
Abstract
The field of health leadership is shifting rapidly, and there is an opportunity to learn with health leaders about what is needed to support health leadership education, research, and practice. In 2022, to augment student feedback and faculty praxis, Royal Roads University conducted 12 virtual interviews with senior health system leaders across various settings to learn how health leaders can better respond to emerging and future leadership needs and priorities facing health systems. Findings from this study informed the development of a health-specific elective for the Master of Arts in Leadership, Health Specialization program entitled Considerations for Health Systems Renewal. This elective explores the following topics that emerged from this research study: (1) an orientation to possibility; (2) emerging strategic human resource concerns; (3) healthcare innovation; (4) relational and social systems leadership; (5) polarity thinking; (6) trauma-informed leadership; and (7) Canadian healthcare networks. In this article, we share our research process and findings to arrive at these recommendations.
Introduction
The Master of Arts in Leadership, Health Specialization (MAL-H) faculty at Royal Roads University conducted a study to gather insights from senior health leaders on how to better respond to emerging and future health leadership needs. The goal was to design an evidence-informed health-specific course elective to support students in leading key challenges facing Canadian health system leaders now and in the future.
The research question guiding this inquiry was: How might health leaders better respond to leadership challenges facing health systems, both currently and in the future?
Guiding subquestions included the following: (1) What leadership challenges and polarities are alive in health systems and health leadership? (2) Based on first-hand experiences, what do health system leaders see as opportunities to strengthen the MAL-H? (3) What do health leaders see as current and emerging leadership learning needs to integrate into the MAL-H program?
Literature review
Canadians have an expectation that the public should fund our healthcare needs. 1 This expectation is also one of five national principles set out in the Canada Healthcare Act, with the remaining four being universality, comprehensiveness, accessibility, and portability. 2 Each of these principles requires management to be manifested and also involves leadership across an array of topics ranging from personal, relational and systemic leadership.
Renowned author Barry Oshry described how our collective blindness to system contexts can thwart strategic efforts in even the most highly regarded institutions and organizations. 3 Oshry asks us to consider the various patterns of relationships that constitute an organization as we remain focused on productive partnerships amid changing social conditions. Shifts in social system contexts, patterns, and processes require leaders to consider their centrality to systems and how what we experience is a function of our reflex responses, what he termed “the dance of the blind reflex.”3-7 Leadership skills and strategies are context-specific; we need to adapt our strategies depending on the particular pattern of relationship we are in.
Van Aerde noted, “The ultimate external crisis [in the health system] can be triggered at any time by an economic collapse or a global pandemic disease.” 7 Van Aerde added that internal and external stresses in our human-made systems were indeed exposed during the pandemic. 8 We now find ourselves facing the very stressors and conditions Homer-Dixon 9 noted when he used the term “catagenesis” to describe the process of growth that can emerge from a crisis—the two are inextricably linked. This sense of renewal borne from a crisis is arguably a leadership opportunity facing health leaders today—an inflection point requiring leadership optimism, creativity and an orientation to possibility.
Recent strains on health systems exacerbated Human Resource (HR) staffing shortages 10 , made worse by burnout, mental fatigue, and unprecedented demand on frontline staff, signals a need for compassionate, trauma-informed leadership.11-15 In hindsight, researchers found three cognitive antecedents to leadership failure during the crisis phase of the COVID-19 pandemic: (1) ignoring the precautionary principle, (2) the illusion of taking control, and (3) poor uncertainty management tactics. 16 These antecedents can serve as indications of the shifting leadership practice and our need to continually adopt a systems mindset when framing leadership development.
Further, the COVID-19 pandemic revealed some liabilities in how leaders approach problems and tensions in human social systems, where some issues are unsolvable, unstoppable and unbreakable. Polarity management16-21 is a helpful framework for understanding the tyranny of the “OR” and the genius of the “AND.” Researchers have noted, for example, that the issue of staff well-being and patient well-being is a polarity to be managed and not a problem to be solved.22,23 In other areas of healthcare, a polarity framework may help leaders who need to manage polarities such as centralization AND decentralization, tasks AND relationships, and perhaps more recently, strategy AND tactical leadership. 24
Lastly, if innovation in our healthcare system is to occur, innovation will happen locally and be physician-involved. 25 Accessing sources of support for healthcare innovation is essential for systems transformation 26 while concurrently contributing to high-quality patient outcomes.26-28
Within today’s healthcare landscape, inquiry to inform leadership development is timely.
Methodology
Participant ID, sector element, and current position.
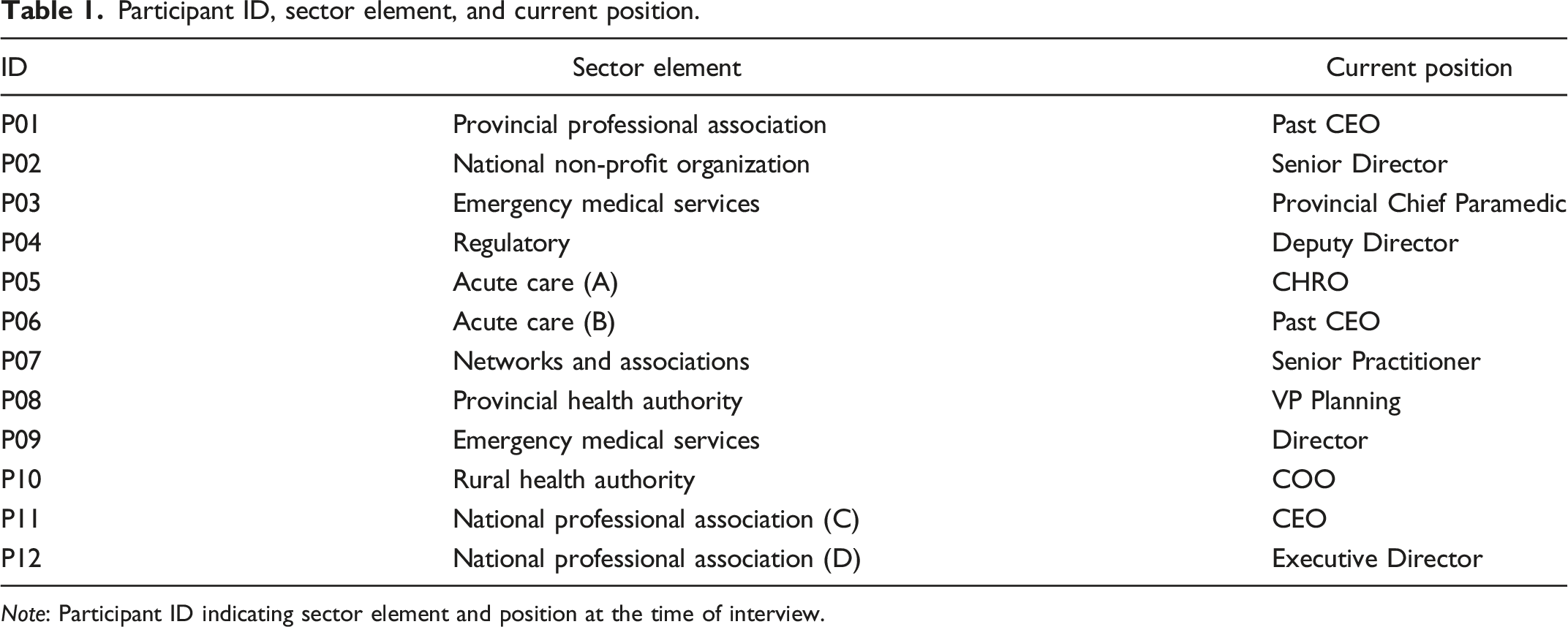
Note: Participant ID indicating sector element and position at the time of interview.
Interviews were recorded using Zoom™ and synced with Otter.ai—an automated transcription software platform. Each file was reviewed for interim thematic analysis, formatted, and member-checked for accuracy and anonymity. Research questions are available upon request.
Results
We conducted a thematic content analysis to identify patterns in the data. 30 Specifically, we used Braun and Clarke’s coding framework (familiarization, coding, themes, reviewing themes, defining and naming, and report writing) to yield the following findings. 31
Thriving in a world of volatility, uncertainty, complexity, and ambiguity amidst ever-changing demands is an ongoing reality for health system leaders. Participants described constantly changing work pressures, shifting political considerations, and emergent priorities as characterizing their day. For example, participant 03 commented, “There is no real [sic] typical day anymore. We seem to jump from fire to fire right now.” Participant 01 added, “[previously] there was some manufactured urgency, but at this moment, it is actual urgency.” In a similar vein, one provincial leader said, “Well […] for me, it's making plans and then changing those plans” (P09).
The ability to manage competing priorities is a core skill moderated by context. Participants frequently noted that pre-pandemic, they could focus on one specific element or priority; however, priorities have shifted, causing a re-focusing of effort often at the expense of a different competing priority. For example, a participant working in a strategic planning role said, “In my base position … it would be probably 95%, dealing with what's happening today, and trying to find some time to deal with what's happening in the future” (P09). While this person described the focus on tactical elements of their professional role and the resulting impact on longer-term planning, others described the opposite. For example, one CEO described their organization’s ability to balance the strategic and tactical focus despite the turbulence of the pandemic when they said, “We're still in the pandemic, we refreshed our strategic plan, with a co-design model with engaging patients and everybody else in strategic planning, which you wouldn't normally have done during a shorter-term crisis” (P06).
One example of competing priorities was in the area of staff burnout where staff prioritized serving patients while neglecting one’s own needs. To develop one’s leadership practice, Participant 12 recommended that people “take time for yourself in the broadest sense because we're burning out. I mean, two-thirds of the docs are burned out now. Seventy percent of the nurses … and we don't have anybody to replace them. So many priorities …”
Authenticity and critical self-reflection sustain leaders over time. Participants described self-awareness and authenticity as fundamental to their leadership during the acute phase of the pandemic. One participant noted how they adopted a practice of starting meetings and appointments 10 minutes past the hour to allow for personal reflection and connections with others and to ground themselves to approach their interactions authentically. This interviewee said, “It allows me to depart one conversation and create space, mind space, more than anything, to be able to tackle another conversation … It's my core values around compassion and being able to listen” (P08).
Relatedly, one CEO commented, “I keep coming back to authenticity. You're careful how you speak, but you're not somebody different. I found that [authenticity] to be very important from a leadership perspective” (01), where according to Participant 09, “authenticity is being grounded in personal values of integrity, truth, and high ethical bar.”
A looming HR shortage is a significant consideration for health system leaders. The majority of participants commented on HR staffing shortages which have become exacerbated by burnout and unprecedented demands on frontline staff, and expressed concern for how the health system would continue to function. One participant commented, “It used to be we were always at 100% staffing. And now we're hovering around 90%. So, we've got fewer staff doing 30% more work” (P05).
Participant 08 went on to say that “our near-term challenge is to be able to have some type of strategy [to this HR crisis] … we need to recognize that we're not going to get out of it, not for the next several years, but we can mitigate it.” Participant 11 agreed when referring specifically to the profession of nursing in Canada. Citing recent national survey data, they commented, “66% of the nursing workforce is considering themselves having burnout and a 40% increase in the nursing population that are saying that they are having mental health deterioration, one in three talking about leaving the profession.” This comment, along with comments from the majority of participants, foreshadows downstream workforce challenges calling for health system leadership.
Ambiguity, uncertainty, and complexity have caused social system context changes for leaders. Many participants commented on how ambiguity, uncertainty, and complexity have impacted their social system roles and how this shift in system context requires different approaches to leadership. Participants described an increase in accountabilities, a reduced opportunity to be strategic, and at times, a sense of being overwhelmed. One participant commented, “I don't think that we give ourselves time to just really think strategically about what's going on frankly, whether that's your issues or development that you're dealing with or issues of the organization” (P03).
When speaking about a shift in the social system context, one participant described “The hard part for me was realizing that I was a middle and not a top because I was working with the region. There were times when a decision was made, and I had to go back to all regions and say, ‘This is what I've been asked to do. I understand it doesn't make one word of sense to most of you, however, now I need to figure it out.’ I realized I was uncomfortable because I was in the middle” (P06).
Participants described the need to be reactive (I need to address a situation urgently) and responsive (what is it that others need from me, and what is my role in addressing what is emerging before me?). Similarly, one participant commented on the shifting system challenges that “what is different […] is the vacillation and the amplitude of the vacillation […]” (P12).
Participants noticed how their colleagues responded to the demands of the pandemic differently. Some leaders prefer familiar structures and processes, whereas others thrive amid ambiguity. For instance, a participant commented that “some groups of executives were very excited about the fact there was no roadmap. Others said, ‘Where’s the playbook?’” (P06).
Post-pandemic leaders need to be compassionate and practice trauma-informed leadership. When asked to envision leadership skills in a post-pandemic world, all participants expressed concern for the human enterprise and the emotional toll the pandemic has taken on healthcare workers. For example, one senior leader commented, “I think we need to focus on building compassion into leadership” (P03).
Making a direct connection to the intention to leave, one CEO summed up the effect of an absence of compassion when they said, “I think they're going to need compassion … but they're also going to need to see that we do things differently and that we act. If it's the ‘same old, same old’ after we return to whatever the new normal is, they will be gone” (P11).
Caring concern also refers to the need for self-compassion. One participant commented, “Where does self-compassion fit into this because only in the last couple of months, it occurred to me that this is at the core of it: be compassionate with yourself” (P01).
Participants spoke of trauma in different ways. One national leader shared, “Busy ICUs or LTC centres that had 20-30 people die … that was traumatizing, let alone may be losing family members because of COVID” (P11). One participant spoke directly to staff traumatization when they said, “Leaders are going to have to be trauma-informed… and that's fresh” (P04).
Recommendations for health leaders when addressing future leadership needs
The study results are instructive and offer clear areas where health leaders could benefit from deeper insights and leadership strategies. The findings presented are consistent with student program research, program evaluations, and emerging literature. Content areas shown below were identified through faculty praxis discussions and a review of program evaluation feedback to help prepare leaders for the challenges they may face both now and in the future. 1. An orientation to possibility and renewal. Grounded in the panarchy cycle (exploitation, conservation, release, and reorganization in systems),
8
this topic could help set the stage for course content by exploring how health leaders can help avoid the “rigidity trap”
8
in the Canadian health system. 2. Emerging issues in strategic HR planning. Health leaders today and tomorrow need to know what efforts are underway to address looming staffing shortages, the issues it is likely to exacerbate, and what leaders can do about it. An important consideration is that this content focus should be instructive and, most importantly, practical and viewed through an equity, diversity, and inclusion lens. 3. Sources of support for innovation in healthcare. Leaders need to be familiar with innovations to meet emerging challenges. Similarly, as system constraints are still “light,” innovation is required to avoid the “rigidity trap” of the panarchy cycle. 4. Relational and social systems leadership in healthcare. Context is always the moderating variable in social systems. With the changes that have occurred and continue to occur, leaders could benefit from practical social system leadership strategies. 5. Polarity thinking in healthcare. Many participant narratives centred around several key, archetypal polarities such as, but not limited to, staff well-being AND patient well-being, tactical AND strategic, and task AND relationship. Polarity management, as a practical framework, offers leaders a way to address seemingly intractable issues and tensions. 6. Trauma-informed leadership. This particular focus of leadership is both timely and necessary. Post-pandemic renewal will require a different approach to leadership and diverse skill sets, particularly after such an intense, operationally focused period in our collective history. 7. Canadian healthcare networks and associations. The Canadian health network landscape could be characterized by fragmentation and over-differentiation. Health leaders need to know this system landscape to influence larger and larger audiences; integrate where necessary; and acknowledge and celebrate the diversity of associations within the sector.
Conclusion
Keeping leadership development and learning processes relevant and up-to-date through engagement with experienced health leaders is a meaningful way to adopt an evidence-informed approach to course design. Although this research focused on healthcare, the findings and recommendations presented extend beyond healthcare and could be applicable in most sectors and contexts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.