
Abstract
We identify the core services included in a community hub model of care to improve the understanding of this model for health leaders, decision-makers in community-based organizations, and primary healthcare clinicians. We searched Medline, PubMed, CINAHL, Scopus, Web of Science, and Google from 2000 to 2020 to synthesize original research on community hubs. Eighteen sources were assessed for quality and narratively synthesized (n = 18). Our analysis found 4 streams related to the service delivery in a community hub model of care: (1) Chronic disease management; (2) mental health and addictions; (3) family and reproductive health; and (4) seniors. The specific services within these streams were dependent upon the needs of the community, as a community hub model of care responds and adapts to evolving needs. Our findings inform the work of health leaders tasked with implementing system-level transformations towards community-informed models of care.
Introduction
Community-informed models of care often provide integrated and coordinated services and supports that reflect the health goals of their community members. A community hub is a central place within a community where members can receive health and social care, education, and connect with others who have similar interests and goals for their health and well-being.1-3 Community hubs have been described in schools, corner stores, libraries, community centres, community health centres, and other central, easily accessible locations within a community.3-7 Community health centres are an example of a community-informed model of care;8,9 however, community health centres historically provide primary healthcare to underserved populations (eg, precariously housed, low-income, and refugees) within communities,10,11 whereas a community hub caters to all who live in the community. 12
A community hub model of care focuses on community connection and community-informed service delivery. 12 Community hubs co-locate and integrate health and social care within communities to maximize access to services and supports.1,2,13-15 Community hubs create economies of scale through housing health and social care services and organizations in a single, centrally located place within the community.2,13 Co-locating these services and providers for the community improves integration and continuity of care, which can enhance patient experience, satisfaction, and maximize the efficiency in how care is delivered, particularly for those in the community who have complex and intersecting needs. 16
A community-level model of care is not the dominant model for health and social care delivery in Canada and many other jurisdictions. 11 The value of community-level models are gaining renewed interest among health leaders and clinicians to support patients, their caregivers, and clinicians in improving their respective experiences in accessing and providing care, improving community and population health, and reducing healthcare expenditures.17,18 In Ontario, Canada, the implementation of the Connecting Care Act, 2019 aims to improve access to care; integration and coordination of services; patient experience; and use of resources. 19 The health system transformations attributed to this legislation in Ontario resemble a community hub model of care, but a clear definition of which services and supports are provided in such a model requires a more in-depth investigation. In this study, we identify the core services included in a community hub model of care to improve the understanding of this model for health leaders, decision-makers in community-based organizations, and primary healthcare clinicians.
Methods
We used a narrative synthesis approach to synthesize literature. This approach supports policymaking, the design of interventions, and is appropriate to conduct when the literature is diverse.20,21 The output of a narrative synthesis explores relationships and connections among and between the synthesized sources. 21 We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. 22
We searched Medline (via Ovid), PubMed, CINAHL (via EBSCOhost), Scopus, and Web of Science to retrieve peer-reviewed original research in the English language on community hubs during the 2000 to 2020 period on January 27, 2021. The lower bound of our search was set to the year 2000 because the early 2000s were when primary care reforms began. 23 There were no country restrictions in order to capture a range of community-informed models of care and community hubs in different jurisdictions. Titles, abstracts, and keywords that contained the term “community hub” were searched as a MeSH or subject heading term for community hubs does not exist in these databases. Google web searches were conducted using this term to obtain grey literature as grey literature may contain unpublished original research.
We applied the following criteria to screen sources and establish eligibility for inclusion in the narrative synthesis: (1) model of care was informed by those who lived in the community; (2) care was integrated with other services or supports in the community; (3) care was centrally located in the community or co-located with other care services; and (4) care and/or care services had a specific focus on the health of individuals and their communities. These inclusion criteria align with the description of a community-level model of care. We did not place any restrictions on the research methodology (ie, qualitative, quantitative, or mixed methods) or publication type (eg, conference proceeding, and journal article).
We applied the following criteria to exclude sources: (1) Organizational, technical, or management issues were addressed, explored, or described in a community-based organization or location (eg, strategic planning and investments and health informatics implementation); (2) focused on internet-based communities; (3) focused on the physical or biological sciences; and (4) non-research (ie, research not conducted with human participants and/or their data) and/or non-health focus publication. These exclusion criteria ensure only studies related to service delivery in a community-level model of care were included in the synthesis.
Two reviewers screened titles and abstracts of all sources for eligibility and assessed full-text articles for inclusion. In cases of disagreement, agreement was reached through discussion. Source screening was conducted using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia (Available at www.covidence.org). We extracted the country of origin, location of the community hub, populations served, and the care services offered from each source deemed eligible for inclusion.
Given the diversity of research designs eligible for inclusion, we used a diverse designs scoring tool to assess the quality of the literature. 24 This tool includes 16 quality dimensions for mixed studies (maximum score: 48) and 14 dimensions for quantitative and qualitative studies, respectively (maximum score: 42). We defined low quality sources as those with a score less than or equal to 25, moderate quality sources as those with a score between 26 and 32, and high quality sources as those with a score equal to or greater than 33. The core and optional services included in a community hub model of care were identified by thematically grouping the populations and care services served in such a model.
Results
There were 236 records identified through database searching, and 13 records were identified through Google web searches (n = 249). There were 170 duplicate records that were removed; after title, abstract, and full-text screening, 152 records were excluded, and 18 records were eligible for inclusion (n = 18) (Figure 1). These records were published between 2012 and 2020, and the records reflected community-level models of care in the following countries: United Kingdom (n = 7, 38.8%),2,16,25-29 United States (n = 4, 22.2%),4,5,30,31 South Africa (n = 3, 16.6%),32-34 Canada (n = 2, 11.1%),35,36 Australia (n = 1, 5.5%),
37
and Peru (n = 1, 5.5%)
38
(Table 1). Through our quality appraisal, we found 4 studies that were low quality (n = 4, 22.2%),25,26,31,37 5 studies that were moderate quality (n = 5, 27.7%),2,4,30,33,35 and 9 studies that were high quality (n = 9, 50%).5,16,27-29,32,34,36,38 Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram. Data extraction from synthesized studies (n = 18).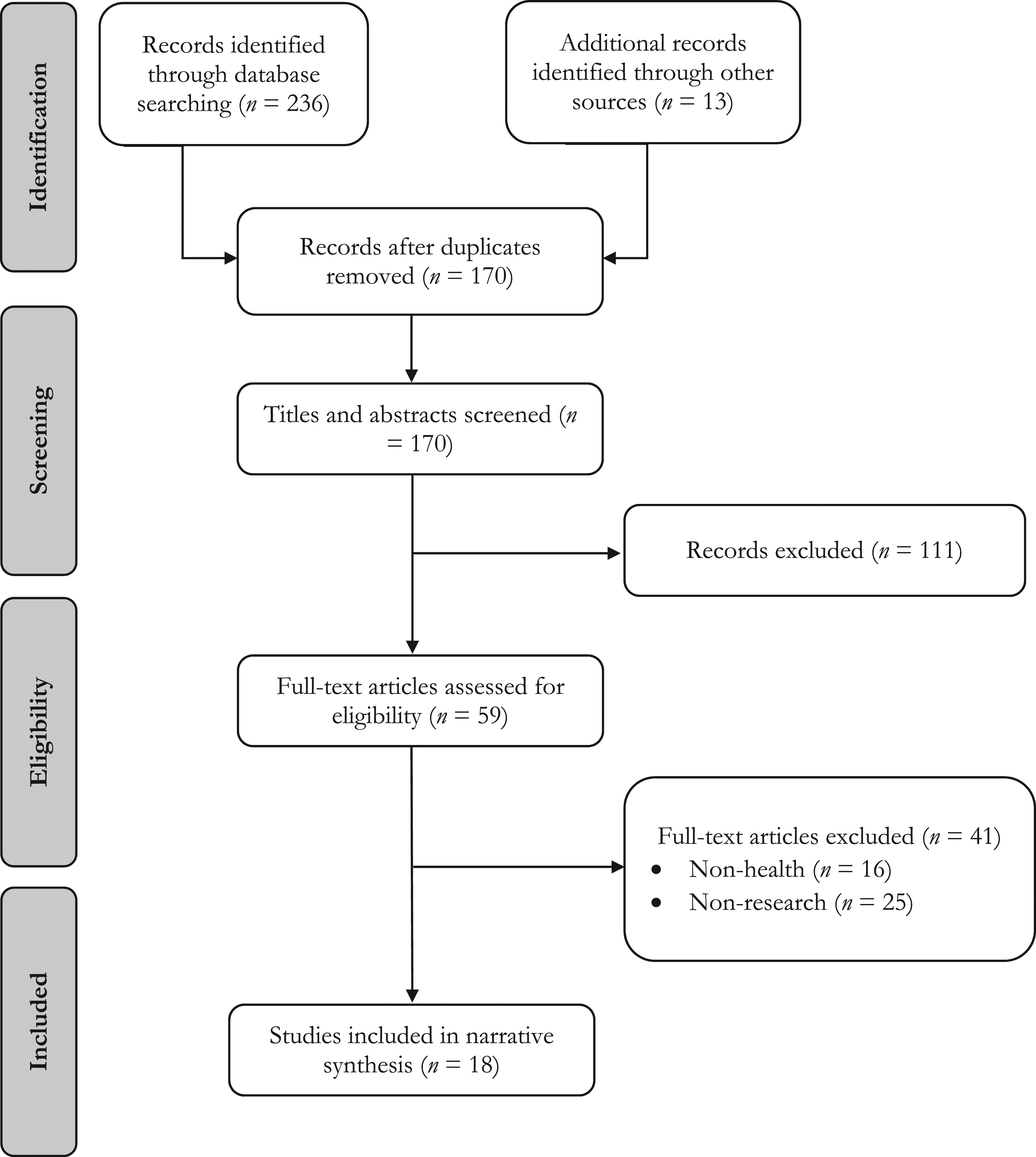
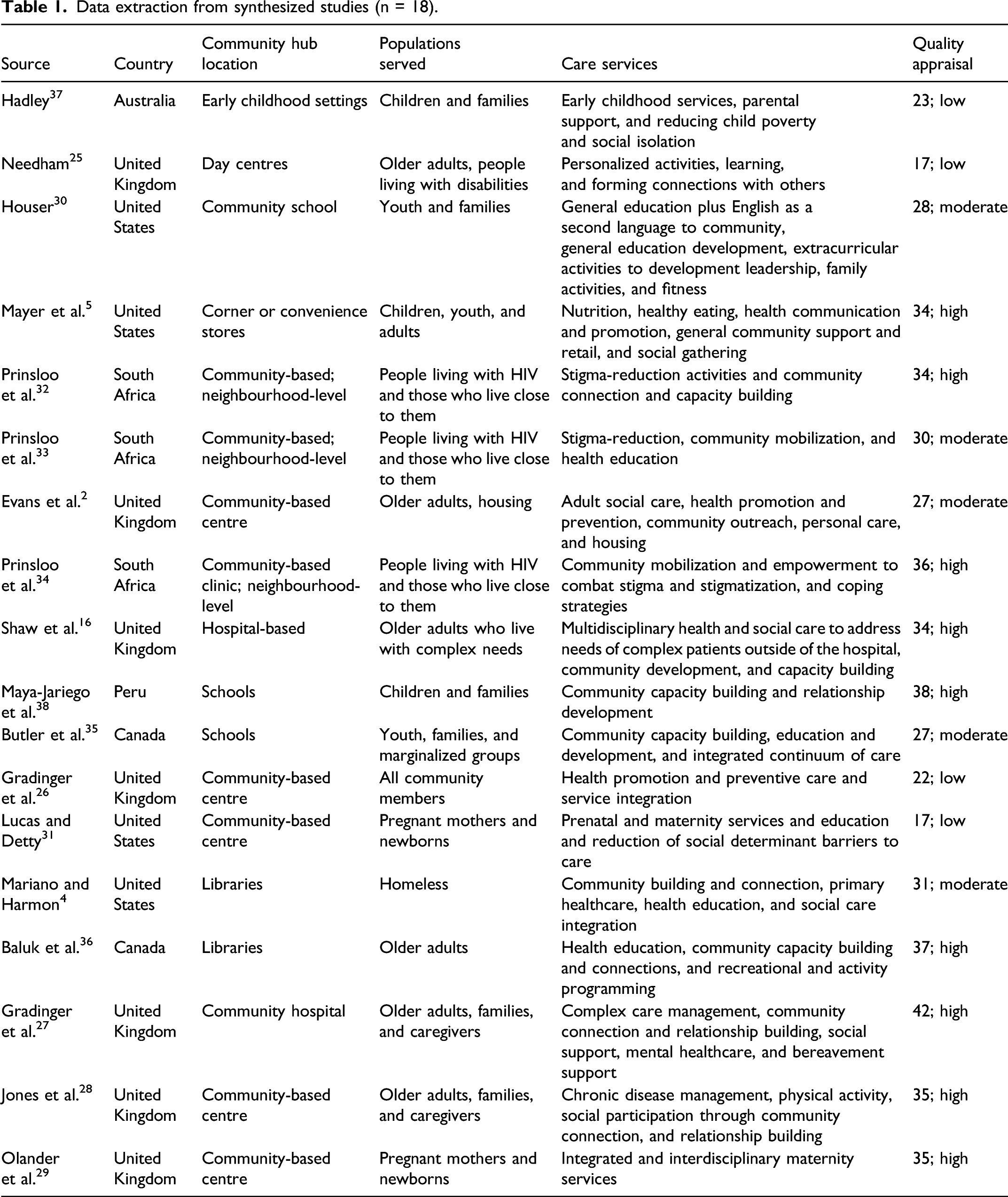
Community hubs were primarily found in the context of community-based centres or clinics (n = 9, 50%);2,25,26,28,29,31-34 however, schools (n = 3, 16.6%),30,35,38 hospitals (n = 2, 11.1%),16,27 libraries (n = 2, 11.1%),4,36 early childhood education centres (n = 1, 5.5%), 37 and corner stores (n = 1, 5.5%) 5 were locations that also housed community hubs. Community hubs were centrally located and easily accessible, and members of the community could often connect with others and access services and supports relevant to their health needs and goals.
Our thematic analysis established four thematic service areas: (1) Chronic disease management (ie, health promotion and education and lifestyle and behaviour modification); (2) mental health and addictions (ie, psychotherapy and social inclusion); (3) family and reproductive health (ie, STI/HIV testing and prenatal and early childhood development); and (4) seniors (ie, housing and recreational programming) (Figure 2). These were the core services included a community hub model of care. There was overlap between each of these thematic pillars, and so these pillars were not mutually exclusive. The services provided in a community hub were reflective of, and adaptive to, the needs of the community. Diagram of core and optional services of a community hub model of care.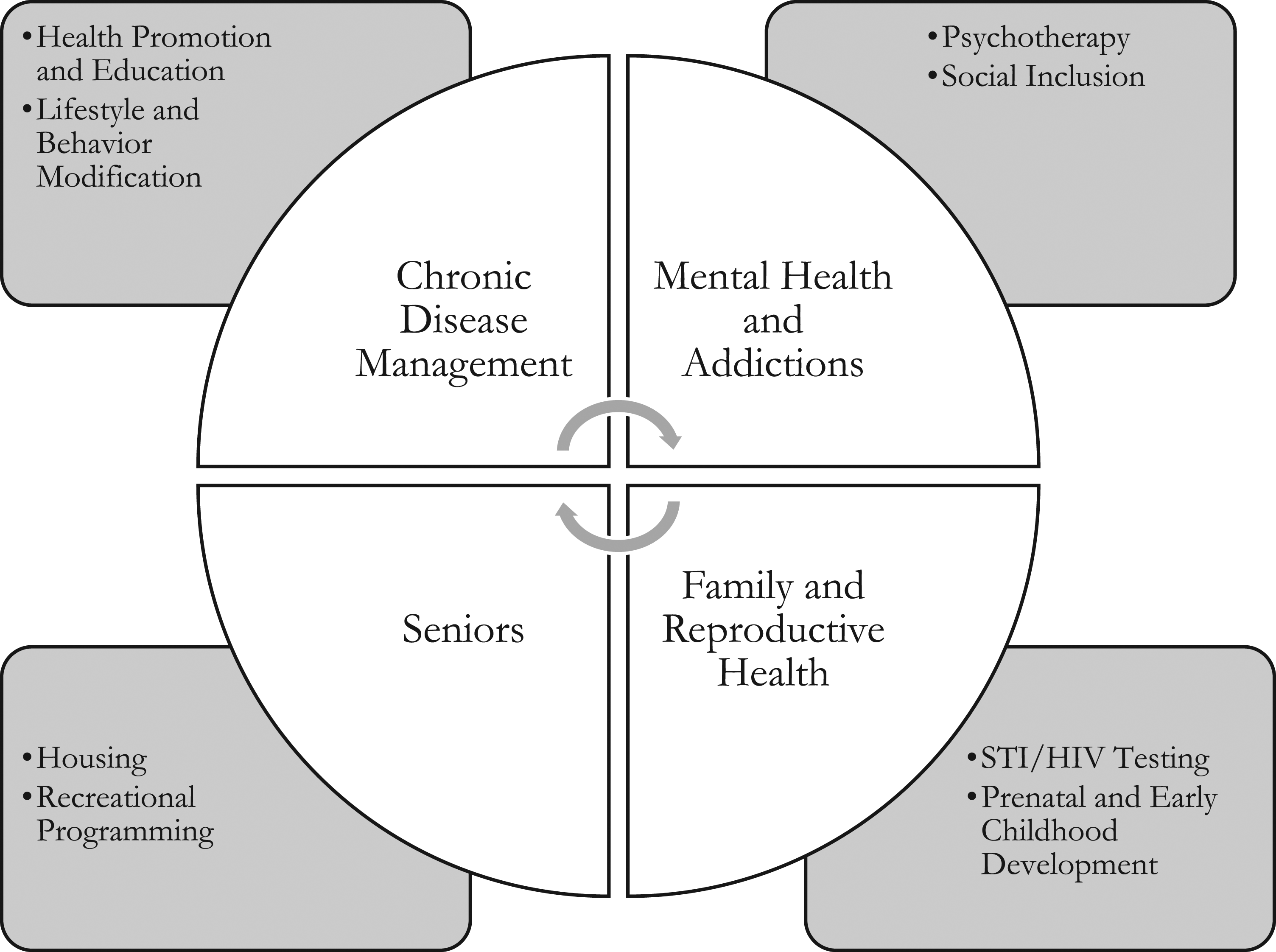
Discussion
Our narrative synthesis of the core services provided in a community hub model of care found there were four streams related to the service delivery: (1) Chronic disease management; (2) mental health and addictions; (3) family and reproductive health; and (4) seniors. The specific services are dependent on the needs of the users to ensure the community hub reflects the needs of the community. Community hubs foster relationship building with others in the community and facilitate access to co-located and integrated health and social care services. Community hubs leverage existing spaces and facilities within communities to support community health and improve the continuity and efficiency of care service delivery.
Community-informed models of care are inextricably linked to the delivery of primary healthcare. Primary healthcare leverages primary care (ie, family physicians providing care in communities, potentially in independent practices isolated from other healthcare practitioners) and additionally incorporates determinants of health among individuals and within communities.11,39 Primary healthcare has an inherent biopsychosocial orientation to promote, achieve, and maintain health and wellness among individuals and the communities in which they live. 39 Community-informed models of care consistently employ a biopsychosocial approach to facilitate person-centred care and strengthen health and wellness within communities. 12
There have been many reforms to primary care in Ontario. Capitation-based models were introduced in the early 2000s (eg, Family Health Network and Family Health Organization), but these models lacked a comprehensive interprofessional care component.11,40 Subsequent models aimed to increase access to interprofessional, collaborative healthcare (eg, Family Health Teams and Patient Medical Home models),11,23 but these models, too, were subject to capitation-based funding. Capitation-based funding provides physicians with a fixed payment per patient per time period,41,42 which can incentivize them to skimp on care and only take responsibility for healthier patients who have fewer needs for care. 41 Physicians who provide care in community-level models are salaried employees; they do not receive remuneration on a fee-for-service, capitation, or other forms of financial incentive (eg, performance-based payment), 11 and this can be a helpful strategy for encouraging interprofessional collaboration, reducing health system expenditures, and facilitating equitable access to care.43,44
Community-level models of care are governed by members of the community rather than by a board comprised of physicians.1,11,12 Many other primary care models (eg, Family Health Teams and Patient Medical Home models) are predominately governed and led by physicians or others who are not necessarily members of the community in which the centre serves.11,45 Governance by members of the community, rather than by physicians who govern, lead, and are accountable to the community, ensures the needs of the community are at the forefront of decision-making. Community governance should be considered a foundational component of patient and community involvement and participation in a community-informed model of care. 46
Community health centres have existed for more than 40 years, 47 yet previous reforms to primary care have not prioritized the physical co-location of providers and community partner organizations across the spectrum of health and social care characteristic of a community hub. The community hub engages community partners in a shared space to address the health and social care needs of all individuals who live within the community. 12 The adaptability and flexibility of the community hub model of care to leverage existing resources within the community to support individuals in achieving health and wellness throughout the life course is a notable strength.1,13 Moreover, there are reduced administrative costs (eg, rent and utilities) to housing providers and community partners in 1 location.
A key feature of community hubs was that the hub was in a central, easily accessible location within a community. In rural and remote areas, this may present a challenge.1,12,48 Recently, the rural health hub was proposed in northern Ontario. 49 All respondents supported the concept of the rural health hub (ie, co-location of all health and social care), independent of the need to travel, which was acknowledged as an inherent component of living in a rural and remote area. 49 This study supports that there is buy-in for a community hub model of care among those who live rural and remote regions.
Health leaders, decision-makers in community-based organizations, and primary healthcare clinicians considering the implementation of a community-level model of care should take an inventory of community-based groups and organizations that have a stake in the health, well-being, and social supports of residents within their community. 13 It is also important to identify the health needs and goals of community members to map possible services within the community hub. Strategies for ascertaining the health status of community members could be achieved through surveys, provincial statistics and other health system administrative data sources, and town halls or other engagement methods. Engaging community residents should be a core component of the process for designing and implementing a community hub. This engagement should refine and establish the health and wellness goals of the community, which should help to determine the most salient services and organizations that can contribute to achieving the community’s health and wellness goals. To ensure the community-governed focus of the community hub, we recommend members from the community in which the community hub serves constitute a majority of the steering committee and governing board. 1 Health leaders tasked with the implementation of these models of care should proactively engage community members to evaluate aspects of service delivery to ensure the model is reflective of the community’s needs and goals. Additionally, they should determine how the community hub will be funded, including the identification of specific financial sources, and how the amalgamation of providers and community partners in one location will affect funding and collective bargaining agreements of existing unionized staff.
There are limitations to our synthesis. The variation in health and social care system governance, financial, and delivery arrangements in each of the countries that had a community hub may affect the implementation and scaling up of community-informed models of care in other jurisdictions. There were no unpublished original research studies in the grey literature, and this may affect publication bias. Also, we did not hand search the reference lists of included sources to identify other potentially relevant sources.
Conclusion
Community-informed, integrated, and coordinated models of care are valuable community-level interventions to support the health and social care needs of all members within the community throughout the life course. Health system transformations towards these models of care support improved experiences, strengthened community and population health, and contribute to reduced healthcare expenditures. Future research should evaluate community hub level interventions and the preferences and values of community members for care to inform the development of community-level models of care.