
Abstract
Now in the post-pandemic era, healthcare employers and leaders must navigate decisions around use of telework arrangements made popular during the COVID-19 pandemic. Among healthcare employees who teleworked during the pandemic, this study investigates preference to continue teleworking post-pandemic and the determinants of this preference. An overwhelming majority (99%) preferred to continue teleworking to some degree and the majority (52%) preferred to telework for all work hours. Healthcare employers should consider that most employees who teleworked during the pandemic prefer to continue teleworking for most or all work hours, and that hybrid work arrangements are especially important for clinical telework employees. In addition to space and resource allocation, management considerations include supports to promote productivity, work-life balance, and effective virtual communication while teleworking to promote positive employee health, recruitment, and retention outcomes.
Introduction
In April 2020, a rapid global shift from traditional on-site work to less traditional telework occurred in response to the COVID-19 pandemic in many sectors, including healthcare. 1 During the first year of the pandemic, approximately 17% of Canadian healthcare employees performed most or all work hours via telework. 2 Healthcare employee preference to continue teleworking post-pandemic and the determinants of this preference are important considerations for navigating establishment of future work arrangements as well as broader healthcare organizational planning and workforce management.
While preference to continue teleworking post-pandemic has not been measured in Canada for healthcare employees, a survey of corporate and non-clinical health district employees in Sydney, Australia, who teleworked as a response to the pandemic, found that 90% would take the opportunity to telework again. 3 A multi-sector survey of Canadian employees who newly started teleworking during the pandemic had a similar estimate of 91%; and flexible hybrid work arrangements with telework and on-site components were a more common preference than exclusive telework. 4
Two studies on the determinants of employees’ post-pandemic telework preference were identified. Among Canadian employees, higher productivity while teleworking was a strong determinant of preferring to telework for most or all work hours post-pandemic. 4 Among Vietnamese employees, valuing telework as a solution to air quality issues and having workaholic characteristics such as working late or overtime were positively associated with a preference to telework post-pandemic, while finding pleasure in elements of on-site work such as in-person collaboration or communication with colleagues was negatively associated. 5 A study of university employees in Malaysia conducted shortly prior to the pandemic found that both personal (having a higher number of children in the home and a longer morning commute) and job-level factors (less frequent use of face to face communication or fax machines and more frequent use of e-mail and cellular phones) were important determinants of telework preference. 6
The current study expands knowledge of employee telework preference and determinants to the post-pandemic period with a focus on the healthcare sector. Workplace social norms and practices may vary by sector and geographic region and influence employee telework preference. They may also change over time, particularly in response to the pandemic. As such, findings from prior to the pandemic and other sectors or geographic regions may not be generalizable to the current and future telework preferences of Canadian healthcare employees.
According to person-environment fit theory, compatibility between employee need and the demands or opportunities presented by the work environment contributes to the development of positive health and occupational outcomes.7-8 Improved understanding of healthcare employees’ preferences for the post-pandemic work arrangement can help healthcare organizations to maximize person-environment fit and potentially to recruit and retain employees while also combating burnout and benefiting employees' health and work outcomes.7-8
The aims of this study were two-fold. Using employees of a large healthcare authority in British Columbia, Canada, who teleworked at some point during the pandemic as the target population, the aims were to identify 1) the proportion of employees with a preference for a post-pandemic work arrangement that is exclusively telework, mostly telework, mostly on-site, or entirely on-site and 2) sociodemographic and occupational characteristics and e-working conditions and practices associated with employees’ post-pandemic telework preference.
Methods
A detailed description of the study methods is available on-line. 9
Study sample
The target population included clinical and non-clinical employees of a large regional health authority in British Columbia, Canada, who teleworked during the COVID-19 pandemic. Data were collected using a voluntary survey distributed via Qualtrics 10 between May and June 2021. This was during the latter half of the Delta wave, which was one of the two largest COVID-19 waves in British Columbia. By the end of the data collection period (June 30, 2021), nearly 80% of British Columbian adults had received a first dose of COVID-19 vaccine, and the province was entering step 3 of its 4-step restart plan. 11
Study variables
For the outcome variable, participants were asked “Would you like to continue working from home or performing virtual work following the end of the COVID-19 pandemic?” with four possible response options: “No, not at all,” “Yes, but for less than half of the time,” “Yes, for more than half of the time,” and “Yes, all the time.” “Virtual work” was included in the telework outcome to capture work that adapted use of information technology to communicate with patients or colleagues virtually in place of in-person, as a response to the pandemic, although this work may have been performed in clinic or hospital and not at home. Due to a small number of respondents (n = 5) who indicated “No, not at all,” these respondents were grouped with those who answered “Yes, but for less than half the time” for analysis.
Sociodemographic characteristics included gender identity, age group, and whether or not the respondent identified as having a disability or long-term health condition. For gender identity, due to a small number of non-binary respondents (less than 5), non-binary and women respondents were grouped together to maintain anonymity.12,13 The number of children under 5-years old in the home during work hours and the number of other people over 5-years old in the home during work hours were also included.
Occupational characteristics included having direct reports, full-time job status, being a provider of direct patient care, prior telework experience, and years worked at the organization.
Description of e-work-life scale subscales and items 14 and ergonomic e-work items included on survey.
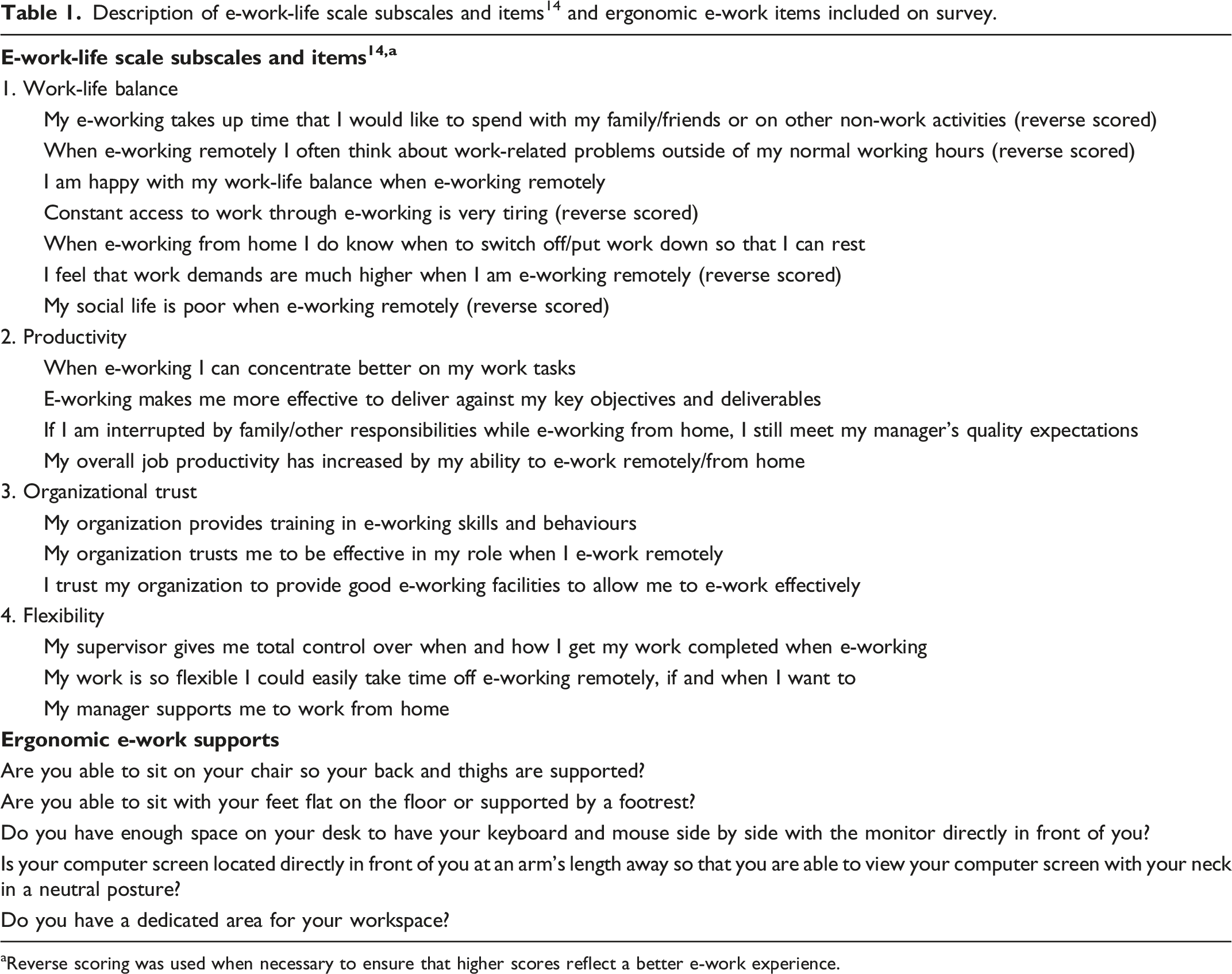
aReverse scoring was used when necessary to ensure that higher scores reflect a better e-work experience.
Analyses
Multinomial logistic regression models were conducted using “less than half the time or not at all” as the reference outcome group. 15 Unadjusted models for each independent variable and the outcome were conducted. For the adjusted models, a three-step hierarchical approach was used 16 with sociodemographic and occupational variables added as the first and second blocks, respectively, and e-working variables added as the third block. Odds Ratios (ORs) and 95% Confidence Intervals (CIs) are reported for all multinomial logistic regression models. Odds radios below .5 or above 2.0 were considered moderate to strong. 17 To assess if each successive block improved the model fit, the Akaike Information Criterion (AIC) value was reported. 18
Results
A total of 453 of an estimated 1,100 employees who teleworked at some point during the pandemic answered the survey. Of these, 53 (11.7%) were excluded due to missing data for one or more study variables. The final study sample included 400 respondents for a 36.4% participation rate.
Characteristics of the study sample by telework preference and overall.
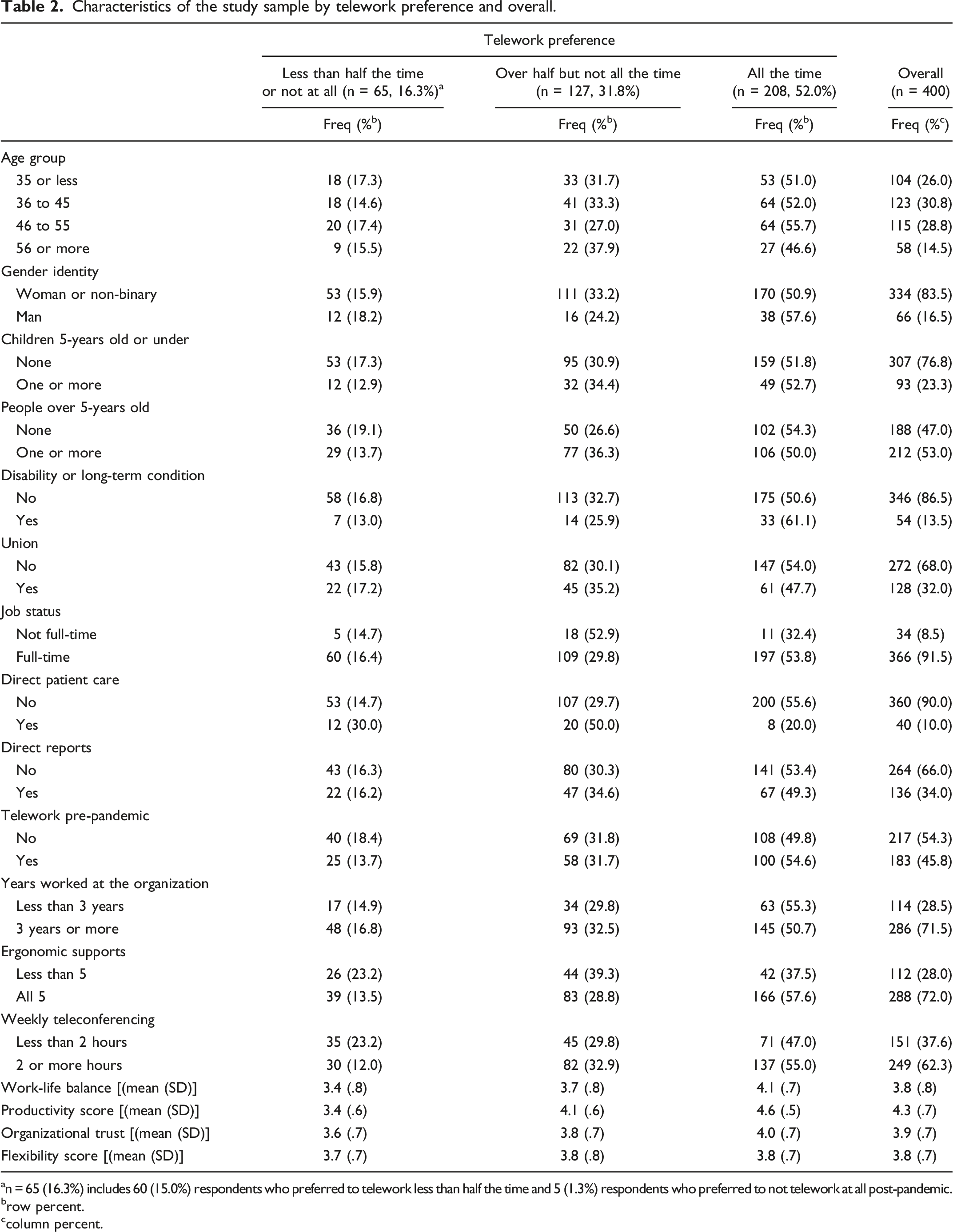
an = 65 (16.3%) includes 60 (15.0%) respondents who preferred to telework less than half the time and 5 (1.3%) respondents who preferred to not telework at all post-pandemic.
brow percent.
ccolumn percent.
After adjusting for other sociodemographic factors, having at least one other person over 5 years of age in the home during working hours was moderately associated with a higher preference to telework over half but not all the time compared to less than half the time or not at all (OR = 2.07, 95% CI: 1.11 to 3.87) (Figure 1). After adjusting for sociodemographic and other occupational factors, being a provider of direct patient care was strongly associated with a lower preference to telework all the time (OR = .14, 95% CI: .05 to .40). After adjusting for sociodemographic, occupational factors, and other e-working conditions, two or more hours of teleconferencing per week compared to less than two hours was moderately associated with a higher preference to telework over half but not all the time (OR = 2.85, 95% CI: 1.25 to 6.46) and all the time (OR = 3.69, 95% CI: 1.52 to 8.92); higher work-life balance was moderately associated with a higher preference to telework all the time (OR = 3.06, 95% CI: 1.65, 5.65); and higher productivity was strongly associated with a higher preference to telework more than half but less than all the time (OR = 7.46, 95% CI: 3.70 to 15.05) and even more strongly associated with a preference to telework all the time (OR = 28.84, 95% CI: 13.22 to 62.92). Association of sociodemographic and occupational characteristics and e-working conditions with telework preference, three-step hierarchical adjusted multinomial logistic regression models (odds ratios (ORs) and 95% confidence intervals (CIs)). *Indicates an odds ratio considered to be moderate or strong (below .5 or above 2.0). Reference groups: Telework preference (less than half the time or not at all), age group (35-years old or less), gender identity (woman or non-binary), children under 5-years old in the home during work hours (none), people over 5-years old in the home during work hours (none), disability or long-term condition (no), union (no), job status (not full-time), direct patient care provider (no), direct reports (no), telework pre-pandemic (no), years worked at the organization (less than 3 years), ergonomic supports (less than 5), and average number of hours spent teleconferencing in a week (less than 2 hours). Interpretation: An odds ratio greater than “1” indicates that the determinant is associated with higher odds of preferring the indicated outcome level rather than the reference level of “less than half the time or not at all.” Conversely, an odds ratio of less than “1” indicates that the determinant is associated with lower odds of preferring the indicated outcome level rather than the reference level of “less than half the time or not at all.”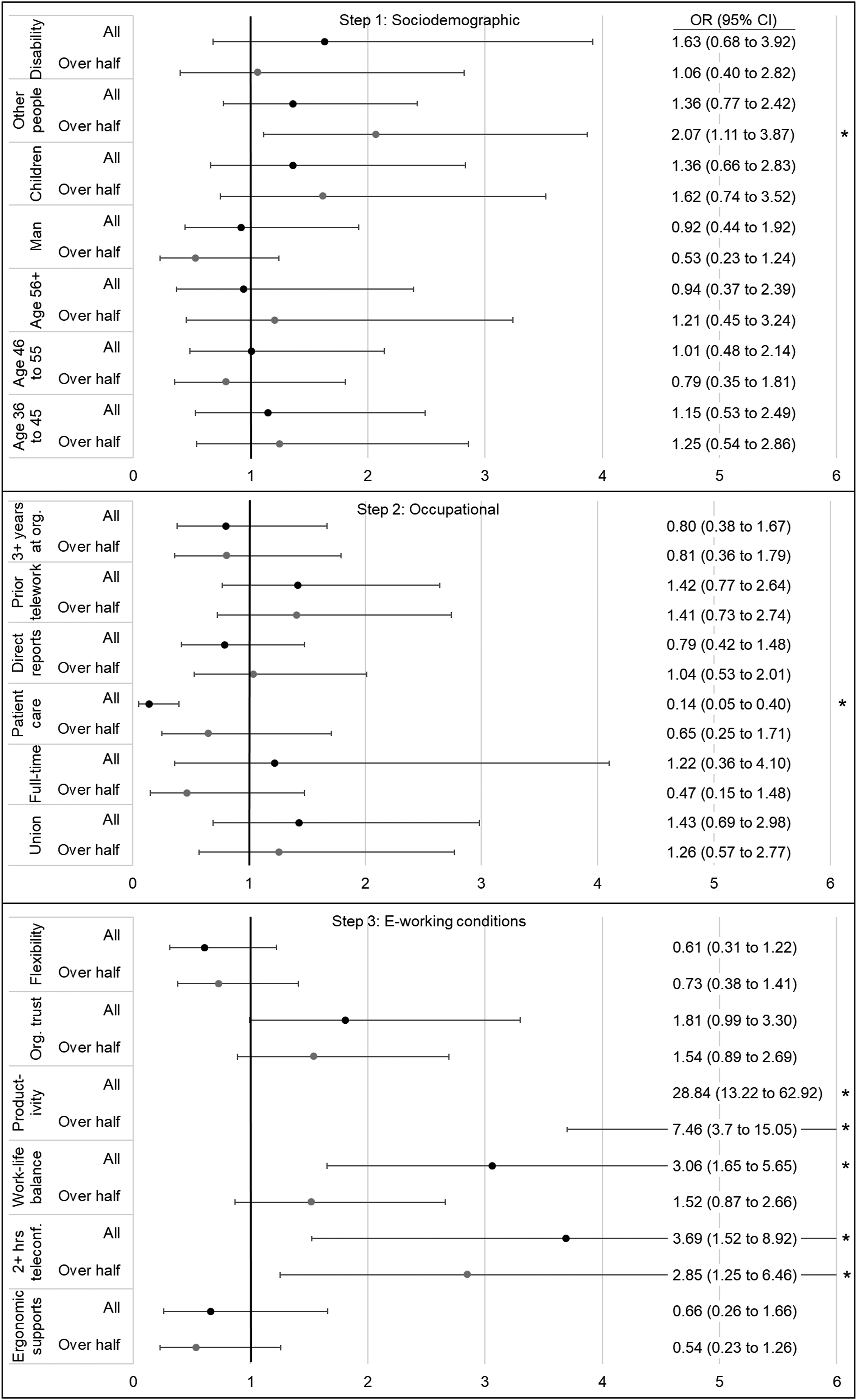
The AIC value decreased across each successive step of the adjusted hierarchical models indicating that the model fit improved with each step.
Discussion
Employee telework preference for the post-pandemic period is a pressing issue for society and employers. Ensuring fit between employee need and the work arrangement has implications for employees and organizations including employee health, job performance, recruitment, and retention.7-8 This study sought to expand current knowledge on telework preferences and its determinants in the healthcare sector for the post-pandemic context.
A key finding was that 99% of the study sample of healthcare employees who teleworked during the pandemic preferred to continue teleworking for either all or some of the time post-pandemic. This estimate is higher than the estimate of 90% reported by an Australian survey of corporate and non-clinical employees of a large health district who adapted home-based telework during the pandemic. 3 This difference may be due to the inclusion of non-home-based telework including virtual work performed in a clinic or hospital in this study’s telework preference measure. It is also higher than a Canadian multi-sector study where the proportion of employees preferring to telework post-pandemic was 91%. 4 In addition to the inclusion of non-home based telework in the telework preference measure, this may be due to a higher proportion of jobs with telework capcacity, higher job security, and longer commute times in the current study sample.6,19 It is notable that 45.8% of the study sample teleworked at least partially immediately prior to the pandemic—indicating a high capacity for telework arrangements under normal circumstances. Long commutes are a potential determinant of telework preference 13 and also likely in the study sample as the regional health authority covers a large geographical service area. Employees with high job security may have less concern about negative occupational outcomes due to being a teleworker, like lack of career progression, and this may in turn increase preference to telework. 19
Another key finding is that there was a relatively even split between preference to telework all the time versus a hybrid arrangement. This finding varies from a multi-sector study of Canadian employees, where employees were five times more likely to prefer a post-pandemic hybrid arrangement over exclusive telework. 4 Reasons for a majority preference to telework for all hours in this study sample may be due to the same mechanisms discussed above.
In this study, being a direct patient care provider was a strong determinant of not preferring to telework for all hours, and higher productivity while teleworking was a strong determinant of preferring to telework for over half and even more so, all work hours. Having two or more weekly teleconference hours and having one or more people over 5-years old in the home while teleworking were both moderate determinants of preferring to telework for over half or all work hours, and higher work-life balance while teleworking was a moderate determinant of preferring to telework for all work hours.
Being a provider of direct patient care may be associated with a preference to not telework all the time due to the limitations of virtual settings for healthcare delivery including difficulty reading body language or social cues, 20 making accurate diagnoses, and delivering treatments especially those that involve physical procedures. Notably, the majority of direct patient care providers in the study sample preferred a hybrid work arrangement with the most common preference being over half the time but not all the time spent teleworking followed by some of the time but less than half the time. This finding is compatible with the results of a recent review finding that overall, healthcare providers were satisfied with use of telehealth during the pandemic and willing to continue using it post-pandemic. 21
Employees with higher work-life balance or productivity while teleworking may prefer to telework for a greater proportion of their work hours due to increased job satisfaction, general health and well-being, and mental health while teleworking.14,22 Employees who scored high on work-life balance or productivity while teleworking may also anticipate that returning to on-site work post-pandemic will negatively affect their work-life balance or productivity, leading them to strongly prefer to continue teleworking for most or all work hours. The current finding for productivity was replicated in a recent multi-sector survey of Canadians. 4
Employees with less than two hours of weekly teleconference activity may be more likely to feel socially isolated from their work colleagues, and this may in turn increase preference to partially return to on-site work with a greater number of hours on site. Alternatively, spending over two hours a week on teleconference activities may reflect effective adaptation of virtual teamwork or telehealth practices which in turn may increase productivity and preference to continue teleworking for a greater number of work hours. In a similar line of thought, employees with no other people over 5-years old in the home during working hours may experience more social isolation while teleworking and this may increase preference to partially return to on-site work with a greater number of hours on site.
Limitations
There are some potential limitations to consider in the interpretation of this study. While a participation rate of 36.4% was achieved, information on non-respondents necessary to determine the representativeness of the study sample was not available for analysis. In addition, no survey questions addressed commuting practices when working on site. Another consideration, for the interpretation of the findings, is the timing of data collection. On the one hand, health anxieties related to COVID-19 and the social normalization of “staying home” due to pandemic restrictions and recommendations may have been elevated and contributed to a higher preference to telework, even post-pandemic. On the other hand, optimism around high rates of vaccine coverage and provincial reopening 11 may have increased preferences to return to on-site work post-pandemic (although the current findings overwhelmingly in support of employees having a positive preference for post-pandemic telework do not support this latter point). Lastly, the results are most generalizable to healthcare and other large organizations in high-income countries, particularly those with a workforce or service area distributed across multiple communities, and a highly educated or skilled workforce with job tasks that can be performed remotely using information technology.
Concluding remarks
These findings have multiple considerations for healthcare organizational policy and practice and workforce planning. They indicate extremely low preference for exclusively on-site work arrangements post-pandemic among healthcare employees who teleworked during the pandemic with over 80% preferring to telework for most or all work hours. This has implications for on-site space allocation, support equipment and services for telework, work-home boundary management, networking facilitation and productivity management for telework arrangements, and return to work planning particularly the allowance of continued telework arrangements for employee satisfaction and retention. The findings indicate a special consideration of continuation of telework for providers of direct patient care; and that hybrid work arrangements with more on-site work hours but not all the time may be more popular among these employees than among employees who do not provide direct patient care. With an increasing shift towards virtual healthcare delivery, this finding still emphasizes the importance of in-person direct healthcare delivery. Another consideration is that long-term continuation of telework practices established during the pandemic may have implications for the on-site work environment including employees unable to perform their job via telework, which is common in healthcare. These include changes to management and collaboration practices and a potential lack of on-site presence by senior employees or decision-makers as well as changes to moral or satisfaction with the work arrangement or overall job for exclusively on-site employees. For employees who experience low productivity, low work-life balance, or infrequent or ineffective virtual communication or socialization with colleagues while teleworking, work arrangements with at least some on-site components, or rather targeted training and supports to address these issues while teleworking, may be beneficial. Lastly, ongoing monitoring of and “check ins” on employee telework preference and telework needs is recommended, both at the organizational and individual employee levels, by employers and managers, respectively. This can inform decision-makers on the need for intervention to maintain or improve compatibility of the work arrangement and employee supports with employees’ preferences with implications for employee well-being, job performance, and retention.7-8
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding acknowledgements
Andrea Jones, Jonathan Fan, and Christopher McLeod are supported by research operating funds through the Partnership for Work Health and Safety—a research partnership between WorkSafeBC (the provincial workers’ compensation system) and the University of British Columbia. Christopher McLeod and Wei Zhang are partially support by a Michael Smith Health Research BC Scholar Award.
Author contributions
We thank Remi Adejumo, Thomas Cline-Salley, Mieke Koehoorn, Melanie Gee, and Suhail Marino for their contributions to the survey development and distribution, participant recruitment, knowledge translation, and project coordination.
Ethical approval
All participants provided informed consent, and ethical approval was provided by the UBC Behavioural Research Ethics Board (#H21-00434) and the Fraser Health Research Ethics Board (#FHREB 2021-030).
Data availability statement
In accordance with the ethics agreement and to protect participant anonymity, data are not available for sharing.