
Abstract
Supportive smart home technology, for older adults living with dementia and their informal care partners, has shown some benefits in private homes. In this study, a supportive smart home system is being implemented in a hospital alternative level of care setting. This case report describes how a team of researchers and healthcare managers are navigating the complexities of a hospital setting, using human-centred design and implementation strategies, to facilitate the implementation and adoption of the technology.
Introduction
As the world’s population ages, increasing changes in mobility, cognition, medical complexity, and activities of daily living present varying challenges. Older Canadians, like their peers around the world, would prefer to “age in place,” but their needs often exceed existing human and financial resource capacities. Most jurisdictions have long waiting lists for home care services and institutional spaces. These have been amplified by COVID-19 and will be impacted further as Boomers age. 1 Because of this, researchers worldwide, including those part of the AGE-WELL Network of Centres of Excellence in Canada, see a potential role for smart supportive technology specifically designed to facilitate ageing in place (AgeTech). The AGE-WELL National Innovation Hub on Sensors and Analytics for Monitoring Mobility and Memory (SAM3) was created in Ottawa, Canada, in 2017 to advance AgeTech developments for mobility and cognitive declines.
A considerable number of older persons live with dementia and thus require additional assistance to age in place. Self-care and safety are often affected, and one of the recurring issues is nighttime exploring (formerly referred to as wandering)—which can lead to tragic consequences. One risk associated with exploring is weather exposure, with both high and low temperatures increasing risk. Other risks include traffic and the built environment which can lead to falls and injury. Significantly, the worries around People Living with a Disability (PLWD) exploring cause significant burden to care partners. A number of research teams have worked on solutions to address this.2-5 Similarly, the SAM3 team helped develop an off-the-shelf smart supportive nighttime wandering detection and diversion system.6-7 This “DementiaTech” system provides visual and auditory cues to the PLWD to direct them back to bed. At the same time, the care partner can sleep knowing the system will “keep an eye on the PLWD,” and only wake them when a door to the exterior is opened. This DementiaTech was tested in 18 homes in the Ottawa region and the overall response by care dyads showed that the system was perceived as helpful, with many participants asking if they could keep it after the research project ended. 7
However, PLWD can be admitted to hospital for an acute illness or if the care needs exceed what is able to be provided at home. Given the afore-mentioned resource challenges, many of these individuals wait long periods of time before they are discharged from acute care into long-term care, or back into the community with the needed additional care. Many acute care facilities co-locate these “Alternate Level of Care” (ALC) patients on special units within the hospital to provide better and more efficient care. Recently, in Ontario, some cities are using custom-built transitional care facilities as a temporary solution to the ALC challenge. Because a large proportion of the patients in ALC are PLWD, these facilities face similar challenges regarding nighttime exploring and associated risks (eg, falls and entering the wrong room).
The objective of this research project was to trial the implementation of a DementiaTech product in a transitional care environment. Notably, healthcare Information Technology (IT) projects are challenged by a risk of unrealistic expectations of technology, lack of commitment from end users, and a resistance to change. Therefore, it is important to engage and involve end users early in the IT project lifecycle in order to support its success 8 and ensure its patient-centredness. 9 Knapp et al. describe a six-step implementation science model: Assessment, Deliverables, Activate, Pre-training, and Sustainability, that was used to guide this project. 10
This paper will describe the first three steps of Knapp’s model of implementation of DementiaTech into a sub-acute hospital transitional care unit using a staff-centred design model. The hope is that this case report will help health leaders consider some of the challenges of new tech implementation in their institutions.
Methods
The site
Greystone Village Retirement Home is a newly constructed, multi-storey building in a new subdivision. Before construction was finalized, the owners were approached about the possibility of implementing a physical redesign that would allow its conversion to a Transitional Care Unit (TCU). The building would be leased, and the conversion would be funded by the Ontario Ministry of Health and Long-Term Care. Since retirement homes do not typically have “nursing stations” on most floors, a subset of resident rooms was converted into charting/staff rooms, facilitating the potential future return to retirement home living. After conversion, a total of 120 beds were available for transitional care. Initial plans included a 25-bed closed dementia TCU on the fifth floor, with the option to create a second one. The shape of the building, an angled “T,” provided optimal viewing of the near-by river. However, it also created specific sight line challenges for clinical staff. The site has pre-existing bed alarm technology, which notifies staff on a pager-like system when patients at risk get out of bed.
The healthcare team
Bruyère Continuing Care, an Ottawa sub-acute care provider with over 1,100 sub-acute, Long-Term Care (LTC), and supportive housing beds, provides physician in-patient services and operations oversight. Bayshore Healthcare, a national home care provider, supplies on-site operational management, care, and services, consisting of all nursing, allied healthcare and support services. Staffing on each of five floors consists of a day shift: two Registered Practical Nurses (RPNs) and five Personal Support Workers (PSWs), and night shift: two RPNs and three PSWs. In addition, three physiotherapists (2.4 FTE), two occupational therapists (2.0 FTE), and 10 rehabilitation assistants provide care to all patients in the building. There are six managers on site during the day and one each on evening- and nightshifts. This staffing ratio reflects current practice in this sector.
The patients
Admission of patients to Greystone began in November 2020. The majority of patients are admitted from The Ottawa Hospital and other acute care hospitals in Ottawa. There are some direct from home admissions for patients in crisis. Ninety-six percent of patients admitted to Greystone are over 65 years old, with an average age of 81.5 and just under 60% being female. The average length of stay is 75 days, with half of discharges going to long-term care. Patients discharged from the fifth floor were 82.3 years old, 44.7% were female, and after 90.4 days just over 2/3 were discharged to long-term care.
The research team
The core of the research team was from the SAM3. The group consists of clinician-researchers from University of Ottawa’s Faculty of Medicine (Family Medicine, Neurology), Health Sciences & Rehabilitation, engineering researchers from Carleton University’s Systems and Computer Engineering, industrial design and human factors researchers from the School of Industrial Design at Carleton University, and a healthcare management researcher from the Telfer School of Business at the University of Ottawa. A local start-up in smart supportive monitoring technology, Esprit-ai, was selected based on their system’s flexibility, early experience in a retirement home, and previous collaboration with SAM3.
The project
The research objectives for this project focused on its implementation of DementiaTech in an institutional setting. This would require adaptation of both the actual technology and the implementation strategy. Rather than one system per home, the DementiaTech would now serve multiple PLWD, all within close proximity. The living quarters were changing from private homes/apartments to TCUs. The latter have smaller private living areas, no private kitchens or living rooms, and instead share common areas. In turn, this required adaptation in product design and functionality, as well as the approach to implementation and use. New implementation strategies needed to consider multiple stakeholders: patients, on-site formal caregivers, off-site informal caregivers, the research team, the management teams of the healthcare providers, the owners of the building, and the technology provider.
Funding and ethics applications
The core team of researchers, healthcare managers, and building owners gathered in mid-2020. A high-level work plan was prepared, and a funding application was submitted in October 2020. Funding was approved in March 2021. Bruyère Research Ethics approval was obtained on July 26, 2021.
Steering committee and workplan
A steering committee was formed, consisting of the initial team, a research coordinator, and a research assistant. The role of the building owners was assumed by the healthcare administrators. Over the first few months, a detailed project plan was devised and approved. A human-centred design approach was chosen independent of the choice of technology solution. 11 The solution for each patient would be custom-designed based on this approach. Frontline staff would therefore be included in all aspects of the project plan, to provide insight and feedback on challenges with their workflow, technology design, and project evaluation. Given that this project was implemented during the COVID-19 pandemic, access to the site was restricted, creating some delays vs. the original timelines.
Kick-off meeting with staff
The first step was to introduce frontline staff to the project. A small group, which included the primary investigator, a research assistant with an engineering background, as well as the co-investigator from industrial design met with the unit staff: RPNs and PSWs. Two days were selected to allow contact with the largest possible group of staff representing the main two shifts providing care on the unit. A mid-afternoon meeting was chosen to minimize impact on bedside care. The intent of the project was introduced: to explore the potential of adding technology to the unit to help with nighttime care. After showing the staff some sample sensors that could be integrated into rooms, they were asked to reflect on the types of clinical situations where technology might help. Initial reflections included residents at risk of falls and residents that explored at night. The potential installation of speakers into rooms led to a discussion on caring for residents whose first official language was neither English nor French.
Workflow mapping
Before considering changes to nighttime staff workflow, a team member and her student documented baseline workflow. Analyses included in-person shadowing of staff on the unit, while care was being provided. This allowed for opportunities to observe natural and regular staffing behaviours and discussions, insights which were further enhanced as staff were encouraged to “talk out loud” about the challenges they experience. These naturalistic observation sessions, which totalled 24 hours, were instrumental in identifying the design requirements for the development of the DementiaTech concept and prototype.
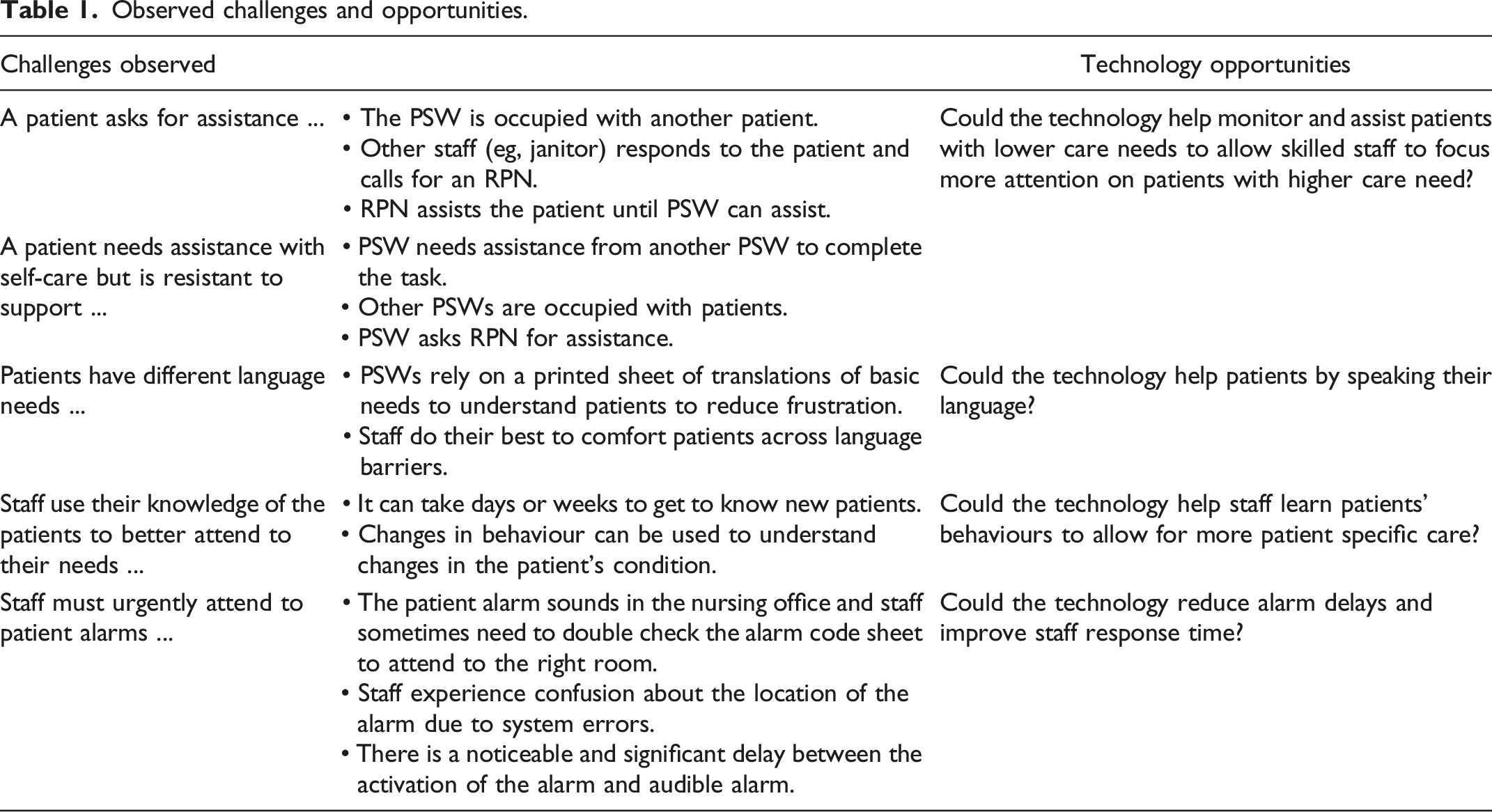
The night shift was divided into three, four-hour blocks. To maximize the chances of being exposed to different types of care situations, the RA scheduled two visits for each time block. Over six nights in August and September 2021, the RA was able to observe the care provided to 16 patients and interact with six RPNs and 10 PSWs. The activities that were documented were then categorized deductively using the AEIOU framework (Activities, Environment, Interactions, Objectives, and Users) to identify what aspects of the context were challenging for staff, design requirements and opportunities for design intervention. 12
Observed challenges and opportunities.
Staff feedback and ideas for technology implementation
Greystone brainstorming: Technology and patients’ behaviour.
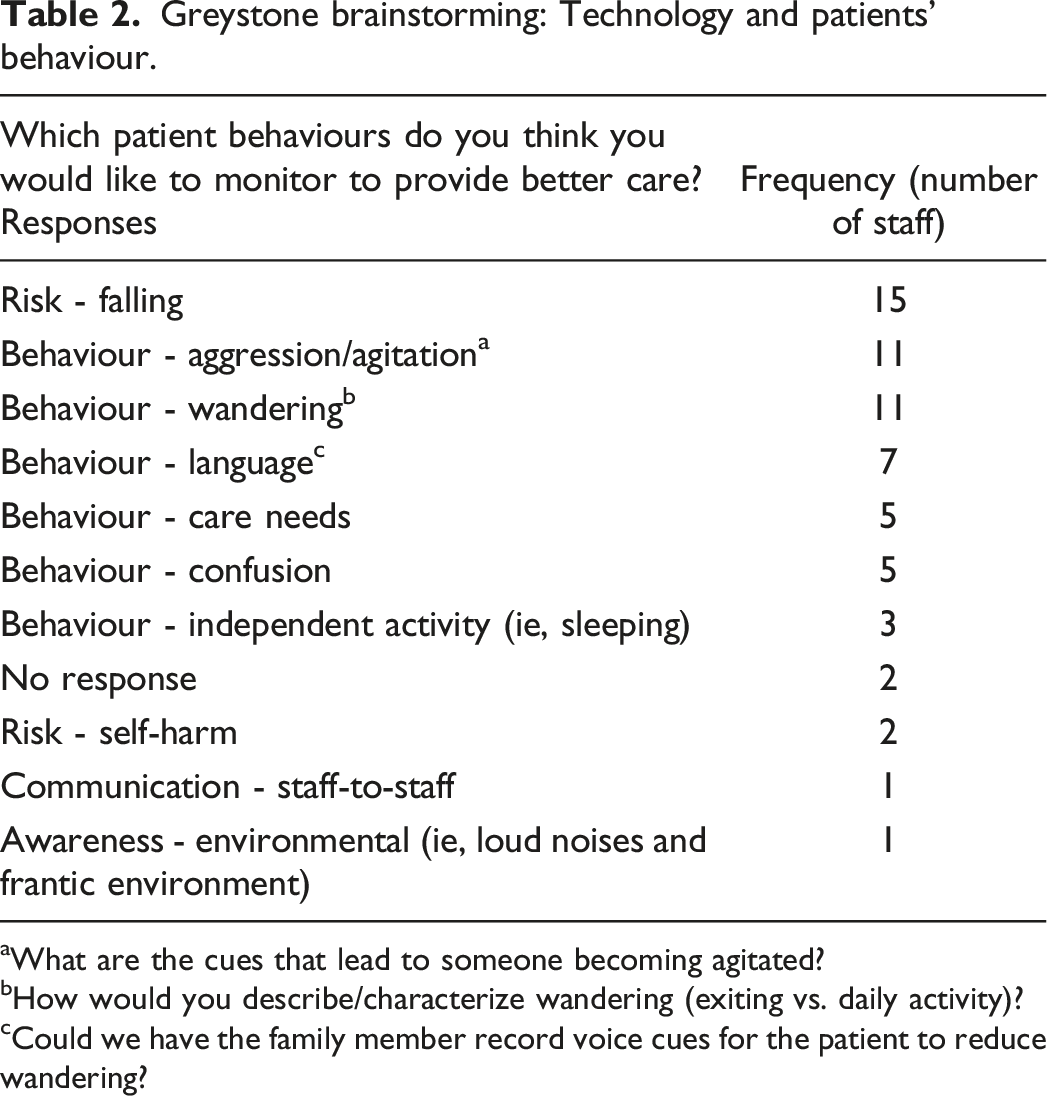
aWhat are the cues that lead to someone becoming agitated?
bHow would you describe/characterize wandering (exiting vs. daily activity)?
cCould we have the family member record voice cues for the patient to reduce wandering?
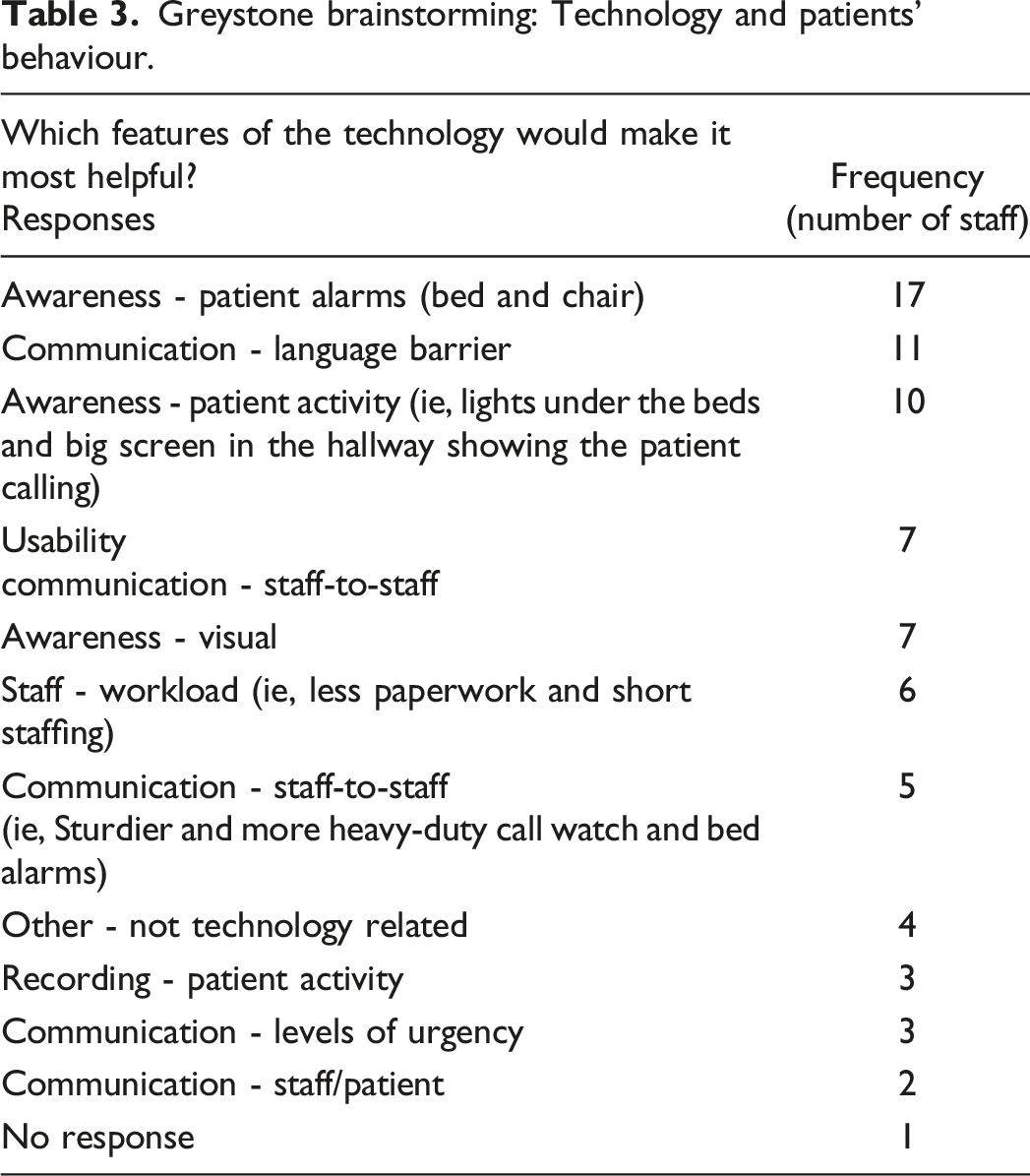
Greystone brainstorming: Technology and patients’ behaviour.
The workflow model was developed over several weeks and was validated by staff and reviewed by the steering committee.
Technology concept and piloting a prototype
A concept and pilot prototype which combines a variety of in room sensors, including detecting the patient’s presence in the bed and motion sensors in the room, would provide better monitoring of nighttime wandering/exploring and falls. It was important to have an application that would allow for staff notification. However, given that the nurses already had a portable notification device, alternative ways of notification were considered, for instance, a light in the hall or a message board in the documentation room.
Installing the technology prototype and baseline questionnaire
Informed consent was obtained to install the first pilot system into a patient’s room. The patient was English-speaking, and at risk of wandering/exploring at night. In-room installations included a bed sensor to monitor bed exit, a motion sensor in the room, and two door sensors on the closet—as the patient did enter the closet occasionally. The preliminary objectives for the technology were to notify staff when the patient got up from bed and again if that person opened the closet. Our usual approach is to monitor sensor outputs for a couple of weeks to ensure they are working properly. During this pilot period, a few issues needed addressing, including re-installing the bed sensor and reattaching a wall mounted sensor, both of which had likely been removed by the patient.
Next steps
Once the first pilot room is operational, additional patients will be recruited and the technology will be installed in their rooms. The plan is to recruit 10 patients and collect data for two months. Implementation will continue using this design methodology and will have to consider the changing healthcare environment, as well as privacy issues. The customization of the system for each new resident will be paramount, for instance, providing cuing to them in the language of their choice. Some of the technical issues to monitor will be on how information from multiple rooms is managed on the phone app and ensuring the ideal number of alarms is provided to avoid alarm fatigue. Similarly, comparing the new technology to the existing bed-alarm system will be important to determine if a replacement or integration strategy will be most helpful.
After the usual quality improvement cycling, there will be a more extensive evaluation at the end of the project. Did the technology work? Did the sensors connect to the hubs? Did the data go to storage and was the correct message transmitted to nurses? Next, did nursing staff get the specific information they wanted for each patient in a timely manner, and do they feel that this has a positive impact on care?
To formally evaluate the impact of the technology on care, a pre-implementation questionnaire was prepared to evaluate staff’s perceptions of the proposed intervention. This was done by adapting the Unified Theory of Acceptance and Use of Technology13‐15 framework.
In the final phase of this project, the industrial design team will prepare a user interface for informal caregivers to be able to “check-in” with their loved ones on the TCU.
Discussion
Implementation of new technology into a hospital setting is a complex endeavour. It requires collaboration by multiple partners from the hospital. In this project, a team of DementiaTech research experts was augmented by the addition of industrial design and healthcare management specialists. Hospital and healthcare provider management teams were included from the project onset. While this is not an official part of staff-centred design, it is essential in our current healthcare environment. In addition, to minimize the risk of implementation process challenges, end-users’ involvement was initiated early in the project lifecycle. The healthcare providers’ perspectives were assessed before the deployment of the technology, to make sure that it addresses the patients’ needs. The staff-centred design methodology was used, involving frontline staff in the design, through the pilot testing, and in the pre-pilot evaluation.
Conclusion
Our team believes that smart supportive technology has a role in the future care of older adults and can be implemented in complex environments, like hospitals. To ensure success, implementation design needs as much attention as technology design. We hope that this article encourages further reflection on health technology implementation by health leaders.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participation of staff and the patients, without whom this project would not have been possible. Julie Langton provided some of the demographic data for Greystone. Christine L. Laurin’s editorial support is also gratefully acknowledged.
Declaration of conflicting interests
F. Knoefel received shares in Esprit-ai for consulting work he did with the company three years ago. Esprit-ai did not have any influence on the content of this paper, except where P. Tan ensured that the technical information presented in this paper was correct.
Funding
The project received financial support from the Ontario Academic Health Science Centres Academic Funding Plan Innovation Fund and was supported by the Bruyère Academic Medical Organization. AGE-WELL NCE Inc. has provided financial support to AGE-WELL NIH SAM3. Frank Knoefel acknowledges funding for the University of Ottawa Brain and Mind – Bruyère Research Institute Chair in Primary Health Care Dementia Research.