
Abstract
Canadians face prolonged waits for primary care, specialist care, hospital care, elective surgery, and advanced imaging relative to peer countries. A root problem is unclear queue management expectations. If programs have no mandate to provide timely care, the intuitive approach to demand challenges is not to innovate and improve, but to block access, create a queue, and force patients elsewhere. Patient care accountability frameworks define program expectations and accountability zones, clarifying that every patient has an accountable healthcare home and every program has a population (accountability zone). Program accountabilities include timely patient assessment and disposition; budget, space, and nursing care for program patients; and contingency plans for surges and queues. Accountability frameworks are an evolutionary stressor that would drive strategies to expedite appropriate care in the right place, to move patients out of queues into care. This article discusses accountability, accountability frameworks, and accountability strategies to improve system-wide access.
Introduction
Canadian healthcare is characterized by waiting. Canadians wait weeks or months for advanced imaging, and months to years to have a joint replaced or get a family doctor. Canada provides poor access to primary care, specialist care, hospital care, elective surgery, and advanced imaging relative to other Organization for Economic Development (OECD) countries.1,2 Queueing, wait times, and care delays are all manifestations of access block, which is the number one problem for Canadians requiring healthcare.1,3,4
Access blocks in any program have a domino effect, compromising other components of an interdependent system. 5 Alternate Level of Care (ALC) patients waiting for Long Term Care (LTC) or rehabilitation lie in hospital beds for days or weeks, often deconditioning or cognitively deteriorating as they do.6-8 Resulting hospital bed blocks delay medical admissions and cause surgical cancellations. 9 Admitted inpatients unable to access hospital beds are held for hours or days on Emergency Department (ED) stretchers, preventing the inflow of emergency patients with serious illness or injury. This leaves ambulance crews lined up in congested ED hallways, unable to offload acutely ill patients or respond to emergencies in the community. 10 At every level, providers assume that someone else will deal with the waiting patients. Access blocks permeate the system, compromising patient outcomes, system efficiency, and cost.5,11
Access block has many causes, including poor system integration, limited bed capacity, staffing shortfalls, care maldistribution, process inefficiency, and an ageing population with rising care needs.12-14 A critical root cause seldom discussed is the absence of healthcare accountability frameworks and a lack of access and queue management expectations. Logically, all programs should strive to assure timely care for their patients. They should also have surge and queue management contingency plans, but unclear expectations reduce the impetus for programs to address today’s growing care gaps. 11 When accountability is vague and no one is accountable to solve specific access blocks, no one solves them.
Accountability frameworks, strangely lacking in Canadian healthcare, would address this lack of clarity by identifying functional units (programs) that are accountable for specific populations and care needs. Although aspects of accountability are widely discussed in business and administration, there are no descriptions in the peer-reviewed literature addressing the need for care accountability frameworks to improve care access.
Alternatives to program accountability
In the face of growing demand and limited capacity, health leaders have choices. They might consider innovative staffing models, efficiency initiatives, or flow improvements. They might modify care allocation, develop surge strategies, and queue management contingencies, or even lobby for new funding and capacity, but these approaches are challenging. In a system where programs are not accountable to provide timely care for their populations, there is an easier solution.
Management by closing doors
When patient demand outstrips apparent care capacity, the intuitive approach is to block inflow and form a queue, leaving patients to seek care elsewhere. Blocking access is a default response and primary coping mechanism for most programs. It is the opposite of a solution but delivers huge rewards. Workload is controlled, waiting patients are out of sight and out of mind, staff stress is relieved, and budgetary challenges are mitigated. Care shortfalls become someone else’s problem and programs are protected from evolutionary stressors that would otherwise mandate innovation and improvement. 11
In the absence of an accountability framework defining access expectations, it is acceptable to address demand challenges by closing the door.5,15 This approach prevents patients from getting the care they need, shifts care demands away from programs that can provide a service to programs that can’t, and displaces the consequences of program shortfalls to other parts of the system, reducing the need to address them. If consequences are expressed remotely from causes, leaders who can solve root problems have little need to do so, while highly affected (and motivated) leaders have no way to do so.5,11 Inpatient leaders cannot solve community care delays and ED leaders cannot solve inpatient mental health shortfalls. Management by closing doors is therefore a recipe for perpetual system failure, and there are few open doors for Canadians who fail to plan their illness or injury. 5
“Go to the emergency department”
Emergency departments have become healthcare’s “universal contingency plan.” 16 Canada has the highest rate of ED use in the First World and visits are rising rapidly because the ED is often the only place patients can get care when they need it.17,18 Community providers direct patients to EDs for a second opinion, a Computed Tomography (CT) scan, or off-hours care. Surgical patients are advised to go to the ED if they develop post-operative complications. Long-term care facilities that cannot manage sick or difficult residents transport them to EDs, not because it’s an emergency or because EDs have geriatric expertise, but because no one else is available to see the patient. Family physicians who need urgent surgical or specialist advice instead send their patients to EDs because there are no urgent speciality referral pathways. Patients enduring prolonged delays for imaging studies or specialist appointments head for EDs when they deteriorate or become frustrated. Marginalized patients who cannot access care elsewhere depend heavily on EDs, and answering machines throughout the healthcare system dispense the same advice: “Go to the emergency department.” The ED’s heaviest burden is admitted patients waiting for unavailable hospital beds, and the primary role of most urban EDs is no longer emergency care, but rather to serve as holding areas for admitted patients awaiting inpatient transfer. 19 These examples reflect the absence of effective queue management strategies and the consequences of management by closing doors.
Accountability frameworks
Appropriateness
“Programs” are functional units in the healthcare system. The term usually refers to population level programs like primary care, acute care, or long-term care, but also to facility-level programs like pediatrics or medicine. Programs are staffed, equipped, and structured for the work they do. Emergency departments are designed to treat acute injury or illness over minutes to hours, surgical programs to manage surgical conditions over days to weeks, and rehabilitation programs to restore long-term function. Acute hospital wards do not provide high-quality rehabilitation and EDs do not offer excellent mental healthcare. The best patient outcomes and system efficiencies occur when patients receive care from the right providers in the right place; consequently, appropriateness (right care-right place) is a core goal for all health systems.14,15,19
Accountability frameworks are a critical first step.5,11 They present a clear and different understanding of program accountability, intended to drive the implementation of strategies that will expedite the right care in the right place, and move patients out of queues into care. Accountability frameworks define care expectations and accountability zones. They link programs to populations, clarifying that every patient has a home and every program has a population.11,15 Accountability frameworks will not by themselves improve access nor will they immediately eliminate access blocks, but their absence is a recipe for failure.
Program accountability.
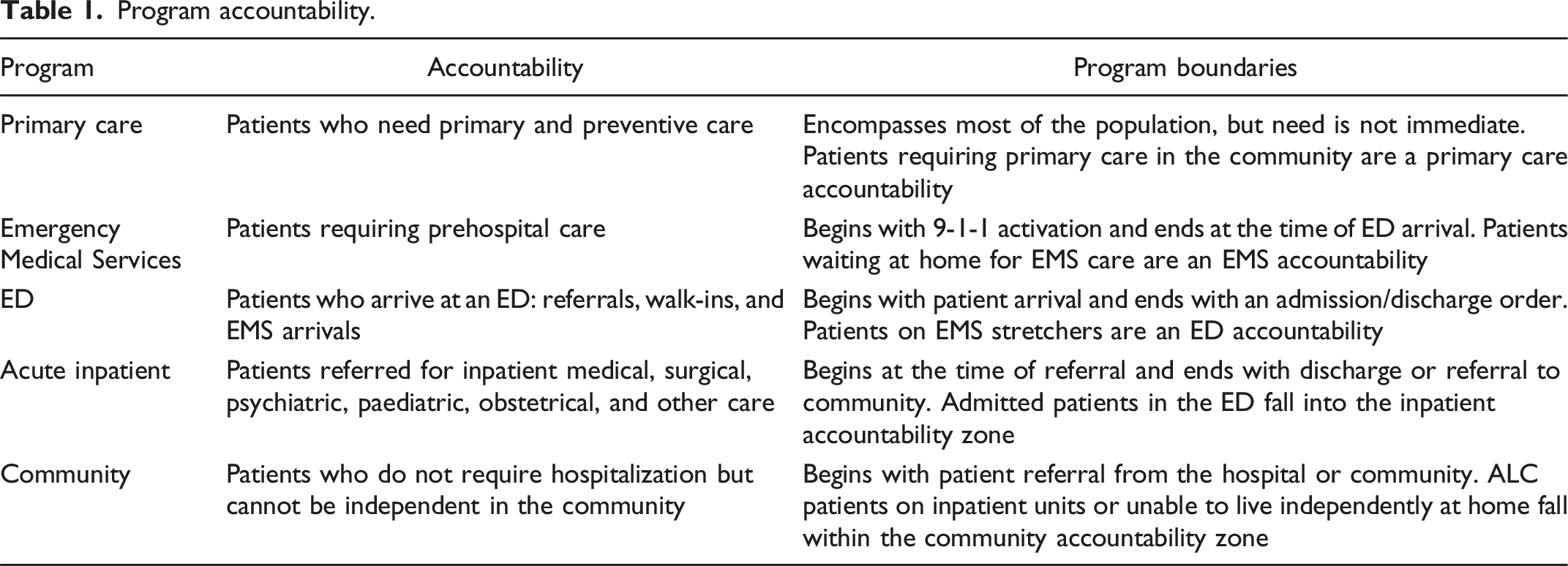
Accountability shifts as patients flow through the system. Patients self-refer for primary and emergency care, but specialist and surgical care requires referral, and the referral process usually defines the accountable program. Accountability is obvious in the case of a patient requiring mechanical ventilation or fracture fixation, but it may be unclear at the margins. Program boundaries can differ by hospital based on available resources and expertise, but accountability is always identifiable and can be clarified by facility-specific policies. If accountability is in dispute (e.g., the septic patient who is too sick for a medical unit but not sick enough for an Intensive Care Unit (ICU)), services at the relevant interface must resolve the disposition because they best understand the clinical and operational factors in play. 5
What is care accountability?
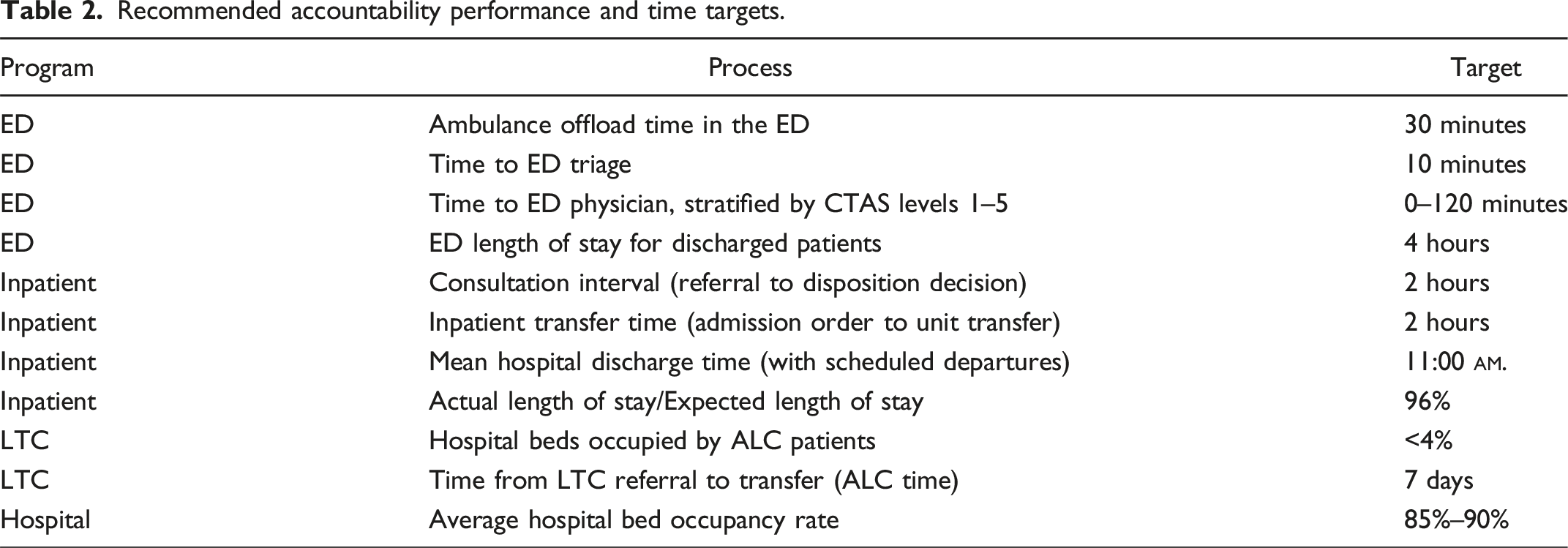
Recommended accountability performance and time targets.
If the queue isn’t your problem, whose problem is it?
Program leaders generally have system perspective and recognize the need to care for populations, while frontline providers may believe accountability extends only to patients already in their care. 21 Family physicians rarely feel accountable for orphaned patients who cannot get a doctor. Emergency providers act as if patients blocked on ambulance stretchers are an EMS problem, and inpatient staff usually believe that admitted medical patients blocked in ED stretchers are a problem the emergency department should solve. 16 This is a pernicious paradigm that guarantees ongoing system failure, because leaders have little ability to solve access and flow shortfalls occurring in other programs.
If accountability extends only to patients already in care, several failure mechanisms arise. Without queue management expectations, programs have no need to develop queue management contingencies. Closing the door and blocking access becomes the default approach, and providers may resist or sabotage access initiatives because they see patients queueing for their care as someone else’s problem. To illustrate, when hospitals implement overcapacity flow plans devised to move admitted inpatients more rapidly to inpatient units, inpatient providers often wonder why they are expected to solve “an ED problem.” Providers must understand who is in their waiting room and programs must develop service delivery plans that rationally allocate staff and resources to their target population, including patients in the queue.20,22,23 To avoid compromising care elsewhere in the system, contingency plans must involve more than blocking access. In an accountable system, the program responsible for the wait would provide the waiting room.
If you’re not fixing a bottleneck, you’re not fixing anything
Queues form at bottlenecks. They can be mitigated by increasing capacity or reducing demand at the bottleneck, but specific measures will differ by program and setting.10,14 Most programs can improve their intake processes. Some can increase care capacity by rethinking provider models. Many should better match care provided to care required or reduce artificial variability (e.g., surgical scheduling).24-26 Some programs are efficient but under-resourced. These require more money, beds, or providers. Many programs can increase efficiency and reduce lengths of stay. Some need to rethink the allocation of limited resources, triaging care to high-needs patients and reverse triaging care away from lower-needs patients.27,28 Because waste and low-value care account for much health system utilization,29-35 all programs should minimize the use of low-value tests, processes and procedures that do not improve patient outcomes. Almost all programs need to develop better queue management strategies and surge contingency plans.
Achieving accountability
Most leaders and providers agree with the concept of accountability. It is logical that someone must be responsible to assure patients can access care, but accountability often stalls at a conceptual level. Leaders find that accountability is difficult when demand is rising (an argument for demand management), when capacity is limited (an argument for thoughtful allocation, efficiency, and high value care), or when their beds are blocked by patients awaiting downstream care (an argument for appropriateness and program accountability). Regardless of challenges, accountability must extend into the real world where surges occur and patients stress systems. Leaders must solve occupancy and flow problems to assure care for their patients as much as possible, rather than assuming other services will step up and deal with their queue.
Program leads often argue that they cannot be accountable because the system is under-resourced. They are partly correct. Canada has fewer hospital beds, magnetic resonance imaging machines, and physicians per capita than most OECD countries1,2; however, governments are unlikely to fund more resources when they see poor demand-capacity management, inefficiency, care misallocation, low-value care, and inappropriateness (wrong patients in the wrong places) throughout the system. We may not have the capacity to provide timely care for all, but it’s clear we can do better with the resources we have.
Accountability strategies
Accountability frameworks clarify patient care expectations, but accountability strategies are necessary to move from concept to reality. Programs should introduce many or most of the access strategies described.
Understand your waiting room
Know who is in your accountability zone and plan for all the patients—not just those already in care.
Open the door
Letting patients in is the most important accountability strategy. Closing the door creates an illusion of control that reduces the need for program adaptation and efficiency. Ask your team: How would you change your system if it is no longer an option to block sick patients outside. Unconditional inflow puts patients in front of providers and introduces an evolutionary stressor that drives system improvement. It focuses smart people on problems they have not yet had to address, and forces program leaders to ask: How would you change your processes if blocking access was not an option?
Manage demand and capacity
Variability kills efficiency and causes more prolonged overcapacity situations that aggravate access blocks.25,26 Programs should match capacity (staffing and resources) to natural/unavoidable patient demand, then free up additional capacity by eliminating low-value activities, including redundant processes, unnecessary tests, and processes and procedures that don’t improve outcomes. Providers can reduce avoidable lengths of stay, especially if patients are no longer benefitting from hospital-based care, and remove patients from monitors or beds they don’t need.27,28 After freeing up care resources, programs should match elective/scheduled demand to newly available capacity. Rather than stacking elective variability on top of natural variability and creating demand surges that overwhelm the system, they should schedule elective admissions and surgical slates around natural variability to create more stable workloads25,26 and add buffer capacity to deal with predictable high demand periods.
Allocate limited care resources wisely
Ethicists say that if resources are insufficient, care priority is allocated preferentially to patients with the greatest need and likely benefit.20,22,27,35,36 High-risk, high-needs patients are usually found waiting at the program’s front door. During the early phase of care, where time is measured in minutes or hours, high-risk patients receive high benefit care. 23 Through the hospital stay, transformation to wellness continues but illness severity (need) and treatment intensity (benefit) diminish over time. 5 At the back end, where time is measured in days or weeks, convalescing patients consume more bed and nursing hours while accruing less health benefit. 11 Triage and reverse triage activities help focus resources on patients with the greatest need.27,28 If care rationing is necessary, it should occur at the back door, not the front door.
Identify and manage bottlenecks
Bottlenecks, which manifest as queues or delays, highlight the largest demand-capacity mismatches. Programs should add resources at bottlenecks—not elsewhere. They should support bottleneck providers and unload bottleneck servers by diverting demand from bottlenecks if possible.
Improve inflow processes
Bring decision-makers to the front door. This is usually the main bottleneck and the site of the sickest patients. It is a place for rapid expert disposition decisions—not trainee care. Develop surge contingencies (mini-disaster plans) and queue management strategies.
Fix transitions
Inefficient admission and discharge processes and cumbersome transitions between programs or care areas (e.g., Post Anesthesia Care Unit (PACU) to ward) are major causes of access block.
Implement a demand-driven overcapacity protocol
An Overcapacity Protocol (OCP) is a push contingency to be activated when proactive pull systems are failing and the system is overwhelmed.37,38 Demand-driven OCPs prioritize patient need over system norms, a patient-focused approach. They do not apply arbitrary caps on overcapacity care, but rather open the door to all high acuity patients. These protocols stress receiving programs by temporarily removing inflow control. Supply driven OCPs limit care supply by identifying a few OCP spaces on each unit and stopping inflow when these spaces are full, regardless of how many incoming patients need care. Units can regain inflow control and opt out of surge responses by assuring that OCP spaces remain occupied. Supply-driven protocols compromise flow rather than enhancing it, and generally fail.
Accountability frameworks go beyond programs and providers. Health ministries are accountable to assure that programs have the infrastructure and resources necessary to care for their populations, assuming high levels of efficiency and appropriateness (population-capacity alignment). 39 They must create the legislative and labour environment that enable chief executive officers, boards, and program leads to be effective. 13 They should lead the implementation of accountability frameworks like those described here, which incorporate accountability zones, access targets, and key performance indicators for all programs. Regional, facility, and program leads should implement accountability measurement and reporting systems, monitor care gaps, and use performance measures to determine whether gaps are best addressed through new capacity, enhanced efficiency, or reallocation of existing resources. Where the root cause is capacity, they must advocate for new resources; where it is inefficiency or misallocation, they must demand change. 13 Facilities should develop policies to clarify care accountability in grey zone or disputed cases (see accountability zones), and they should implement demand-driven overcapacity protocols to be activated when pull systems are failing. Overcapacity protocols should also bridge the hospital-to-community transition.
Conclusion
Many say the task is hopeless: we are already working as hard as we can and burning out. The latter may be true, but none of the recommendations here include “working harder.” The solution is seeing and acknowledging accountability zones, building systems rather than silos, and planning for all the patients. The solution is reconsidering care allocation, opening the front door, prioritizing patients with the greatest need, limiting inefficient and low-value care, increasing appropriateness (right care-right place), and incentivizing program accountability to populations. Clarifying program accountability and having a plan for all the patients will substantially improve access, and even small improvements across the system will provide huge benefits for Canadians needing care. 40
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.