
Abstract
This article examines the leadership challenges of prison healthcare, specifically focusing on the ageing inmate population. It highlights the distinct health burdens faced by this demographic, including higher disease prevalence and an accelerated ageing process. The concept of prison activities of daily living is central to addressing these challenges, emphasizing the need to tailor health assessments and care plans to the unique prisoner-environment interactions. This article advocates for inclusive person-centred care. It suggests that involving older prisoners in their care planning, aligned with the “ageing in the right place” principle, can significantly improve their quality of life. Additionally, it explores strategies to combat social isolation and loneliness among older prisoners, such as intergenerational activities and prison-community partnerships. Health leaders can echo these findings in policy development and incorporate collaborative, inclusive, diverse, and intergenerational models that address the complex health needs of older prisoners.
Introduction
The population of older people in prisons is expanding disproportionally worldwide. 1 The prison population of Canada was 104 per 100,000 residents. 2 According to Statistics Canada, the total number of custodial admissions in 2022/2023 was 163,387. 3 About 25% of federal prisoners were over 50 years old. 4 There is no universal definition of “older” among prisoners, with age thresholds ranging from 45 to 65 years. However, recognizing the phenomenon of accelerated ageing in this cohort, most research tended to classify prisoners aged 50 and above as older adults.5, 6, 7 Studies reported that the ageing process of older prisoners was accelerated due to multiple factors, including poor health, mental health needs, substance misuse, and social determinants like trauma and homelessness.8, 9
Evidence suggests that older prisoners are at risk of dementia and psychiatric disorders. 10 , 11 In addition, older prisoners have a higher disease burden and suicidal risk compared to younger prisoners and community-dwelling older adults. 12 , 13 From 2000 to 2013, the overall suicide rate among younger prisoners (under 50 years) was reported at 1,157 per 100,000 prisoners, while older prisoners (50 years and above) showed a significantly higher rate of 2,042 per 100,000. 14 More importantly, studies reported gender differences in perception of physical health, mental health needs, safety, and suicidal rates. Older female prisoners had a higher chance to labelled negatively for their physical health and about three times higher suicidal rates than older male prisoners. 15 , 16 Direct healthcare only contributes 15% to a person’s overall health, with the remaining 85% being affected by other determinants. 17 These include social and structural determinants of health, for instance, healthcare accessibility, social networks, food security, recreation, education, law, and policy. 18
Optimizing health for older prisoners is a complex challenge for healthcare management due to the marginalized and non-dominant population they represent. This includes person-centredness, ageing in place, social isolation, and loneliness to achieve optimization. However, most correctional facilities’ designs and policies emphasize security over older prisoners’ needs. The conflicting goals between custody and healthcare directly impact older prisoners’ self-management and autonomy. 19 Macleod and colleagues shared the story of an 84-year-old prisoner who had been incarcerated for 55 years on a life sentence. He suffered from advanced chronic lung disease and liver failure, with a recent rapid deterioration. Due to security regulations at the prison prioritizing maximum security, his medical team could not inform him of his scheduled hospital visits for fluid drainage, which was necessary for his severe oedema. This led to significant stress on him, as he could not anticipate relief from his discomfort and remains anxious about the uncertainty of his care. 20 This real-life experience exemplifies the tension between security measures and prison healthcare provision, affecting older prisoners’ autonomy, care and mental health. Research on the care needs of older prisoners compared to the community is limited, and there is a lack of studies on health optimization from the social lens of older prisoners. 21
This article aims to explore the effects of prison on the functional health needs of older prisoners, examine the adoption of “ageing in the right place” under person-centred care, and propose solutions to combat the social isolation of older prisoners. This will be based on evidence from intergenerational activities, prison-community partnerships, and correctional gardening in Canada.22, 23
Methodology
Two databases, CINAHL and PubMed, were searched using specific search terms, Boolean operators, and limiters. The focus was on older prisoners, healthcare, social isolation, determinants of health, ageism, and outcome. The search was refined to include studies published between 2013 and 2023 for participants aged 50 or older.
In CINAHL, a comprehensive combination of keyword searches was utilized, targeting older adults, prison, incarceration, determinants of health, ageism, and social isolation. The search strategy was refined using specific limiters and limited to studies published from 2013 to 2023. This method provided a thorough and focused review, synthesizing the latest relevant literature in this domain. This approach retrieved 30 results.
In PubMed, separate searches were conducted for each aspect of the research, using relevant MeSH terms and keywords. The social determinants of health search yielded 7,203 articles, the ageism search yielded 1,095 articles, and the prison and social isolation searches yielded 12,092 and 26,456 articles, respectively. By applying term combinations and a filter for publication date, language, full-text availability, and subject age, 13 articles were retrieved.
In the literature search, 43 articles from CINAHL and PubMed underwent comprehensive screening. After assessing titles and abstracts for relevance, 20 articles were made for in-depth analysis and knowledge synthesis (Figure 1). PRISMA 2020 flow diagram*.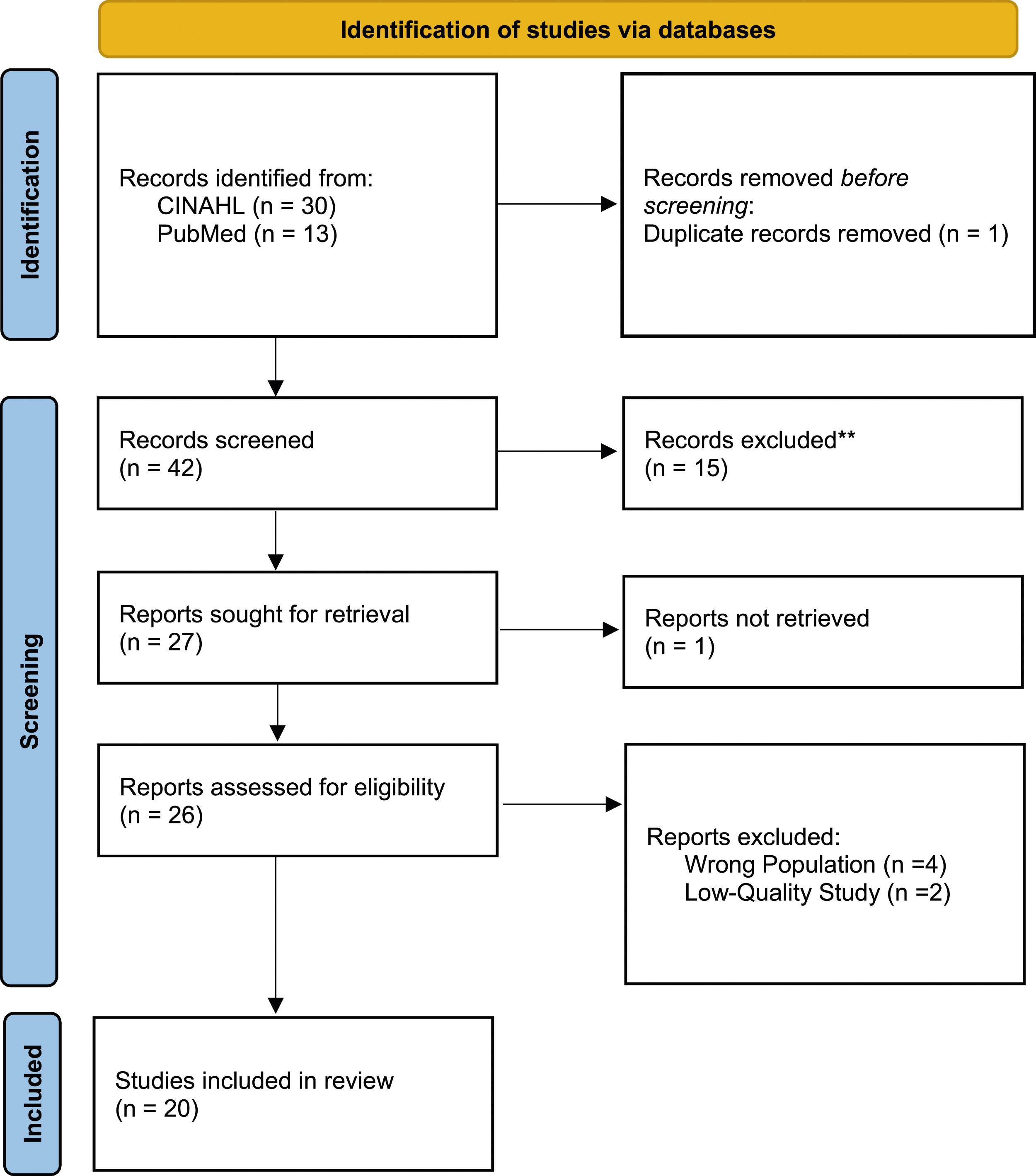
Findings and implications
Context-specific functional health needs
“Functional health needs” denote the ability of a person to engage and perform a range of Activities of Daily Living (ADLs), including grooming, dressing, toileting, ambulating, and eating. 24 These activities meet basic needs in the community across multiple modalities. Conversely, it is widely acknowledged that the unique daily activities performed in correctional facilities shall be considered in the functional health needs assessment of older prisoners, for example, the ability to drop to the floor when the alarm goes off, bunk bed climbing in prison, stand for headcount, hear orders, and go to the dining hall for meals. 25 These prisoners-specific ADLs are stated as Prison ADLs (PADLs).26, 27 PADLs demonstrate interaction among environmental context, custody logistics, and people’s functional health needs. The prisoners must be able to perform PADLs to cope with the prisons’ physical design, logistics, and policies to survive. This person-environment exchange denoted the interlocked relationship among older prisoners, their physical-social environments, and how these relationships shape their late-life experience and perceived well-being.28, 29 Importantly, the evidence highlights that the execution of PADLs falloffs before performance across traditional community-dwelled ADLs. 30
Therefore, care models and assessment tools for older prisoners should consider contextual-personal interaction. Correctional facilities might develop training modules co-created with geriatric associations and not-for-profit organizations like the Canadian Geriatrics Society and Alzheimer Society of Canada to enhance staff understanding and fundamental skills in older adult care and the development of prison-specific comprehensive geriatric assessment tools to provide timely assessment and effective inter-disciplinary communications.
Ageing in the right place and person-centredness
Quality service delivery to older populations in the community depends on person-centred care. It takes people’s values, preferences, and chosen needs to the centre of care beyond their medical conditions. Involving older prisoners in care planning is vital for successful interventions and meeting their unique needs and preferences. 31
World Health Organization (WHO) advocates the importance of ageing in the right place to achieve healthy ageing. 32 Older people have an active relationship with their environment. As they age, many people prefer to remain in their familiar community, valuing the sense of closeness, connectedness, and security it provides.33, 34 This echoes the findings of older prisoners. Older prisoners, particularly those serving long sentences and without family connections, consider prisons their homes. They would rather die in prison than be released early and compassionately into society. 35
Person-centred care can apply to prisoners’ relocation preferences. A few studies showed the benefits of transferring older prisoners to purpose-built specialized units that address the declining older prisoners’ physical and functional needs. Such policy-driven segregation showed the advantages of convenience, cost-saving, and safety promotion.36, 37 However, the older prisoners were excluded from the decision process. Segregation does not necessarily result in healthy ageing or ageing in the right place and could have negative effects. Older prisoners with dementia, when placed in an unfamiliar environment, may exhibit behavioural issues, resulting in disciplinary actions from correctional staff and peer victimization. 38
Conversely, through the lens of older prisoners, some prefer to stay in the original prisons to age, where they spend a significant lifetime and develop trustable close bonds with workers and prisoners. 39 Therefore, it is essential to note that structural determinants of health, for example, law and prison policies, must align to address this preference and person-centred care.40, 41 Government and correctional facilities may include the voices of older prisoners, their families and staff in the policy development journey concerning the care of elderly prisoners.
Social isolation and loneliness of the older prisoners
There has been widespread concern about older people’s social isolation and loneliness associated with adverse health impacts. 42 Various interventions have been organized to tackle this pressing issue in the community. Research showed that shared characteristics of successful programs include community participation, productive engagement activities and reciprocity. 43 Nevertheless, little about alleviating older prisoners’ social isolation and loneliness is discussed.
In Canada, the Indigenous community-prison partnership is an initiative in which federal prisoners make items or grow organic vegetables to donate to underserved Indigenous communities. It was described as “healing on both sides” by the recipient First Nation's woman and may positively impact the prisoners’ identity and sense of self. 44 This initiative helps build relationships and potentially reduces prisoners’ loneliness. 45 In 2004, a prison garden program was launched in British Columbia. In contrast to other gardens, the engaged prisoners also participated in the subsequent donation of produce to vulnerable communities. It provided a mutually beneficial healing connection, work satisfaction, and the opportunity to increase the self-esteem and self-worth of the prisoners. 46 It can be expected to reduce social isolation and loneliness.
Alternatively, intergenerational contact intervention can alleviate older prisoners’ social isolation and loneliness. It has the successful features of community participation, mutual productive engagement, and reciprocity. 47 Intergenerational inclusive programs have been proven beneficial to children and young people in the community and older prisoners in the United States, Europe, and Asia. 48 It promoted social connection, trust, autonomy, self-esteem, and generativity, giving daily life more meaning. 49 The program activities could be educational, scientific base, experience and wisdom translation, awareness actions, theatre plays, and traditional games. 50 The pearl of success is an interactive, inclusive approach to fostering generational links and understanding. 51
Considering the benefits of the above two strategies, it has the potential to incorporate into a new initiative: an intergenerational community-prison agricultural partnership that includes older prisoners, trans generations in the community, and Indigenous people. It can be expected that the loneliness of the older prisoners will be relieved, and understanding among older prisoners, different generations, and the Indigenous community will be enhanced. The garden will be a fertile platform for dialogue, connection, and reciprocity. 52 In addition, this new initiative is in line with one of the advocates of WHO in combating global ageism. 53
Conclusion
The evolving demographics within Canadian prisons highlighted a growing need to shift focus from traditional security-focused matrices to frameworks that embrace more inclusive, community-involved strategies in healthcare. These re-orientations aim to enhance the well-being of older prisoners by reducing isolation and improving social connections through innovative community-prison partnerships.
One promising approach is involving older prisoners in intergenerational and agricultural projects, which not only helps reduce loneliness but also bridges gaps between older prisoners and the community at large, including Indigenous communities. This shift would better meet the health needs of older prisoners and build a more equitable and humane correctional system.
Health policy makers and correctional leaders should consider prioritizing these integrative and person-centred strategies to ensure the correctional system supports the dignity and rights of all prisoners. This approach calls for rethinking how we provide care in prisons, making it more community-focused and responsive to the needs of an ageing prisoner population while balancing security, safety, and resource allocation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.