
Abstract
Billions of dollars are invested annually in leadership development globally; however, few programs are evidence-based, risking adverse outcomes, and wasted time and money. This article describes the novel Inspire Nursing Leadership Program (INLP) and the outcomes-based process of incorporating gold standard evidence into its design, delivery, and evaluation. The INLP design was informed by a needs analysis, research evidence, and by nursing, Indigenous, and equity, diversity, and inclusion experts. The program’s goals include enabling participants to develop leadership capabilities, cultivate strategic community partnerships, lead innovation projects, and connect with colleagues. Design features include an outcomes-based approach, the LEADS framework, and alignment with the principles of adult learning. Components include leadership impact projects, 360-assessments, blended interactive sessions, coaching, mentoring, and application and reflection exercises. The evaluation framework and subsequent proposed research design align to top-quality standards. Healthcare leadership programs must be evidence-based to support leaders in improving and transforming health systems.
Introduction
Internationally, the annual investment in leadership development is estimated at $50 billion.1,2 Many organizations consider leadership development an obligatory cost, 3 a source of competitive advantage,4–7 and a key retention strategy.8–12 Organizations across sectors offer internal leadership programs, along with an increasing number of external providers, including business schools, private corporations, and individual consultants. 13
Evidence of leadership development outcomes
The increasing abundance of leadership training corresponds with evidence that programs can facilitate improved participant outcomes, such as increased confidence, knowledge, skills, capabilities, engagement, well-being, job satisfaction, self-efficacy, and performance.14–16 Leadership interventions have also been correlated with organizational-level outcomes, including decreased absenteeism, increased staff retention, engagement, motivation, and sense of shared purpose, increased organizational performance, financially and clinically, and improved patient outcomes and patient safety.14–16 There is also evidence that interventions can demonstrate financial Return-on-Investment (ROI). 17
Uncertain quality of evidence and potential consequences
Despite this evidence and the extensive global investment, there is widespread ambiguity regarding which program designs are linked empirically to outcomes.1,18–22 Even in academic literature, purported as the most credible source of evidence, the knowledge base is of predominantly poor quality.15,23–25 This situation can obscure what works best, why, and with what reliability 17 , can perpetuate ineffective practices, and can be confusing, misleading, and potentially harmful.22,23 Equally, designing interventions based on questionable evidence (or none) risks program underperformance or, worse, adverse outcomes.22,26–30 For example, despite typically favourable program evaluations,22,31,32 reports of the proportion of trainees applying their learning to the workplace—the enterprise’s currency of success 13 —are as low as 5%. 19 The stakes of substandard interventions for organizations heighten when budgets are strained, priorities are competing, and capacity is limited.33–35
Gold standard program elements and research quality
Establishing gold standards
To address the knowledge gap and to isolate evidence-based elements of leadership development programs linked to outcomes, the systematic review by Geerts et al. 15 introduced a novel methodology. This involved building on the foundational and most-cited review of medical leadership development, that by Frich et al., 31 and applying a validated instrument, the Medical Education Research Study Quality Instrument (MERSQI), to all relevant studies from 2007 to 2016 (K = 25) to assess their quality.
Gold standard elements of program design, delivery, and evaluation incorporated into the Inspire Nursing Leadership Program (INLP).
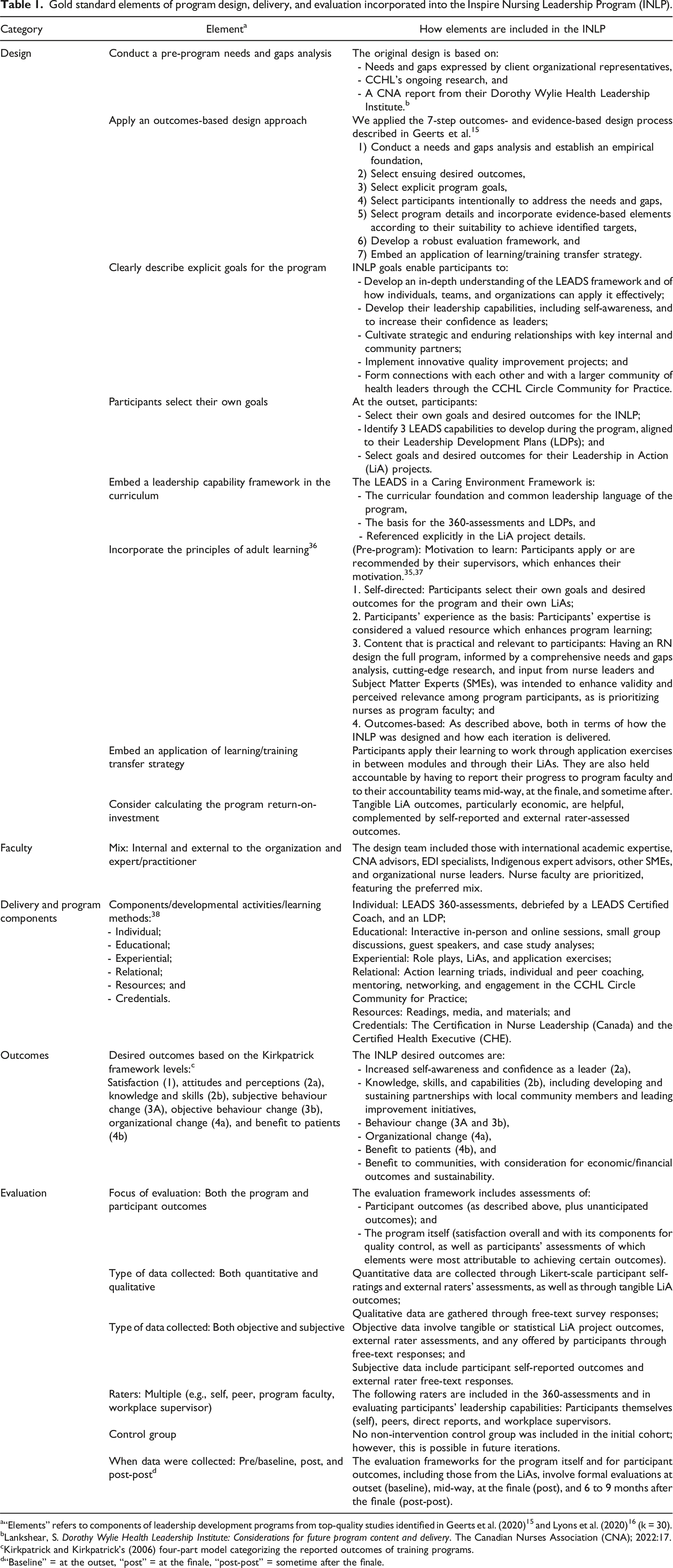
a“Elements” refers to components of leadership development programs from top-quality studies identified in Geerts et al. (2020) 15 and Lyons et al. (2020) 16 (k = 30).
bLankshear, S. Dorothy Wylie Health Leadership Institute: Considerations for future program content and delivery. The Canadian Nurses Association (CNA); 2022:17.
cKirkpatrick and Kirkpatrick’s (2006) four-part model categorizing the reported outcomes of training programs.
d“Baseline” = at the outset, “post” = at the finale, “post-post” = sometime after the finale.
In summary, “gold standard” refers to (a) the methodological characteristics of highest standard research studies, whose findings are empirically anchored, and (b) the best scientific evidence regarding elements of leadership development programs that have been linked to outcomes.
Expanding the credible knowledge base
To augment the breadth of gold standard evidence, Lyons et al. 16 applied MERSQI and the Joanna Briggs Institute (JBI) Critical Appraisal Tool39,40 to 117 included studies from 2000 to 2020. This review found no correlation between program curriculum content and improved outcomes,7,41 but identified a statistically significant correlation between having mixed faculty in terms of (a) internal/external to the organization and (b) experts/practitioners and organizational outcomes. 16
These two reviews provide unique clarity regarding the most reliable evidence in the field based on 30 high-quality studies. This exclusive subset can inform future research and programming and potentially enhance their quality and maximize their impact. 15
Context (professional and academic) and article purpose
The need for robust leadership development is particularly urgent in healthcare, especially since internationally, the sector is plagued by a severe Human Resource (HR) crisis, marked by massive staff and leader shortages, high turnover, expected retirements, 42 and droves of rapidly promoted leaders who have not received adequate—or any—preparation for those roles.8,22,43 Many of these “battlefield promotions” are early- to mid-career nurse leaders, who, having survived their trial by immersion, are now requesting formal training.44,45
The need to provide leaders in healthcare and other sectors with evidence-based programs20,22,46 is mirrored by a further knowledge gap regarding how top-quality evidence can be integrated into programs.
The Canadian Nurses Association (CNA) and the Canadian College of Health Leaders (CCHL), partner organizations, addressed this challenge when healthcare organizations approached them requesting leadership development specifically for nurses. In response, the design team created a customized 47 novel intervention, called the Inspire Nursing Leadership Program (INLP), which had not yet been delivered when this article was first written.
The purpose of this article is to describe the outcomes- and evidence-based process that the INLP creators implemented, including how they incorporated gold standard elements of program design, delivery, and evaluation, as well as of top-quality research, into the program design.
To the best of our knowledge, this is the only published account of this kind of application of evidence to either program or research designs. The intent is to provide a credible foundation for the design of other programs and studies in healthcare and beyond and to potentially improve their quality and impact.
Design of the Inspire Nursing Leadership Program
The core design team of the INLP included the CCHL Vice-President of Research and Leadership Development, the CCHL Senior Vice-President of Professional and Leadership Development, and a CCHL Faculty, with input provided by others described below. This section outlines how the team applied the 7-step outcomes-based design approach created by Geerts et al. 15 and incorporated each of the gold standard elements listed in Table 1. The latter includes alignment with Knowles’s principles of adult learning, which are: (pre-program) motivation to learn, self-directed, participants’ experience as the basis, relevant and practical content, and outcomes-based. 36
1. Conduct a needs and gaps analysis and establish an empirical foundation
Step 1 involved conducting a comprehensive needs and gaps analysis based on meetings with representatives from client organizations, to ensure the program would address the prospective participants’ professional context precisely.22,48
To establish an evidence foundation, two authors conducted a literature search for reviews of nurse leadership development from 2010 to 2024, guided by a University of Manitoba specialist librarian. This resulted in 14 unique reviews. Since none systematically isolated the best available evidence of program elements linked to outcomes, the team consulted Geerts et al. 15 and Lyons et al. 16 Despite their medical focus, many of included studies in these reviews included nurse participants. Further, research evidence confirms that empirically based components of effective leadership development translate considerably across sectors and professions within healthcare.15,49
With this empirical foundation, the lead author drafted an initial program. To enhance its validity among nurse leaders, a Registered Nurse (RN) and CCHL Leadership Faculty designed the full program, with input from several Subject Matter Experts (SMEs), including from the CNA Indigenous Council, the Canadian Indigenous Nurses Association, and an Equity, Diversity, and Inclusion (EDI) specialist.
The purpose of the INLP is to increase the leadership capacity of nurse leaders in their organizational and community contexts, including to facilitate quality and system improvement.
2. Select program desired outcomes
Step 2, informed by step 1, involved selecting desired outcomes according to an extended version of the Kirkpatrick framework
50
to achieve this purpose. INLP desired outcomes include enhancing nurse leaders’: - Self-awareness and confidence as leaders (Level 2A), - Leadership capabilities (knowledge and skills, Levels 2B, and behaviours (Level 3)), including cultivating partnerships with local community members and leading improvement initiatives, - Familiarity with a leadership framework as the common language to facilitate change (benefit to the organization, Level 4A), and - Capacity to positively impact patients (Level 4B), staff, and communities, with consideration given to economic and sustainability impact.
A key curricular foundation is the LEADS in a Caring Environment Leadership Capability Framework (LEADS), 51 which is comprised of 5 domains and 20 capabilities, with behavioural descriptors at 4 levels of leadership for each capability. This framework is the basis for much of the CCHL programming, including its 360-assessments, and is reported to be the most widely used resource of its kind in healthcare in Canada.52,53 Integrating LEADS organization-wide has been empirically correlated in multiple sites with improved outcomes at the individual and organizational levels. 54
3. Select explicit program goals
To achieve the desired outcomes, the design team identified 5 program goals (Table 1), which are stated prior to registration and at the beginning of the program, are revisited throughout, and are included explicitly in the evaluation framework. At the outset, INLP participants also select personalized goals and desired outcomes, 55 including 3 leadership capabilities to develop, and goals and desired outcomes for their Leadership in Action (LiA) projects.3,56 Personalization enhances perceived relevance and application of learning.57–59
4. Select participants intentionally
The INLP features cohorts of 15–24 participants and is intended for early- to mid-career nurse leaders. Participants are usually nominated by their supervisors or apply and are selected based on their leadership potential to meet the priorities identified in step 1.35,37
5. Select program details (structure, content, faculty, and components) and prioritize evidence-based elements
Step 5 involved incorporating the gold standard elements (Table 1) and selecting the corresponding program details to best achieve the program goals.
Structure
Structurally, the INLP involves 3 months of blended learning, 60 including 8 hour-long synchronous virtual sessions and a central 2-day residential component. The total time commitment, including asynchronous requirements inbetween modules, is 45–50 hours. The INLP can be delivered as an open-enrolment or organization-specific intervention. 16
Content
The content covers the 5 domains of the LEADS Framework: Lead self, engage others, achieve results, develop coalitions, and systems transformation, with a focus on supporting participants to design and implement LiAs. EDI is interwoven explicitly throughout.
Faculty
Faculty with a nursing background are prioritized, along with a mix of internal/external and expert/practitioner. 16
Delivery
In addition to effective facilitation techniques, the delivery aligns with the principles of adult learning. 36 This involves self-directed aspects, involving participants’ insights and experience as valuable learning resources throughout, and application exercises.
Components
Of all gold standard components, the INLP includes the following (based on a novel framework):
38
- - - - - -
Along with selecting components specifically based on their intended efficacy in achieving program goals, it is important to provide a variety to appeal to different learning preferences.59,61,73
6. Develop a robust complementary evaluation framework
Program evaluations typically only assess participant satisfaction (Level 1), 1 but a robust evaluation framework can enhance outcomes by providing focus, motivation, and accountability5,32,74 and can demonstrate ROI. 75 For example, tangible LiA outcomes, particularly economic, such as cost savings, can enable organizations to calculate the program ROI, measured against the expense and opportunity cost of the program.
The INLP evaluation framework: Participant outcomes.
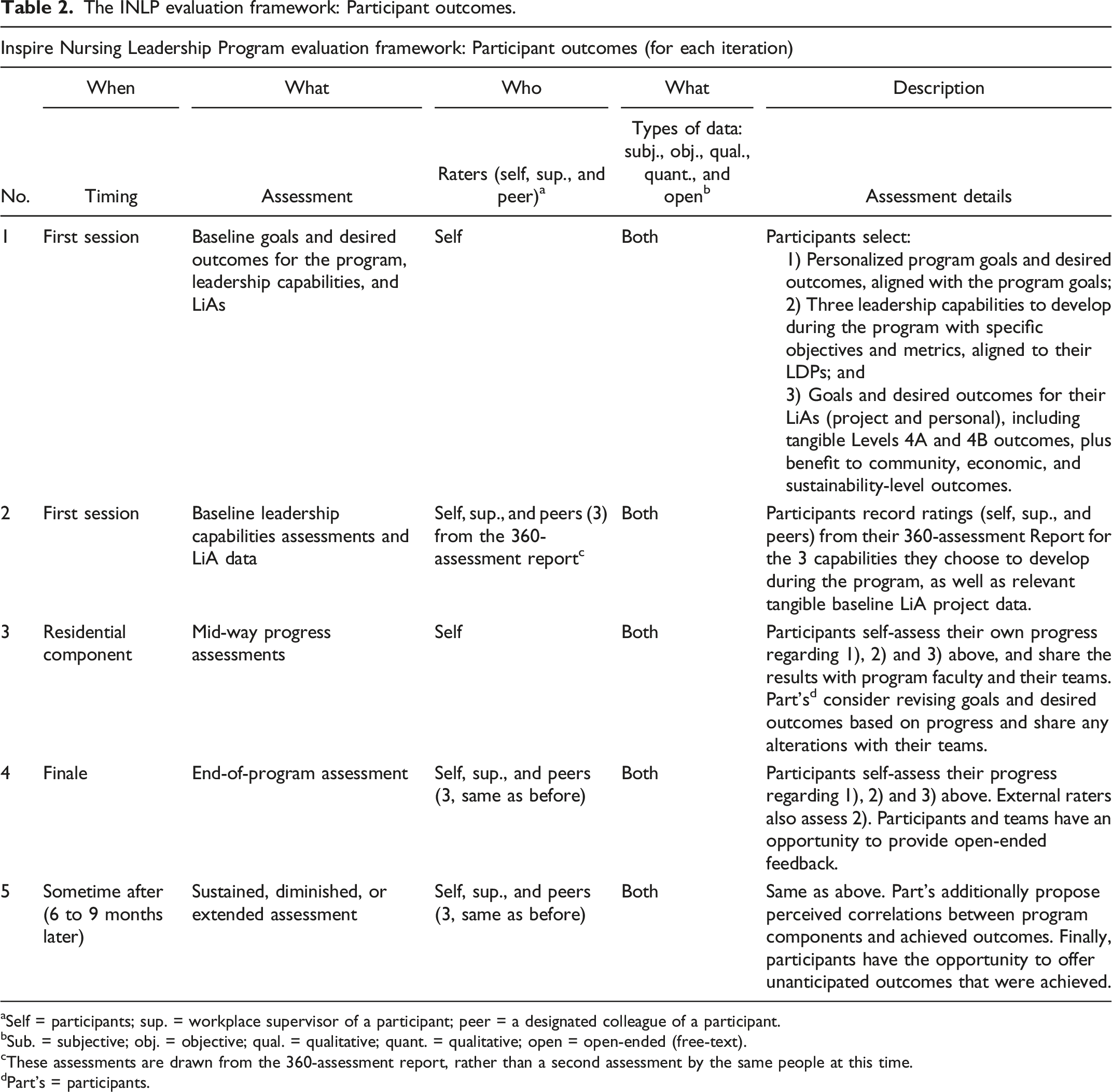
aSelf = participants; sup. = workplace supervisor of a participant; peer = a designated colleague of a participant.
bSub. = subjective; obj. = objective; qual. = qualitative; quant. = qualitative; open = open-ended (free-text).
cThese assessments are drawn from the 360-assessment report, rather than a second assessment by the same people at this time.
dPart’s = participants.
7. Embed an application of learning/training transfer strategy
The quintessential hallmarks of successful development are improved tangible outcomes and yet, the process of participants applying their learning to work is not automatic or guaranteed.7,13 Without effective transfer strategies, even outstanding programs can underperform or fail.7,18
Accordingly, the INLP requires participants to apply their learning through exercises inbetween modules and through the LiAs, experiences which are debriefed afterwards and are reinforced by reflection activities. These iterative learning-cycle steps 76 can enhance learning, since participants can discuss their experiences and lessons learned after each cycle, with support from program faculty. Accountability is also augmented by requiring participants to report their progress to program faculty and to their accountability teams (see below) throughout.
Strategies to enhance outcomes and support organizational receptivity to change include involving participants’ colleagues through the 360-assessments and accountability teams, as well as requiring participants to engage with colleagues and community members before launching their LiAs to ensure that the importance and goals are shared. These measures can also enhance the support others provide.77,78
Gold standard evaluation and research design
The following sections demonstrate how the gold standard elements were incorporated into the INLP evaluation framework (Table 2) and into a potential subsequent research design.
Evaluation framework: Program
Participants’ evaluation of the program is preceded by creating their own personalized goals. Mid-way, they self-assess progress toward achieving program and personal goals, as well as rating their satisfaction with the program and its components thus far. These evaluations are repeated during the final session and sometime after, along with enabling participants to propose program improvements. Participants are also asked to identify any program components that they perceive were most directly linked to specific improved outcomes.
Evaluation framework: Participant outcomes and accountabilities
Similarly, evaluation regarding participant outcomes is preceded by establishing baseline scores for the three designated leadership capabilities that they aim to develop and tangible LiA baseline data. INLP participants identify a core accountability team, called “the team”, ideally including their workplace supervisor, program colleagues, and three non-program colleagues, and share results periodically. This transparency establishes an informal social contract and can increase outcomes,7,79 as well as prompting the team to offer any requisite support or resources to enable success.77,78
Participants share their goals and baseline metrics with their teams, followed by their self-ratings mid-way, which can enable course correction and goal revisions or extensions based on progress.80,81
At the program conclusion, participants repeat the process. Team members also rate the frequency with which participants demonstrate their 3 designated leadership capabilities effectively, along with providing qualitative feedback. Participants share the synthesized results with the program faculty and with their teams, along with any revised goals and metrics. They repeat this process 6–9 months later.
External ratings and tangible LiA outcomes provide objective data, which can demonstrate the program’s ROI and can increase external validity and minimize bias, compared to self-ratings alone. 82
Finally, at the finale and afterwards, participants may propose any unanticipated outcomes that were achieved, along with any supporting evidence.
Foundation for a subsequent high-quality research design
The majority of research in the field is of unreliable quality, which is problematic.15,23–25 Robust study designs, conversely, can advance knowledge and potentially enhance the quality and impact of interventions,15,22 minimizing the notorious research/practice divide.83,84
Consequently, the INLP team embedded key elements in the design of the program to ensure that once it had been delivered and data had been collected, a subsequent research study would align with the criteria for gold standard quality in Geerts et al. 15 These elements included collecting data from multiple iterations of the program to address generalizability, securing high response rates by administering evaluations during synchronous sessions, collecting objective data pre- and post-intervention through external raters and tangible LiA outcomes, targeting benefit to patients outcomes (Level 4B), and exploring the relationship among program variables (program components and outcomes).
In addition to potentially contributing to the scholarly knowledge base, aligning to top-quality research criteria bolstered the INLP design.
Discussion and limitations
The purpose of this article is to describe the process by which the INLP design team applied an outcomes-based approach to create the program, including how they incorporated gold standard evidence and components of top-quality research, concomitantly. This article is the first to demonstrate these applications, which is vitally important in healthcare, given the high stakes, considerable investment of money, time, and resources, and the predominantly unreliable knowledge base.
Despite limitations associated with publishing before initial program delivery and evaluation, given the robust evidence-based design, implementation lessons are anticipated to reveal nuances, rather than foundational flaws. First iterations of the program will yield early data, lessons, and opportunities to refine the design accordingly and to report these evolutions when publishing.
A second potential limitation concerns the extent to which lessons from this novel program for nurse leaders in Canada might apply to other contexts, such as different levels of leadership, professions, sectors, and geographical locations. Research indicates that credible evidence has the potential to be considerably generalizable.
Further research and practice
Further research could identify other gold standard studies, including those from other sectors, to expand the existing pool, and to analyze the extent to which key principles translate effectively to different contexts. Future research and practice could also explore alternative applications of the gold standard elements in various contexts, as well as which program components and formats correlate with specific desired outcomes, supported by objective data. It would also be interesting to explore how artificial intelligence can enhance development and training programs. Finally, beyond individual interventions, investigating evidence-based strategies for organization-wide leadership integration, development, and support toward becoming a Leadership Organization would be beneficial.
Conclusion
There is an urgent need to support leaders, particularly in healthcare, with programs based on high-quality research evidence. This calibre is crucial, given the context of the current health HR crisis, the risk of potentially wasted spending and other adverse consequences, and the parallel opportunity to potentially improve and transform health systems.
Footnotes
Acknowledgements
The authors would like to thank Tim Guest and Misty Fortier (CNA), Brenda Lammi and Alain Doucet (CCHL), Caroline Monnin (University of Manitoba), and Dr. Ibrahim Jahun (University of Manitoba) for their excellent contributions, as well as the guest and managing editors and the anonymous peer reviewers for their insightful suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.