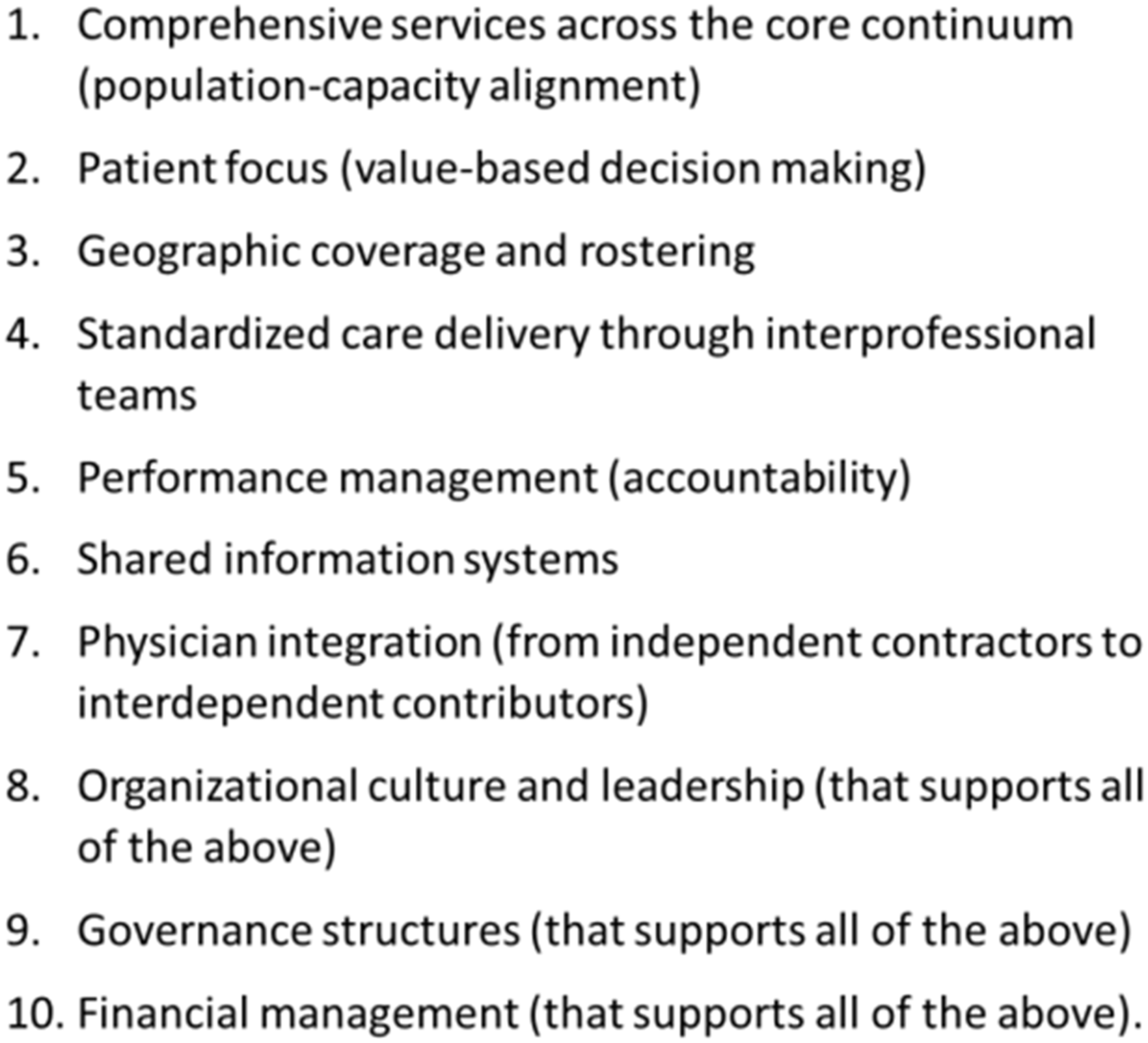
Optionality in complex adaptive systems is a good thing. It, along with surge capacity, and many other factors can contribute to resilience in healthcare systems. 26 That said, if options are implemented haphazardly and without following the 10 key principles of successful health system integration (see Figure 2), this may cause more harm than good.27,28
In the United States, allowing a free market approach to filling gaps in the provision of primary care has led to “the rise of the middleman” and to what has been called a Frankenstein system—an inelegant and clunky monster. 29 This Scandinavian study used a different metaphor for a similar phenomenon. 30 Their investigation looked at what happens when private corporations are allowed to bill public funds to create healthcare options that are not associated with the more traditional Health Home model or integrated with hospital based clinics. This led to what they call a tapeworm economy where profits were syphoned from the system and not reinvested into broader improvements of the whole.
For an individual patient, this fragmentation also leads to poor continuity of care over time and worse outcomes.31,32 A 1984 randomized controlled trial published in Journal of the American Medical Association (JAMA) demonstrated significantly better outcomes in the cohort assigned to continuity of care guided by a single family physician than the cohort managed by a broader range of clinicians in a primary care clinic. 33 The findings were so significant that it was felt to be unethical to repeat a Randomized Controlled Trial (RCT) where patients were randomized to a discontinuity of care arm. Other cohort studies and meta-analyses have also demonstrated the population outcome benefit to care coordination over time and having a relationship with your treating physician.34-36 Along the same vein, a recent large study out of Ontario compared virtual urgent care provided by a patient’s own family physician versus being provided by a transactional retail virtual care app. 37 They found that the transactional retail virtual care patients were 66% more likely to be subsequently sent to the Emergency Department (ED).
In these challenging times, there will be many conflicting opinions on the best way forward.38-42 A diversity of opinions can create the potential energy to drive change at a systems level. Pilot projects and a broad range of experimentations is not the problem in complex healthcare systems change, in fact they are a necessity. The problem is not properly evaluating the impact of implementing pilot projects on the hypothesized outcome.43,44 Further, each project or “part” experimentation/innovation must be considered in the context of how it contributes more broadly to the Quintuple Aim at the whole-of-system level now, and over time (in light of potential unintended consequences). Therefore, the most important challenge we must meet is creating learning health systems as we move forward with novel approaches. 45
21st century medicine: The promise of integration in healthcare systems?
In 1990, Boyers published the promising white paper entitled Scholarship Reconsidered. 46 It argued that universities, for the sake of the societies they served, needed to broaden their understanding of scholarship and value more than the traditional research (scholarship of discovery) and education (scholarship of teaching) publish or perish mantra. This admonition was also motivated by the recognition that overspecialization in many fields was leading us to know more and more about less and less to the detriment of progress and pragmatism.
To that end, Boyers articulated the importance of the scholarship of application in which these questions were asked: “How can knowledge be responsibly applied to consequential problems? How can it be helpful to individuals as well as institutions?” And further, “Can systems problems themselves define an agenda for scholarly investigation?” He also introduced the scholarship of integration in which “we underscore the need for scholars who give meaning to isolated facts, putting them in perspective. By integration, we mean making connections across the disciplines, placing the specialities in larger context, illuminating data in a revealing way.” It’s not hard to see how medicine as an applied science, and healthcare writ large, so in need of integration, could take up this new call to action. Unfortunately, it’s debatable whether the promise of Boyers has been met.
In 2010, there were many commentaries written in medical journals on the 100-year anniversary of the Flexner report. Donald Berwick wrote about preparing the medical students of the 21st century for “the new public interest.” 47 He suggested that physicians must learn to navigate and continually improve the complex systems in which healthcare is delivered, in service of their patients. Mastering their own speciality and withdrawing into their own silo was not good enough. They must understand the scientific bases of system performance and take an active role in integrating care across subsystems, disciplines, and sectors. Since then, the development of a curriculum in Health Systems Sciences has helped to forward that agenda, but again, the promise is largely unmet. 48
In Canada in 2015, the federal report Unleashing Innovation: Excellent Healthcare for Canada was published. 49 Chapter 6 of that report was entitled: Integration and Innovation: The Virtuous Cycle of Seamless Care. The authors compellingly argued that Canada does not have an integrated healthcare system (for many reasons) and that creating one must be a priority. In fact, they recommended, integration is innovation, and the federal government should enable system integration through strategic investments. Given that health is a provincial responsibility, provincial governments should also create the conditions for the emergence of integration through better legislation, incentives, leadership, governance, and accountability.
If the 20th century was the era of differentiation/specialization in medicine, the 21st century (or maybe even just the next decade given the urgency of our current crises) must be about integration. And as we move forward, we must optimize the balance of the two as per Figure 1. It is also important for system leaders to recognize that “regionalization” is not integration.
50
Merging organization charts, combining budgets, and/or sharing procurement practices is not integration in and off itself. The principles as outlined in Figure 2 must be achieved. Furthermore, integration can occur under many different governance structures ranging from “decentralized” to “centralized.” This modified polarity management map depicts the risks and benefits of both differentiation and integration, and why balancing the best of each, while avoiding the worst of each, is the key to system evolution as from deVos.
4
The ten key principles for successful health system integration as modified from Suter et al.
27
Integration as system innovation: Examples
System innovation (as opposed to part or thing innovation) is defined as “a new systems-based approach… that looks more broadly at how the whole system is organized and aims to change the way the parts are interrelated and organized to realize new outcomes.” 51 Given the strain of COVID pandemic place on our systems, calls for system resilience and more integrated care delivery systems grow stronger.52-55 Here are three practical examples that will catalyse broader change if prioritized.
Public health and care delivery
Like the proverbial frog swimming in the pot being slowly brought to boil, the primary/acute/continuing care delivery systems are immersed in the socio-economic determinants of health and other emerging population health issues. Yet there are few connections between public health and care delivery systems. 56 In Canada, federal-provincial governance structures, balkanized budgeting, and entrenched cultures perpetuate the divide. In the United States, the COVID tragedy has prompted reflection on the need for better collaboration and a narrowing of the distance between the two. Five leading organizations in the United States have created the Common Health Coalition with four priorities—C.A.R.E: (1) coordination between healthcare and public health, (2) always-on emergency preparedness, (3) real-time disease detection, and (4) exchanging data to advance health equity. 57 The Public Health Agency of Canada has recommended similar priorities but the lack of systems integration (and the lack of political/operational will) remains an obstacle. 58
Health Homes
Population-based, regionally rostered, multi-disciplinary, same-day/next-day accessible primary care homes—or centres—are also hubs unto themselves. 59 The metaphor of being the foundation of a healthcare system might work if modern healthcare were a building (static, linear cause and effect, and clear boundaries), but it’s not. Healthcare systems are more like an ecosystem or a complex network (dynamic, inter-dependent cause and effect, fuzzy, and expanding boundaries) and in that context, foundations quickly lose their footings. Health Homes provide essential and direct patient care while also functioning as keystone connectors or nodes within an integrated network, with the capability to evolve with the changing ecosystem. The physicians, nurses, paramedics, nurse practitioners, physician assistants, pharmacists, occupational therapists, physiotherapists, psychologists, social workers, dieticians, and/or others coordinate care at the individual level, and also strengthen connections in the system with the recommendations for ongoing care plans from specialists, and sometimes multiple specialists. Health Homes are also best suited to support the integration of patient needs from prevention to primary care to urgent, continuing, and long-term care.
IMPAC2T Centres
Another adaptive response to the strain of the pandemic on “normal operations” in our systems was the development of care coordination centres, (care coordination in delivery systems at the community/population level).60-62 The concept here was to leverage the experience, technology, relationships, and systems savviness of the ambulance dispatch centre, or Emergency Medical Service (EMS) communications centre, to play a bigger role in the real-time assessment (right patient), coordination (right care and right time), and potentially treatment/transport (right medium, right team, right transport vehicle, and right destination) of 8-1-1/9-1-1 calls and interfacility transport requests. An IMPAC2T (Integrated Medical/Primary-health Assessment, Care Coordination, and Treatment) Centre would have five areas to support (see Figure 3). The five components of the healthcare system to be supported by an IMPAC2T Centre. The first (red) is the response to emergent and urgent 9-1-1 calls. This includes the traditional lights and sirens response of ambulances and transport to emergency departments, but not all of these calls require this level of activation and this is where some secondary triage comes in.
63
Some calls may warrant a single paramedic response and assessment followed by non-traditional transport means to the ED, or an integrated urgent care clinic, or healthcare home appointment the next day.
64
Sometimes the needs of the patients may be met safely by integrated virtual care options.
65
The second (yellow) grouping of care coordination would include direct to alternate (non-ED) pathways. This includes direct to specialists or subspecialists clinics, if the patient meets pre-agreed criteria. The third (green) area that a coordination centre could direct calls to, or book appointments with, is the regionally rostered, multidisciplinary Health Home.34,59,66 The fourth (blue) area is supporting care after an ED visit or hospital admission. Home hospital programs have showed some promise in safely reducing hospital admissions.67,68 Lastly (purple) is the interfacility care coordination role. One-way funnels from the periphery to the central tertiary care centre have been replaced by a network model, where patient and information can travel in both (or many) directions.
69
Sometimes, peer-to-peer virtual care support allows for patients to stay in their home hospitals.
70
Sometimes this helps in pre-transport stabilization and most appropriate vehicle/team and destination decisions.71,72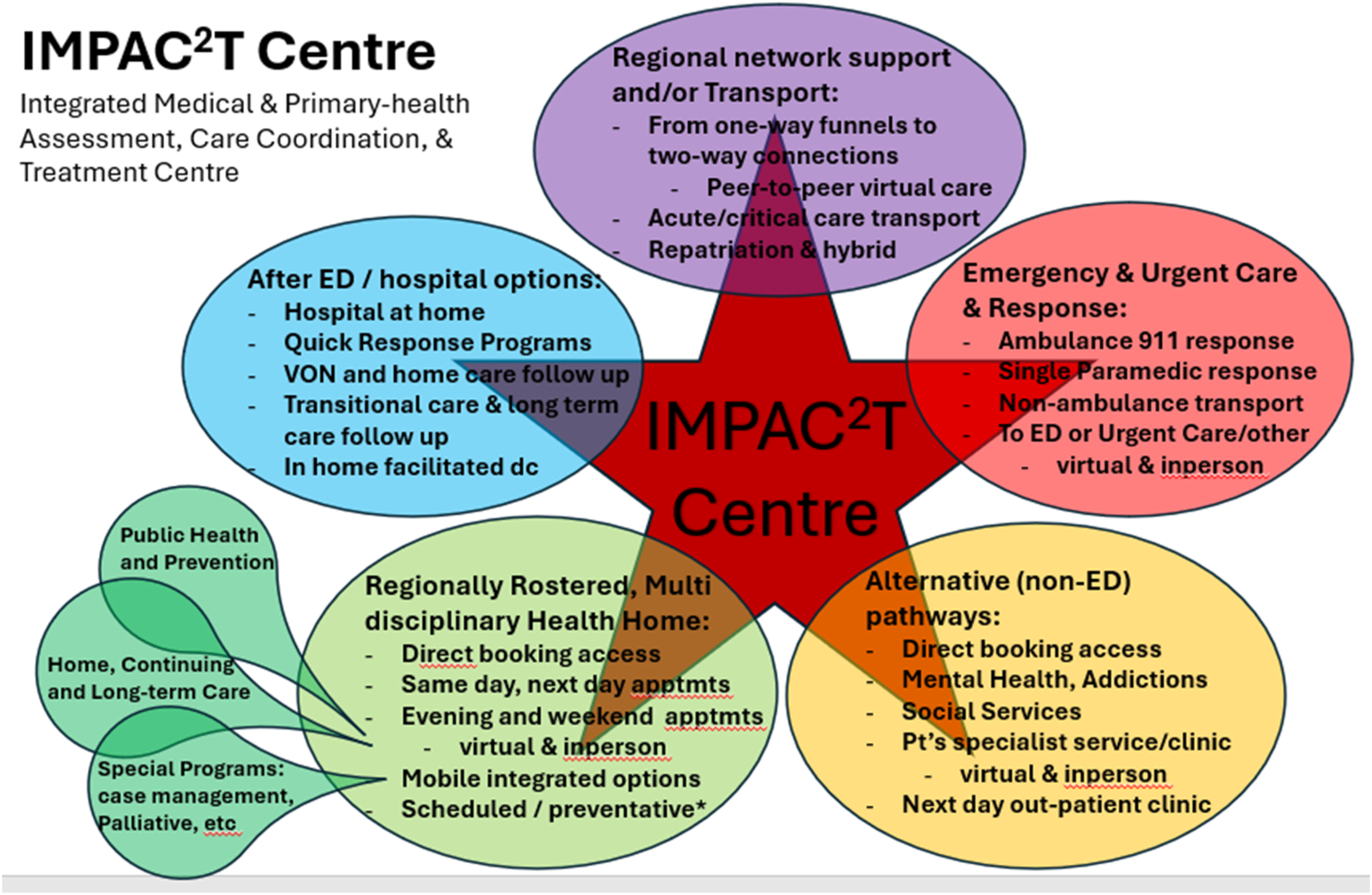
Conclusion
Overspecialization in medicine, and the well-intentioned but uncoordinated development of primary care “options” in care delivery, without Health Homes, can lead to system fragmentation and poor continuity of care. The issue should not be framed as a specialization vs. generalization problem, but rather the question is: how do we best integrate specialist and generalist care to improve outcomes for the patients/populations we all serve? Integration as innovation is an important concept required to improve system performance. In healthcare system redesign we must put more emphasis on our shared goals across sectors and programs of care and minimize the suboptimization of silos and parts. Given the interconnectedness of healthcare, we must also be intentional with our pilot projects and process changes. Strategically focusing on key relationships in the system can catalyse whole-of-system improvements. Most importantly, we must evaluate our experiments and innovations against whether they improve population outcomes and patient experience in an equitable, workforce-supporting, and cost-effective way.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.