
Abstract
For-profit virtual medical care has been expanding rapidly in Canada, creating new societal and practical challenges requiring policy and regulatory reform. We mapped the current state of regulatory policy across 10 Canadian provinces by analyzing practice standards and guidelines for virtual care from medical profession regulators. Through a comparative framework, we assessed the extent to which virtual practice policies addressed issues around mobility and licensure, equitable access, privacy, complaints, and continuity of care. We also compared these regulatory documents to the model standards from the Canadian medical regulatory consortium and considered implications for practicing in for-profit virtual environments. We found considerable variation across provincial regulatory bodies, with most existing frameworks not adequately addressing equity, access, and practitioner competency and not providing flexible, nuanced, or risk-based approaches to virtual care provision. As we compared jurisdictions, we identified gaps and leading practices to inform recommendations for professional regulators and policy-makers.
Introduction
For-profit virtual medical care has been expanding rapidly in Canada—with growth driven by the pandemic, primary care provider shortages, digital literacy, and consumer interest1,2—generating new challenges for regulators, governments, and other policy-makers. Several regulatory gaps and problem areas have been revealed, including cross-jurisdictional service provision, continuity of care, complaints, privacy, and equitable access.3–5 Many Canadian medical profession regulators have recently reformed their standards and guidance to keep pace with this quickly evolving digital space. We examined regulatory guidance and standards published by provincial colleges regulating physicians and surgeons in Canada, considering their implications for challenges raised by for-profit virtual practice. We identify leading practices and conclude with recommendations for professional regulators and policy-makers.
Virtual medical practice (public and for-profit)
Virtual medical practice entails providing services via Information and Communication Technologies (ICTs) to patients who are not in the same physical location as care providers.1,6 Alternative terms include telehealth and telemedicine, but as virtual care is the terminology most used by medical regulators, we utilize this term here.2,6 Some commentators label these ICTs “disruptive technologies” that alter traditional modes of professional practice. 7 However, the technologies involved in virtual practice are not inherently disruptive and are likely regarded by most users as mundane: telephones, smartphone applications, and video chat software. What is disruptive is the use of these technologies in a manner that disrupts traditional relationships and modes of communication between patients and providers. This is particularly the case with for-profit virtual medicine, where ICTs are used by private corporations to generate profit within the existing public healthcare system.8,9 This is a particularly important issue for professional regulators as they are responsible for regulating these relationships between care providers and consumers/patients. The expansion of virtual practice also challenges prevailing provincial and federal government policies.10,11
The literature on virtual care has identified several areas for societal and regulatory concern. For example, there are questions about the quality of care that can be provided virtually given that some ailments cannot be diagnosed without a physical assessment.1,4,12 Furthermore, ICTs facilitate medical practice across geographical borders making it possible, if not always legal, for a consumer to receive virtual care from a medical provider in another province or country. 5 The ease with which virtual care can be provided at a distance increases pressure to relax regional licensing regimes (and to facilitate more global labour mobility).1,13 At the same time, virtual care has increased privacy and confidentiality concerns and raised questions about how to address patient complaints and professional malpractice.1,3,5
These challenges and others are amplified in the case of for-profit virtual care. 14 The number of corporations providing virtual care through smartphone applications (apps) has increased substantially since early 2020, as has the willingness of provincial governments to cover the cost of at least some of these services through provincial health insurance plans—although the extent to which this occurs varies by province. 4 Whether they charge a subscription or membership fees from users or bill the government (or both), these corporations employ medical doctors who provide care through the app at a fixed wage. For care providers, these arrangements can be economically advantageous and may free them from the burden of running their own practice.8,9
Advocates contend that these for-profit platforms help to ease the primary care provider shortage in Canada, facilitating access to routine episodic care in times and areas of need. 1 During the COVID-19 pandemic, the need for virtual care rose dramatically and for-profit corporate providers filled a gap as governments pivoted to provide reimbursement for virtual services. Patient (and potentially provider) preferences for virtual care services, even post-pandemic, will ensure a continued market for corporate providers.
Critics, however, raise several concerns about for-profit virtual care. One set of concerns surrounds data privacy and the security of patients’ health information. 1 For example, patient medical information might be stored outside of Canada and used by corporations (or foreign governments) for unspecified purposes; a review by Alberta’s Office of the Information and Privacy Commissioner found violations by both corporations and care providers.10,11 Concerns have been raised about quality and continuity of care since apps function as virtual walk-in clinics. Providers on these apps may not have access to patients’ medical records to inform their assessments or the ability to update medical records.3,14 Moreover, there can be little to no follow-up to ensure patients get the treatment they need. Critics also contend that for-profit virtual care adds burdens (and, somewhat counterintuitively, costs) to the public health system: Many providers on for-profit telehealth platforms cannot offer in-person visits and may instead refer patients to hospital urgent care or emergency departments, leading to unnecessary emergency crowding and double-billing for healthcare services (once by the corporate virtual care provider, and once by the in-person provider).9,14 Critics also question if for-profit virtual platforms incentivize ordering unnecessary tests given the priority of revenue over patient outcomes, further increasing costs to the public purse. 14
Equitable access is one of the most significant concerns about the rapid expansion of for-profit virtual care.1,5,14 These apps do not increase the number of providers available; rather, they redistribute existing health workforce resources, moving some on-line. 4 Access to care, then, is not expanding but instead shifting in a manner shaped by prevailing digital inequalities, which privilege the young, well-to-do, and urban.15,16 Populations with higher health needs or greater access barriers—such as racialized, Indigenous, older, and rural populations—could see their access to services decline. For-profit virtual care, like all for-profit care, has the potential to expand access to the privileged, at the expense of others, exacerbating health inequalities. For these reasons, commentators raise concerns about the emergence of a two-tiered healthcare system.8,14
In this manner, for-profit virtual care has created several societal and practical challenges requiring policy and regulatory reform.
Methodology
We explored how well medical profession regulators were grappling with these issues as they revised their policies to address the expansion of virtual medical care, especially for-profit virtual care through apps. We mapped the current state of regulatory policy across ten Canadian provinces by collecting and analyzing practice standards and guidelines from physician regulators’ web sites. We also included the Federation of Medical Regulatory Authorities of Canada’s (FMRAC) 2022 Virtual Care Framework 6 to determine how closely individual regulators’ guidance conformed to these model standards. We used spreadsheet software to organize and analyze the information from the retrieved documents. A comparative descriptive structure was developed based on our objective to analyze the comprehensiveness and content of the professional regulatory frameworks for virtual care across Canada. Our analytical strategy was both deductive and inductive. Deductively, we assessed the extent to which virtual practice policies addressed issues raised in the literature around mobility and licensure, equitable access, privacy, and continuity of care. Inductively, we examined the content of the policies, attentive to emergent categories and areas of difference and convergence. As we compared jurisdictions, we identified gaps and leading practices that inform our policy recommendations.
Findings
Comparison of regulatory guidance, standards, and policies for virtual care across 10 Canadian provinces.
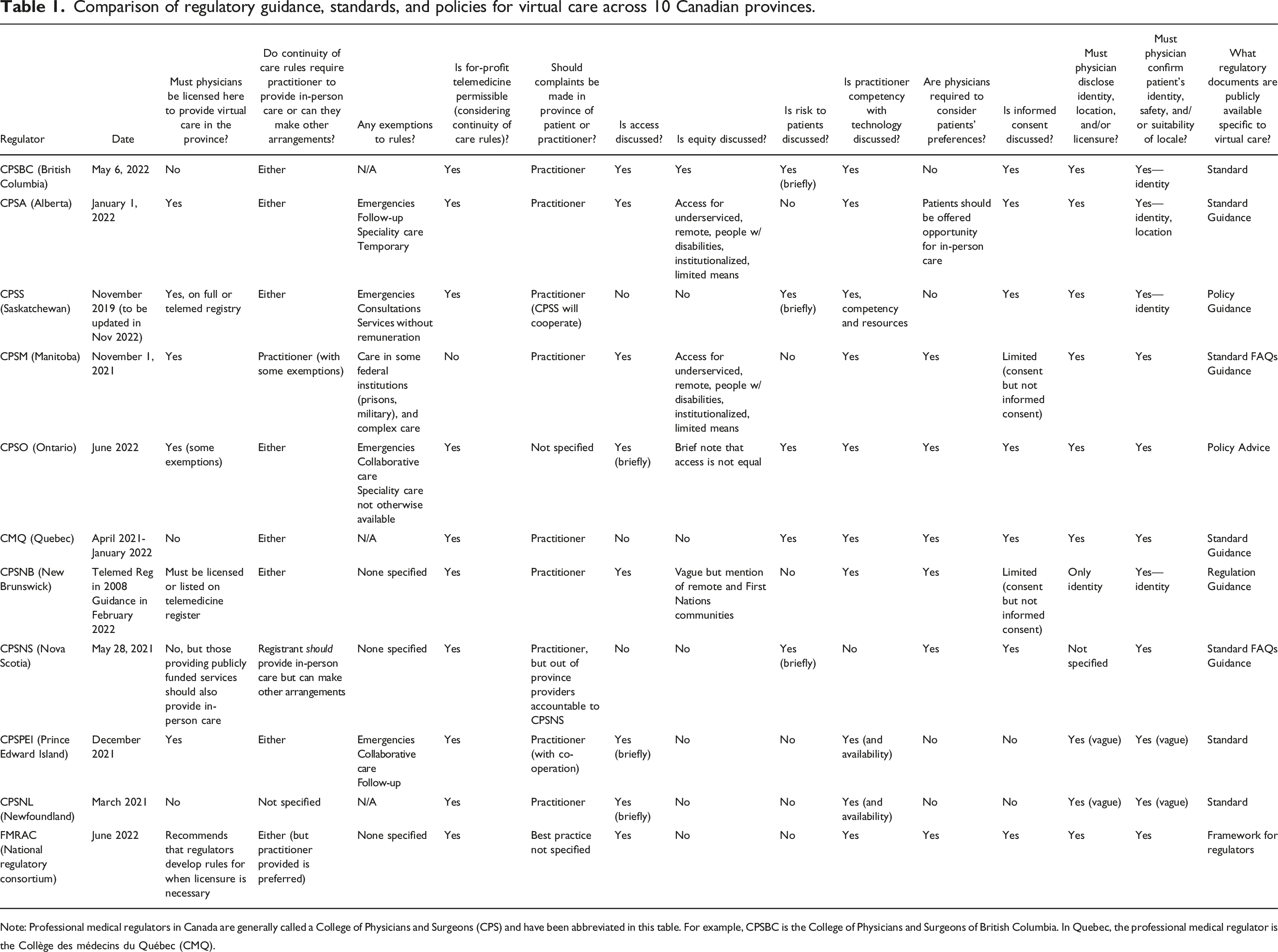
Note: Professional medical regulators in Canada are generally called a College of Physicians and Surgeons (CPS) and have been abbreviated in this table. For example, CPSBC is the College of Physicians and Surgeons of British Columbia. In Quebec, the professional medical regulator is the Collège des médecins du Québec (CMQ).
One key, yet not surprising, finding was that policies and guidance differ across provincial regulatory bodies; even the wording of the definitions of virtual practice varies across documents. Many policies focus on licensing/registration requirements, privacy considerations, and requirements for continuity of care. Attention to other areas of concern like equitable access, discipline/complaints, and risks to patient care was uneven. Competencies required to meet the standard of care in virtual encounters and accommodating patient preferences received more attention but were not incorporated in every province.
Location of licensure
In most provinces, medical practitioners providing services to patients living in that province—whether virtually or in person—are expected to be licensed/registered to practice in that province. Two provinces (New Brunswick and Saskatchewan) have a telemedicine registry for virtual practice17,18; in Saskatchewan, the fee for this licensure category is tiered based on the number of patients (with physicians seeing over 52 patients paying the regular fee). 17 At least half of the provinces provide exemptions to the licensure rule, allowing virtual practice on an emergency or temporary basis, as part of follow-up care, or when providing speciality services or collaborating with physicians in the province. Typically, documents specify that complaints about care are handled in the practitioners’ home province. Nonetheless, some add that the regulator where the service was provided (and the patient was located) will collaborate with the home province regulator to address complaints and discipline.
Continuity of care
Continuity-of-care provisions are a newer addition to regulatory guidance/standards in many provinces, receiving more attention in documents produced in the last year or two. Most medical regulators now require physicians providing virtual care to have arrangements to ensure patients have local access to in-person follow-up care, should that be necessary. Several regulators strongly encourage registrants to provide that follow-up care personally, but this is not a requirement except in Manitoba 19 (and, for publicly funded services, Nova Scotia 20 ). In other provinces, regulators state that if the virtual care provider cannot personally provide in-person care, they must establish what the Collège des médecins du Québec (CMQ) refers to as a “corridor de référence” 21 —a referral network with clinics and practitioners in the region where virtual care is being provided. General referrals to clinics or emergency departments (for non-emergency care) are sometimes explicitly forbidden. This continuity-of-care guidance addresses the lack of follow-up and unnecessary emergency visits associated with for-profit virtual medical care. However, stringent policies like the CPSM’s in Manitoba prohibit employment on virtual platforms, especially cross-provincially. 19 Regulators with similar policies in the United States have been accused of being anti-competitive and taken to court. 13 In contrast, policies in other provinces that allow for a referral network are compatible with (for-profit) virtual care, although their requirements could make participating in for-profit virtual care (especially across provinces) a challenge for some providers (those employed by corporations that also operate in-person clinics should have fewer difficulties).
Privacy, consent, and risk management
Given the concerns about privacy and data security in for-profit virtual medical care, it is not surprising that most recently revised policies speak to privacy, security, and the risks of virtual practice, with a majority requiring that physicians obtain informed consent before providing virtual care, as recommended by FMRAC, 6 after explaining the risks and limitations of these virtual encounters to patients. Five provinces, however, do not mention risks, and an additional three mention them in only a cursory way. All mention privacy considerations, although some go into more detail than others. The more detailed policies and guidance from the CMQ appear to represent leading practice in this category. Half of the policies mention that the patient’s preferences should be considered when physicians determine if virtual care is in the patient’s best interest.
Equitable access to care
Standards and policies say little about equitable access to care. Several provincial regulators include a statement highlighting that virtual care can improve access to underserviced groups; however, only CPSBC acknowledges that virtual care can exacerbate inequalities. 22 Equity is rarely mentioned. CPSBC’s standards stand out in advising registrants to use “an equity-oriented approach and seek to understand and address any barriers that their patients may face in participating in virtual care.”22(p2)
Technological competence
In terms of the patient-provider interaction, most policies insist that practitioners have sufficient technological competence to provide virtual care; however, there are few details about what this means. FMRAC 6 and some provincial guidance specify exactly what practitioners should tell their patients about themselves (identity, location, and licensure) and what practitioners should confirm about their patients (name and suitable location), but others do not. Some regulators refer doctors to the helpful Canadian Medical Association’s Virtual Care Playbook, which details how physicians can provide virtual care safely and with appropriate “webside manners.” 12 Team-based care, however, is not addressed in standards or guidance.
Discussion and policy considerations
Professional regulators are finding ways to regulate for-profit, platform-mediated virtual care, but most existing frameworks do not adequately address equity, access, and practitioner competency. Existing frameworks are inflexible, making it difficult for practitioners to provide care virtually in some regions, or for regulators to deal with complaints should they arise in others. The requirement for a referral network is positive for continuity of care but may erect barriers for care providers, except those employed by large corporations with access to a network of corporate clinics. There are challenges with the existing complaint process, as the CMQ explains: patients unsatisfied with their virtual care provider located outside of Quebec must file a complaint with the doctor’s home regulator, and that could be challenging (potentially involving language and other barriers). 23
Further challenges with the complaints and discipline regime may arise when technological incompetence is alleged in the provision of virtual care. While most virtual care standards we reviewed included a general requirement of technological competence, the scope of this duty was not clear. Medical profession regulators should consider more clearly articulating what is required for providers to be technologically competent. Many Canadian and American legal regulators have enacted a more comprehensive duty of technological competence that might provide guidance for medical profession regulators.2,24,25
Moreover, despite the trend towards risk-based and right-touch regulation, few regulators have adopted a risk-based approach to regulating virtual care. A risk-based approach would help identify current and emerging risks associated with virtual care, particularly where commercial interests are involved. These emerging risks include increased reliance on artificial intelligence for clinical decision-making, an area where lines of accountability and the role of professional regulation is currently unclear.26–28
Furthermore, there is considerable inconsistency across provinces, which could lead to confusion, hampering the provision of competent, safe care. The FMRAC’s model standards for virtual care 6 are meant to advance pan-Canadian consistency, but they came out in mid-2022 after most regulators had revised their virtual care standards and guidance in 2021 or earlier in 2022. Thus, the influence of these model standards is unclear. Of note, FMRAC also halted its work on telemedicine licensure and license portability agreements. 29 Additionally, those policies prohibiting for-profit virtual care could generate opposition from corporations for being anti-competitive.
Recommendations for regulators and policy-makers.
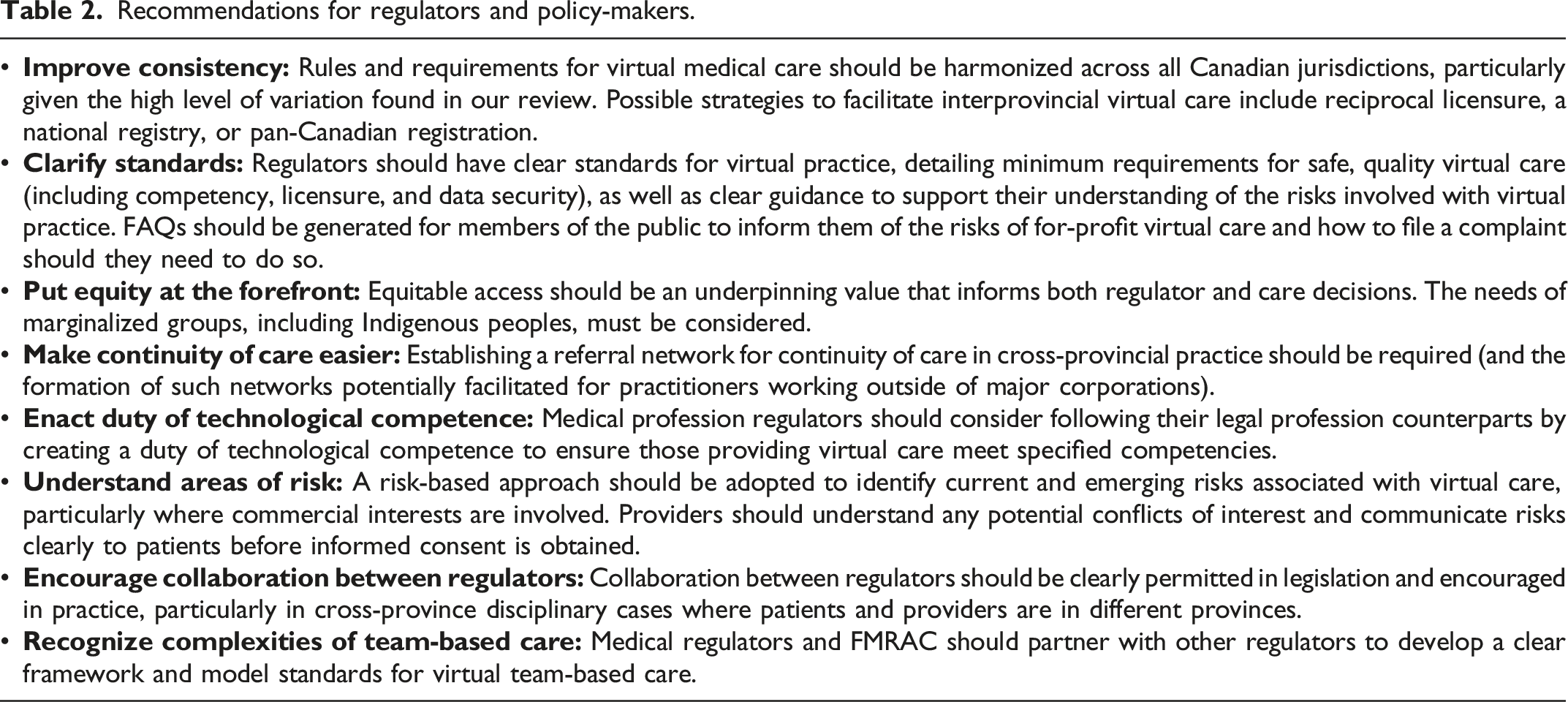
Together these changes would generate regulatory guidance and standards that are not only more consistent across the country, but that also address key concerns with virtual care including privacy, access, equity, risk, and competency. Such guidance is crucial to inform the practice of physicians and allow informed decision-making by the public, ultimately contributing to the public interest in the context of the expanding privatization of virtual care in Canada. Co-operation and collaboration among regulators, governments, and virtual care corporations in Canada and internationally is necessary to address the more systemic concerns around for-profit virtual care.
Footnotes
Acknowledgements
This research is based in part on a grant from the Social Sciences and Humanities Research Council. We would like to thank the reviewers and editor for their helpful feedback and guidance and Bruna Moraes for her research assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada.
Ethical approval
Institutional Review Board approval was not required.