
Abstract
In an era of significant human and fiscal constraints, hospitals increasingly rely on industry representatives to fill gaps related to practice-based education. Given their dual sales and support functions, the extent to which education and support functions are, or ought to be, fulfilled by industry representatives is unclear. We conducted an interpretive qualitative study at a large, academic medical centre in Ontario, Canada, during 2021-2022, interviewing 36 participants across the organization with direct and varied experiences with industry-delivered education. We found that ongoing fiscal and human resource challenges prompted hospital leaders to outsource practice-based education to industry representatives, which created an expanded role for industry beyond initial product rollouts. Outsourcing, however, generated downstream costs to the organization and undermined the goals of practice-based education. To attract and retain clinicians, participants advocated for re-investment in practice-based education in-house, with a limited and supervised role for industry representatives.
Introduction
In an era of significant human and fiscal constraint, hospitals increasingly rely on representatives of pharmaceutical, medical device, and other health products industries to fill gaps related to practice-based education. Practice-based education is the ongoing process of cultivating expert clinical knowledge with the aim of advancing safe, high-quality patient care. 1 Ideally, clinicians across career stages view teaching and learning as ongoing aspects of their role, and various actors within an institution, including educators, preceptors, managers, and leaders, can enable onboarding, capacity building, and professional development. The introduction of new and updated medical products, equipment, and devices into a hospital requires practice-based education to ensure that clinicians can safely and appropriately integrate new products into practice. The product expertise of industry representatives is generally considered essential to this process. 2
Industry representatives inherently occupy a dual sales and support function and their presence within hospitals is associated with an increased adoption of newer, high-cost devices. 3 Since industry representatives performing educational and support tasks are filling roles historically occupied by hospital staff, 4 industry’s involvement in practice-based education constitutes a form of outsourcing, one that is considered to be of material benefit to hospitals. Public procurement policy thus requires that industry provided education and support be considered a “value add” and not a primary weighted criterion factored into procurement decisions. 5
In Canada, the extent to which education and support functions are, or ought to be, fulfilled by industry representatives is unclear. Outsourcing expert education to commercial entities may have deleterious effects, including conflicted assessment of the value of different innovations, 2 adoption or use of low value technologies, even patient harm.6,7 Yet, hospitals face significant challenges fulfilling even the minimum demands of practice-based education including onboarding and orienting new staff; managing back-ordered products; retaining expert clinicians; and recruiting preceptors, educators, and clinical resource specialists. We sought to understand the nature of industry’s expanded role in practice-based education and its implications for Canadian hospitals in the context of the current human and financial pressures.
Theoretical framework
Practice-based education, as conceptualized in this project, aims to cultivate expert and ethical decision-making in the context of a clinical environment characterized by complexity, acuity, specialization, and a rapid proliferation of technologies. 8 Clinicians across all career stages are supported in a process of developing clinical expertise and leadership skills by educators, preceptors, managers, professional practice leads, and clinical directors. The model of practice-based education posits that clinical skill acquisition and development proceeds through levels of proficiency, ranging from novice through expert.1,8 “Competent” clinicians situate their actions within the context of care goals and plans as they assess the salient aspects of a clinical situation, and act consciously, deliberately, and efficiently. 1 “Proficient” and “expert” clinicians appraise situations holistically and grasp those aspects which are most salient in order to intervene in a way that appears intuitive. 1
Expertise is cultivated and validated within interprofessional communities of practice, which increasingly include industry representatives. 9 However, reliance on industry representatives for the provision of practice-based education constitutes a partial privatization of professional expertise as, in many cases, the manufacturer becomes the only source of product-related information or training resources.6,9,10 Reliance on industry for practice-based education risks establishing marketing feedback loops where industry is perceived as the authoritative expert and clinicians are persuaded to adopt products into practice regardless of clinical need, efficacy, or cost-effectiveness. 11
The outsourcing of practice-based educational activities to industry has occurred alongside the shift to competency-based education in nursing. Consistent with the implementation of neoliberal market principles and managerial techniques within Canadian hospitals as part of “new public management,” competency-based education is characterized as measurable, technical, and amenable to interventions promoting efficiency, standardization, and auditability. 12 Most in-service educational sessions, a dominant format for practice-based education, aim to foster a competent level of achievement, but rarely the development of holistic, relational, expert clinical practice. 1 In contrast, the novice to expert model posits that expert practice is achieved through refining theoretical knowledge through encountering the diversity and complexity of practice and is fostered through recognition, reward, and retention of clinical experts. 1
Methods
Setting and participants
This project was an interpretive qualitative study 13 conducted at a large, academic medical centre in Ontario, Canada, between September 2021 and August 2022.
Recruited using purposive and snowball sampling methods, 36 participants with direct and varied experiences interacting with industry representatives in the context of practice-based education agreed to participate in the study. Figure 1 illustrates participants’ characteristics in terms of clinical specialty or department, then separately (to preserve confidentiality), their role within the organization. Participants included not only point-of-care clinicians, predominantly nurses, advanced practice clinicians, managers, and senior leaders, but also respiratory therapists, physicians, pharmacists, and an industry representative. Participant roles, clinical areas, and hospital departments: the outer circle shows the number of participants by hospital role; the inner circle shows participants’ clinical specialty or hospital department.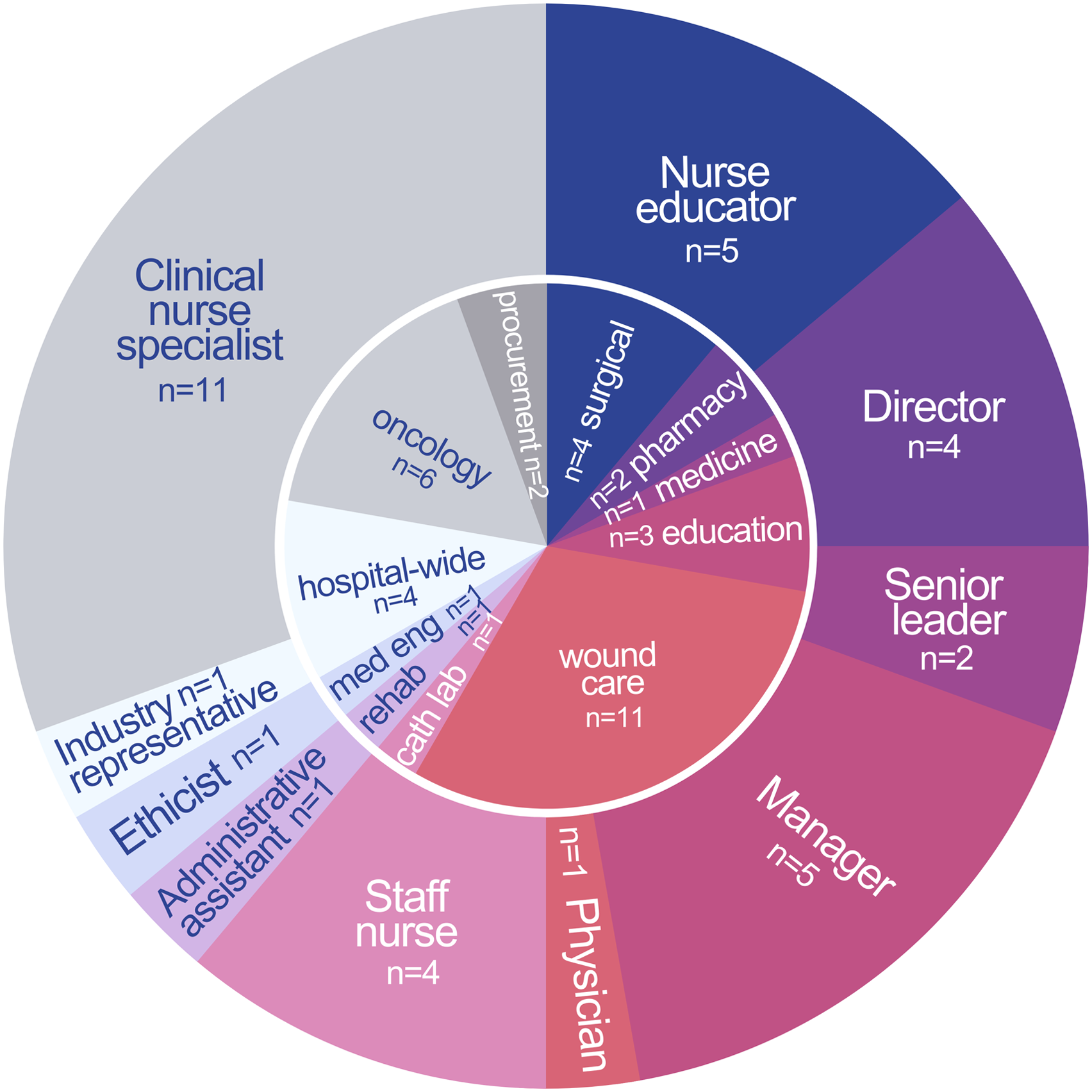
Data collection and analysis
This study triangulated three data collection methods: interviews, focus groups, and document analysis. Due to the COVID-19 pandemic, all data were collected virtually. The lead author conducted 21 semi-structured interviews (lasting a mean = 46 minutes; range 24-60 minutes), and two, 1-hour focus groups (n = 11; n = 4) (see on-line Appendix 1 - Interview Guides). Two participants agreed to follow up interviews. Marketing materials and policies referenced by participants during interviews were collected for analysis.
All transcripts, field notes, and documents were imported into NVivo12 (QSR International). Using an interpretive approach, 13 we conducted preliminary coding and sorted the text into categories (e.g. education “in-house,” education by industry, and policy context). The research team met regularly to review the data, emerging codes, and analytic memos. We identified emerging themes and illustrative quotations, synthesized data across participants in interpretive memos, and then generated visualizations of the data to explore and report on key themes.
Results
Three overarching themes emerged across participants’ experiences. First, fiscal and human resource constraints have prompted an outsourcing of practice-based education to industry, thereby creating an expanded role for industry representatives. Second, outsourcing practice-based education to industry has resulted in downstream costs to the organization and undermined the goals of practice-based education. Third, participants advocated for re-investment in practice-based education and recommended a more circumscribed and supervised role for industry representatives.
An expanded role for industry: Outsourced education
Participants characterized education as a core value of the organization and recognized that effective practice-based education was time and resource-intensive. In an ongoing climate of resource constraints, hospital leaders turned to industry to leverage and scale resources external to the hospital. This logic of outsourcing promoted an expanded purview for industry representatives in providing practice-based education to clinicians.
Participants responsible for practice-based education (such as managers, clinical nurse specialists, and advanced practice nurse educators) and point-of-care staff described an erosion of organizational resources dedicated to educational activities. Budgetary and staffing realities typically confined paid education for point-of-care clinicians to one day per annum. Clinical nurse specialists, for example, described a steady expansion of their role and workload in terms of patient acuity and non-clinical responsibilities such as policy development, explaining, “We weren’t able to fit everything that we needed to do into our day… so then we started transitioning more to the vendors being the ones that do the education.” Participants across roles and departments characterized current practice-based education as frequently organized “off the side of a desk” and occurring in clinical areas in the few moments available between patient care activities.
In the context of these pressures, participants described industry representatives as pragmatic extensions of advanced practice clinicians and educators. Having industry representatives conduct in-services for new products, for example, provided an opportunity to create “efficiencies” or “economies of scale.” One director explained, “As hospitals’ budgets get tighter, we rely a lot more today on the industry than we would before … The efficiency of having the expert come in and train your staff is really good.” Participants found industry representatives to be “helpful” and “flexible” as they were willing to deliver “rolling education” on the units and across multiple shifts and would provide user-friendly resources in multiple formats that clinicians could rely upon when unit educators were unavailable.
Constraints on the ability of staff to deliver and engage in practice-based education meant that managers and educators sought industry involvement in a range of educational activities that went far beyond the initial contact that was specified in typical procurement contracts. Participants described industry involvement in practice-based education including: Initial product in-services to introduce new products or equipment to cover “what’s different than what we had before, how is it different, how is this to be used, and what are the ‘watch outs’ and risk associated with it” (Director); “Refresher” education regarding infrequently used or specialty products, or to cope with high rates of staff turnover; “Remedial” education to address issues caused by improper use (e.g. frequent breakage) or troubleshooting; “Emergency” education prompted by pandemic conditions, preparation for accreditation processes, and in response to backorders; and Periodic involvement in fundamental and continuing education (e.g. the physiology of a disease or management of surgical site infections).
Finally, participants involved industry in educational activities simply to leverage additional resources, such as sponsored lunches, to encourage clinicians to attend unpaid education.
Industry representatives were also seen to push for an expanded role in practice-based educational activities. Leaders noted that educational offerings were a point of competition for companies since the success and future applications of the product within the hospital largely depended on point-of-care clinicians’ familiarity and confidence in using the product. Thus, industry representatives frequently offered to provide education to point-of-care staff with the goal of developing ongoing relationships with clinicians as a vehicle for product-related support. For example, participants described being “hounded for education” in the years between procurement contracts, including for educational opportunities that did not align with clinical or educational priorities. Despite this, industry found that clinicians were largely receptive given the value placed on continuing education by the organization and clinicians. Consequently, an industry representative participant noted that activities with an education focus greatly facilitated access to the hospital: “I always found that I could get in though, fairly easily, especially if it was education-based.”
The COVID-19 pandemic exacerbated organizational pressures owing to staff shortages, employee redeployments, rapidly changing clinical and policy contexts, supply shortages and backorders, and increased patient volume and acuity. In this context, there was a sense that education could only occur infrequently without industry resources.
Outsourcing has downstream costs
While ostensibly a pragmatic solution to organizational challenges, participants described the expansion of industry’s educational roles and responsibilities as generating downstream costs to the organization. They noted that industry education was (1) not sufficiently effective or relevant to clinical practice and (2) could serve to undermine, rather than cultivate, clinical expertise. Consequently, while most participants perceived no alternative to relying upon industry in delivering practice-based education, they also characterized the outsourcing of practice-based education as fostering a “lack of control over the education” (Senior Leader).
While viewed as helpful, and at times necessary, to conducting requisite education, participants questioned the effectiveness of industry-delivered education. Conducted within the coordinated chaos of the practice environment, clinicians, although physically present, were generally “busy with their own lunch in the microwave and their colleagues … asking them questions.” Thus, in-services were described as “full of interruptions” (Manager). One point-of-care nurse described caring for a full patient load whilst receiving education for a recent product rollout. He characterized his learning outcome as: “Basically, I’m just going to disconnect it and reconnect it and hope for the best.” Similarly, while participants appreciated the user-friendly nature of industry reference materials, they also reported deficiencies in the materials including misleading claims, the misuse of research evidence, and discrepancies with hospital policy or local clinical environments.
Paradoxically, involving industry to further educational goals sometimes undermined the clinical expertise these activities sought to develop. Owing to a reliance on industry representatives to design and deliver practice-based education, participants noticed an emphasis on product solutions for practice problems, noting that products and equipment require expert users and that industry representatives were not substitutes for best practice. For example, one nurse manager described interacting with an industry representative who kept asserting that their product, a dressing used as a prophylaxis to skin breakdown, had universal application. However, the nurse manager explained, “You don’t need to have a dressing on every butt,” because nursing care including skin assessment, appropriate turning, and positioning is more effective, and evidence-based. Despite pressure from the industry representative to administer the product to all patients, clinical leaders pushed back, identifying an absence of benefit and signs of patient harm; the nurse manager noted that when the product was in place nurses were less likely to perform a thorough skin assessment.
Recognizing that industry representatives are “really good at doing the education as long as you have an educator…sorry, a vendor … who also doesn’t try to sell to the nurses” (Clinical Nurse Specialist), educators described a need to provide oversight and enforce boundaries around industry’s role in practice-based education to mitigate patient harm or budgetary impact. As an educator explained, “Somebody has to work with the vendors to understand how their product integrates with everything else... they can’t just have the free access to say whatever.” However, participants noted that the reason for outsourcing the education in the first instance was because staff rarely had the capacity to provide such oversight.
Course correction: Moving toward an ideal
Despite ongoing challenges, participants articulated an ideal for practice-based education based on what had worked in the past and what they thought would help in the future. Many recommended a limited and supervised role for industry representatives and advocated for greater investment in practice-based education in-house as a key clinician recruitment and retention strategy.
The kind of education that participants valued as ideal (see Figure 2) would not necessarily occur in a classroom or through formal offerings, but rather as part of a larger culture of developing, sharing, and cultivating expert clinical knowledge within and between professions and across career stages. A group of nurses, for example, described previous experiences of a “high performance” unit culture that valued learning, continuing education, and mutual aid: “It was an expectation that you knew your stuff inside and out. . . And it was an awesome way to practice . . . I know that I taught senior nurses things, and I know that junior nurses have taught me things, and there’s always that influx of information” (Staff Nurse). A visualization contrasting the ideal and current states of practice-based education.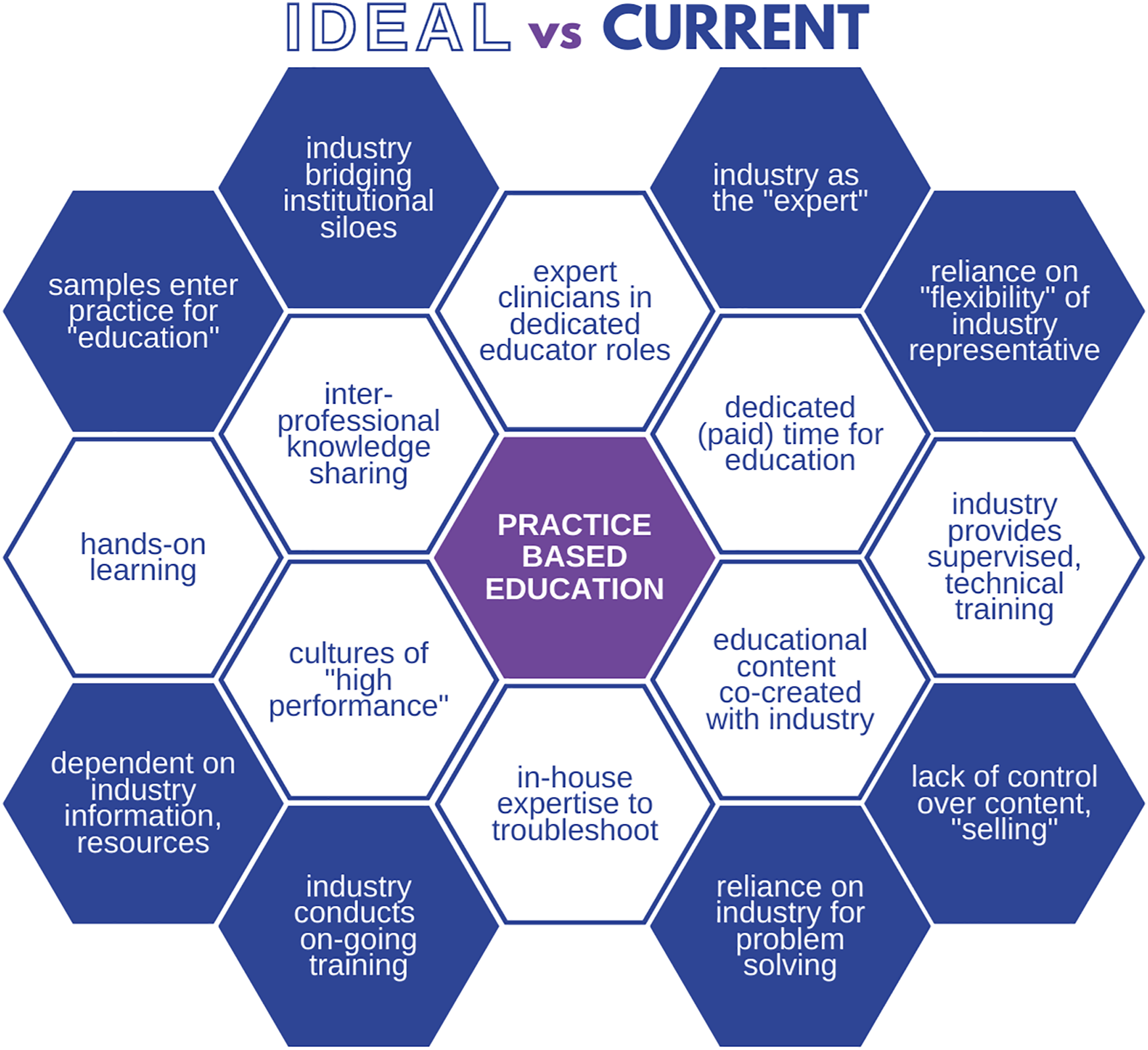
Participants emphasized that industry representatives had a role in providing in-depth product information and were most effectively employed to supplement education that was staff-led, aligned with clinical learning needs, occurring just-in-time, and addressing important contextual factors.
Participants who directly received, planned, or delivered education stressed that cost-effective, safe, high-quality patient care requires practice-based education to be an upstream consideration in all hospital processes, beginning with the identification of practice needs through to how products and equipment are integrated and maintained long term. However, nurse educators frequently experienced being involved in product changes only as a final step when leadership or the physician requesting a product would involve them in scheduling the education: “They say, ‘This is coming down and the vendors are going to provide in-services, so you plan it and let the staff know.’ It has happened quite a bit” (Nurse Educator). Educators thus advocated for the strategic involvement of those with insight into educational needs and implementation realities into decision-making processes that currently seem like “black boxes.”
Though the ongoing health human resource crisis has undermined the ability of the organization to implement best practices for practice-based education, leaders struggled with how best to prioritize these efforts given the importance of patient care and nursing retention: “If we do not make sure that nurses have the knowledge and skill and feel competent and safe, then they’ll quit, and so we’re no further ahead, or they cause preventable harm to either themselves or the patient” (Director). Participants, thus, characterized investment in practice-based education as a core retention strategy for point-of-care staff.
Discussion
Sufficient access to continued professional development support and resources within a team environment is recognized as critical for improving the work life of clinicians, a key pillar within healthcare’s Quadruple Aim.14,15 The available evidence suggests that access to continuing education, mentorship, and dedicated time for professional development comprise priority, targeted retention and support interventions to stabilize the healthcare, and particularly nursing, workforce. 16
Consistent with literature on healthcare’s Quadruple Aim,14,15 participants described an ideal working culture as one that prioritized knowledge sharing, learning, and expertise, and they underlined the enormous value, and current erosion, of the clinical expertise to which they aspired. Investment in practice-based education, including dedicated education roles, paid time for practice-based education, internally developed resources, and cultivation of intra- and interprofessional learning will offer a strong return on investment. By attracting and retaining clinicians within cultures of high performance, investment in practice-based education will, in turn, strengthen patient outcomes.
As health systems emerge from the COVID-19 pandemic and grapple with prioritization, 17 these findings can inform analyses of opportunity costs when vital educational activities increasingly are shifted to industry representatives. Participants in this study recognized that industry representatives possessed unique and important knowledge about the functioning and maintenance of their products, devices, and equipment. However, participants simultaneously questioned the value and appropriateness of industry-provided education, reflecting concerns within the literature that reliance on industry may undermine the overall development of expert clinical practices and result in patient harm.2,6,10,18 Thus, these findings support theories of practice-based education that suggest implementing career ladders and novice to expert education pathways, and the development and investment in advanced clinical practice and educational roles. 1
Strengths and limitations
This study took place in 2021-2022 during the COVID-19 pandemic, which at times limited our ability to recruit point-of-care clinicians and managers; recruitment occurred intermittently to minimize health system burden during waves of infection. All data were collected virtually, which facilitated participation, but precluded direct observation of educational activities involving industry. To ensure the study accounted for a full range of experiences, we extended the recruitment period to include additional perspectives across health professions, clinical areas, and organizational hierarchy. However, as this was a purposive sample, these perspectives are not representative and further interviews in other clinical areas, with other healthcare professionals, or within other administrative units (e.g. human resources) may yield additional insights. These findings reflect the experiences of participants at a large academic medical centre in Ontario, Canada, in the context of the COVID-19 pandemic; thus, there may be important differences across Canadian hospitals that shape experiences with industry’s role in practice-based education. Nonetheless, in the triangulation of multiple forms of data and in-depth examination of an understudied phenomenon, these findings raise relevant questions for hospital leadership across settings.
Conclusion
Efforts to address ongoing fiscal and human resource realities within the hospital sector in Canada have created an expanded role for industry representatives within practice-based education. While educators, managers, and leaders relied on these external resources to access necessary information and conduct requisite training, ultimately, industry representatives were not substitutes for best practice. These findings flag downstream organizational costs to hospital budgets, in-house expertise, and patient care and suggest the need for further research into the nature and extent of the impacts of outsourcing practice-based education to commercial entities. To ensure safe, quality, and cost-effective care, educators recognized the need to cultivate and retain clinical expertise, with a limited and supervised role for industry representatives. To achieve these goals, practice-based education must be an upstream consideration for procurement, human resources, clinical operations, and professional practice. Investment in practice-based education will pay dividends by attracting and retaining clinicians within cultures of high performance and, in turn, will strengthen patient outcomes.
Supplemental Material
Supplemental Material - Outsourcing practice-based education: The role of industry representatives and implications for clinical expertise
Supplemental Material for Outsourcing practice-based education: The role of industry representatives and implications for clinical expertise by Quinn Grundy, Dana Hart, Brenda Perkins-Meingast, Ann M. Heesters and Fiona A. Miller in Healthcare Management Forum
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Social Sciences and Humanities Research Council (SSHRC), Insight Development Grant #430-2020-00104.
Ethical approval
The University of Toronto Research Ethics Board approved the study (#40900).
Supplemental material
Supplemental material for this article is available on-line.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.