
Abstract
This scoping review examined the breadth and depth of evidence on Electronic Medical Record (EMR) implementation benefits in outpatient settings. Following PRISMA guidelines for scoping reviews, five databases were searched, and 24 studies were retained and reviewed. Benefits, facilitators, and barriers to EMR implementation were extracted. Direct benefits included improved communication/reporting, work efficiency, care process, healthcare outcomes, safety, and patient-centredness of care. Indirect benefits were improved financial performance and increased data accessibility, staff satisfaction, and decision-support usage. Barriers included time and financial constraints; design/technical issues; limited information technology resources, skills, and infrastructure capacity; increased workload and reduced efficiency during implementation; incompatibility of existing systems and local regulations; and resistance from healthcare professionals. Facilitators included training, change management, user-friendliness and alignment with workflow, user experience with EMRs, top management support, and sufficient resources. More rigorous, systematic research is needed, using relevant frameworks to inform healthcare policies and guide EMR projects in outpatient areas.
Introduction
Electronic Medical Records (EMRs) present opportunities to address challenges facing healthcare systems worldwide, through optimizing efficiency,1-3 reducing costs,1,3,4 increasing productivity,2,4 and improving the quality of care.1,2,4 EMR implementation has been extensively researched in inpatient settings, but little is known about its benefits, facilitators, and barriers in outpatient settings.5,6
Benefits Realization (BR), a core aspect of a project's lifecycle, is the practice of ensuring that measurable benefits are derived from a project’s outputs. 7 Sapountzis, Harris, and Kagioglou investigated the BR process in the healthcare domain and recommended adopting a common BR management approach to steer all healthcare infrastructure or service delivery programs and projects. 8 Moreover, they classified benefits as (1) tangible (hard/direct) benefits that can be quantified and measured and (2) intangible (soft/indirect) benefits related to the improvement initiative but not reportable for accounting purposes. 9
Canada Health Infoway established a Benefits Evaluation Framework for health information technology, with dimensions for service quality, system usage, and net benefits. 10 More recently, Lambley and Kuziemsky proposed a tactical framework with six overlapping categories to support an integrated EMR adoption strategy that considers the implementation context. These categories include change management, training, workflow, technology, environmental design, and exception monitoring. 11
Electronic medical record implementation has been extensively researched in inpatient settings. Previous reviews focused on outcome domains like finance and quality improvement, as the prospect of improved quality and performance was considered the primary motivator for adopting this technology. 12 Financial benefits achieved after EMR implementation were linked to reducing costs4,13,14 and increasing revenue through enhanced billing,13,14 more efficient operations,6,14 and better chronic disease management. 6 EMRs also improved healthcare quality through boosting time efficiency,4,15-17 increasing adherence to best-practice guidelines,4,15-18 facilitating patient monitoring,14,18 and minimizing medication errors.14,15,18
However, EMR implementation in outpatient settings has not been as widely studied. Given the diversity of conditions and cultures across healthcare settings, EMR adoption projects in outpatient settings must account for context in their implementation and BR plans. 11 While hospitals may have the resources and infrastructure to support implementing inpatient EMRs, outpatient areas are typically smaller in size and vary significantly in resource availability and capability for supporting the deployment of EMR projects. 19 This scoping review aims to examine the breadth and depth of reported evidence on EMR implementation benefits in outpatient settings and explore the associated facilitators and barriers.
Methods
Given the limited knowledge of available research on benefits, facilitators, and barriers of implementing EMRs in outpatient settings, we conducted a scoping review following the PRISMA extension for scoping reviews (PRISMA-ScR). 20
Information sources and search strategy
We searched five databases (Web of Science, Scopus, MEDLINE, PubMed, and CINAHL) in May 2018, and updated the search in August 2020, using a combination of keywords that cover four areas (Supplemental material A): (1) benefits, (2) EMRs, (3) healthcare processes, and (4) outpatient.
Eligibility criteria
Eligible articles met all the following criteria: (1) English language; (2) empirical research; (3) reporting EMR implementation results; and (4) outpatient setting. Non-empirical articles, commentaries, editorials, and expert opinions were excluded. We used the National Cancer Institute’s definition 21 for EMRs; eligible articles described a digital record of patient information accessible to all healthcare providers who make care decisions for that patient.
Selection of sources of evidence
A reference management software was used, with a manual second-round check, to remove duplicate articles. Two researchers screened the remaining unique articles against the eligibility criteria. Disagreements about study eligibility were resolved by consensus. The content and bibliographies of the included studies were investigated for additional relevant articles using a snowballing technique.
Data charting process and data items
An initial list of benefit categories across different domains (e.g., information technology, business, and project management) was compiled from prior research on BR management in healthcare, with particular attention given to Sapountzis et al.’s Benefits Realization Process for Healthcare8,9 and the Canada Health Infoway Benefits Evaluation Framework. 10 A coding scheme was developed to extract relevant information from the included articles (available upon request).
Two researchers independently reviewed each article and extracted: (1) general article information (e.g., journal); (2) methods; (3) level of analysis (e.g., patients and physicians); (4) benefits; and (5) facilitators and barriers. The extracted information was imported to a spreadsheet and discrepancies in coding were noted. The reviewers had a 95.5% agreement level; discrepancies were discussed and resolved by consensus.
Critical appraisal
The quality of each study was assessed via Thomson and Greer’s Classification of Evidence Levels scheme. 22 Using research design as the main criterion, randomized controlled trials ranked highest, scoring 2++. Case-control and cohort studies scored either 2+ or 2−, depending on their risk of confounding, bias, or chance. Non-analytical studies ranked lowest, with a score of 3. 22
Results
Selection of sources of evidence
The initial search identified 1,257 records, out of which 139 duplicates were removed. Two researchers excluded 999 records after screening titles and abstracts, then reviewed the full text of the remaining records and discounted another 99 articles. Disagreements about study eligibility were resolved by consensus. The content and bibliographies of the remaining 20 studies were investigated using a snowballing technique, leading to four additional articles. A total of 24 eligible articles23-46 were selected (Figure 1). Article search and selection process.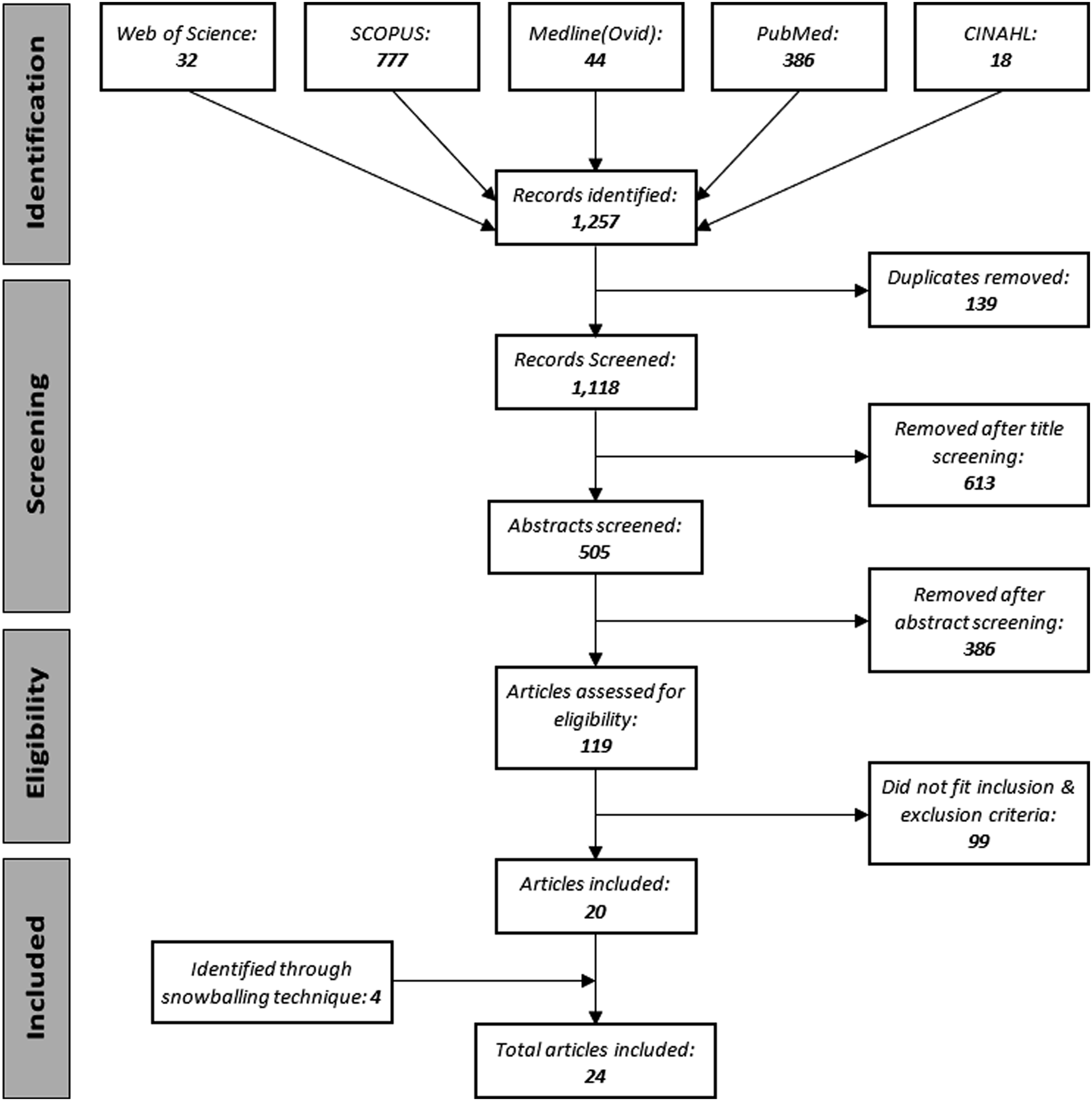
Characteristics of sources of evidence
Eight articles (33%) included in this review were published in clinical journals. Study duration ranged from 4 months to 3 years (mean: 17.5 months). Nineteen studies (79%) were conducted in the United States between 1996 and 2017. Settings included single-practice clinics, multi-practice clinics, hospital outpatient departments, and national physician surveys. Some articles contained both inpatient and outpatient data, presented separately; in these cases, only evidence related to outpatient settings was extracted.
Fourteen studies were quantitative, five were qualitative, and five used mixed methods. Twelve studies (50%) employed a post-assessment design, and the remainder had a pre/post-intervention design. Data collection methods included document analysis, focus groups, interviews, surveys, and database extraction. Primary data sources were physicians, nurses, administrative staff, other clinicians, academics/researchers, and EMR vendors. Secondary data included patient records and administrative data.
The quality of evidence was moderate to low (see Critical appraisal section). Seven studies scored 2++, eight scored 2+, six scored 2−, and three had a score of 3 22 (Supplemental material B).
Benefits, facilitators, and barriers
Benefits, facilitators, and barriers to EMR implementation across the selected studies.
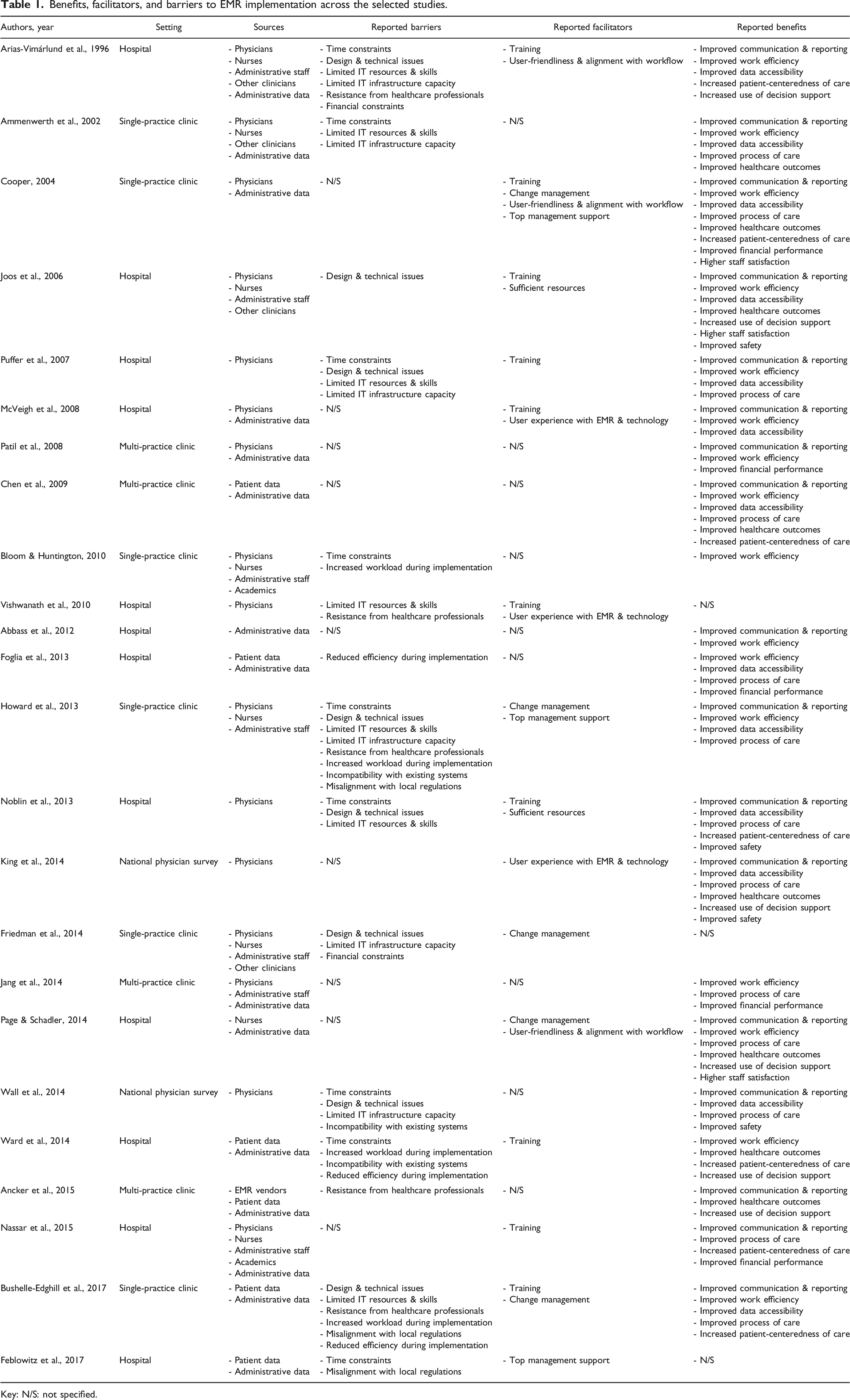
Key: N/S: not specified.
Six reported benefits were directly related to patient care (Improved Communication & Reporting, Improved Work Efficiency, Improved Process of Care, Improved Healthcare Outcomes, Increased Patient-Centeredness of Care, and Improved Safety), while the other four were associated with management activities and operations that support patient care indirectly (Improved Data Accessibility, Increased Use of Decision Support, Improved Financial Performance, and Higher Staff Satisfaction). A detailed description of the benefits, facilitators, and barriers as they appeared in the articles is available in Supplemental materials C–E, respectively. Supplemental material F summarizes our findings.
Variation across settings
The outpatient research settings were mutually exclusive. Most studies describing benefits came from hospital outpatient departments. Improved Communication & Reporting, Improved Data Accessibility, Improved Process of Care, and Improved Healthcare Outcomes were reported in all settings.
Reported benefits, facilitators, and barriers of EMR implementation across different outpatient settings.
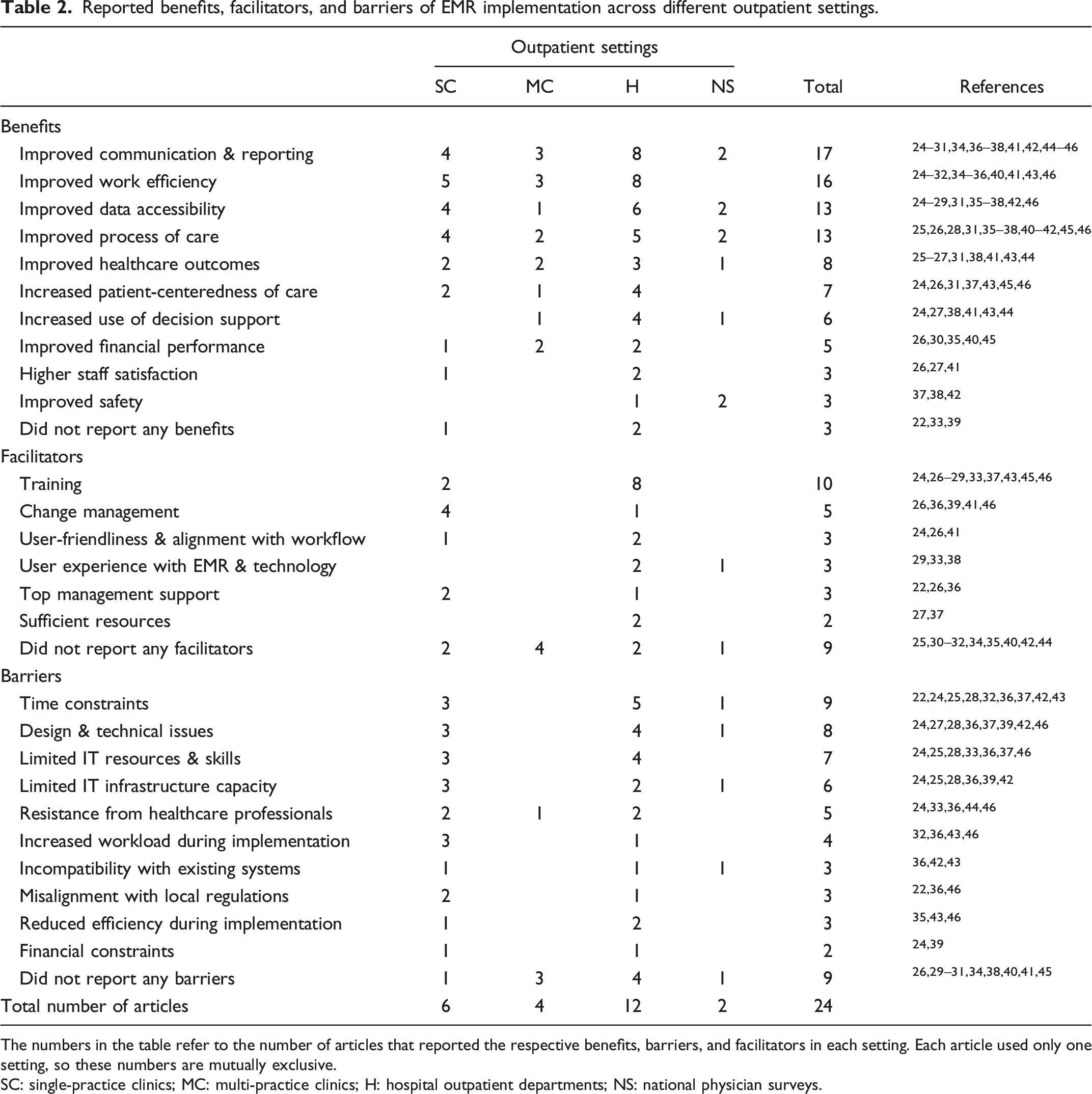
The numbers in the table refer to the number of articles that reported the respective benefits, barriers, and facilitators in each setting. Each article used only one setting, so these numbers are mutually exclusive.
SC: single-practice clinics; MC: multi-practice clinics; H: hospital outpatient departments; NS: national physician surveys.
Variation across sources of data
The sources of data in the selected articles were not mutually exclusive, with some studies using multiple sources. The most common data sources in the 21 articles that reported benefits were physicians and administrative data; the least common was EMR vendors. Studies with input from physicians reported all the benefits in this review, but only Improved Communication & Reporting was reported by all sources.
Reported benefits, facilitators, and barriers of EMR implementation by sources of data.
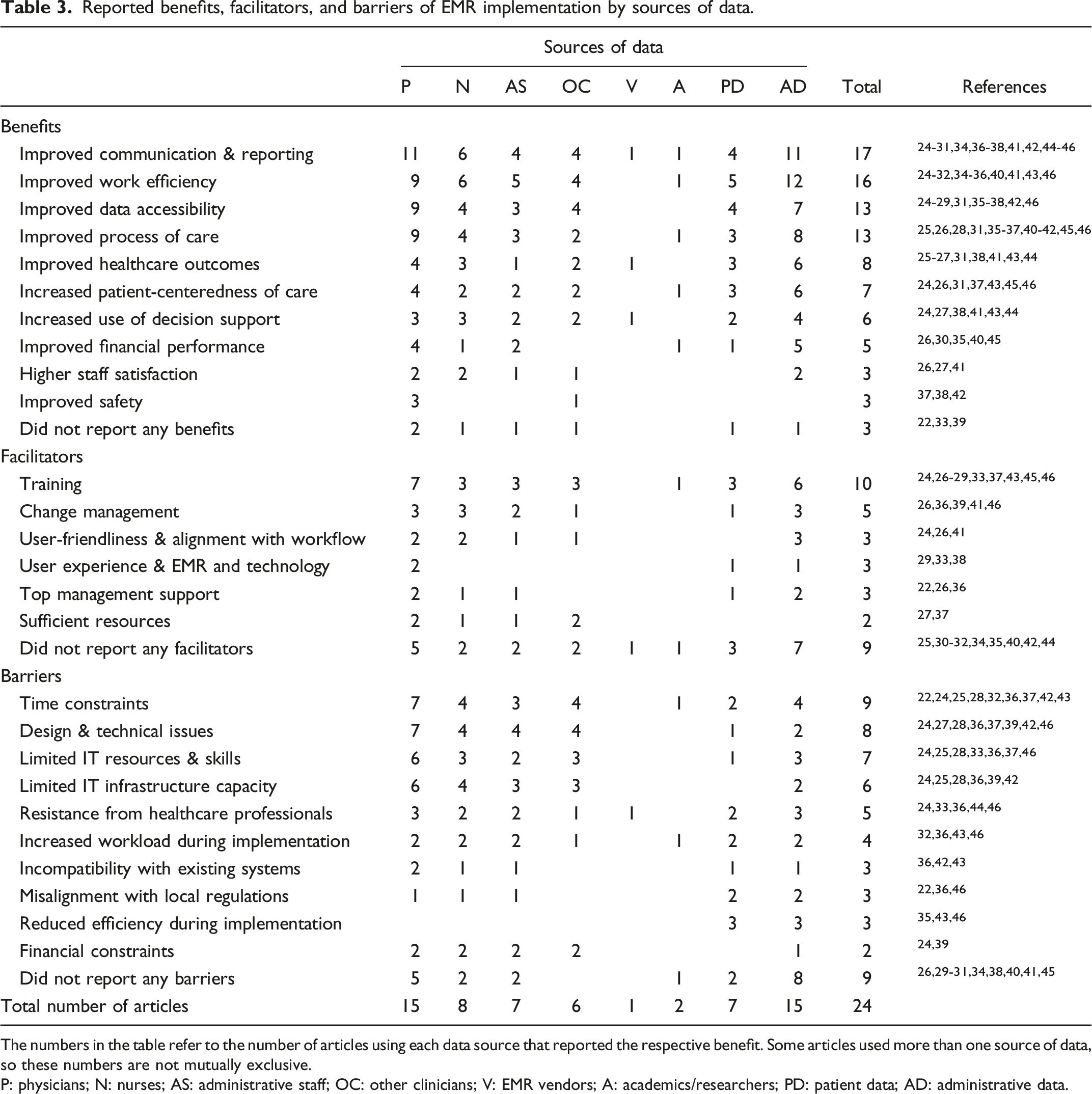
The numbers in the table refer to the number of articles using each data source that reported the respective benefit. Some articles used more than one source of data, so these numbers are not mutually exclusive.
P: physicians; N: nurses; AS: administrative staff; OC: other clinicians; V: EMR vendors; A: academics/researchers; PD: patient data; AD: administrative data.
Discussion
This scoping review aimed to evaluate the breadth and depth of research evidence on the benefits, facilitators, and barriers to EMR implementation in outpatient settings, and the evidence that was found was scant, narrow, and inadequate. There were challenges with the designs and rigour of the studies, which mostly presented clinical perspectives. Half the studies were set in hospital outpatient departments and a majority of 19 (79%) were conducted in the United States between 2010 and 2015, possibly linked to the 2010 Health Information Technology for Economic and Clinical Health Act that authorized incentive payments to clinicians and hospitals using EMR technology meaningfully to improve care. 47
The reported benefits varied across settings. Single-practice clinics commonly found improved work efficiency, care process, communication/reporting, and data accessibility, while multi-practice clinics most frequently experienced improvements in communication/reporting and work efficiency. The most frequently discussed benefits of EMR implementation in outpatient settings were improvements in communication/reporting, work efficiency, care processes, and data accessibility. Improved safety or healthcare outcomes appeared in relatively few studies, possibly denoting limited leveraging of EMR functionalities for evaluating healthcare quality in outpatient settings. This is further reflected in the small number of studies reporting on staff satisfaction or decision-support usage. Surprisingly, we found limited research that considered non-clinical benefits of EMR implementation in outpatient settings and little discussion of timeframes for achieving short-/medium-/long-term benefits.
Prior reviews on inpatient settings reported similar benefits as those observed in this review, including improvements in clinical documentation, workflows, workloads, productivity, financial performance, resource utilization, information availability, satisfaction, and quality of information and services.2,48 There was no consensus on the time required to realize benefits, but many suggested that benefits do not emerge automatically but are elicited by organizations facilitating EMR usage.28,36,39,49 Existing research on outpatient settings has limited information on timelines and organizational interventions to facilitate system use, but recommendations include promoting group norms related to the required EMR usage levels 49 and providing support during the transition period. 14 Future studies should examine the role of organization leaders in supporting enhanced EMR use and BR.
This review found that EMRs enhanced communication among healthcare providers23-26,35,36,45,50 and between them and their patients,23,30,35,36,50 potentially improving care quality.25,50 However, one study had contradictory findings: the EMR seemed to impair communication with patients during the visit but significantly improve follow-up communication. 36 This is consistent with a prior literature review that found that EMRs competed with patients for physicians’ attention by introducing new appointment tasks. 51 Researches should aim to develop a comprehensive, unified BR framework for outpatient settings that captures both EMR benefits and unintended consequences, accounts for the BR timeframe (short-/medium-/long-term), and enables more systematic and rigorous assessments of EMR benefits that can inform managerial and clinical decision-making.
This research focused on BR and thus does not view EMR implementation impacts through a holistic lens. However, some selected studies discussed negative and unintended effects. One study did not find sufficient financial improvement 1 year after implementation, 23 and others reported a transient reduction in patient satisfaction post-implementation 41 and that new documentation requirements reduced patient-clinician time. 36 Moreover, healthcare providers did not always perceive empirical, EMR-linked improvements in patient safety. 26 Sharing and disseminating evidence of these hurdles is critical for identifying mitigation strategies and preparing outpatient settings for EMR implementation projects.
Electronic medical record implementation facilitators and barriers reflect the variation in organizational environments that shape the resulting benefits, but the literature lacks a comprehensive assessment of these factors, given that only few studies reported this information. Most reported facilitators and barriers came from studies set in single-practice clinics and hospital outpatient departments. Multi-practice clinics provided limited information, reporting only one barrier and no facilitators, which calls for more research in this setting.
The facilitators reported most were Training and Change Management. Prior studies emphasize training as a success factor for EMR implementation in various settings,14,52 and the lack of training was often cited as a barrier. 19 Previous IT implementation research also emphasized change management as important for facilitating the implementation and BR of new technology. 6 Nevertheless, for EMR implementation in outpatient environments, the discussion of facilitators and barriers remains limited. This calls for more thorough investigation in this context, to optimize the success and the benefits of these new systems.
Knowledge-based barriers, like a lack of expertise or technical support, have been discussed in the literature throughout all stages of EMR implementation. 19 In line with this, technical issues and limited information technology resources were among the most common barriers in this review. These are important factors to address in the Canadian context of overloaded systems struggling with a shortage of providers.
Limitations
The studies included in this scoping review were primarily cross-sectional, with a majority conducted post-implementation. Eight studies had small sample sizes, some had poor quality of evidence scores, and 79% were conducted in the United States, which may not be representative of other health systems. Therefore, we recommend additional qualitative research on EMR implementation in outpatient settings to examine the implementation process, as well as quantitative pre-post assessments to accurately depict the changes in indicators related to benefits and impacts. Future studies should also focus on multi-practice clinics (e.g., Family Health Teams in Ontario), which are becoming more prevalent as healthcare systems move towards integrated patient-focused primary healthcare services. 53
This review only included English articles and the search strategy focused on studies reporting EMR benefits and thus might not have fully captured articles discussing only facilitators or barriers. Nevertheless, we searched five major databases and bibliographies of relevant articles, and our combination of keywords was comprehensive. Finally, outpatient settings are highly diverse in size, staffing, resource availability, management styles, and other factors that impact EMR implementation success. Thus, this scoping review sought to deliver an overview of the available evidence in this area, draw attention to existing research gaps, and guide future EMR implementation projects and studies in outpatient settings.
Conclusion
Electronic medical records are increasingly prevalent in healthcare settings, but their implementation often overlooks important considerations that would increase their chances of realizing benefits. This scoping review revealed scattered evidence on EMR implementation benefits, facilitators, and barriers in outpatient environments, with considerable variation in findings, rigour, and research methodologies across the included studies. Moreover, very limited research on EMR benefits considered facilitators and barriers to EMR implementation or examined the healthcare manager/leader’s role in shaping these benefits. Based on our findings, further research is needed to address the gaps we’ve noted in outpatient settings, and in the Canadian healthcare system context, to explore the potential outcomes of EMR adoption and inform future EMR implementation projects. More rigorous evaluations using existing implementation frameworks can support policy and management changes to facilitate more effective diffusion and optimal use of EMRs in outpatient settings.
Current literature on EMR implementation benefits, facilitators, and barriers varies considerably by setting and stakeholder perspective. A more systematic evaluation approach taking into consideration the particularities of the outpatient settings and the patient perspective is essential for informing future technology implementation projects and policies.
Recommendations
Considering the findings of this scoping review, we recommend that health leaders: • Ensure that all stages of EMR implementation projects are well planned and informed by existing evidence on what enables or hinders the process (i.e., facilitators and barriers), and consider realistic timeframes for achieving benefits. • Engage in research collaborations (practice-research partnerships) that would support a systematic assessment and a better understanding of the benefits that can be reaped from these systems and the factors that may hinder/facilitate their success. • Be prepared for the potential of EMR implementation projects causing a disruption in capacity and workflow and develop mitigation strategies to address the barriers commonly reported in the literature (e.g., time constraints, design issues, technical complications, and limitations in information technology, resources and skills). • Consider and develop a change management approach and encourage effective group norms that facilitate EMR implementation projects. Prioritize adequate training as the primary facilitator. • Monitor the risk level in the process of EMR implementation projects to enable timely adjustment and mitigation strategies that can optimize the chance of success. • Document best practices and unintended consequences of EMR implementation that can be used as a benchmark for other clinics and outpatient settings that consider adopting EMRs. • Manage the stakeholders’ expectations for benefits realization through effective communication about the timeline considerations and develop mitigation strategies for the anticipated challenges related to the potential disruption of regular activities and the transient reduction in patient satisfaction.
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Supplemental Material
Supplemental Material - Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review
Supplemental Material for Benefits, facilitators, and barriers of electronic medical records implementation in outpatient settings: A scoping review by Hamidreza Kavandi Zeina Al Awar and Mirou Jaana in Healthcare Management Forum
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.
Supplemental material
Supplemental material for this article is available on-line.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.