
Abstract
Building high reliable healthcare systems to reduce avoidable patient harm is a global priority. However, there is variability in the application and understanding of the previously identified High Reliability Organization (HRO) principles to make improvements. We describe specific organizational activities exemplifying the five HRO principles during the planning and go-live periods of the new Electronic Health Record (EHR) system at a multi-site academic health sciences centre in Ontario, Canada. Further, we describe a case example where all five HRO principles were exemplified during EHR implementation. Overall, 23 activities exemplifying organizational anticipation and resiliency were identified. Of the 23 activities, 12 occurred during the preparing for go-live and 11 activities occurred during the go-live periods. This article demonstrates how HRO principles can be used in healthcare to detect and adapt to patient safety threats, in order to prevent avoidable patient harm during large scale change.
Introduction
The World Health Organization (WHO) identified building high reliable systems as one of the seven strategic objectives in the Patient Safety Action Plan to eliminate avoidable patient harm. 1 Weick and Sutcliffe described five principles of High Reliability Organizations (HROs): preoccupation with failure, reluctance to simplify, sensitivity to operations, commitment to resilience, and deference to expertise. 2 The first three principles are related to anticipating threats and the latter two principles are concerned with resiliency and adapting to threats. 2 Although the principles of HROs have been characterized and recognized as key in improving health systems, there is variability in the application and understanding of these principles in the healthcare system to make improvements.1,3,4
Our organization is on a journey to becoming a HRO where patient safety threats are anticipated, detected, and contained quickly before compromising patient care. 2 In 2015, our organization made a commitment to reducing avoidable harm. Dedicated resources, education, and structures were developed to improve safety culture, reduce hospital acquired conditions, prevent harm to workers, and decrease avoidable patient harm. Our organization also identified HRO training as a key enabling function for new leaders to be effective in their role. As part of new leader onboarding, leaders are provided with foundational education on HRO principles delivered by the Quality, Safety and Clinical Adoption Team to support leaders in solving problems, and ultimately, contributing towards the organizational goal of zero preventable patient harm. 5 The Quality, Safety and Clinical Adoption Team is a corporate department responsible for developing, implementing, and evaluating structures and processes to support teams in reducing avoidable patient harm and improving quality of care delivery across the organization. This department also supports the organization in meeting provincial regulations related to quality care and Accreditation Canada standards, as well as conducting the review of critical incidents.6,7
In 2022, our multi-site academic health sciences centre in an urban setting with approximately 1,500 beds in Ontario, Canada, went live with a new Electronic Health Record (EHR) system which replaced a primarily paper-based record system. This was an organization-wide change with the potential to impact patient safety and the quality of care delivery. During the planning and go-live periods for the implementation of the new EHR, leaders operated using HRO principles which contributed to a strong organizational focus on quality and safety. 2
In this article, we describe specific organizational activities exemplifying the five HRO principles during the planning and go-live periods of the new EHR system. 2 Further, we describe a case example where all five HRO principles were exemplified during EHR implementation.
Methods
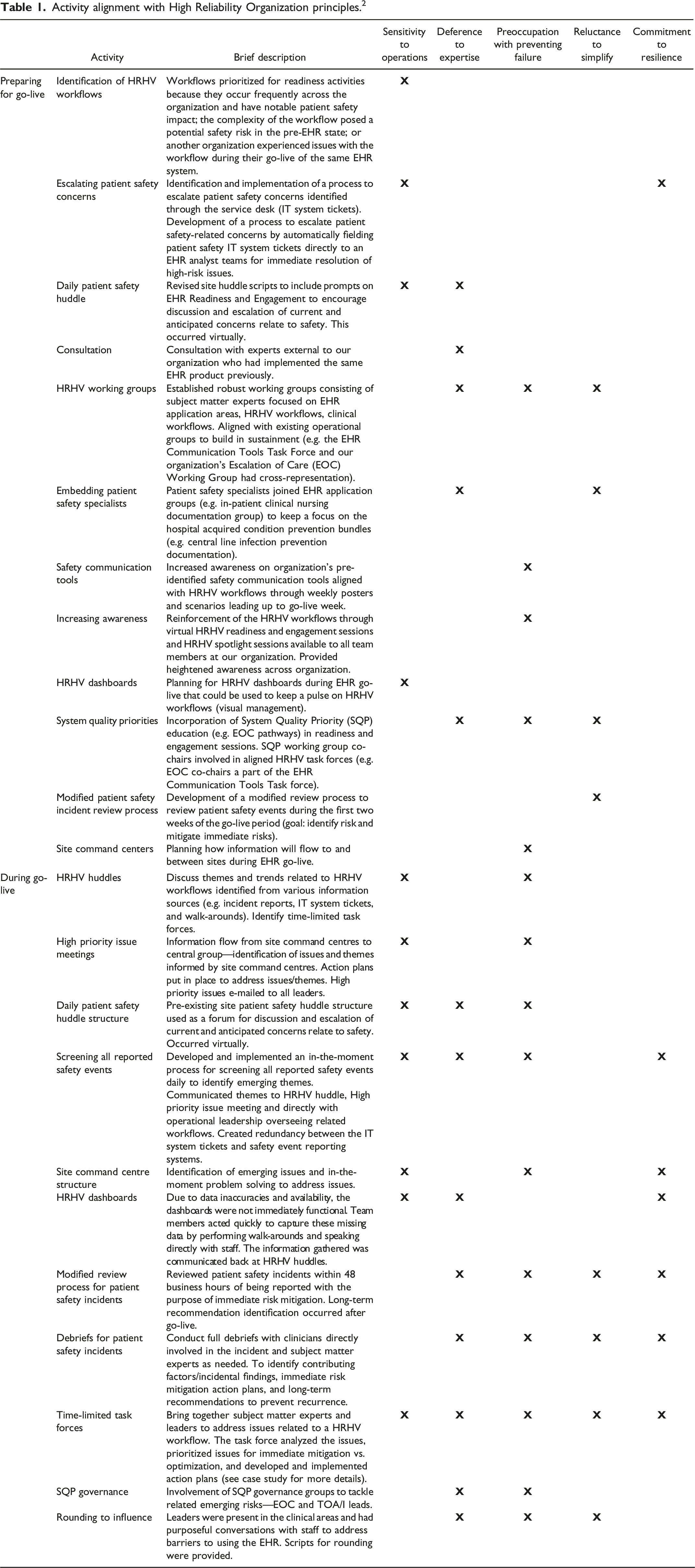
The Quality, Safety and Clinical Adoption Team and other key collaborators of a multi-site academic health sciences centre in Ontario, Canada, identified and documented specific activities exemplifying organizational anticipation and resiliency in the planning (18 months prior to go-live) and go-live periods (the four weeks following go-live) of the new EHR system. Each activity was mapped to one or more of the five HRO principles by members of the Quality, Safety and Clinical Adoption Team and validated by leaders responsible for the clinical transformation. 2
Results
Activity alignment with High Reliability Organization principles 2 .
Case example: Time-limited task forces
Prior to go-live of the new EHR system, the organization prioritized 11 workflows for readiness and engagement activities. These workflows were termed “High Risk High Volume” (HRHV) workflows and were prioritized because they occur frequently across the organization and have notable patient safety impact; the complexity of the workflow posed a potential safety risk in the pre-EHR state; or another organization experienced issues with the workflow during their go-live of the same EHR system. Two days into go-live, the first time-limited task force was struck following the HRHV huddle, which occurred daily and virtually during the first two weeks following go-live. The purpose of the HRHV huddle was to bring subject matter experts and leaders together daily to raise and/or anticipate safety concerns related to HRHV workflows. Data was identified through various sources of information (e.g. incident reporting system, information technology service request tickets, and leader discussions with frontline staff). The huddle structure was familiar and viewed as value-add to leaders as daily safety huddles have been used at our organization since 2017 as a patient safety tool to identify and effectively fix issues as they arise, as well as build awareness around anticipatory thinking with respect to potential safety issues. Attendees of the HRHV huddle were pre-determined prior to go-live and included members from patient safety, practice leadership, and medical leadership, as well as the EHR leaders, educators, and project managers. Preparing for EHR implementation was a multi-year initiative and many individuals were hired or seconded to work on facets of the EHR project (e.g. education and change management) prior to and after go-live.
The first of a few time-limited task force was established to address concerns related to the heparin nomogram infusion workflow—aligned with a pre-identified HRHV workflow. During a HRHV huddle, multiple sources of information came forward highlighting a potental safety risk with the administration of unfractionated heparin through continuous infusions. The huddle attendees were preoccupied with preventing failure and recognized the concerns raised regarding heparin could be indicative of a larger safety concern. With a reluctance to simplify, the time-limited heparin task force was developed to delve deeper into the concerns raised. Prior to go-live, the need for time-limited task forces was not anticipated. The concept and use of time-limited task forces emerged during the go-live period to adapt to patient safety threats as they were detected, an example of resilience.
The time-limited heparin task force deferred to experts and included representation from the Safe Medication Practice Committee, Quality, Safety and Clinical Adoption, Healthcare Human Factors, Pharmacy EHR Application Team, Pharmacy, Haematology, Professional Practice-Nursing, and the EHR Education Team. The majority of these teams had dedicated resources prior to go-live recognizing the EHR would need to be optimized. This time-limited task force brought together experts to identify issues related to the HRHV workflow; prioritize issues for immediate mitigation vs. optimization; and assign and validate actions to the appropriate organizational governing groups.
In order to understand the heparin nomogram workflow concerns, the time-limited heparin task force looked into patient safety incidents reported in the organization’s incident reporting system. As the time-limited task force was preoccupied with preventing failure, they recognized reported incidents could be a signal for a widespread issue. Further, a heuristics evaluation was performed on the technology used to administer the continuous heparin infusion with frontline staff by experts in Human Factors. The time-limited heparin task force was also reluctant to simplify the heparin nomogram concerns. Recognizing the heparin workflow concerns were likely not unique to the heparin nomogram; the time-limited heparin task force expanded their scope to all nomogram workflows (e.g. insulin and argatroban). With a holistic understanding of the nomogram workflow concerns and input from a multi-disciplinary team, the time-limited heparin task force was able to quickly develop and action multiple recommendations to improve the safety of nomogram infusions within 13 days. Through the time-limited heparin task force’s anticipatory and resilient actions, the organization was able mitigate the identified issues preventing patient harm related to nomogram infusions during the go-live period.
HROs are not only concerned with preventing error but also learning from when things go right (resiliency and adaptability). 4 Our organization recognized the benefits of a coordinated approach to anticipate, as well as adapt and respond to safety threats. Following the time-limited heparin task force, five more time-limited task forces were struck to address concerns related to other pre-identified HRHV workflows. These ad hoc and time-limited task forces contributed to preventing critical incidents related to the pre-identified 11 HRHV workflows during the go-live period.
Discussion
Implementing a new EHR system across a multi-site academic health science centre was a large clinical transformation requiring coordinated attention to quality and safety in the planning and go-live periods. The introduction of the new EHR disrupted the pre-existing work system, and new processes were introduced which had the potential to impact patient and organizational outcomes (e.g. avoidable patient harm). 8 Applying HRO principles enhanced the organization’s ability to provide high quality care, as well as understand the complexity of the system during a large scale clinical transformation. 2 Further, the HRO principles supported the organization in continuously developing practical solutions for specific problems informed by experts. 5 As this clinical transformation had implications for almost everyone in the organization, we believe it created the burning platform for engagement and focus on quality and safety concerns related to the EHR. This reinforces the need for coordinated efforts to reduce avoidable patient harm, which can be challenging to consistently achieve in healthcare when leaders have multiple competing priorities. 4
The alignment of HRO principles depicted in Table 1 and the case study were shared with senior leaders within our organization, which also was important exercise in reinforcing how HRO principles can be embedded into daily work. Although providing HRO trainings is key in implementing HRO principles, variability in understanding of HRO principles exists and is a challenge in healthcare.3,9 Thus, providing specific examples to leaders, with a focus on the goal of eliminating preventable harm, may improve understanding and utility of the principles moving forward.
Conclusion
Practical examples of HRO principles in action to improve quality and safety during a large scale clinical transformation were provided. This experience reinforced the requirement for a coordinated and collective commitment to HRO principles in order to create system redundancies capable of detecting and adapting to patient safety threats, in order to prevent avoidable patient harm. Although this article reports on the experience of a single organization, providing concrete examples can support individuals and other organizations in understanding the importance of implementing HRO principles into daily work.
Footnotes
Acknowledgements
Chelsea King, Robert Slepin, and University Health Network’s Quality, Safety and Clinical Adoption Team reviewed HRO principle mapping. Dr. Lucas Chartier reviewed the manuscript draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.