
Abstract
The COVID-19 pandemic particularly affected social connection through enforced social isolation and loss of regular activities. For healthcare systems, various initiatives have sprung up, leveraging existing technologies to connect people with services, activities, and loved ones. Here we review some AgeTech offerings to address social isolation for healthcare leadership and management to consider.
Introduction
Understanding the difference between social isolation and loneliness
The pandemic could have reasonably been expected to increase the incidence of social isolation and loneliness among older people, given the risk factors they faced before the pandemic. In everyday life and the research literature, social isolation is often conflated with or seen as interchangeable with loneliness. 1 However, loneliness and social isolation are distinct entities 2 and our understanding of each will shape thinking about how to address them in services.
An estimated 30% of older Canadians are socially isolated or at risk of becoming so. 3 Social isolation is often considered to be an objective condition that can be measured.1,4 Specifically, it is argued that the number of contacts a person has can be counted and quantified, with those individuals who have a limited number of social contacts being classified as socially isolated. Greater social isolation is experienced by the oldest (above 80 years). 5 As the proportion of older adults in Canada is predicted to grow from 15% of the population in 2013 to 23-25% by 2036, the need for solutions to address the risk and the experience of social isolation in later life is clear.
Social isolation is linked to poorer health and reduced quality of life and presents a growing challenge not only in Canada but across the world. In terms of targeting individuals most at risk of social isolation, a plethora of indicators has been previously reported in the literature. 5 These include living alone, being unmarried, having a small social network, infrequent contact with network members, lack of social network diversity, low participation in social activities, emotionally distant relationships and feelings of loneliness, and lack of connection. In the Canadian context, increased risk of social isolation has been identified among specific groups of older adults, namely, individuals who are First Nations, Inuit, and Métis (FNIM), caregivers, immigrants, or newcomers to Canada, 2SLGBTQ+, living alone, living in rural or remote areas, on a low income, disabled, or living with dementia.3,5
Being socially isolated does not necessarily lead to loneliness and being lonely is not always the result of being alone and/or isolated. 4 Loneliness occurs across the lifespan and has been linked to poorer mental health at all ages, particularly depression and anxiety.6,7 The UK Campaign to End Loneliness proposed that “loneliness happens when the social connections that people want, don’t match their actual experience of relationships with others.” 8 An extensive review of literature from 1945 to 2018, further differentiated loneliness into three subtypes: “Social Loneliness,” “Emotional Loneliness,” and “Existential Loneliness.” 9 The review authors report that all three types of loneliness have been identified in work with older adults, 9 which is important for developing and offering appropriate health interventions and services to match their needs. For example, addressing loneliness related to bereavement (Emotional Loneliness) vs. terminal illness (Existential Loneliness).
Based on reports before the COVID-19 pandemic, around 6% of the UK population reported often or always feeling lonely. 10 A comparable analysis of baseline data from the Canadian Longitudinal Study of Ageing (CLSA) linked to the 2016 census data found the prevalence of loneliness to be slightly higher at 10.2% with social isolation reported by 5.1%. 11 The authors concluded that personal characteristics (such as age, income, and chronic disease) were the biggest contributors to loneliness, whereas geographical factors, such as clustering of low income older adults, were associated with increased risk of social isolation. 11
These data provide a baseline against which to compare the impact of the COVID-19 pandemic. Vulnerable groups of older adults did face an increased risk of loneliness due to social isolation. For example, a survey of 701 adults over 50 years old living with chronic health conditions in the United States, conducted in the early months of the first lockdown, found that 66% reported feeling somewhat or always lonely. 12 Other groups disproportionately affected by the pandemic include older adults living with dementia and family carers, who are often spouses. Two UK studies conducted in August 2020 found that the sudden removal of social support at the start of the pandemic negatively affected people living with dementia and family carers, 13 and reduced hours of social service support significantly predicted anxiety among older adults with and without dementia. 14 A Canadian interview study with 10 people living with dementia found they were worried about contracting COVID-19 as well as losing contact through program closure, plus concern for the well-being of people newly diagnosed with dementia or living alone. 15
However, two Canadian surveys conducted early in the first lockdown in 2020 found lower levels of loneliness among older adults than younger ones. In their survey of 3,012 English-speaking Canadian adults (over 18 years of age), conducted between May 8 and June 23, 2020, Wickens and colleagues found greater odds of loneliness among all groups under 60 years of age, compared to those over 60 (5.5%) with the highest odds in the 18-29 years age group (13.8% 16 ). Similarly, a survey of 4,879 members of a national retired educators’ organization found that increasing age reduced the risk of loneliness, with those over 65 years of age reporting less loneliness than those under 65 years old. In both surveys, just over 8% of respondents reported feeling lonely most or all of the time.16,17
While these data suggest that older adults fared better than younger age groups during lockdown, as highlighted, social isolation and loneliness were already a feature of many older people’s lives before the pandemic and lockdown was a continuation of their “normal.” 18 Among the many effects of the COVID-19 pandemic, however, has been raising awareness and concerns about the issues 19 due to the global use of quarantine and physical isolation as tools for managing the spread of the pandemic. 6 This has created increased opportunities to help tackle social isolation for older people by increasingly utilizing digital technologies to connect with them.
Role of technology
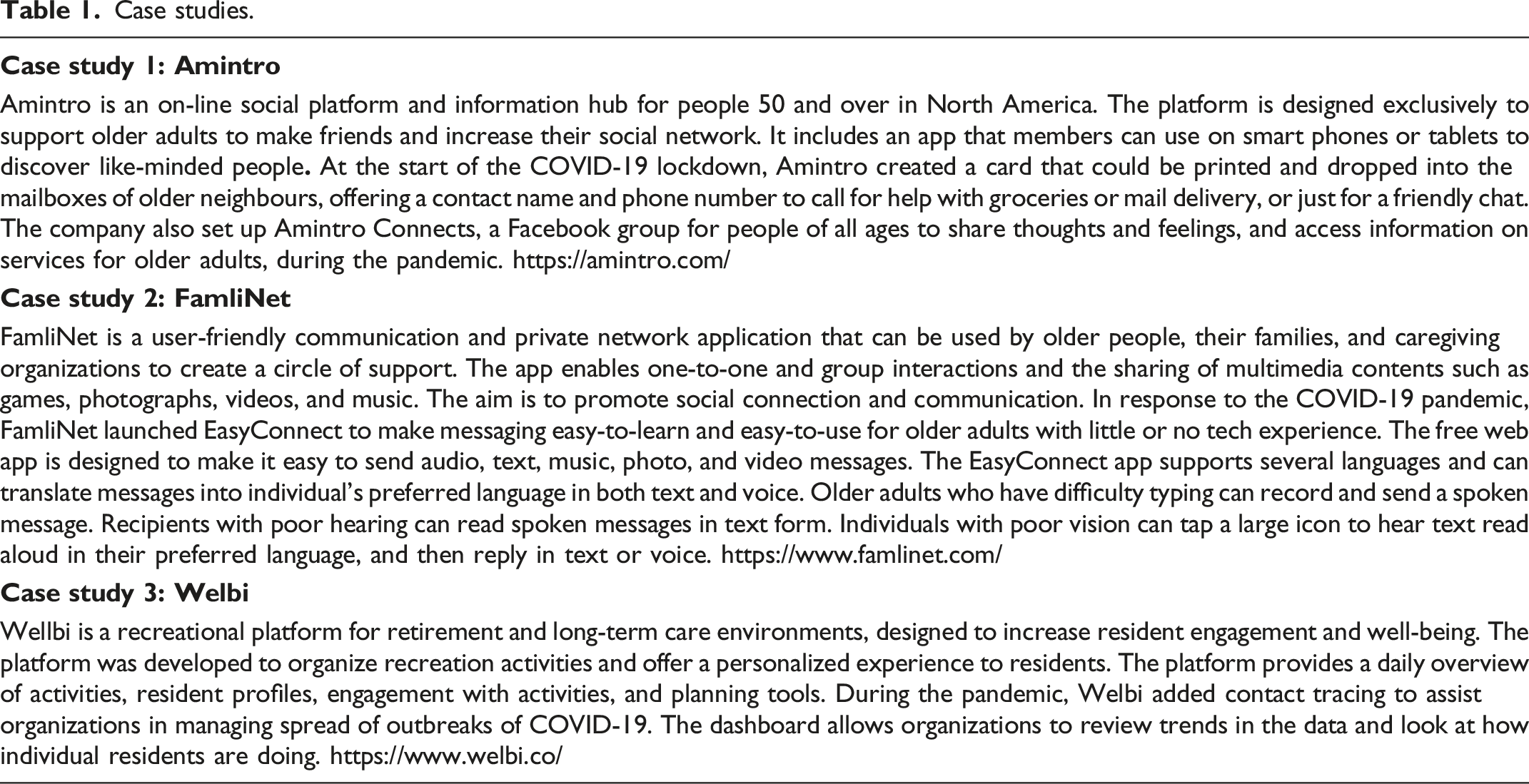
Case studies.
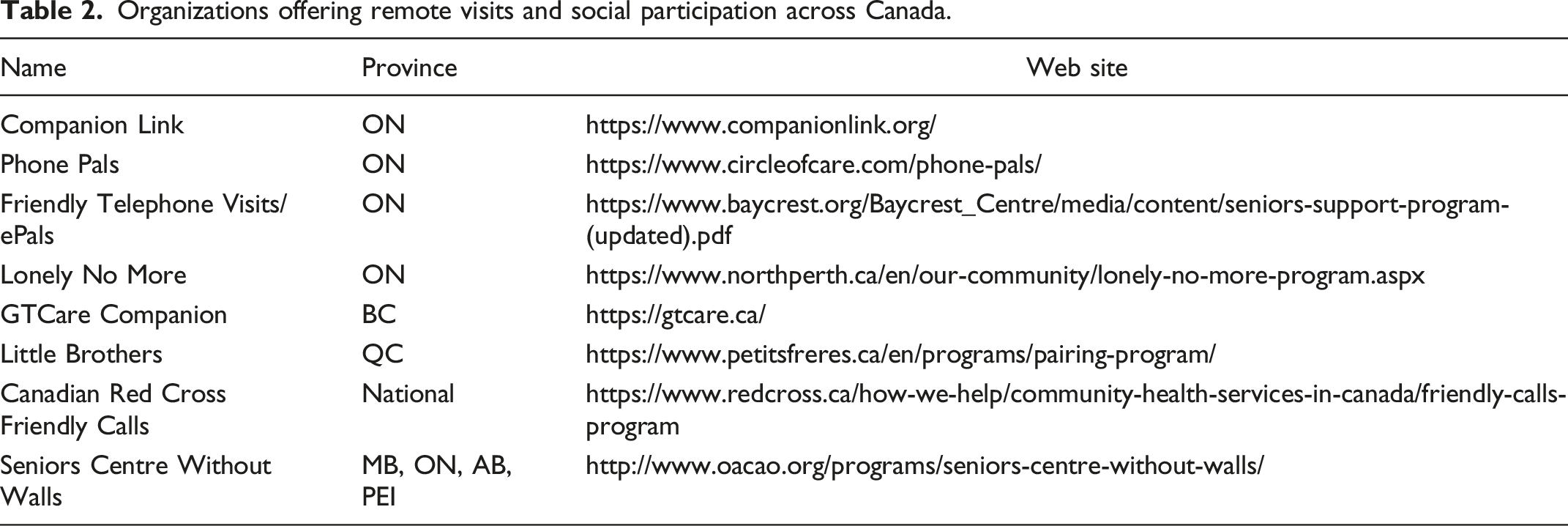
Organizations offering remote visits and social participation across Canada.
Key lessons for health leaders
While the COVID-19 pandemic has accelerated the introduction of digital technologies into all realms of people's lives with positive impacts as more older people are using internet-connected services, 24 the pandemic can also be seen to have cemented or even widened the digital divide. 25 While services and communities attempted to bridge the gap, individuals in vulnerable groups, through low socio-economic and/or health reasons, continued to be excluded. Persistent problems with digital access, digital literacy, and digital skills were observed among people marginalized before the pandemic. 25 While it is clear that existing smart devices contain multiple functions such as telephone and video calling, texting, calendars, reminders, 26 and plus apps to support leisure and cognitive engagement 27 could benefit older people, this raises the question of who could or should provide them?
While it can be argued that the internet is an essential service such as water and electricity, these are not provided by governments. People on fixed incomes such as state pensions will continue to decide between heating and food, and access to the internet will continue to be a luxury. Another challenge in the Canadian context is geography with rural and remote areas much more poorly served than urban ones. The Broadband Fund launched by the Canadian Radio-television and Telecommunications Commission 28 is intended to address the digital access problem through improved provision of broadband and mobile internet access. While this can start to address the internet availability challenge, device availability, as described above, also needs to be addressed. Accordingly, the introduction of digital technologies to services requires careful consideration if aimed at those who lack access to the internet or digital devices.
Similarly, training and support for digital novices must be factored into tackling the digital divide. Pre-pandemic research highlighted gaps in knowledge and also confidence in starting to use digital technologies. 29 This included requiring support to access and select devices, as well as getting started and maintaining them. Given the pandemic-created necessity to be on-line, service providers should consider not only providing internet access and devices but also digitally confident staff to set them up for successful technology use.
When implementing digital technologies that address social isolation, engaging with all stakeholders to consider these issues is an essential step as those who experience social isolation will have limited social networks It is particularly important to bring together stakeholders that do not normally interact, such as product developers and older adults, or when there are power differentials, such as care staff speaking to service directors. 30 Co-production—where end-users work together with service providers to innovate new services—is increasingly being adopted in healthcare systems. The New Economics Foundation 31 proposed five principles for successful co-production: (1) building and maintaining relationships, (2) reciprocity, (3) sharing of power, (4) including all perspectives and skills, and (5) respecting and valuing the knowledge of all.
Health leaders who consider implementing digital technologies and services to tackle social isolation should carefully design co-production sessions and use activities to create a safe environment where everyone’s voice is heard. AGE-WELL has supported the development of TUNGSTEN tools, a set of interactive activities to foster co-production. TUNGSTEN tools have been used to explore the role of technology in late-life mental health, 32 co-production of a self-management app for people newly diagnosed with dementia, 33 agile development of an on-line memory intervention program for healthy older adults, 34 and a framework for evaluating technology to manage chronic pain. 35 These freely available tools plus case studies and guidance for organizing co-production sessions and workshops can be found on the TUNGSTEN website: http://tungsten-training.com.
The increased use of digital technologies is likely to remain after the pandemic. Post-COVID will see the necessity to continue to access services such as healthcare on-line as they remain remotely delivered potentially leading to more rather than less social isolation. As noted above, a focus on social isolation prevention and building protective factors using digital technologies is important along with tackling wider structural issues like technological disadvantages to increase digital participation. Digital technologies are one solution to tackle social isolation that has gained more attention and intensity as a result of the pandemic;36-39 however, it is doubtful that one method alone will tackle social isolation. Some have also suggested that despite the benefits of using digital technology and the emerging evidence it can help with social isolation, using it should not be at the expense of face-to-face contact as their use will not create meaningful contact for everyone.37,40
Utilizing digital technologies will not meet everyone’s need for social connectedness. A personalized framework for thinking about how digital technology can mitigate social isolation and loneliness is therefore required. 41 An individual’s journey into social isolation entails multiple factors and it is not easy to identify or differentiate one particular cause. 2 Research into the effectiveness of strategies and interventions to deal with social isolation, including digital technologies, is still in the early stages and it is not clear what the long-term impact of services moving on-line will have on social isolation compared to other times.2,42 Health leaders, therefore, need to remain proactive in contacting people in “traditional” ways to offer “digital support” as services change on-line to avoid greater isolation. Such interventions may wish to focus on specific groups who are more at risk of isolation and on protective factors such as good physical and mental health, good income/housing, safe neighbourhoods, communication and literacy skills, good support networks, and access to transport.