
Abstract
Lack of access, system inequities, and inefficiencies plague our current healthcare system. With a challenge this complex, no one intervention is sufficient; all will be necessary. The primary care system needs a strong health workforce prepared in bold new ways. Students represent an important voice, given their role as future leaders of health education and healthcare. For students to lead, educators must leverage education paradigms that position current students as leaders of transformation. Yet, in current health education systems, students are often seen as passive recipients of knowledge and skill. Transformative education seeks to foster critical reflection (an ongoing process of questioning unhelpful assumptions and power relations) and informed action in students to enable them to challenge and change norms and change practices, structures, and society. This article highlights the value of transformative education in cultivating thoughtful change agents and provides one tangible example of a new education/practice model that puts this paradigm into action.
Introduction
It is no longer debatable that the primary healthcare system in Canada is in crisis. We know the numbers (6.5 million Canadians without access to primary healthcare 1 ) and we hear the stories across all primary healthcare sectors and domains2-6 around lack of access, system inequities, and inefficiencies in care and service. We also know that without collective action for a better system, it will only get worse. With a challenge this complex, no one intervention is sufficient; all will be necessary.
The primary care system needs a strong health workforce prepared in bold new ways. The most realistic and necessary care model envisioned to date is a team-based approach that prioritizes community and relationships. 7 This call also includes an appeal to equity, access, and inclusion of individuals across diverse social and structural positions and backgrounds. Health professions students represent one group of voices that we must listen to closely.
Amplifying the need for transformative education
“What got you here, won’t get you there” – Marshall Goldsmith
Students represent an important voice of change, given their role as future leaders of healthcare and Health Professions Education (HPE). Yet, in current HPE systems, students are often seen as passive recipients of knowledge and skill. This common trend runs counter to evidence across paradigms of education. 8 In fact, no matter one’s paradigm of education—for example, education as knowledge acquisition or as the creation of agents of change—there is benefit to active engagement of students in their own learning, for future learning, and for the future of society. For example, cognitive constructivists advance students’ active engagement in knowledge-building as key to learning and humanists focus on enabling self-actualization among students. Transformative educators seek to foster critical reflection (an ongoing process of questioning unhelpful assumptions and power relations) and informed action in students to enable them to challenge norms and change practices, structures, and society. 9
True transformation must attend to the entirety of a system. In education, attention must be paid from student admissions processes, to pedagogy, to the culture of our schools and workplaces. Students are socialized into the current healthcare system throughout their educational journey, learning how to act—what it means to “be” a health professional—and some ways of acting and being are reinforced and rewarded while other ways of being can be suppressed. Wright 10 has demonstrated that personal statements used to assess candidates for medical school inadvertently favour cultural capital (e.g., playing a musical instrument and certain forms of work experience) rather than assessing desirable attributes in a physician. These proxies for commitment and motivation (extracurricular activities or work experience) are highly dependent on a student’s access to various forms of capital (social, economic, and cultural). 10 This misplaced attention in the admissions process may then restrict who is able to become a physician at all and represents a lack of critical reflection within the medical school admissions process. 10 This socialization process continues within medical school; in a study of medical students who were the first in their family to attend university, Wright et al. 11 further demonstrated that medical school culture can suppress students’ ability to show up as their authentic selves, conforming them to the status quo and thereby stymying their strong potential to be leaders of transformative change. 11
The examples above illustrate why we require critical knowledge in order to truly achieve transformative change. Critical knowledge is that which explicitly asks questions about who benefits, who has been included, who has been excluded, and who might be harmed by existing practices and structures. Critical knowledge is taught through transformative education approaches that strive for dialogue and critical reflection.12,13 Importantly, we do not advocate for critical knowledge in place of relevant conceptual knowledge, but rather in addition to it. Where conceptual knowledge includes understanding of “why” (and not just “what to do”) the “why” in critical knowledge is not only technical or bioscientific mechanisms; it also includes social and structural mechanisms, including power relations. For example, in healthcare, we have constructed interprofessional differences that serve practical purposes (e.g., specific roles on a team and distinctive scopes of practice). When teaching students about the nuances of role negotiation and conflict management, it would benefit them to learn why interprofessional tensions arise. Thus, beyond the practical purposes of differential roles and scopes, students could learn that in addition to function, differing roles and scopes also create differences that impact personal situations and interpersonal relations, such as differential pay, power, and hierarchy. These symbolic and material gaps between professions may then inadvertently enforce unhelpful practices, such as unmitigated interprofessional conflict.
Transformative education aims to support students in self-actualization and change agency; it thus represents a pathway to students as leaders. It ultimately strives to move from reproducing the way of the world toward transforming the way of the world. It aims to do this by fostering critical reflection as a continual process of questioning why things are as they are and imagine a more just way for all. Critical approaches align well with interprofessional collaboration, given the inextricable role of power relations 14 in team-based practice. Thus, transformative education aligns well with interprofessional education and leadership development. Importantly, the aim of transformative education is not to arrive at a fixed destination; to do so would run counter to transformation. Rather, transformative education aims to support learners in understanding that leading and enacting change must be continual. Through critical reflection, we are always looking at how else a situation could be viewed, who else needs to be included, and ultimately how we could do better for all.
Illuminating the way: Creating student leadership experiences
Examples of two existing Student-Led Learning Environments.
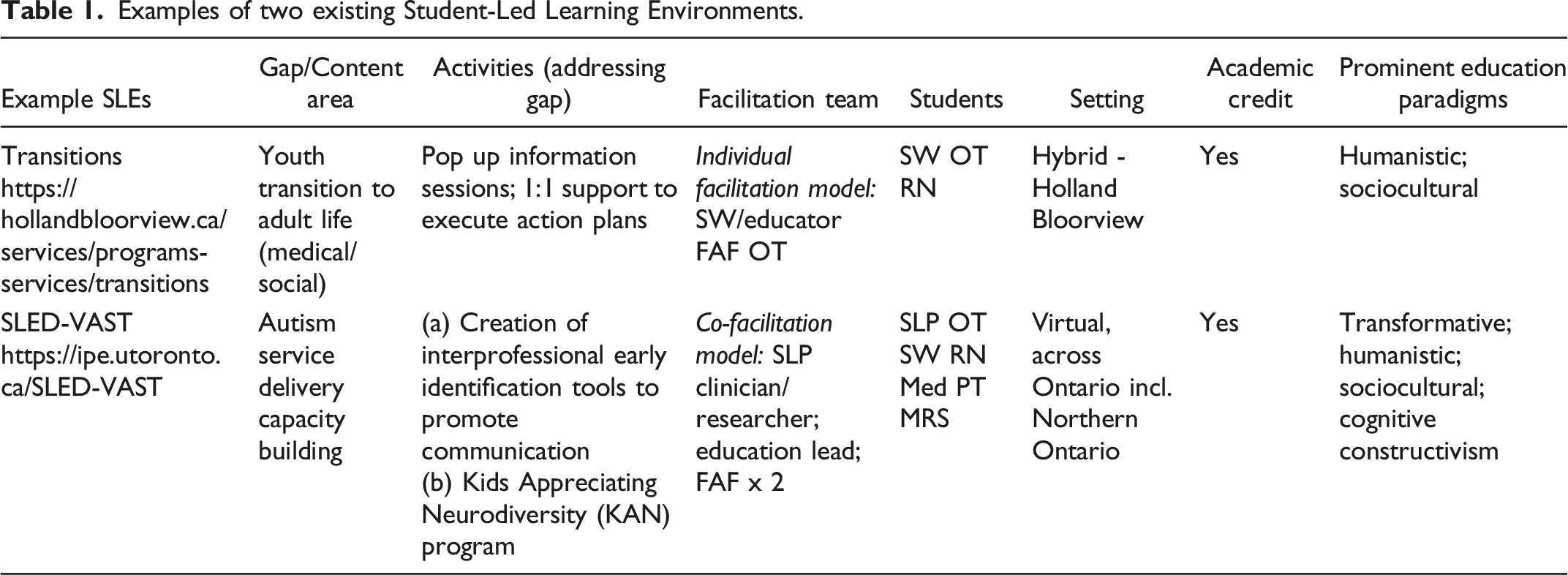
In the 2022-2023 academic year, members of the TAHSN SLE Steering Committee created nine unique SLEs with 79 learners spending a cumulative total of over 8,000 learning, leadership, and service hours in an SLE. These students, representing 12 unique health professions, worked with 3,228 patients/clients/family members as part of their SLE experience. 15 Importantly, through evidence-informed education design and delivery, these learners were prepared for future learning and to be leaders of transformative change when confronted with inevitable future uncertainties. 16
Being part of Team Primary Care (TPC) allowed for the authors’ first SLEs with primary care intersections, expanding the availability of SLEs to medicine students and engaging students in different forms of interprofessional work. 17 This expanded context and reach of the SLE pushed the authors to consider how the SLE model applies to primary care as much as to other settings. As part of TPC, the authors were also supported to attend a longitudinal leadership program (described below) which enabled the ongoing iteration of the SLE.
A word about leadership within student-led learning environments
Since 2009, University Health Network’s award-winning Collaborative Change Leadership Program™ (CCL)
18
has been at the forefront of shaping the future of leadership in healthcare. The program’s purpose is to “develop people to lead health system transformation and enable a more just world for all.” Unique to the CCL model is the integration of both the “being” (how we show up as leaders, fostered through self-awareness) and the “doing” (what we do as leaders to co-create possibilities for change). Some of the CCL concepts of “being” and “doing” that have been integrated and operationalized into SLEs include employing generative change processes, compassion, critical reflection, and strengths-based practices. These are elucidated below. (1) Learners facilitating processes of co-creation. Co-creation entails the active involvement at various stages of the production process, a “collective creativity”
19
that necessitates trust
20
and equal, reciprocal relationships between all partners.
21
Supporting students as facilitators of co-creation entails explicit attention to “equalizing (or at least reorganizing) power relations in service design and delivery.”
21
As described in the CCL model, in SLEs, learners convene system voices, facilitate dialogue, and nurture opportunities to co-create innovative solutions that are meaningful to all system stakeholders. Learners realize that they themselves are not the experts, and they do not have the answers to the question of what is possible. The collective voices in the system co-create possibilities together. Learners are honing their skills as facilitators of that process. (2) The dynamic process of compassion. In this context, compassionate leadership is defined as an approach to leadership that “grows from meaningful human connections and responds to human needs within complex organizations.”
22
Learners need not only technical skills but social and emotional ones, “exemplified by shared vision, compassion, and relational energy.”
23
Compassion is not a trait that one either does or does not possess; rather it is a “dynamic process”
24
and relational, “occurring in and through interactions and connections between people.”
24
The CCL model positions being a collaborative change leader as being present as an equal in a shared human experience. Within an SLE, learners are viewed not only as passive vessels awaiting knowledge, but recognized and valued as leaders, teachers, and humans who bring their lived experiences to their contributions and development of innovative and compassionate care solutions. (3) To address issues of inequitable primary care, SLE supervisors create spaces and opportunities to deepen learners’ self-awareness by fostering critical reflection on the processes and structures enabling oppressive structures and practices to remain in place. As previously mentioned, critical reflection is the “process of examining assumptions (i.e., individual and societal beliefs and values) and power relations, and how these assumptions and relations shape practice.”
25
Within the SLE, through meaningful dialogue13,26 with supervisors, learners notice when assumptions might lead to harm and therefore continually question and challenge assumptions and change practices.
27
An SLE might call explicit attention to how power and hierarchy are working against the emergence of a new system that is more equitable and compassionate in primary care. By first noticing inequities, then one might re-imagine and create innovative, potentially more equitable practices and possibilities. (4) Knowing the strengths of self and others. Investing in your own strengths and maximizing the strengths of the team can unleash tremendous potential for change.
28
Working together collaboratively allows learners to use and combine their strengths to create and deliver something that otherwise would not exist. The collaborative and interprofessional nature of SLEs creates an environment that enables celebration of strengths across domains, and can encourage the cross-pollination of ideas, knowledge, and clinical skill development.
An invitation to all leaders
To actively respond to system pressures, “SLEs integrate best evidence in both education and clinical practice, workplace learning, and community partnership to: (a) create cost-effective and customized care solutions; (b) promote the growth of care teams, creatively addressing health workforce shortages; and (c) embrace health professional students as team members and leaders, maximizing both learning and the rapid creation and implementation of care solutions.”
14
These types of learning experiences, which attend to both critical system needs and nurture the next generation of collaborative, compassionate leaders of change, could complement uniprofessional and interprofessional curricula, enhancing the direct relevance of HPE programs to society. This brings us to a point of curiosity, and an invitation, for all leaders: (1) For leaders in higher education - How might SLE experiences be integrated into existing curricula? Should these experiences be a requisite for all health professions students prior to graduation? How might we integrate and nuance existing professional development programs, such as CCL, for undergraduate and pre-licensure learners? (2) For leaders in accreditation bodies - SLEs have already been acknowledged as components of Leading Practices by Accreditation Canada.
29
What might be possible if models of transformative education were an integral component of accreditation standards for uniprofessional curricula? (3) For leaders of faculty development programs - SLEs require facilitators to eschew teacher-learner hierarchies and to adapt to student needs and community contexts. Shifting away from typical perspectives on education will require educators to develop skills in interprofessional education, transformative education, and education science. How might faculty development programs be created to support the development of SLEs across contexts by educators and facilitators prepared to mobilize education science along with clinical, research, and experiential knowledge?
Conclusion
To transform primary care, educators need to let go of assumptions that it is those with the most experience and structural power that must lead the change. In fact, it may be those less mired in the way things are, that is, students, who may most freely innovate with fresh eyes and eager minds. By recognizing, examining, and letting go of assumptions embedded in current HPE practices, we can accelerate change.
Our invitation is to support the creation and democratization of workplace-based interprofessional learning opportunities for students that will hone their leadership abilities to transform primary care so that “individuals, organizations, and communities can flourish.” 30 An intentional focus on applying transformative education models in developing students as collaborative leaders can fulfil the promise of creating leaders of primary care transformation. Education systems will need aligned restructuring to truly enable and embody this orientation. By restructuring education, and adopting SLEs within HPE curricula, student leadership can begin to shift the primary care system toward a community- and relationship-focused, sustainable, equitable model. SLEs are one powerful and evidence-informed intervention that can be adopted to begin to address the existing, complex health and social care challenges.
Footnotes
Acknowledgements
The authors wish to thank TPC for their support of this work and to Maria Tassone and the faculty of the Collaborative Change Leadership ProgramTM for their contributions to this article. Finally, to the faculty and learners engaged in SLEs for their curiousity, compassion, creativity, and dedication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Team Primary Care (TPC) was supported by Employment and Social Development Canada through a grant to the Foundation for Advancing Family Medicine, co-led by the College of Family Physicians of Canada and the Canadian Health Workforce Network.
Ethical approval
Institutional Review Board approval was not required.