
Abstract
Transitional care programs are effective for improving patient outcomes upon discharge from acute care services and reducing the burden of healthcare costs; however, little is known about the types of transitional care programs for older adults across Canada. This exploratory study gathered an in-depth understanding of Canadian transitional care programs and described how each program functions to support older adults and family/friend caregivers. Nine key informants were interviewed about the development of transitional care programs within four Canadian provincial regions including Atlantic, Central, Prairie, and West Coast. Key facilitators and barriers influencing the development and long-term success of transitional care programs included program scope, program structure, continuity of care, funding, and health system infrastructure. Future research is required to identify how a broad range of transitional care programs operate and to disseminate knowledge with health leaders and decision-makers to ensure transitional care programs are embedded as essential health system services.
Introduction
The most vulnerable exchange point within the healthcare system is when a patient is required to transition from one healthcare service to the next, with the greatest potential of health disparities for older adults and chronically ill patients. 1 –3 This is particularly challenging for older adults and their caregivers who are required to navigate within and between many acute and post-acute services. 4,5 It is often during these transitions that issues arise including delayed, unnecessary, and poorly coordinated care; poor communication; exacerbated mental health challenges; worsening health outcomes; additional family and friend caregiver burden; and inappropriate placement in long-term care facilities. 6 –8
Transitional care refers to a wide range of time-limited services designed to ensure the coordination and continuity of care for patients as they move between different locations, healthcare providers, or different levels of care within the same location. 9,10 The majority of transitional care programs are initiated while patients, predominately older adults, are hospitalized and awaiting discharge, 11 although some identify patients from primary care practices or other health and social service organizations. 12 The length of time that transitional care services are provided varies greatly and can range from 1 month or less to several years, and support is typically provided through a combination of face-to-face and telephone contacts. 12 Research indicates that transitional care is multifaceted and requires various healthcare professionals to be involved in providing rehabilitative and skilled care to ensure that transitions are safe and effective by fostering coordination and continuity across health settings, bridging medication continuity, early identification and response to health changes, facilitating access to the right services at the right time, planning for future health needs, and advocating for the needs of patients. 4,13 –16 A recent study that conducted a clinical audit of transitional care programs found that best practice recommendations to improve clinical care and the health of older adults after a transition from hospital include patient-centred discharge instructions, telephone follow-up, and family caregiver preparedness. 17 There is an increasing need to understand how transitional care programs can improve care and support older adults with increasingly complex care needs and reduce gaps in the continuum of care that ease the pressure on acute care systems. 18
Research has uncovered many benefits of transitional care programs for the healthcare system and users of the healthcare system. There is mounting evidence that transitional care programs are essential in addressing important challenges facing healthcare systems and our aging population by increasing the utilization of primary care services and reducing the use of more costly forms of healthcare such as unnecessary hospital admissions, readmissions, and premature nursing home placements. 12 –19 Older adults and their family and friend caregivers who have access to professionals with a coordination function across healthcare settings experience improved physical and psychosocial health status, an increase in self-management knowledge and skills, and a deepened sense of patient empowerment and safety during transitions. 9,20 –22
It has been posited that transitional care services are often lacking in Canada, 19,23 and there is little published research available focused on transitional care in Canada. Based on a systematic review published by our research team in 2018, we identified a very small number of Canadian studies conducted on transitional care programs 12 ; only 2 of 23 studies were conducted in Canada. 24,25 A scoping review published in 2019 that focused on community transition interventions to prevent hospital readmissions identified 35 studies that met the inclusion criteria, but none of the studies examined Canadian transitional care programs. 26 In 2020, Tomlinson and team 16 published a systematic review focused specifically on medication continuity during care transitions. Of 24 studies included in this systematic review, 2 were published in Canada, but these studies focused only on medication continuity during the transition from home to hospital admission. 27,28
It is apparent that a complete picture of transitional care programs in Canada cannot be obtained through the existing published research alone. An identified challenge in the published research is the lack of consistent terminology used to refer to transitional care programs and to refer to those that provide these services. 19 An additional challenge is that there appears to be a less consistent adoption in Canada of transitional care compared to other countries, such as the United States where the Transitional Care Model is quite widely adopted advanced practice nurse–led team-based model designed to support older adults throughout acute care transitions. 29
The aim of this exploratory study was to gather an in-depth understanding of transitional care programs across Canada by selecting a small number of exemplar transitional care programs and describing how each program functions to support older adults and their family and friend caregivers. While some programs are designed to support people with a single diagnosis, such as cancer or stroke, 30 –33 this research is focused on the transitional care programs that provide acute and post-acute support to older adults with multiple health conditions and their family and friend caregivers across a variety of settings.
Methods
After receiving approval from the Health Sciences Research Ethics Board at Dalhousie University (2017-4313), we created a list of diverse transitional care programs in Canada through a search of published studies, a grey literature search, and an on-line search. We defined transitional care programs as those ensuring the coordination and continuity of healthcare as older adults transfer between different locations or different levels of care within the same location. 9,10 Two authors then prioritized the list using maximum variation sampling 34 (eg, services provided, target population, location) to obtain a broad perspective on transitional care programs. Using these criteria, we prioritized 17 programs. Of these programs, six did not respond to the request to be interviewed, one did not meet the criteria of a transitional care program, and one interview was cancelled, and we were unable to reschedule. Key informants from the remaining programs were invited to participate in an interview. We interviewed nine key informants, which is considered a reasonable sample when utilizing qualitative data collection to generate rich descriptions and meaningful data. 35,36
The inclusion criteria for key informants were those knowledgeable about the development, characteristics, and outcomes of their respective transitional care program and could provide recommendations about the development of transitional care programs in Canada. Prior to participating in an interview, each person was sent the consent form electronically. At the beginning of the interview, the first author reviewed the consent form, answered questions about the study, and obtained verbal consent. Key informants were informed that interview data would be anonymized and would not contain information that would potentially identify the individual or program they worked with during dissemination of results of the study. All key informants gave permission to use non-identifying quotes. To ensure that the key informants or programs were not identifiable in the results, we only used a participant number to identify quotes and omitted potentially identifying information, such as location or type of program.
Key informants were invited to describe their job title, role, qualifications, and history with the program. The semi-structured interview guide included questions to elicit details about the transitional care program including its history, mission, target population, personnel, and services provided. They were invited to describe what worked well, what they would like to change, and recommendations for others developing similar programs.
All interviews were conducted by the first author. The interviews were audio-recorded and transcribed verbatim. Interview transcripts were analyzed using thematic analysis, a form of pattern recognition for inductive coding 37 useful for understanding influences and motivations related to how people respond to events. 38 Data analysis was facilitated by using QSR International’s NVivo12 software. Data analysis involved generating initial codes, searching for themes, reviewing themes, and defining and naming themes that represented responses within the data set. 37 –39 Two members of the research team read the transcripts and collaboratively developed codes for the thematic analysis focused specifically on facilitators and barriers to the development of transitional care in Canada: program scope, program structure, continuity of care, funding, and health system infrastructure. Then, two members of the research team independently coded one transcript and met to compare their results. This resulted in further refinement of the definitions of each code. They then independently coded each of the remaining transcripts and met to compare codes. Any discrepancies were resolved through consensus.
Findings
Key informants
We conducted individual interviews with nine key informants in November and December 2017. The interviews were conducted by telephone (n = 8) or face to face (n = 1). We conducted interviews in the Atlantic provinces (n = 3), Ontario (n = 3), the Prairie provinces (n = 2), and British Columbia (n = 1). The interviews ranged from 30 to 57 minutes (mean = 42 minutes) and included eight women and one man with a variety of backgrounds including nursing (n = 5), social work, dietetics, advocacy, and business.
Summary of transitional care programs identified
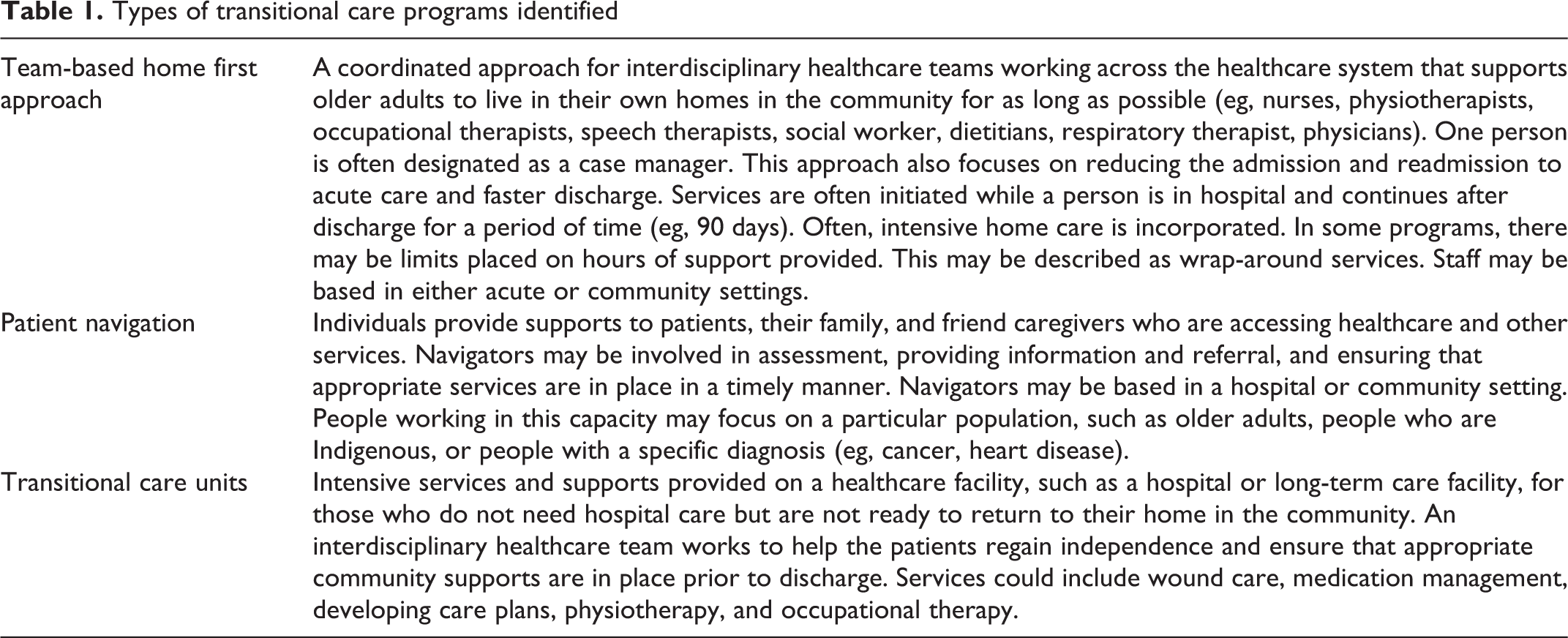
Many programs identified appeared to be quite new or were pilot projects that no longer existed. How the phrase transitional care was used appeared to be quite broad. The language surrounding transitional care professionals varied, as there were navigators, care coordinators, and case managers doing transitional care work, but they did not necessarily define this work as transitional care. Results from the initial search for transitional care programs in Canada and interviews with key informants led to the identification of three types of programs currently in existence (see Table 1).
Types of transitional care programs identified
Facilitators and barriers
Five themes emerged as key facilitators and barriers influencing the development and long-term success of Canadian transitional care programs.
Program scope
Program scope is a key facilitator for transitional programs and was defined as having program vision, mission, and goals to inform program design and model of care to best meet the needs of patient populations and community contexts. It was important to “look as a leadership team on the vision and mission statement. Really making that statement first, and then building the program from there” (P4). Key informants discussed the importance of tailoring the program goals “and working with the public to better serve the needs of a population” (P1) to deliver relevant services based on existing resources available within a community.
Program structure
Program structure included several aspects of how the professionals worked together to provide transitional care including defining the role of key healthcare providers and the structure of interprofessional teams for delivery of a broad range of services. Key informants described the importance of interprofessional team members developing collaborative relationships early on in a program’s development such as highlighting the importance of “having a good team approach and working closely with resources in the community for quicker access to resources so that people don’t fall through the cracks” (P6). Program structure was strengthened by supporting ongoing education and training of healthcare professionals, knowledge sharing among team members, and flexibility for healthcare providers to deliver a broad range of services, such as “being able to go out to homes and do assessments to respond immediately to what their needs are” (P3).
Continuity of care and individualized care
Based on program scope and program structure, a facilitator included the ability for transitional care programs to operate as a “hospital without walls” (P9), assisting patients with not all of the services of a hospital, but facilitating meeting individualized needs and continuity of care during discharge planning and transition from one service to the next. Individualized care and continuity of care were key: “there is a shared care plan with patients to set up goals, educate, allow patients to be more independent, set up equipment, and then discharge patients from the program” (P9). Programs were successful at filling gaps in healthcare service delivery by “identifying where people fall through the cracks and streamlining things for people” (P5). Working one-on-one to adjust discharge plans within the community and connecting patients with appropriate resources faster are advantageous: “the patient can’t wait in the hospital for 6 months. The amazing thing is that the hospital becomes a resource and they put the money upfront and the public guardian and trustee would reimburse them. This creative work moves things along” (P8).
Funding
A key barrier included the limited capability to secure dedicated and ongoing funding. Funding was a key barrier for hiring additional healthcare providers or increasing hours of enhanced support for patients. For instance, “it would be great if we could provide more than the current intense hours. Some patients need more, but due to fiscal restraints, we can’t do 27/7 care” (P7). Programs were challenged to provide services for patients with complex needs: “We recognize these people are getting older and are requiring more complex health needs. We don’t really have a place for them or standard way of supporting them” (P7).
Health system infrastructure
These programs faced barriers from health system organization and operation of segmented health services, a lack of infrastructure for tele-homecare and electronic medical records, and regulations that limit the expansion of transitional care programs. A primary challenge is with the way Canada’s healthcare services are designed to operate independently such as multiple, “facades within department of health that handle acute care, like all the different external agencies, whether it’s mental health or addictions. But they aren’t conjoined in one place, it’s a little more fractured to find anything” (P2). Another major barrier was the lack of a shared electronic health record for each patient, leading to disjointed communication between healthcare professionals and vast amounts of time for clerical paperwork. Lastly, key informants described health system barriers from inconsistent regulations across different regions preventing transitional care programs from gaining access to patients waiting in hospital for discharge and requirements of a facility when delivering short-term care.
Discussion and conclusions
Our results point to a lack of consistent terminology used to refer to transitional care programs and even the model of service delivery which further reflects challenges identified by key informants towards having transitional care services institutionalized across healthcare systems. We identified three types of transitional care programs that provide support to older adults with multiple health conditions across a variety of settings: a team-based home first approach, individuals providing patient navigation, and transitional care units. Given this study was exploratory, we encourage other researchers to further delineate transitional care programs operating within the Canadian context and build upon our results by comparing existing transitional care services that support strategies and best practice recommendations for improving older adult health outcomes. Delineating transitional care programs is critical for revealing gaps in acute and post-acute care service delivery that could lessen the burden of healthcare costs such as reducing the number of patients waiting in hospital as well as reducing readmission rates due to failed transitions between services. 5,12,26,40
We found that many Canadian programs represented in this study were newly developed or initiated as pilot projects. Given that evidence exists that transitional care programs contribute to cost savings in the healthcare system, 12,19 it is surprising that we found evidence of the lack of funding stability of these programs. Changes to health system infrastructure are required to reduce silos between the delivery of acute care and community services, increase investments towards the redesign of how we provide care for older adults, and embed the institutionalization of transitional care as a publicly funded essential service. 18 Incremental changes and improvements to Canada’s health system infrastructure such as the development of electronic medical records emerged as a key factor that could contribute to the success of transitional care programs. 41
A larger and more inclusive study of transitional care programs in Canada is warranted. We recognize that individual provinces/territories or health regions may provide transitional care services that we did not identify. A gap is that we did not conduct any interviews in French. Also, research is needed in Canada that focuses on the needs of diverse older adults and their caregivers requiring transitional care. For example, transitional care studies elsewhere have focused on older adults with low income, low health literacy, and limited English proficiency. 42
Recent studies in Canada and elsewhere have identified the important role that family and friend caregivers have to provide support for older adults after discharge from the hospital. 17,43,44 In particular, family and friend caregivers have a crucial role in contributing to the development of care plans and their implementation after hospital discharge. 17,45 While it is recommended that family and friend caregivers of older adults be involved in discharge planning from hospital to home, 17,46 most transitional care programs we identified in this study, and in the published research, do not specifically state that their target population included family and friend caregivers of older adults requiring transitional care. There is value in expanding the target population of transitional care programs to include the needs of familial and friend caregivers 47 who can contribute to older adults aging in place.
In this study, we provided insights into the current state of transitional care for older adults in Canada including the identification of three types of transitional care programs. We also identified current key facilitators and barriers to the further development of transitional care. We encourage other researchers to build upon our results to further delineate transitional care programs operating within Canada. Investments towards transitional care programs are critical for improving health outcomes for some of the most vulnerable older adult and chronically ill patients and decreasing the high burden of costs associated with unnecessary healthcare spending from potentially avoidable usage of the acute care system. 2
Footnotes
Acknowledgments
The authors recognize the Research Assistant Support received from Ememoh Ogheneruemu in the preparation of this manuscript.
Funding
The authors acknowledge funding received to support this research from the Nursing Research and Development Fund, School of Nursing, Dalhousie University.