
Abstract
The idea that actions of people, organizations or governments may lead to Unintended Consequences (UICs) is not new. In health, UICs have been reported as a result of various interventions including quality improvement initiatives, health information technology implementation, and knowledge translation, especially those involving translation of broad policies (evidence-based medicine and patient-centred care) or system level improvement into actionable items or tools. While some unintended consequences cannot be anticipated, others may be predictable. In this article, we present a model based on cultural historical activity theory, which may help policy-makers, health leaders, and researchers better anticipate UICs resulting from implementation of new programs or technologies and take action to address them or mitigate their risk of occurrence. We support this model using examples of UICs of implementing family centred care principles, electronic health records, and computerized templates for quality improvement in chronic disease management.
Background
The idea of Unintended Consequences (UICs), that is, outcomes of human and social purposive action that are different from those initially planned or anticipated, is not new. Health systems, in general, provide numerous examples of UICs including those resulting from clinical interventions, quality improvement initiatives, and health information technology.1-3 Specific examples include the following: fall prevention policies leading to “an epidemic of immobility;” 4 implementation of performance measurement program leading to inappropriate clinical care, decrease in provider focus on patient concerns, and compromising patient education and autonomy; 5 quality improvement resulting in increased costs and health disparities, or “caring only for patient populations amenable to high performance on quality metrics;” 6 and health information technology implemented to improve efficiency but leading to more administrative work for clinicians and clinician burnout. 7
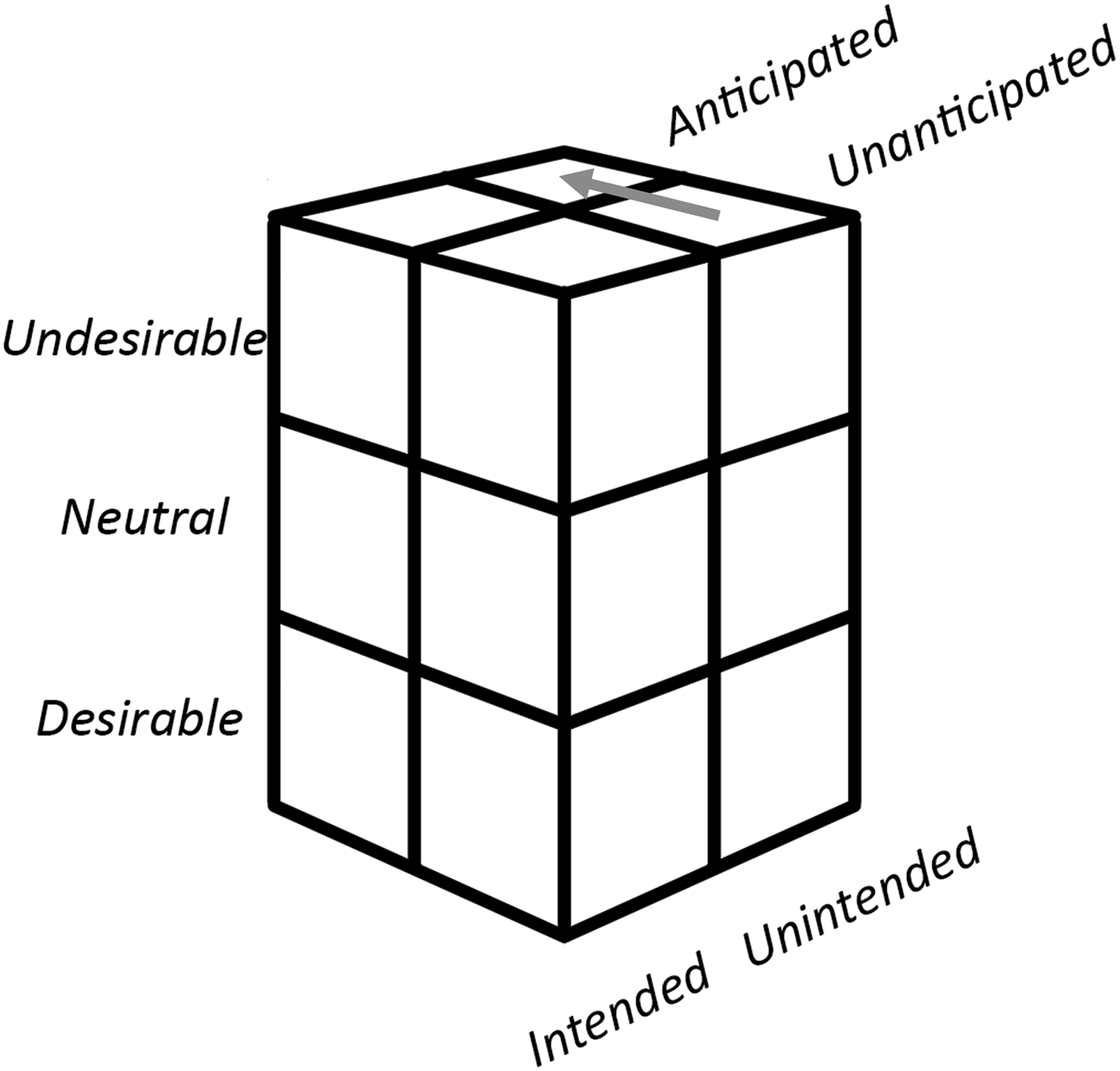
Unintended consequences may be positive, neutral, or negative, and although the terms unintended and unanticipated consequences are often used interchangeably, UICs are not necessarily unanticipated (Figure 1). A contemporary example of the distinction between unintended and unanticipated consequences is provided by COVID-19, where steps taken in response to the pandemic such as prohibiting large gatherings, closures of schools and non-essential businesses, and travel restrictions had negative impacts on education and the economy in many countries. While this “collateral damage” is by no means intended, it was not entirely unanticipated either. Techniques such as scenario planning and systems modelling may have helped in mitigating some of these outcomes. Other, perhaps less anticipated, UICs of COVID-19 mitigation strategies include increase in domestic violence and alcohol consumption.
8
Finally, COVID-19 also provides an example of positive UICs in that less travel during the pandemic resulted in lower levels of air pollution and greenhouse gas emissions.
9
While much research has focused on characterizing and classification of UICs in health, there is a dearth of work on how UICs occur and the relationship between unanticipated and unintended consequences. Classification of consequences based on intention, ability to anticipate, and outcomes. Arrow indicates the goal of the proposed model (Adapted from Turcotte-Tremblay).
8
This article begins to address this shortcoming by reviewing some of the causes of UICs suggested in the literature. We then propose a new model of system change that includes factors leading to select UICs, based on Cultural-Historical Activity Theory (CHAT). We focus specifically on UICs that are associated with implementation efforts, that is, “the systematic uptake of research findings and other evidence-based practices into routine practice, and, hence, to improve the quality and effectiveness of health services and care.” 10 This model may help health leaders and policy-makers gain awareness of the circumstances under which negative UICs arise, and enable them to be proactive in anticipating, preventing, or mitigating them.
What causes unintended consequences?
In his seminal 1936 article “The unanticipated consequences of purposive social action,”
11
sociologist Robert K. Merton proposed the following five causes of UICs, which are not mutually exclusive: 1. Inadequate knowledge. 2. Error. 3. Activities meant to achieve the short-term intended consequences while ignoring potential long-term UICs, which Merton labelled “the imperious immediacy of interest.”
11
4. Basic values that lead to outcomes contradicting the same values. The example provided by Merton is of the Protestant values of hard work and asceticism that “paradoxically leads to its own decline through the accumulation of wealth and possessions.”
11
5. The prediction itself leads to actions that affect the predicted outcome. For example, the identification of the Y2K bug and the prediction of its impact on computer systems around the world led to global efforts to fix the issue.
Others suggested that UICs may be caused by naivety or lack of awareness of the outcomes being pursued. 12 Furthermore, system complexity may contribute to UICs. Concepts from the literature on complex-adaptive systems, such as non-linearity, emergent self-organized behaviour, and adherence to simple rules can help understand the properties of a system and the conditions under which UICs occur. 13 Finally, several process models have been proposed to explain UICs in fields such as program evaluation and organizational change.14,15 However, we only found one framework specific to unintended consequences in health, which uses a sociotechnical perspective to explain unintended consequences of health information technology. 16
Cultural-historical activity theory
The perspective we propose here is different from the above system-level approach in that it uses activity as the level of analysis. It builds on concepts from CHAT, which originated from the works of Russian psychologists Vygotsky, Leont’ev, and Luria,17-19 and later expanded by Finnish researcher Yrjö Engeström.20,21
In CHAT, an activity consists of conscious actions and unconscious operations aimed toward a certain object (as defined below) and is viewed as a process, which exists within a social, cultural, and historical context. The unit of analysis in CHAT is an activity system, which consists of the following six elements with multiple interactions among them (Figure 2):21,22 1. Subject, the person(s) performing the activity. 2. Object, which “refers to the raw material or problem space at which the activity is directed, and which is moulded and transformed into outcomes with the help of physical and symbolic, external and internal tools.”
23
3. Tools or mediating artifacts utilized in the activity, including both material and conceptual tools (skills, competencies, methods, and procedures). 4. Rules that govern the activity, including how subjects interact with the object of activity, the tools they use, and the ways in which they use them. 5. Community, other actors involved in the activity. 6. Division of labour, the division of activities amongst those who participate in them. The activity system.

Implementation science recognizes the interdependence between individual (micro), organizational (meso), and policy (macro) levels, which “determines which strategies are more likely to successfully implement change.” 24 The advantage of CHAT for implementation science research, change management, and understanding UICs specifically is that it is especially suitable for capturing the micro-macro level interaction.
The proposed model focuses on three elements of the activity system: the object of activity, rules, and tools. In CHAT, the object of activity represents both something that is acted upon, an objectified motive, and desired outcome. 22 Rules in CHAT are part of the context in which the activity takes place. They govern the activity, including how subjects interact with the object of activity, the tools they use, and the ways in which they use them. Rules can be either explicit (e.g., formal requirements and legislation) or implicit (e.g., norms, world views, value systems, and conventions). As such, rules are deeply rooted in, and arise from, the broader context of history, culture, and society. Finally, people often use tools or mediating artifacts in their activity. Some tools are technological (physical) and others are symbolic (e.g., language).
A CHAT-based model of unintended consequences
As Guowei 15 noted, “in planned organizational change, intensive social interactions take place on at least two levels: senior management and employees.” While the role of management is to initiate change and develop policies and procedures to govern it, the role of employees is to translate them into practice. Thus, from a CHAT perspective, the process and activities of implementation involve translating rules into tools, which are then employed at the activity level. However, there are some notable differences between rules and tools; especially when the rules are implicit and macro-level (e.g., general policies, philosophies, worldviews, or sets of guiding principles). Macro-level rules are often general, unstructured, adaptable, and somewhat ambiguous and open for interpretation. In contrast, tools are concrete, structured (less adaptable), clear, and often prescriptive in nature. Thus, by translating rules into tools we gain structure, clarity, and actionability.
But what do we lose? We may lose the bigger picture and the broader intention behind the tool, as well as some of the adaptability and personal interpretation of rules. As Kaptelinin et al. put it: “on the one hand, tools expand our possibilities to manipulate and transform different objects, but on the other hand the object is perceived and manipulated not ‘as such’ but within the limitations set by the tool.” 25
Second, tensions may arise between intention and operationalization of the principle, philosophy, or policy. The tools themselves, rather than the macro-level rules behind them, may become the focus of work activities and perceived as rules in the sense that they govern the subject’s interactions with the object of activity and with others in the community. This is especially true if the use of the tool is perceived as an administrative demand. 22
Lastly, following the implementation of tools, the activity system itself may change such that using the tool may become the object of the activity in and of itself (Figure 3). Sometimes, this is implicit but in other times, it is made explicit through new rules that mandate the use of the tool(s). The examples in the following section demonstrate how these issues, and especially changes to the object of activity, can sometimes lead to undesirable UICs. A proposed model of unintended consequences of implementation efforts, based on cultural-historical activity theory.
Unintended consequences of rules translated into tools
Difficult decisions for children with medical complexities
The first example to demonstrate the above idea comes from a study of physicians’ difficult decisions concerning children with medical complexities. 26 Throughout this study, it was found that two high-level rules guide physicians in the process of decision making. The first is providing Evidence-Based Medicine (EBM) and the other is Family Centred Care (FCC). Both EBM and FCC acknowledge the need to engage patients (or families) in the process, either by considering their values (EBM) or as full partners in the care process (FCC).27,28 While EBM has been very successful in providing explicit rules and a variety of tools to search for, retrieve, and appraise scientific evidence, what is meant by incorporating patient values remains vague, and often there are no clear established ways to implement it in practice. The same applies to engaging families as “full partners in the provision of healthcare to children,” 28 which is a core tenet of FCC.
One of the ways for physicians to overcome this ambiguity was to ask family members of children with medical complexities a set of standard questions to elicit their values, needs, and preferences. 26 What happened as a result is that asking (and answering) the questions became the object of the activity in and of itself. However, this new activity, which is part of the greater activity of making a difficult decision, often did not serve to provide care that is more family centred. Instead, it helped physicians frame their perspective in a light that is acceptable to the family. Rather than reflecting the true partnership spirit of FCC, using the tool (standard questions) resulted in a practice that was more consistent with a paternalistic model of care, whereby the doctor makes the decisions for the patient. 26
Meaningful use regulations for electronic health records
The second case is the implementation of Electronic Health Records (EHRs) via the Meaningful Use (MU) regulations in the United States.
Recognizing the need for high quality data for research and quality improvement, the first phase of MU provided incentives for physicians and hospitals to document and report data in structured ways to improve data quality and enable information retrieval and analytics- and sanctioned them if they did not meet the targets set in the regulations. 29 One of the intended consequences was rapid increase in EHR adoption and the development of structured data entry and reporting tools within EHRs. 30 However, this came at a cost. Caring for patients now involves additional documentation and reporting burden to the extent that in some cases physicians spend more than 50% of their time interacting with the EHR (often after clinic hours), and this additional work has been associated with increased physician burnout. 31 In other words, a whole new activity system around documentation and reporting has been added to the existing activity system of patient care.
Certainly, EHR design issues are adding to the problem; 32 however, it has been noted that policies, regulations, and organizational practices are also important contributors. 33 This case illustrates our idea that high-level rules (quality improvement manifested through MU policies and regulations) translated—perhaps poorly—into tools (EHRs and data entry and reporting tools within them) may lead to UICs (more and new work for clinicians; burnout).
Electronic templates for quality improvement of chronic disease management
The last case is somewhat similar to the one above but is described at the level of the clinical encounter. In this case, reported by Swinglehurst et al., 34 electronic templates were implemented as part of the Quality and Outcomes Framework (QOF) in the United Kingdom to collect data about patients’ chronic conditions. The templates may be used for both support of individual patient care and to “produce aggregated data on costs and/or organizational performance.” 34 As the authors report, when these templates were used in clinical encounters between patients and nurses, they “change[d] the very nature of what it means to ‘care’ in the contemporary chronic disease clinic.” 34 For example, the use of templates often shaped the encounter around information gathering and the nurses often looked at the computer monitor when explaining the purpose of the visit to the patient, which is a well-documented negative impact of EHRs on patient-clinician communication. 35 The authors further illustrate how the templates might affect the nurse’s thinking and reasoning process and how they define what it means to be a patient, for example, by making it difficult to see the unique characteristics of individual patients, beyond the label assigned to them by the template, or to see the complexity of patients with multiple co-morbidities (as separate templates are used for each chronic disease). 34
Once again, this case illustrates high-level rules (from the QOF) that are translated into specific tools (electronic templates). When these tools are implemented at the micro-level (patient–nurse encounter), the object of activity becomes using the tool, which results in the UICs described above.
Discussion
Translating rules into specific tools is a common practice. In this article we propose that there are both gains and losses from this practice: while it often helps achieve intended goals, the introduction of new tools may critically affect multiple aspects of how the activity unfolds thereby contributing to UICs. Health leaders, managers, and policy-makers may be able to better understand how (and why) UICs of implementation and knowledge translation efforts occur, and potentially anticipate them by: defining and modelling the system; understanding the potential impact of system changes (rules to tools); and, determining options to manage the changes.
Throughout this process, one has to look at both macro and micro levels and how changes to one affect the other. Our model begins to do this by looking at the problem from the perspective of CHAT, which allows capturing both levels within a single unit of analysis.
Limitations
Our proposition does not, nor is it meant to, contradict the root causes and sociotechnical framework of UICs discussed earlier. Rather, it provides a level of specificity, and potentially more applicable way to anticipate UICs. The proposed model has not yet been tested and validated empirically in prospective research. It is unlikely that using it will prevent all UICs as there is always an element of uncertainty when implementing new initiatives in healthcare.
Conclusion
Health leaders need to move from simply reacting to UICs as they happen to proactively anticipating them and mitigating potential negative effects of implementation initiatives. The model we propose here can help with this challenge. This model should be further validated in future research and applied in practice to fully assess its utility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.