
Abstract
Registered nurses’ practice in primary care varies and is sometimes sub-optimal. To fill the gap in primary care-specific knowledge, we co-constructed a national educational program to reinforce the nursing workforce. We based our project on the knowledge-to-action approach. Many lessons were learned during the development phase: (1) The experiential knowledge of patient partners and stakeholders allows an education program based on real needs; (2) The development of a national education program requires high-intensity investment from all involved persons; (3) An in-person meeting at the beginning of the project enables robust discussions and optimal co-creation; and (4) In a country where two official languages are spoken, it’s essential to create a safe environment and a translation infrastructure that allows everyone to express themselves in the language of their choice. Finally, other initiatives in healthcare education or professional practice improvement could leverage our findings to realize national-scale projects using knowledge creation approaches.
Introduction
While Canada has invested significantly in restructuring primary healthcare, we still fall behind other countries regarding the availability and consistency of care provision and coordination. According to the World Health Organization, “primary care is a model of care that supports first-contact, accessible, continuous, comprehensive, and coordinated person-focused care.” 1 Not only is it crucial for population health but a strong primary care system reduces the health system’s costs by reducing emergency consultations.
In primary care, a nursing presence promotes health equity and improves access, care continuity, patient satisfaction, and clinical outcomes, especially for vulnerable populations. 2 For experts and stakeholders, the integration of nurses is critical to improving primary care system performance. In Canada, the foundations of primary care-specific knowledge are not delivered in nursing education, which may limit the enactment of an optimal scope of practice for Registered Nurses (RNs) in primary care.3,4 Nelson explains that “working to the optimal scope means achieving the most effective configuration of professional roles, determined by other healthcare professional relative competencies.” 5 Since nurses are the largest non-physician providers in the primary care workforce in Canada, 6 there is a considerable gap in healthcare training.
To fill this gap and develop a strong primary care workforce, we focused on post-licensure education and credentialling for RNs in primary care (also referred to as family practice nurses or primary care nurses). Therefore, we co-developed an educational program based on Canadian Competencies for RNs in Primary Care 7 and the Patient’s Medical Home vision. 8
We chose the Knowledge-to-Action (KTA) model as the guiding framework that supports our vision of developing knowledge with knowledge users and how we can capture change connected to the creation process. As Graham indicated, “the implications of knowledge translation for continuing education in the health professions include the need to base continuing education on the best available knowledge, the use of educational and other transfer strategies that are known to be effective, and the value of learning about planned action theories to be better able to understand and influence change in practice settings.” 9 We structured our project with these principles to ensure the efficiency and success of our educational program to reinforce Canadian primary care and be of use to practitioners, policy-makers, patients, and the public. In this article, you will learn how the KTA model contributed to the success of the first phase of the development and deployment of our national educational program in Canada.
Approach
For 18 months, we have conducted this multiphase project to develop and implement a national educational program by and for RNs in primary care. In addition to the KTA model, we selected relevant frameworks, such as developmental evaluation, 10 RE-AIM, 11 Eco-Normalization, 12 and the New World Kirkpatrick model 13 to guide the evaluation of the implementation and effect of this national project. The protocol for this vast project will be published in a separate manuscript. 14 The implementation process and effects will be reported in another paper.
We identified KTA key steps and applied them in the complex process of translating knowledge into action in primary care settings.
15
We used the KTA approach to making change, including a six-stage action cycle that enables the translation of knowledge into practice.
16
We represented our research action cycles in Figure 1. Partnership approach in knowledge creation. The principal steps undertaken by the project team are associated with the KTA approach in knowledge creation and action cycles.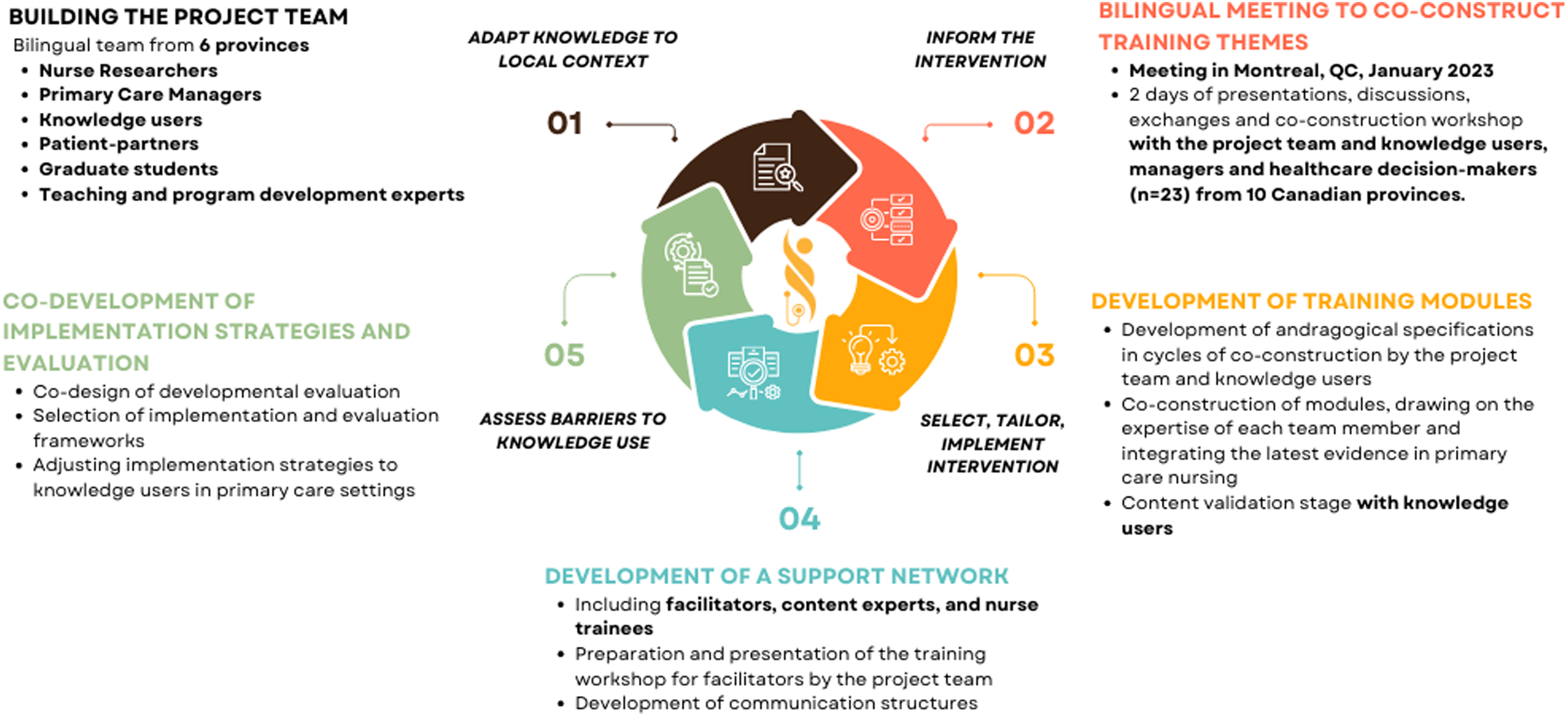
Building Team Primary Care Nurse
In developing our program, we utilized the best available knowledge and effective educational strategies for primary care RNs. Through the support of Team Primary Care and the strong leadership of the nursing co-investigators, we assembled a coast-to-coast Canadian team, including RNs in primary care, researchers, patient partners, nursing educators, mentorship experts, policy-makers, and primary care administrators. As we expanded our contact network, we included relevant knowledge users in each co-construction phase. To develop an educational program that would be bilingual and representative of primary care across Canada, it was essential to build a team with respect to the KTA principle that knowledge is research-based but also encompasses experiential knowledge.
15
TPCN is a bilingual team composed of 16 members from six provinces with complementary expertise.
Phase 1: Co-creation of the educational program and its implementation strategies
Inform the intervention
We tailored the knowledge co-creation process by selecting the educational program’s overarching themes and program structure. We conducted an environmental scan that included a literature review, stakeholder consultations, and a 2-day in-person meeting with the research team and knowledge users across Canada. 17 We adapted the program to respect diverse local contexts in Canada and identified implementation barriers and enablers.
Co-construction cycles of the educational program content
In co-construction cycles, we selected and tailored the knowledge for RNs in primary care. First, we developed the educational plan for each module with learning outcomes and suggestions for learning activities. Then, we assembled the appropriate learning content. Each of these steps included co-construction with all the research team members and validation with relevant knowledge users.
Co-development of implementation strategies and evaluation
In co-construction cycles, we established a network of RNs in primary care, facilitators (mentors), subject matter experts, nurse educators, health researchers, primary care administrators, and patient partners to form a community of practice. We co-designed the developmental evaluation 10 for the educational program assessment, supported by RE-AIM, 11 Eco-Normalization theory, 12 and the New World Kirkpatrick models, 13 to assess the implementation process and the intervention’s effects on RNs and professional practices in primary care.
Phase 2 (ongoing): Evaluation of the educational program’s impact and implementation
According to the KTA steps, 16 monitoring knowledge use, evaluating the outcomes, and sustaining ongoing knowledge use by RNs and its effects on professional practices in primary care are essential to measuring knowledge transfer into practice and adjusting the implementation strategies with knowledge users in primary care settings.
Results: Presentation of the learning from the pre-implementation phase
Key output of the application of the KTA approach
We produced an evidence-informed knowledge tool,9,18 the official name of the program: Team Primary Care Nurse Post-Licensure Educational Program. We included patient partners in the co-creation cycles with researchers and experts in primary care nursing to ensure that the program meets the requirements of the primary care setting and is relevant to nursing practice in primary care. We adapted the format to practitioners’ needs: asynchronous, bilingual, and accessible across Canada on various platforms to overcome barriers such as RNs’ workload and the limited time they have to complete continuing education.
17
We also obtained accreditation for the program, which is important for RNs’ recognition and motivation to undertake the program. We combined our observations and findings of an effective KTA integration in the design, delivery, and implementation strategy. Characteristics of the educational program: TPCN educational program takes approximately 2.5 hours to complete and contains six modules. The different themes are learned in progression from module to module. Interactive assessment questions are asked for each module objective. The last module involves resolving complex case studies to promote learning and critical thinking integration. Learners receive feedback and access additional resources and complete references within the program.
Importance of knowledge users’ involvement
We found that in-person meetings were essential to establish a strong foundation for our project. By bringing together our team members with various knowledge users from every province in Canada, we determined the core components of our educational program. Moreover, we initiated our collective reflection about our teamwork approaches, dissemination strategy, and training modalities. The 2-day in-person meeting helped build trusting relationship, which are foundational for effective team functioning and co-creation cycles. We also acknowledged that this meeting was important to identify barriers and enablers to the implementation of the national education program. Then, we integrated participants’ perspectives to contextualize the educational program to the different realities in Canada.
For this event to be bilingual, we had a simultaneous translation, which allowed participants to engage in robust dialogue in the language of their choice. Through bilingual co-creation, we discovered and addressed cultural issues far deeper than language differences. We reached a common perspective that has enriched the educational program and allowed French and English versions to be consistent and truly representative of the primary care nursing practice in both languages.
Additionally, we observed that the inclusion of patient partners brought a unique perspective to our team process and educational content. Patient engagement has been determined as an essential component of the educational program’s content. We collaborated with the patient partners in all co-creation step. Including their perspectives enriched the learning modules. “Participating in co-construction is important because enabling RNs in primary care to be recognized as experts in their field also help patients better understand the benefits of their expertise.” Marie-Dominique Poirier, patient partner.
“Co-constructing with patients is an essential part of creating a project that considers all aspects of the RN’s role and relationship with their work. RNs and patients work together in our healthcare, and we work together on solutions, like this project, to improve that care. It is a special and novel thing to be a part of.” Toni Leamon, patient partner.
Finally, robust discussions regarding comprehensive team-based care led us to integrate this as another essential component of our educational program. We consulted physicians and other professionals during the co-creation process to ensure that our education content was relevant for interprofessional collaboration and representative of different practice settings in primary care. By consulting literature and experts, we recognized that effective team-based care improves access to primary care and makes the delivery of care a higher quality with better patient outcomes, particularly with complex care management and vulnerable populations.19,20
Recommendation: In-person meetings should be included in other national projects to facilitate their launch and improve efficiency in organizing work within an interprofessional team.
Establishing efficient team functioning to apply KTA action cycles
After the 2-day in-person meeting, we established weekly team meetings to co-create the module plans and develop the learning content. We also established communication lines (mostly via email) and shared folders to perform effective co-construction cycles. As we worked on a short timeline to deliver the educational program, we reinforced and adjusted our team functioning as we went along. For example, when a team member needed help with a particular challenge, we organized shorter meetings with a reduced team with the appropriate expertise to support them and increase the efficiency and quality of content. Following this, we presented the product (e.g., module plan and content for a learning activity) to the broader team. Through this process, we valued the expertise of each team member.
In our project, we have established trust and a common understanding of cultural and language differences which were essential elements that embraced the expertise of each team member and allowed the development of solid communication structures. We observed that this trust was also crucial to creating a safe space that allows each person, including patient partners, to express themselves within the team. This rigorous process facilitated the achievement of a dynamic and bilingual on-line educational program co-created in a short period of time.
Recommendation: Other initiatives in primary care should develop a solid foundation in their interprofessional team to achieve their objectives and deliverables efficiently.
Tailoring the format of the educational program and its support structure
Through co-creation, we identified the need to address adult learning principles and concluded that an on-line gamified digital learning environment was desired. We selected external expertise for both digital design and learning management systems. The selection process focused on finding vendors who valued the co-creation process with our research team and the stakeholders. Over a 7-month period, following the best practices for e-learning educational approaches, we co-designed the digital and interactive educational program. During this time, we engaged various stakeholder groups in testing the initial versions of the digital learning environment, and we expanded our professional primary care nursing network. The professional primary care nursing network plays a crucial role in the community of practice establishment and implementation strategies.
Early on in the project, during the consultation phases, we realized a significant need to develop mentoring in primary care nursing nationwide. According to the KTA approach, we tailored the mentorship structure and implementation strategy of our educational program. We adapted the diffusion strategies and the structure of the community of practice for the reality of primary care and nursing practice by involving the healthcare stakeholders from different provinces and professions in the co-creation cycles. With this process, we laid the foundation for the new Canadian community of practice, composed of facilitators (from different provinces or areas), trained RNs, and primary care experts, including patient partners.
Based on literature and mentorship experts, we integrated a strong support structure to accompany the educational program. We acknowledged that RNs in primary care often experience loneliness, and having a mentorship structure is a factor that can contribute to their job satisfaction and even, their retention in primary care. 21 With this knowledge, we recruited facilitators whose main role is to support learners and help to transfer the new knowledge into their local primary care nursing practice. The facilitators realized the beta-testing of the program and provided comments and improvement suggestions. Additionally, we established a second role that involves their engagement in the dissemination of the post-licensure educational program in their own primary care network. By co-developing our mentorship structure, we aligned with the KTA phase to adapt and sustain knowledge use to local contexts. 9
Recommendation: Other research teams should engage in purposeful networking to find interprofessional and intraprofessional knowledge users to reinforce content and help with the implementation of their nursing or primary care interventions.
Barriers and enablers to the co-creation of an educational program and its implementation strategies
The main enablers in applying the KTA cycle and knowledge co-creation were effective communication channels and meetings. This supported the development of a relationship of trust between team members and the complementarity of individual expertise. We reinforced our strengths by adjusting our team process and consulting the right knowledge users to complement our interprofessional team expertise. We identified the principal challenge as the common understanding of scientific content respecting language differences. We addressed the language and cultural differences by allowing time to discuss those topics and deepening our respective knowledge. Finally, we leveraged this barrier and successfully built a high-functioning bilingual team where each member respects those differences.
Recommendation: Bilingual provinces or countries leading primary care or nursing interventions should dedicate a part of project funding to translation services during in-person meetings and to the co-creation of the knowledge products.
Further KTA action cycles and next steps for the project
Following the same rigorous structure, we also planned to monitor the implementation and evaluate the educational program outcomes (e.g., reach, effectiveness, adoption, implementation, and maintenance 11 with a target of 500 trainees). During the 2-day in-person meeting, we began discussing our research approach and the frameworks to consider, and then we co-designed the evaluation strategy. We described the research protocol in a separate manuscript. 14
Consistent with the KTA model, we must ensure the longevity of our educational program and our team structure, which will benefit further research and lend to improvements in nursing. We will produce knowledge mobilization tools throughout the project to disseminate advances and preliminary results (implementation and effects) to knowledge users. We will also adapt our knowledge mobilization tools to different audiences. For example, we will create short video capsules and infographics describing the project’s advances and developments that will be sent to RNs in primary care, managers, and decision-makers via the various communication channels of our respective networks and partner associations of RNs.
Lessons learned: • The KTA approach and the experiential knowledge of patient partners and stakeholders are essential components that support co-creation based on real needs. • The development of national training for RNs in primary care requires high-intensity investment from all the knowledge users, including patients and researchers. • Where virtual technology will be used to bring a national team together, an in-person meeting at the beginning enables robust discussions and optimal co-creation. • In a country where two or more official languages are spoken, it’s essential to create a safe environment and a translation infrastructure that allows everyone to express themselves in the language of their choice.
Conclusion and recommendations
In conclusion, the KTA conceptual framework is well suited to a national-scale project in primary care nursing. To consolidate the team structure and establish relationships with key stakeholders, in-person meetings should be funded in the budgets of national projects. Research on RNs’ scope of practice optimization in team-based primary care and integrating knowledge into practice needs additional funding to strengthen primary healthcare in Canada.
Our educational program is the first of its kind to be implemented nationally in Canada for RNs in primary care. The success of the first phase indicates that other Canadian initiatives and other countries could take it as an exemplar of an effective KTA structure to build similar educational interventions. Globally, other countries can leverage our project to build their own education. Comprehensive instructional design was required to build this bilingual education program and make it relevant across Canada. This educational program will enable RNs to clearly define their actual and potential role and practice to their optimal scope of practice. By applying the KTA approach, we have identified central themes for improving teamwork, such as clarity in role definition and optimization of scopes of practice, consistent with the work of other Team Primary Care projects. Disseminating our training program not only to nurses but also to decision-makers and other healthcare professionals will help to improve these aspects of professional practice and enhance the effectiveness of primary care teams.
Adopting a KTA approach enabled the project team to create an educational program that was evidence-informed, addressed needs identified by frontline nurses, patients and administrators, and followed best practices in adult education.
Footnotes
Acknowledgements
This article has been written on behalf of all the co-creators involved in the Team Primary Care Nurse project.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Team Primary Care was supported by Employment and Social Development Canada through a grant to the Foundation for Advancing Family Medicine, co-led by the College of Family Physicians of Canada and the Canadian Health Workforce Network.
Ethical approval
Institutional Review Board approval was not required.