
Abstract
In British Columbia (BC) and across the territories of over 200 First Nations and 39 Métis Nation Chartered communities, the COVID-19 pandemic catalyzed a group of partner organizations to rapidly establish seven virtual care pathways under the Real-Time Virtual Support (RTVS) network. They aimed to address inequitable access and multiple barriers to healthcare faced by rural, remote, and Indigenous communities, and provide pan-provincial services. Mixed-method evaluation assessed implementation, patient and provider experience, quality improvement, cultural safety, and sustainability. Pathways supported 38,905 patient encounters and offered 29,544 hours of peer-to-peer support from April 2020 to March 2021. Mean monthly encounter growth was 178.0% (standard deviation = 252.1%). Ninety percent of patients were satisfied with the care experience; 94% of providers enjoyed delivering virtual care. Consistent growth suggests that the virtual pathways met the needs of providers and patients in rural, remote, and Indigenous communities, and supported virtual access to care in BC.
Introduction
Gaps in healthcare for rural, remote, and Indigenous patients exist across Canada.1,2 Disproportionately fewer health professionals practice in rural areas and residents of rural and Indigenous communities experience less access to services and have poorer health outcomes.3-6 In British Columbia (BC), the COVID-19 pandemic created and exacerbated challenges for the healthcare system, such as disruption and closure of local services in First Nations communities and overwhelming nursing in BC’s public health telephone service.7,8 Developing and modifying virtual services to address health system gaps is an ongoing strategy in BC and these efforts align with pan-Canadian priorities for health services and policy research. 6 Several prior on-demand, virtual initiatives have been developed, including CODI 9 and the Robson Valley Virtual Care pilot project, and the Virtual Health and Wellness Collaborative for Rural and First Nations BC were established in early 2020.10,11
Building on existing partnerships and prior work, the COVID-19 pandemic accelerated our development and implementation of multiple on-demand, pan-provincial virtual care pathways under the Real-Time Virtual Support (RTVS) network to address urgent healthcare needs. RTVS is underpinned by a group of organizations supporting the “Partnership Pentagram Plus”12,13 approach and comprised of healthcare providers (HCPs), healthcare administrators, policy-makers, community members, academia, and linked sectors. With the launch of RTVS services in April 2020, we undertook a program evaluation to determine the changes and outcomes of RTVS in its inaugural year. Our evaluation particularly focused on how RTVS improves healthcare quality and cultural safety in terms of access and equity for both patients and HCPs in rural, remote, and Indigenous BC communities.
Methods
Design and setting
We conducted a mixed-method program evaluation of the RTVS pathways from April 1, 2020 through March 31, 2021 (the first year of programmatic implementation in conjunction with the start of the pandemic). A mixed-method approach accounts for complexities, different ways of knowing and understanding phenomena, and for sharing and learning from findings. 14 The RTVS initiative was developed through the collaboration of partnering organizations in BC, including the BC Ministry of Health, the Rural Coordination Centre of BC (RCCbc), the First Nations Health Authority (FNHA), the BC Emergency Medicine Network, and the Digital Emergency Medicine Unit in the University of British Columbia’s Department of Emergency Medicine. Our evaluation comprised a multi-stakeholder advisory committee, collaborative partners, and working groups.
Interventions: Development of RTVS pathways
Description of the seven RTVS pathways launched and evaluated during Y1.
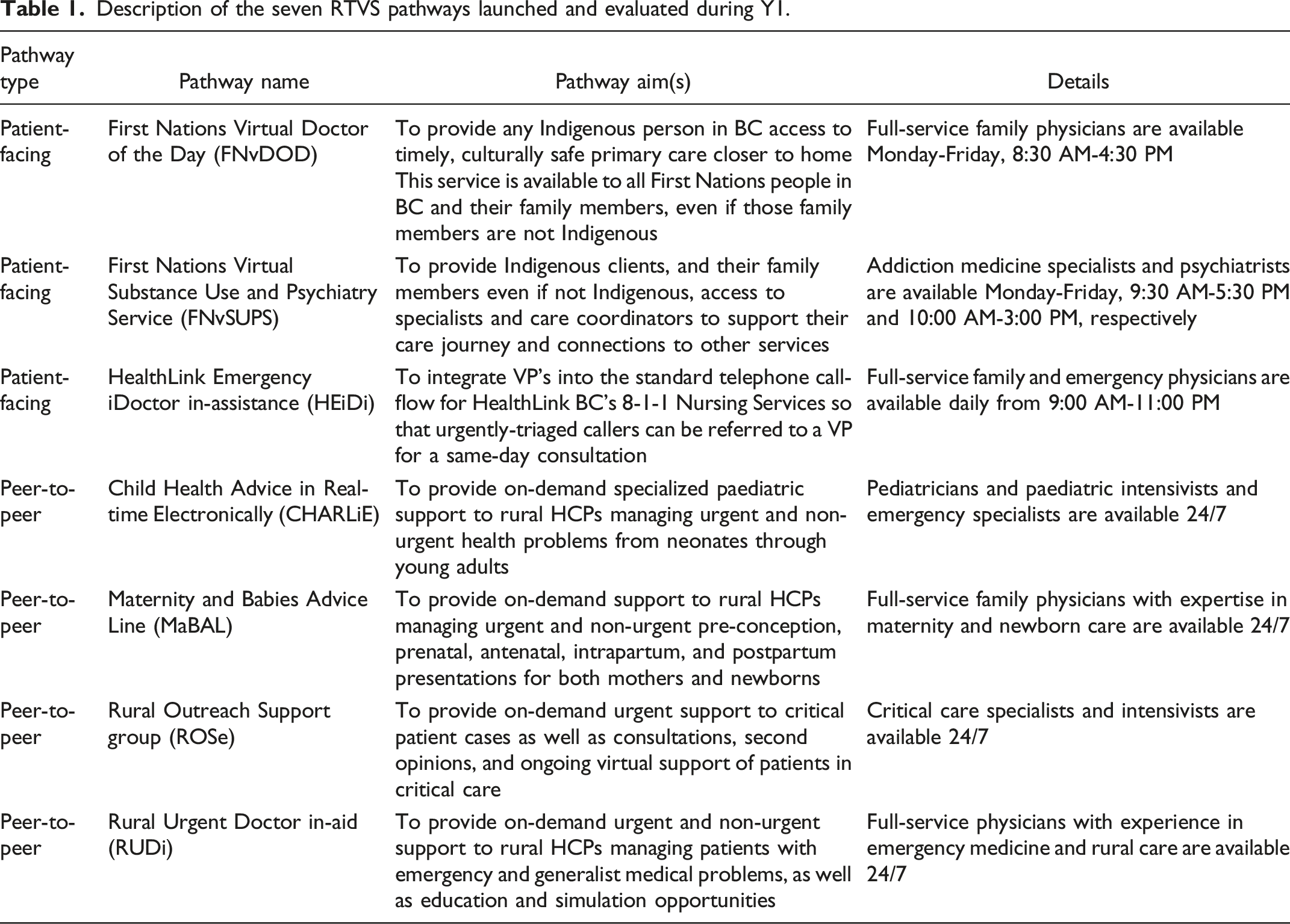
Approximately 75 practicing physicians were initially recruited to serve as Virtual Physicians (VPs) on one or more of the RTVS pathways, growing to 150 VPs by the end of Y1. VPs were engaged based on clinical expertise, being non-judgemental, compassionate, and strong communicators, experienced with different technologies, knowledgeable about rural BC, and experienced in different care settings. Further, they were selected for an expressed commitment to their personal cultural safety and humility journey. RTVS pathways include a number of VPs of Indigenous ancestry, and the ethos of the VP communities of practice emphasizes the importance of knowledge exchange, role modelling and coaching that have support a model of team-based and holistic care. RTVS pathways are intended to augment and integrate with existing health services to support patient-centred team-based care within the publicly funded BC health system.
Evaluation approach
We utilized a participatory, developmental, and iterative approach15,16 to create and refine our evaluation approach and objectives, understanding and respecting that this work is taking place across and within the unceded territories of over 200 First Nations and 39 Métis Nation Chartered communities province-wide. Starting with two core, guiding principles—(1) RTVS seeks to improve access to and equity of care for rural, remote, and Indigenous patients; and (2) RTVS seeks to enable rural HCPs to access on-demand support from non-judgemental, culturally safe, knowledgeable physician colleagues—we developed an RTVS-specific, comprehensive evaluation framework (available on pages 51-53 of the RTVS Year One Evaluation report) 17 grounded in other relevant, validated frameworks, including the Quadruple Aim, 18 Social Accountability,19,20 and the BC Health Quality Matrix. 21 The RTVS evaluation framework was further contextualized through consultation with stakeholders and four guiding images were developed to highlight RTVS functions: a safety net (timely, equitable access to care, irrespective of where patients are located in BC), funnel (help patients navigate the health system and connect them to appropriate longitudinal primary care), fire department (diverse community engagement activities provided by RTVS physicians), and feather (high-quality culturally safe care for Indigenous patients).
Study populations
Given the objectives of the RTVS evaluation, several different participant groups were included. All RTVS VPs were invited to participate in interviews and surveys. Patients utilizing the patient-facing pathways were invited to complete post-encounter surveys. Snowball recruiting methods were utilized to identify HCP users of the peer-to-peer pathways and invite them to participate in interviews.
Data collection and measures
A mixed-method approach was used, including routinely collected operational and administrative data from each pathway to determine utilization rates over time as well as the locations of users. Semi-structured interviews were conducted with RTVS VPs, rural HCPs, and stakeholders to extensively investigate perspectives, experiences, and impacts of RTVS. On-line anonymous surveys (available upon request) were administered to RTVS VPs and patients to determine overall experience and satisfaction outcomes.
Data analysis
For the qualitative interview data, we used a modified constant comparative method 22 to develop themes and determine saturation from a longitudinal and iterative perspective. We calculated descriptive statistics for quantitative operational and survey data. Location data were cross-referenced with BC health regions and visually mapped to determine geographic distributions of RTVS users. Results were iteratively shared with RTVS stakeholders to co-develop next steps and recommendations. Additionally, we have published early, descriptive findings from the HEiDi pathway and refer readers there for more in-depth results. 7
Results
Encounter and call volumes
Summary of quarterly encounter volumes and change recorded by each pathway.
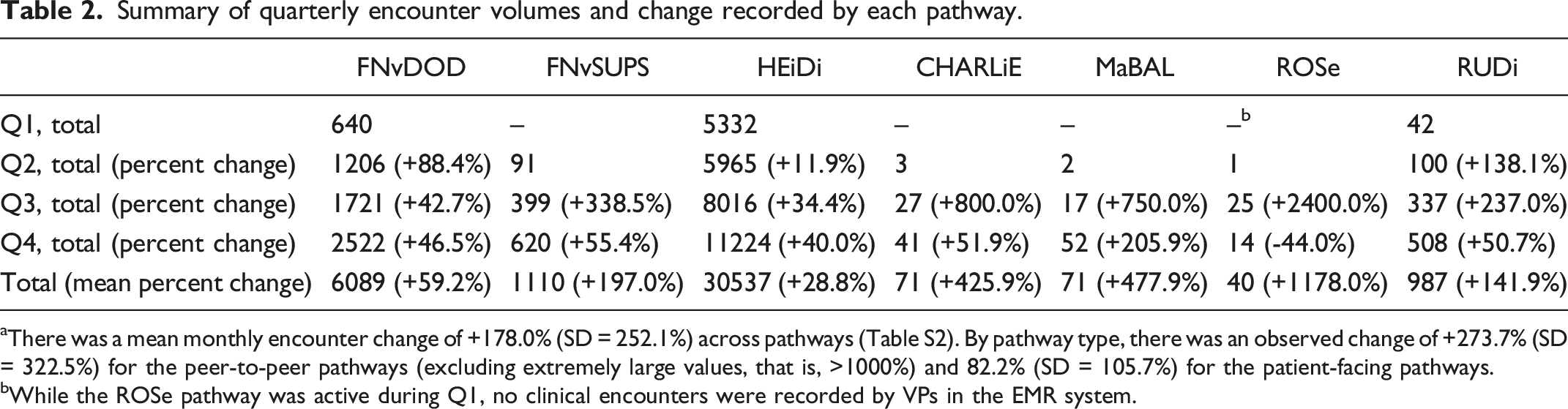
aThere was a mean monthly encounter change of +178.0% (SD = 252.1%) across pathways (Table S2). By pathway type, there was an observed change of +273.7% (SD = 322.5%) for the peer-to-peer pathways (excluding extremely large values, that is, >1000%) and 82.2% (SD = 105.7%) for the patient-facing pathways.
bWhile the ROSe pathway was active during Q1, no clinical encounters were recorded by VPs in the EMR system.
The peer-to-peer pathways offered a combined total of 29,544 hours of continuous, on-demand support to rural HCPs during Y1. 17 They recorded 2,486 calls, either by telephone or Zoom, from rural HCPs, including nurses at remote nursing stations, family physicians, and other rural providers. More complicated consultations involved 30-60-minute calls so that the VP can provide guidance on an uncommon procedure, take the patient’s history, review an electrocardiogram chart or ultrasound, or develop a full care plan with the calling provider that accounts for the limited resources of the setting. Almost all VPs noted a number of urgent, complex cases that required over an hour of time. For instance, VPs described resuscitation cases at rural or remote health centres, where they supported the on-site nurse performing unfamiliar procedures. VPs indicated about 6% of calls received are solely education-based, where they offer simulations or provide guidance to rural healthcare providers on different procedures and other clinical competencies.
Communities accessing RTVS
A total of 87 distinct rural, remote, and Indigenous communities accessed at least one of the peer-to-peer pathways, with approximately half being located in the Northern Health Authority. We observed that the communities most frequently accessing the peer-to-peer pathways typically were FNHA nursing stations and patient cases where RUDi acted as most responsible provider. Fifty-five percent (55%) of clients of the FNvDoD pathway were from Northern or Vancouver Island Health Authorities, while 40% of FNvSUPS clients were from Northern Health Authority. Frequent usage by clients from these regions suggests that these services are addressing previously identified healthcare inequities.
Patient-reported experience of virtual care
A total of 1,762 HEiDi callers completed an on-line survey following their encounter, representing an estimated response rate of 6.5% (denominator = 26,907 encounters since launch of survey) but with a low rate of missing data across questions (range = 7.0%-8.5%); 123 and 16 clients from the FNvDOD and FNvSUPS pathways, respectively, completed a post-encounter survey.
Clients of the FNvDOD and FNvSUPS and callers to HEiDi generally indicated a positive virtual care experience across a range of domains; 98.2% of FNvDOD and 87.5% of FNvSUPS clients were “satisfied” or “very satisfied” with their experience. One FNvDOD client described her experience using the service: “I attended a call with my daughter yesterday and [the doctor] called us back right away. I have not felt that respected, supported and understood from anyone in the medical industry in a very long time. She made our difficult situation so much easier to deal with…We both cried from relief after we got off the phone because we were provided an easy to follow holistic plan and felt like we were heard. Thank you for this critical service for people who are not always treated kindly in this industry. It meant the world in our time of need.” – FNvDoD Client
For HEiDi, 79.4% of callers indicated feeling “better” or “much better” after their encounter and 97.6% responded that they planned to take the action recommended by the HEiDi VP. One client described their experience calling the service when they were unable to see their family doctor: “I … needed to better understand how to handle my concussion. Speaking with the HEiDi VP was a discussion rather than a one-sided delivery of information. He helped me figure out a plan.” – HEiDi Caller
Provider-reported experience of virtual care and support
Fifty-two out of 150 VPs completed the Y1 survey, corresponding to an estimated response rate of 34.7%. Over 90% of VPs were satisfied working on their RTVS pathway. According to respondents, the most important qualities needed in a virtual HCP are: “understanding of low resource practice settings,” “clinical expertise,” and “kindness and empathy.”
Summary of provider interview themes.
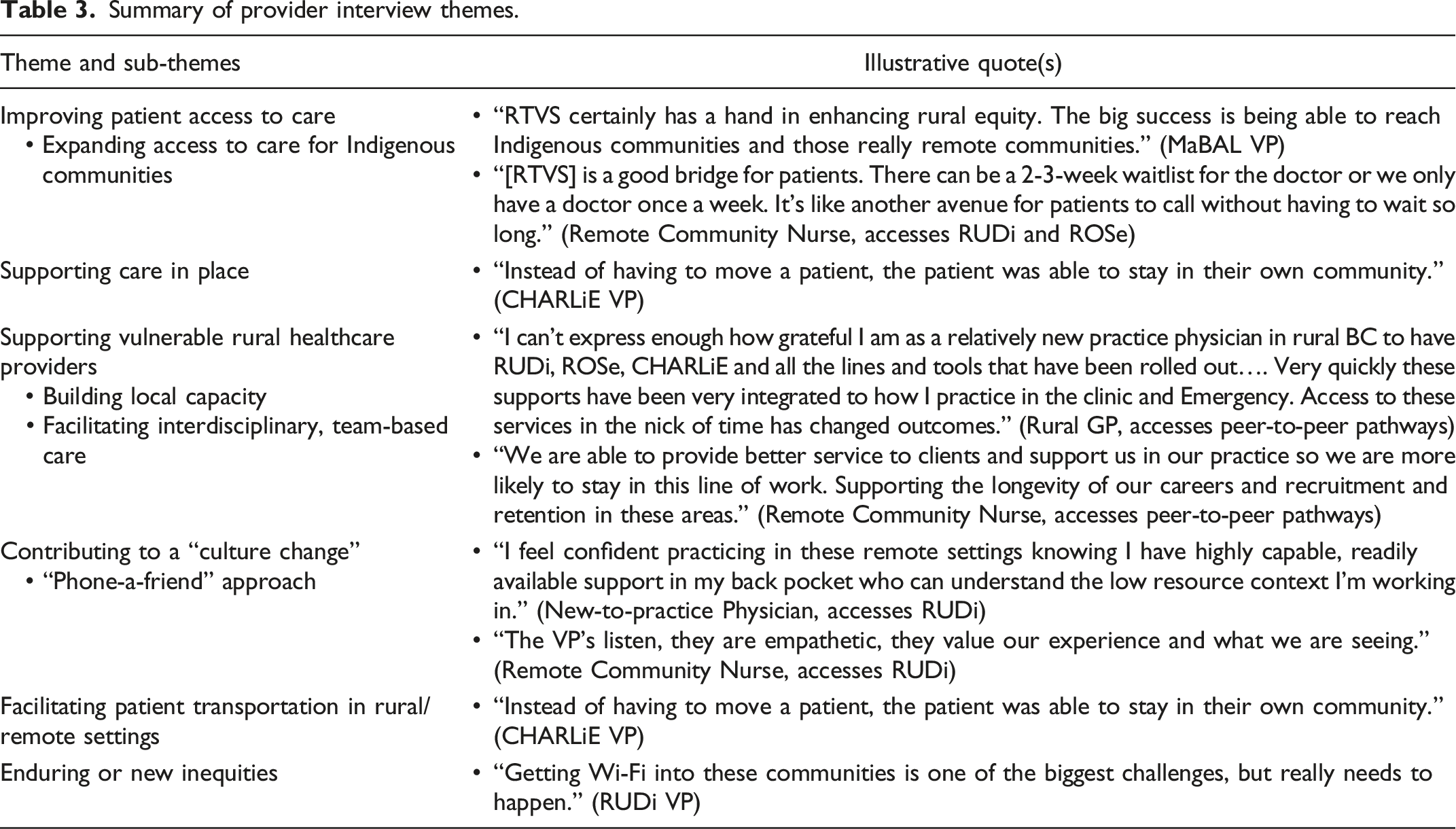
Rural providers also emphasized that RTVS has greatly lowered barriers to accessing collegial support, thus decreasing professional isolation, and strengthening interprofessional relationships, and potentially contributing to recruitment and retention. As one remote community nurse stated, this contributes to retention: “We are able to provide better service to clients and support us in our practice so we are more likely to stay in this line of work. Supporting the longevity of our careers and recruitment and retention in these areas.” – Community Nurse
Interpretation
Our mixed-method Y1 program evaluation of the seven RTVS pathways yielded strong, preliminary evidence of how these virtual interventions are supporting rural, remote, and Indigenous communities in BC. All pathways demonstrated considerable uptake in Y1, with nearly 40,000 patient encounters and 2,500 rural HCP calls recorded in total, suggesting that RTVS increases patient access to timely, appropriate virtual, closer to home care, as well as access to collegial support for the HCPs serving rural communities, who are vulnerable due to contextual factors such as scarce health human resources, and geographic isolation. Findings showed positive experiences for patients and providers related to access to timely care and facilitation of patient transport, which is aligned with the reported potential effectiveness of virtual interventions. 24 Patients and providers self-reported high rates of satisfaction in their experiences with the pathways, similar to other virtual services during the pandemic.25-27
Explanation of findings
RTVS comprises a flexible, responsive suite of virtual services with new pathways launched to address the needs and health inequities that exist/remain prevalent across rural, remote, and Indigenous communities. The observed uptake and growth of RTVS pathways were associated with increased equitable access to care for patients across BC, consistent with factors elaborated in the literature. 28 Particularly, findings across RTVS pathways are emblematic of this initiative’s safety net function. By providing rapid access to VPs for a variety of primary and urgent health concerns, many and diverse patient encounters were performed by patient-facing pathways during Y1. Importantly, we observed the highest volume of encounters for the FNvDOD and FNvSUPS pathways in the Northern, Interior, and Vancouver Island Health Authorities—less-populated regions that have lower access to healthcare services. 29 Similarly for the peer-to-peer pathways, we found that nurses serving in some of the most remote, under-resourced healthcare centres in BC were frequently accessing the pathways for support.3,30
VP interview findings highlighted several ways that RTVS pathways funnel patients and connect them to primary, longitudinal services in the wider health system. In our prior work, we described how HEiDi can divert the majority of patients to less-urgent care while accelerating a minority to more-urgent in-person care. 7 Evaluation participants emphasized the importance of patient transport coordination in rural and remote settings and how RTVS can improve coordination between nurses and BC Emergency Health Services. Thus, RTVS stakeholders and VPs recognize the potential of greater integration with existing, complementary health services to promote patient-centred care in rural BC, which in turn can contribute to longer-term sustainability for RTVS. Further, in an effort to align with the United Nations Declaration on the Rights of Indigenous Peoples 31 and the findings from the In Plain Sight report 32 , as well as the recommendations from the Truth and Reconciliation Committee, 5 the FNvDOD and FNvSUPS services employ team-based care approaches that include connecting Indigenous clients to traditional wellness practitioners, supporting patients in their relationship-based care journey. Underpinning these outcomes and concepts is the feather, guiding the practice of humility and culturally safe care to address historical and current inequities and racism faced by Indigenous patients.5,19
Beyond direct clinical care and support, RTVS pathways function as a de facto “fire department, 2 ” engaging providers and communities in diverse ways when not answering clinical service calls. This included strengthening community capacity through providing educational opportunities and training to community health providers. Evaluation findings suggest that RTVS can enhance rural HCP confidence, decrease isolation by building virtual communities of practice, and improve clinical skills and knowledge through education and simulation sessions. However, existing infrastructural inequities across the province remain a barrier to providing equitable care, as also seen in Quebec, 33 particularly technological limitations for both providers and patients. A multi-modal approach that uses the most reliable communication method for the area requesting assistance would help address these inequities in infrastructure in the short-term. Continued advocacy is needed to ensure that reliable, equitable solutions are implemented for the long-term given the disparities of a standard of connectivity availability, infrastructure, and funding across rural and remote areas.
Limitations
We note several limitations in our evaluation, particularly related to implementation of the mixed-methodology and generalizability of findings. While we were able to combine and analyze data across different sources, it is possible additional data were missed or mischaracterized. Our evaluation work beyond Y1 will utilize more robust reporting and tracking methods. Qualitative data focused primarily on VPs and patients were not interviewed directly, nor is their post-encounter health system utilization known. Our subsequent phase of evaluation will include linkages to provincial administrative databases in order to determine if callers adhere to VP’s advice to attend the emergency department or visit their family physician and allow for incorporation of patient outcomes in evaluation. Subsequent evaluation will also incorporate economic metrics to provide a comprehensive understanding of the costs associated with RTVS use and allow examination of cost drivers. Generalizability of findings to rural, remote, and Indigenous communities outside of BC is unknown. However, further in-depth evaluation of specific RTVS interventions, for example, RUDi’s overnight coverage of a rural hospital emergency department, will likely yield findings that can inform applications across Canada.
Conclusion
Implementation of RTVS pathways has demonstrated successful and rapid growth in improving equity of access and access to care across BC. High satisfaction has been expressed by both patients and providers in rural, remote, and Indigenous communities. Future growth areas for RTVS pathways include not just appropriate health services and clinical care, but equity of access to health information, promotion, and general wellness advice for patients, as well as equity of access to non-judgemental, collegial support for providers. It follows that the central evaluation questions to be addressed in Year 2 are as follows: (1) How has RTVS impacted equity of access to care and support; and (2) How is RTVS participating in and advancing the emergence of hybridized healthcare delivery and what impacts are observable for providers and patients in cases of hybridized care? Following the first year of implementation, RTVS has collaboratively worked on the establishment of a robust, multi-dimensional evaluation framework with ongoing dialogue informed by data for continuous calibration through a Learning Health System.34,35 At the time of this article, these services have continued to be funded provisionally. Such partnership, evaluation, and collaboration are essential to working together to ensure ongoing sustainment of these programs.
Footnotes
Acknowledgements
The authors would like to express their sincere thanks to Ted Patterson, Shana Ooms, and Lindsay Arscott from the BC Ministry of Health, for their support, extensive availability, and collaboration. We would like to thank the Year One RTVS Evaluation Advisory Committee and all the participants who shared their insights and time to take part in the evaluation, and the membership of the RTVS Working Group. Special thanks to Sandra Sundhu, HealthLink BC, BC Ministry of Health, Dr. Don Burke, Dr. David Wensley, Dr. Jeanette Boyd, and Dr. Alan Ruddiman for their insight and guidance on evaluation in the context of the RTVS partnership. We also wish to thank Elizabeth Stacy, Elsie Wang, and Erin Crisfield for their contributions on the evaluation team during the timeframe of the report, and Dave Harris and Tom Skinner for their virtual care, implementation, and technology expertise. We gratefully acknowledge the BC Ministry of Health and the Joint Standing Committee on Rural Issues for being the primary funders of the RTVS Evaluation. We also gratefully acknowledge additional financial and in-kind support from the Rural Coordination Centre of BC, Michael Smith Health Research (formerly BC Academic Health Sciences Network), Emergency Care BC (formerly BC Emergency Medicine Network), and UBC Department of Emergency Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BC Ministry of Health and the Joint Standing Committee on Rural Issues for being the primary funders of the RTVS Evaluation. We also gratefully acknowledge additional financial and in-kind support from the Rural Coordination Centre of BC, Michael Smith Health Research (formerly BC Academic Health Sciences Network), Emergency Care BC (formerly BC Emergency Medicine Network), and UBC Department of Emergency Medicine.
Ethical approval
As this program evaluation work was for quality assurance and improvement purposes, an ethics waiver was provided by the University of British Columbia's research ethics board, in keeping with the Tri-Council Policy Statement. 23
Data sharing
The data are not publicly available.