
Abstract
The time has come to develop and implement a Canadian strategy on equitable access to Assistive Technology (AT). AT use has significant health, social, and economic benefits for people with disabilities and older people, and benefits society by assisting to mitigate the most prominent health and social challenges of our time. Our research with citizens (with/without experiences of disabilities or AT use) and system leaders across Canada determined that access is variable and inequitable, with unmet needs, restricted funding, and inefficiencies. Collaboratively, we devised a blueprint, comprising a policy vision, three priority issues to address, principles to underpin policy actions, and short- and long-term priorities, from which to build a strategy. We hope the blueprint sparks action among citizens and health leaders, especially those working across governments, sectors, and communities to promote leadership and create a cross-jurisdictional coalition to elaborate on a national strategy and action plans for moving forward.
Introduction
“Disability is part of being human. Almost everyone will temporarily or permanently experience disability at some point in their life” (WHO 1 ).
About 6.2 million or 22% of Canadians 15 years and older reported living with one or more disabilities in 2017. 2 This represents a range of 13% of Canadians 15-24 years old to 47% of Canadians 75 years and older. Assistive Technology (AT) helps people with disabilities to manage their conditions, supporting daily function and safety, community participation, productivity, and societal inclusion. AT empowers people to live with dignity, autonomy, and less reliance on others, and to age in their preferred communities. Caregivers may use AT to assist others or perform their roles. AT use may help to reduce direct/indirect costs of health and social services. One or more AT products (i.e., aids and devices) were reported to be used by more than 80% of Canadians with disabilities, with product use increasing with age. 3 Access to and use of AT has significant health, social, and economic benefits, and contribute to mitigating the most prominent health and social challenges of our time.
In this article, we present the case for developing and implementing a national strategy for enhancing equitable access to AT in Canada. We provide an overview of AT, highlight why access is topical, and describe the current state of access, including results from our engagement and research with citizens with/without lived experiences of disabilities and AT use (hereafter called citizens), representatives from disability, older adult, and caregiver advocacy groups, professional organizations, healthcare providers, and industry, policy-makers, and academics. We consolidate results into a blueprint for a national strategy for further development and discuss implications for health leaders.
Background
Assistive technology
AT covers a range of technology products (e.g., devices and software) and services (e.g., assessment and training) used by people with disabilities to perform and participate in daily activities. In Canadian policy and legislation, variable terms are used for AT products (e.g., aids, devices, and durable medical equipment).4,5 AT includes products specifically for people with disabilities, including wheelchairs, medication reminders, or symptom management apps, and products for the general population, including computers and software for teleconferencing, smart home systems, and mobile scheduling apps. AT is a universal enabler since use can have beneficial outcomes for people of all ages with diverse conditions and abilities to perform various activities in different contexts, in addition to helping caregivers in their roles.6-8 For people with disabilities and older adults, AT supports access to health and social services, health and well-being, education, employment, and justice, and use of AT facilitates inclusion and participation in social, economic, and political realms of life.8,9 Beyond economic benefits for individuals, society benefits from individuals’ use of AT through improved health, well-being, and quality of life outcomes, and enhanced productivity, decreased direct/indirect health and social services costs, and a strengthened labour force. 9
Why is access to assistive technology topical?
The convergence of several global and local demographic, social, and economic forces intensify the urgency to implement mechanisms for enhancing equity in health and social circumstances and well-being of citizens and ensuring efficient use of limited resources. Population ageing is the most remarkable demographic shift in industrialized countries like Canada. By 2030, the proportion of Canadians 65 years and older will be between 21.4% to 23.4%, a change from 17.2% in 2018. 10 With advancing age, there is an increased likelihood of experiencing health conditions resulting in disability such as hearing/vision loss, osteoarthritis, pulmonary disease, diabetes, depression, and dementia. 11 People are living longer, and with improved medical care more people are living with non-communicable diseases leading to chronic disability, such as cardiovascular diseases, cancers, respiratory diseases, and diabetes. 12
The COVID-19 pandemic has resulted in a significant number of people living with long-term residual affects after infection and disproportionately negatively impacted the health and wellness of people with disabilities and older people. These groups are at higher risk for infection, more susceptible to poor health outcomes, and less able to access health and social services. 13 As of June 2022, almost 3.9 million cases of COVID-19 infection have been recorded in Canada, 14 although the number is likely an underestimate as 35% of cases are asymptomatic. 15 Post COVID-19 condition involves multiple systems—respiratory, cardiovascular, musculoskeletal, cognitive, and mental health, and involvement of any may have disabling effects. The percentage of people with post COVID-19 condition is between 10% and 70%, with the wide range resulting from inconsistent definitions/assessments, and other factors. 16 Long-term impacts on health and social systems are expected above and beyond existing demographic factors which are driving service demand. Long-term rehabilitation and disability supports such as homecare services and AT will be essential as people contend with disability, 17 as will be the imperative to ensure needs are met equitably and efficiently.
Profound technological advances have afforded people with disabilities greater autonomy and enhanced daily life participation. Proliferation of Information and Communication Technologies (ICTs), ambient sensors, wearable technologies, artificial intelligence, and robotics has created transformational opportunities. ICT use has become commonplace during the pandemic, allowing people to continue social interactions, receive telehealth services, transmit public health information, and maintain productivity. 18 Pervasive use of these technologies in all spheres of life is anticipated to continue. However, opportunities afforded by technology will not translate to benefits if people with disabilities are unaware of or cannot access them, or if services are implemented such that inequities multiply. AT access is a fundamental human right and calls have been made for universal access. 8 There is also increasing support for Internet access as a fundamental right with the transitioning of basic services such as government and emergency information to digital formats.
What is the status of access to assistive technology in Canada?
Canadian systems that provide AT funding and services are highly complex and uncoordinated. Programs and services are variable and characterized by multiple access barriers, coverage disparities, and unmet needs.4,19-21 Twenty-six percent of Canadians 15 years old and older living with a disability experienced unmet needs for disability supports (i.e., aids, devices, and medications). 2 There is no overarching federal legislation or policy covering the needs of people with disabilities and disability supports such as AT. AT is not part of universal health coverage. Funding and services are delivered by government, charity, private insurance (e.g., employment benefits), workplace safety insurance (e.g., provincially/territorially legislated employer programs), automobile insurance (e.g., provincial crown corporations), and other sources. A jurisdictional scan of government programs completed in 2017 showed there were seven federal programs and between two to 10 programs in each province/territory covering AT for adults/older adults. 4 Federally, these include programs within ministries, departments, or agencies, including Veterans Affairs, Immigration, Refugees and Citizenship, Health (for First Nations and Inuit Peoples), Public Safety and Emergency Preparedness (for correctional services), and Employment and Social Development Canada. Diverse ministries and departments (or combinations of these) administer AT programs in provinces/territories, such as health, social services, community services, seniors and housing, children and family services, human resources and skills development, labour, or finance. The scan also found that the charity sector augments government programs through 16 national charities and between two to 19 programs in each province/territory. Minimum standards for who should be covered and what AT should be covered do not exist.20,22 Variations exist for eligibility criteria, types of products or services covered, funding (e.g., co-funding and equipment loans), who is authorized to prescribe, application procedures, and documentation requirements. Inequitable access, including system navigation problems and coverage disparities, and inefficiencies (e.g., excess time and money spent by users and healthcare providers) have been reported by citizens, representatives from disability, older adult, and caregiver advocacy groups, professional organizations, healthcare providers, and industry, policy-makers, and academics.5,20,23-26 Owing to difficulties navigating this complex system, we launched an on-line database resource called AccessATCanada to assist AT users, caregivers, and providers to search for programs and services. 27
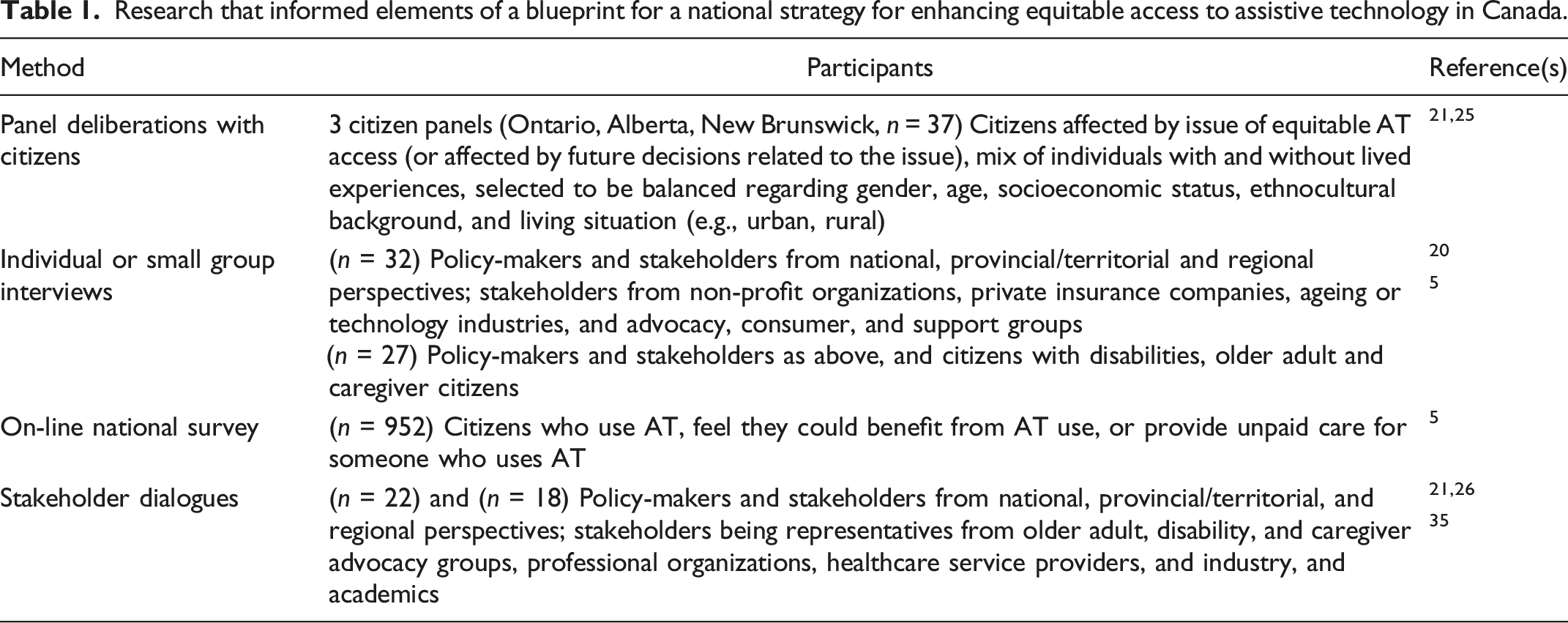
Research that informed elements of a blueprint for a national strategy for enhancing equitable access to assistive technology in Canada.
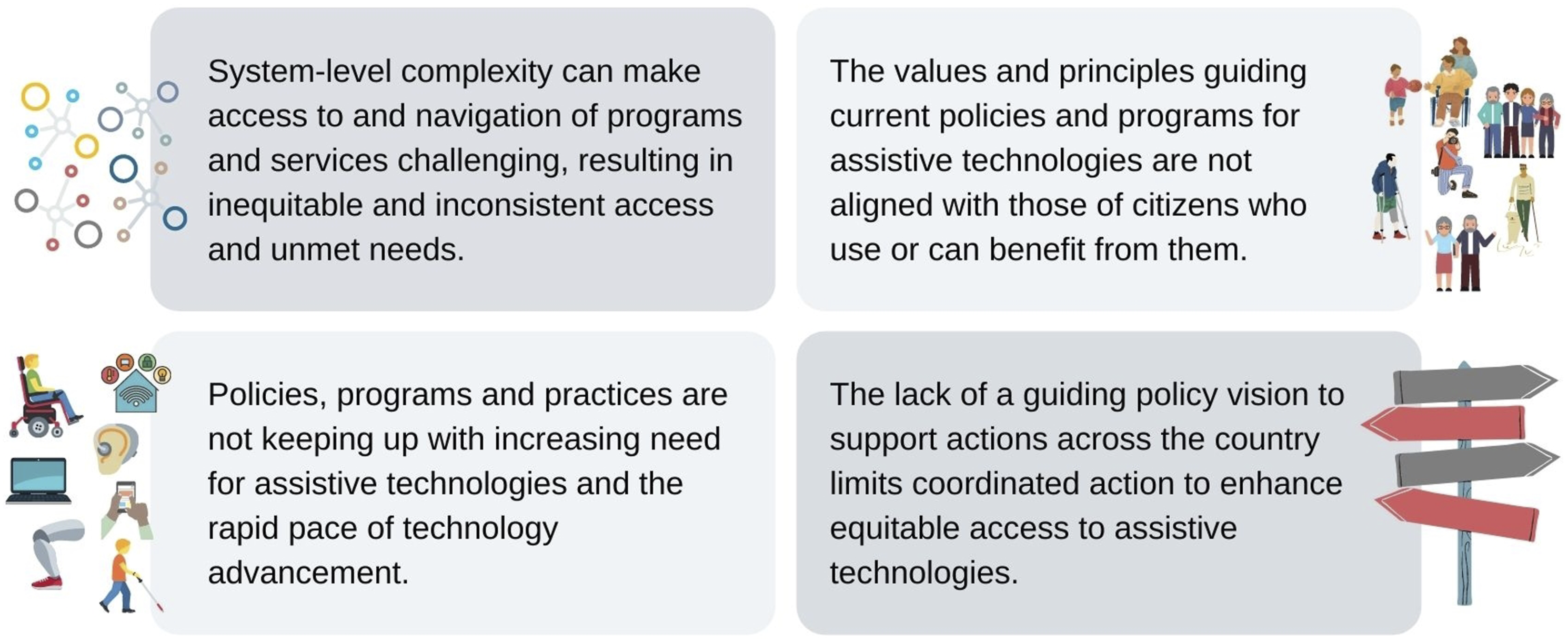
Challenges for enhancing equitable access to assistive technology in Canada.
A national strategy
Why a strategy?
The World Health Organization (WHO) defines National Health Policies, Strategies, and Plans (NHPSPs) as “defining a country's vision, policy directions, and strategies for ensuring the health of its population.” 29 they may be tools used to address complex, high priority issues that cross sectors or silos such as health and social care (e.g., employment and social supports). They often detail consistent and balanced approaches for resource use for future sustainability 29 and are ideally co-created in a process that unifies stakeholder groups through shared goals and values, with agreed actions and outcomes. As informational and awareness raising resources, they specify what is known about an issue and ways in which the issue will be addressed, and what is hoped to be achieved. The WHO and United Nations Children’s Fund (UNICEF) recently released the Global Report on AT and has called on each country to develop some national policy for AT that may be a part of other sector policies and action plans and to include sufficient budgetary allocations such that people have AT access without financial burdens. 30 The report’s first of 10 recommendations is to “improve access to AT within all key development sectors,” particularly in health, education, labour, and social care. 30
What might a Canadian strategy look like?
A strategy will provide a roadmap for implementing a policy vision for AT access that can systematically address challenges impacting equity of access by Canadians. Further, since AT use can facilitate service access, a strategy can mitigate some of the systemic problems in service and information access by people with disabilities (and intersecting characteristics, such as age or poverty that can compound and restrict access) that were exposed throughout the pandemic. Canada has developed several multi-sectoral strategies, including the 2030 Agenda National Strategy (2019),
31
Dementia Strategy (2019),
32
National Housing Strategy (2018),
33
and Mental Health Strategy (2012).
34
Through extensive research involving citizens, policy-makers, and other stakeholders and applying various methodologies (Table 1), we have comprehensively analyzed the situation, identified principles to underpin policy actions, defined short- and long-term priorities, and discussed implementation considerations and opportunities. In a final stakeholder dialogue, participants stressed that focusing on two to three top priority issues with achievable goals is necessary to develop a manageable and impactful vision.
35
Participants agreed on the need to develop a national strategy, foster leadership nationally, and convene a cross-jurisdiction coalition for best practices identification and development of supports. Results (Figure 2) may serve as a blueprint from which to build such a strategy and to catalyze discussions on each of the elements outlined, implementation considerations, and elucidation of action plans. Action plans will ultimately describe the specific groups to be involved, activities to be executed, and timelines for actions.
9
Elements of a blueprint for a national strategy for enhancing equitable access to assistive technology in Canada.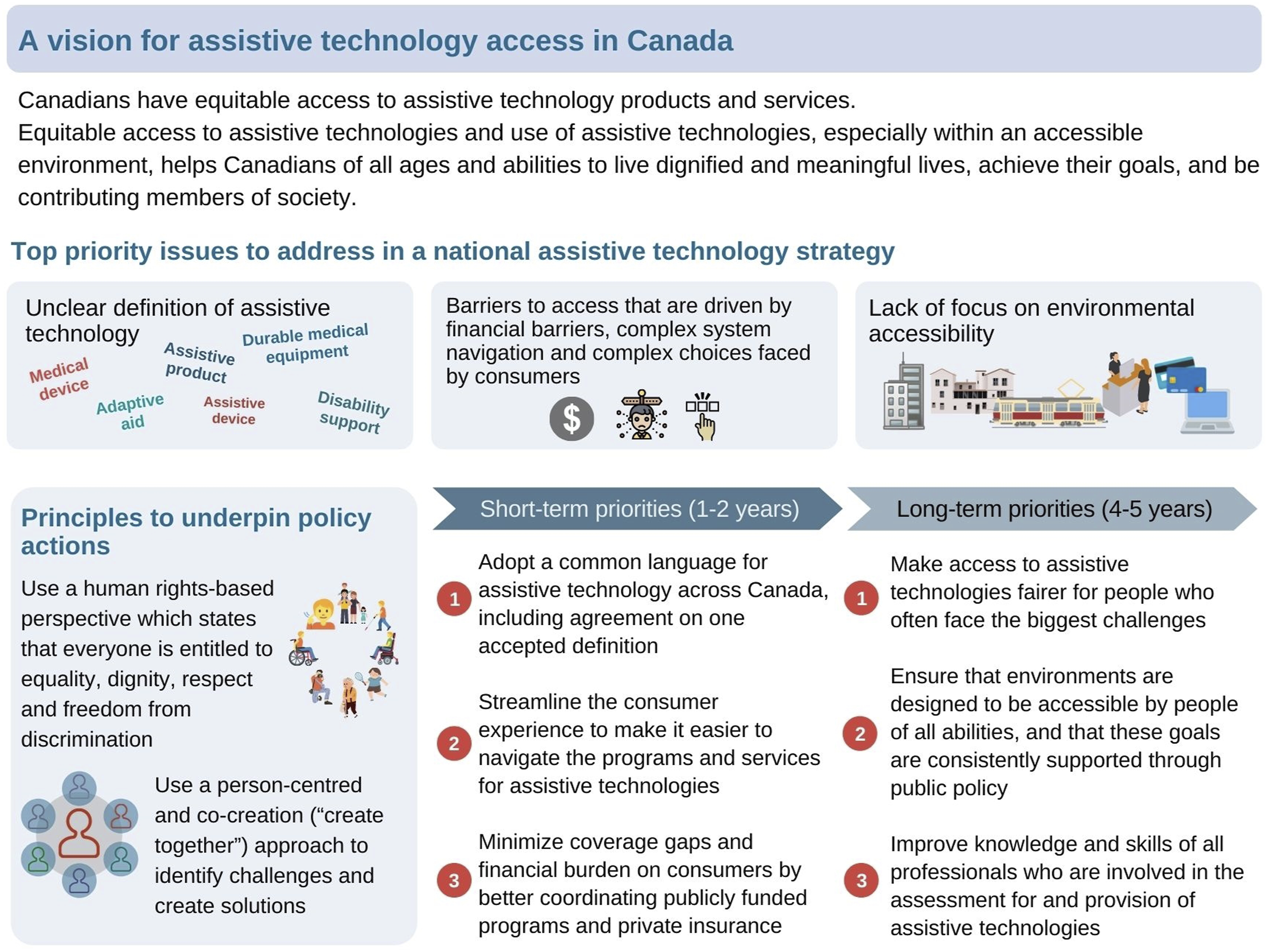
There were many implementation considerations discussed in the dialogue. 35 The decentralized and siloed Canadian governance system was mentioned often as needing change so that government levels/sectors may work better together. National leadership was urged in addition to multi-level/-sectoral actions, particularly to ensure progress on the priority issue of environmental accessibility. National leadership was also recommended for AT access, specifically for the priority issue of defining AT (also short-term priority 1) and outlining consistent criteria for coverage eligibility. For the priority on access barriers (also short-term priority 3), it was clear that removing financial barriers, particularly for those with challenges paying out-of-pocket, could enhance equitable access. Suggestions were made for federal government interventions to increase resources to pay for AT, while supporting choices. Needs-based funding was suggested as a possible approach to ensure the range of programs and citizens’ needs cover and are covered in the care continuum.
Forums and opportunities for governmental discussions on a national vision on enhancing equitable AT access were suggested in the stakeholder dialogue. 35 Proposed forums were the Federal, Provincial/Territorial Ministers Responsible for Seniors Forum and Federal, Provincial/Territorial Meeting of the Ministers Responsible for Human Rights. Discussions on implementing the Accessible Canada Act 36 and drafting of regulations were identified as opportunities to offer input on the necessary interfacing of AT access and environmental barrier removal. While parallels were drawn between creation of national pharmacare and AT programs, participants advised on important differences between drug formularies and AT product lists eligible for coverage (e.g., AT products require extensive resources for delivery, customization, and follow-up). Further, budgets for drugs are expected to be larger than for AT products because more people are prescribed drugs compared to AT.
It is hoped that a blueprint will spark discussions on how an AT strategy will accelerate achievement of established collective goals of Canadians. An AT strategy may facilitate compliance with existing legislation (e.g., Accessible Canada Act, provincial accessibility legislation) or enable outcomes of other policy initiatives to be realized (e.g., 2030 Agenda National Strategy, Dementia Strategy, pandemic response) for full inclusion of people with disabilities and older people by mitigating challenges in access to healthcare and services, quality education, meaningful employment, and home and food security. Finally, the Quadruple Aim framework has been endorsed in health services in many Canadian jurisdictions with the goal of attaining the best possible performance within health systems.37-39 Implementation of a strategy that enhances equitable AT access may fulfil the four inter-related aims with improvements in user experiences and unmet needs, health and well-being of citizens, and healthcare provider work satisfaction, and decreases in health and social services costs.
Next steps
Champions are needed to lead next steps and to convene a national coalition that includes invested citizens, policy-makers, and stakeholders, as previously involved in our research. The coalition, ideally driven by citizens, may develop the blueprint into a strategy by defining working processes that include the identified principles and iteratively defining action plans with specific activities and timelines to address the top priority issues and short- and long-term priorities. Capturing the attention of those in positions to lead change and enact a strategy requires advocacy and positioning priorities and outcomes for equitable AT access with contemporary policy initiatives.
Health leaders have important roles to play in the success of the next steps. Health leaders may advocate within their positions and champion change in their jurisdictions, particularly to support policies and practices that enhance environmental accessibility in conjunction with equitable AT access. They may champion citizens interested in leading or participating in the coalition and be active participants themselves. They may provide expert guidance and knowledge on health and social systems, concerns and solutions in their jurisdictions, and policy and practice evidence. Health leaders may lead coalition activities to define the common language for AT and facilitate consistency in program eligibility criteria nationally. They may partner with academics in integrated knowledge translation research to develop evidence and apply evidence-based frameworks to further define health, well-being, social, and economic outcomes of AT product and service use at individual, community, provincial/territorial, and national levels, and translate this evidence to support decision-making.
Footnotes
Acknowledgements
We wish to thank the citizens, representatives from the advocacy, caregiver, professional, and care provider organizations, industry members, policy-makers, and academics who participated in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Ageing Gracefully across Environments using Technology to Support Wellness, Engagement and Long Life Network of Centres of Excellence (AGE-WELL NCE Inc.) [grant number AW CRP 2015-WP8.2].
Ethical approval
Institutional Review Board approval was not required.