
Abstract
During previous disasters, youth with existing mental health diagnoses have been especially vulnerable to negative mental health outcomes. Yet, longitudinal outcomes for these youth during the COVID-19 pandemic have not been well-studied. In addition, potential protective factors that may buffer this enhanced risk in the context of the pandemic also need to be explored. Thus, this longitudinal study investigates if having a self-reported learning, cognitive, and/or psychological disorder diagnosis placed adolescents at greater risk for trauma symptomology over the first full academic year (2020-21) of the COVID-19 pandemic, and if this relationship was moderated by peer or family support. To answer this question, we collected four waves of data from youth (M age = 14.63) in one province in Western Canada over the 2020/21 school year (N = 1,227). Trauma symptomology was assessed using the Child Revised Impacts of Events Scale (CRIES-13). We used multivariate linear regression to assess if an existing learning, cognitive, and/or psychological disorder diagnosis was associated with trauma symptomatology in June 2021, controlling for symptoms in September 2021, and to explore potential moderation by peer and family support. We found that youth who had an existing learning, cognitive, and/or psychological disorder diagnosis reported significantly higher trauma symptomatology across the 2020/21 academic year, as compared to youth without a diagnosis, but that there was no moderation by peer or family support. Our results suggest that a small but significant subset of youth who were at risk for poor mental health outcomes prior to the pandemic remain vulnerable and require access to ongoing school psychology supports to promote their mental well-being.
Keywords
An ongoing concern during and post-pandemic is the mental well-being of adolescents (Farrell et al., 2023; Korczak et al., 2023; Madigan et al., 2023; Racine et al., 2021; Vaillancourt et al., 2021). Indeed, research shows that direct (e.g., contact with virus) or indirect (e.g., social media) exposure to COVID-19 may have evoked post-traumatic stress disorder (PTSD)-like responses, causing it to now be understood as a traumatic stressor (Bridgland et al., 2021), with particular risk for youth experiencing marginalization or social deprivation (Giannopoulou et al., 2021). If left without intervention, the effects of stressful events like COVID-19 can lead to adult psychopathology (Deeba et al., 2014). Thus, to avoid negative outcomes, it is important for school psychologists to understand which adolescents were most vulnerable to experiencing post-pandemic trauma symptomology, as ongoing detection and intervention are vital for both short and long-term wellbeing. However, longitudinal research on trauma symptomology experienced by adolescents during the pandemic is very limited (Ozamiz-Etxebarria et al., 2023). Thus, the purpose of this study is to investigate self-reports of trauma symptomology among a sample of Canadian adolescents aged 12 to 18, and explore whether youth with an existing learning, cognitive, and/or psychological disorder diagnosis reported greater risk for increased trauma symptomology over the first full school year of the pandemic (2020/21). We also explore whether social support—a key protective factor in adolescence—may have buffered risk for this sub-group.
Adolescents, Mental Health & COVID-19
During the pandemic, school mental health services were interrupted, leading to disruptions in receipt of service delivery for many youth (Masonbrink & Hurley, 2020). Community mental health services were also disrupted (S. L. Stewart et al., 2022). Related, early in the pandemic, Guessoum et al. (2020) wrote on the need to specifically understand the impact of the pandemic on youth with existing psychiatric diagnosis, building on research from prior disasters suggesting that youth with prior diagnosis are a vulnerable population. Yet, we are not aware of research that has explored longitudinal outcomes for youth with a learning, cognitive, or psychological health diagnosis in the context of the COVID-19 pandemic. More information is available in adult samples, which demonstrates that adults with pre-existing mental health conditions were at greater risk for mental health complications during COVID-19 (Buneviciene et al., 2021; Miller et al., 2021; Neelam et al., 2021), potentially due to the social and individual challenges associated with the pandemic (i.e., isolation, anxiety, financial pressure, etc.; Miller et al., 2021). It is thus important to expand research in this area to adolescent populations using longitudinal data.
Trauma Symptomology
A recent meta-analysis found that between 11% and 18% of adolescents experienced PTSD symptoms during the pandemic (Ozamiz-Etxebarria et al., 2023). However, in terms of understanding which youth may have been at greater risk of experiencing these symptoms, most of the extant research has focused on risks related to demographic characteristics such as socioeconomic status, age, and gender (e.g., Selçuk et al., 2021), with limited exploration of other factors, like pre-existing health or mental health issues (Guessoum et al., 2020). We are aware of two cross-sectional studies looking at the association between existing health/mental health conditions and traumatic stress symptoms in the context of the pandemic. Findik et al. (2022) collected data from youth and adults in Turkey, and found that in the context of the pandemic, youth reported more post-traumatic stress symptoms than adults, and that youth with a pre-existing medical condition—but not those with a history of mental health needs—had significantly higher post-traumatic stress symptoms than youth without a medical condition. Another study conducted in China during the pandemic compared trauma symptom scores (assessed on the CRIES-13) in youth with and without major depressive disorder (MDD), and found that youth diagnosed with MDD had higher CRIES-13 scores and were more likely to report scores indicative of a PTSD diagnosis when compared to those without MDD (Zhang et al., 2021). Thus, existing health and mental health status might be potentially important risk factors for pandemic-related traumatic stress (Fegert et al., 2020; Guessoum et al., 2020), but these factors have been under-explored. Therefore, this study aims to investigate and bring awareness to the role that existing conditions—specifically learning, cognitive, and/or psychological health diagnoses—may have had on youth mental health during the first year of the pandemic, in terms of how these diagnoses are associated with pandemic-related trauma symptomology.
Adolescent Resilience During Stressful Events
Although some youth are likely more vulnerable to adverse mental health consequences related to the pandemic, there are also factors that may be protective for these same youth. Research on past natural disasters suggests that many adolescents experiencing stressful events will demonstrate resiliency (Osofsky et al., 2009). During times of increased stress and difficulty, resiliency is the capacity to sustain mental wellbeing through navigation to and availability of relevant resources (i.e., psychological, spiritual, social, emotional, and/or physical support; Ungar & Theron, 2020). One commonly examined source of resilience for youth outside the context of the pandemic is social support, or the delivery of psychological care and resources from people like primary caregivers, peers, and teachers (Dumont & Provost, 1999; T. Stewart & Suldo, 2011). For example, prior research demonstrates that higher levels of social connectedness moderate the effects of stressful events (Dumont & Provost, 1999), and promote higher life satisfaction (Magson et al., 2020). In the context of the pandemic, Magson et al. (2020) found that self-reported feelings of being socially connected during lockdowns moderated against anxiety and depressive symptoms in adolescents. As such, social support may also have been an important protective factor during the acute stages of COVID-19.
When looking at sources of social support, adolescents typically rely on their peers for emotional support (Magson et al., 2020), but disruptions to peer relationships related to COVID-19 health measures (e.g., lockdowns, social distancing) reduced most adolescents’ ability to interact with their peers in developmentally-typical ways (Farrell et al., 2023; Orben et al., 2020). However, though many adolescents were likely physically separated from their peers (at least temporarily) during the first year of the pandemic, even the perception of social support can be beneficial to adolescent outcomes (T. Stewart & Suldo, 2011), and many adolescents were able to stay connected through use of technology (Orben et al., 2020). Family support is also influential in supporting adolescent mental health (Chen et al., 2021; Magson et al., 2020; Wang et al., 2021). Yet, in the context of the COVID-19 pandemic, primary caregivers were forced to adapt to an unexpected situation when schools closed, and as a result, not all caregivers had the capacity and/or resources to provide physical and/or psychological support (Fegert et al., 2020).
Current Study
Per past literature and to address key gaps in COVID-19 mental health research, including the need for longitudinal data on trauma symptomology, the current study investigates (1) if youth self-reporting a current and/or new learning, cognitive, and/or psychological disorder diagnosis also reported a significant change in trauma symptomatology over the first full academic year (2020/2021) of the pandemic, as compared to youth without a diagnosis and (2) if social support from peers and/or caregivers buffered this potential change. We focus on youth as COVID-19 restrictions, such as lockdowns, are speculated to have been particularly difficult for adolescents for multiple reasons (i.e., loss of resources, interrupting peer relationships and academic functioning; Magson et al., 2020). For example, school closures meant that many youth lost access to school mental health services, with particular concern about the amplification of inequities for already disadvantaged youth (Giannopoulou et al., 2021). Although some youth returned to school in fall 2020, it was still not a return to normal for most youth due to masking mandates, social distancing, and changes to curriculum delivery (Schwartz et al., 2021), resulting in the potential for continuing associations between the pandemic and poor mental health.
Hypotheses
For our first aim, we hypothesize that youth reporting any learning, cognitive, and/or psychological disorder diagnosis will report greater trauma symptomology, as compared to adolescents with no diagnosis. For our second aim, we anticipate that (a) since many adolescents were able to stay connected with their peers through technology in the first year of the pandemic, peer social support will buffer against the risk of trauma symptomology in adolescents with a learning, cognitive, and/or psychological diagnosis and that (b) although family support is an effective protective factor during times of high stress, the first year of the pandemic also created unique stress and strain on families, which may have impacted caregivers’ ability to provide social support. As such, we hypothesize that family support will still buffer the diagnosis-trauma symptomology relationship in this sample, but to a lesser extent than peer support.
Method
Participants
Participants in this project were recruited in fall 2020 through partnerships with four large urban school districts (two public, two Catholic) in a Western Canadian province. Information about the study was provided to each school district, who then disseminated the information to parents/guardians and to youth themselves if they were age 18. Parents/guardians electronically signed consent forms using REDCap (Research Electronic Data Capture; Harris et al., 2009, 2019) and provided an email address for their child to receive the survey link. If youth were 18, they were able to provide their own consent. Students aged 12 to 17 also provided written assent prior to beginning the study. To be eligible to participate, youth needed to be between the ages of 12 to 18 and a student in one of the participating school districts. Ethics approvals for this study was obtained from a university research ethics board and each of the participating school districts.
Procedures
Surveys were sent at four occasions in the 2020/21 school year: September 2020 (T1), December 2020 (T2), February 2021 (T3) and June 2021 (T4). For a timeline and summary of data used in this paper, see Figure 1. All surveys were completed on the student’s own time via REDCap electronic data capture tools hosted at the principal investigator’s university. REDCap is a secure, web-based software platform designed for research studies (Harris et al., 2009, 2019). The surveys took approximately 20 min each to complete. At each timepoint (T1, T2, T3, T4), students who completed the survey received a $10 electronic gift card as a thank-you for their participation (maximum $40 CAD across the four timepoints).
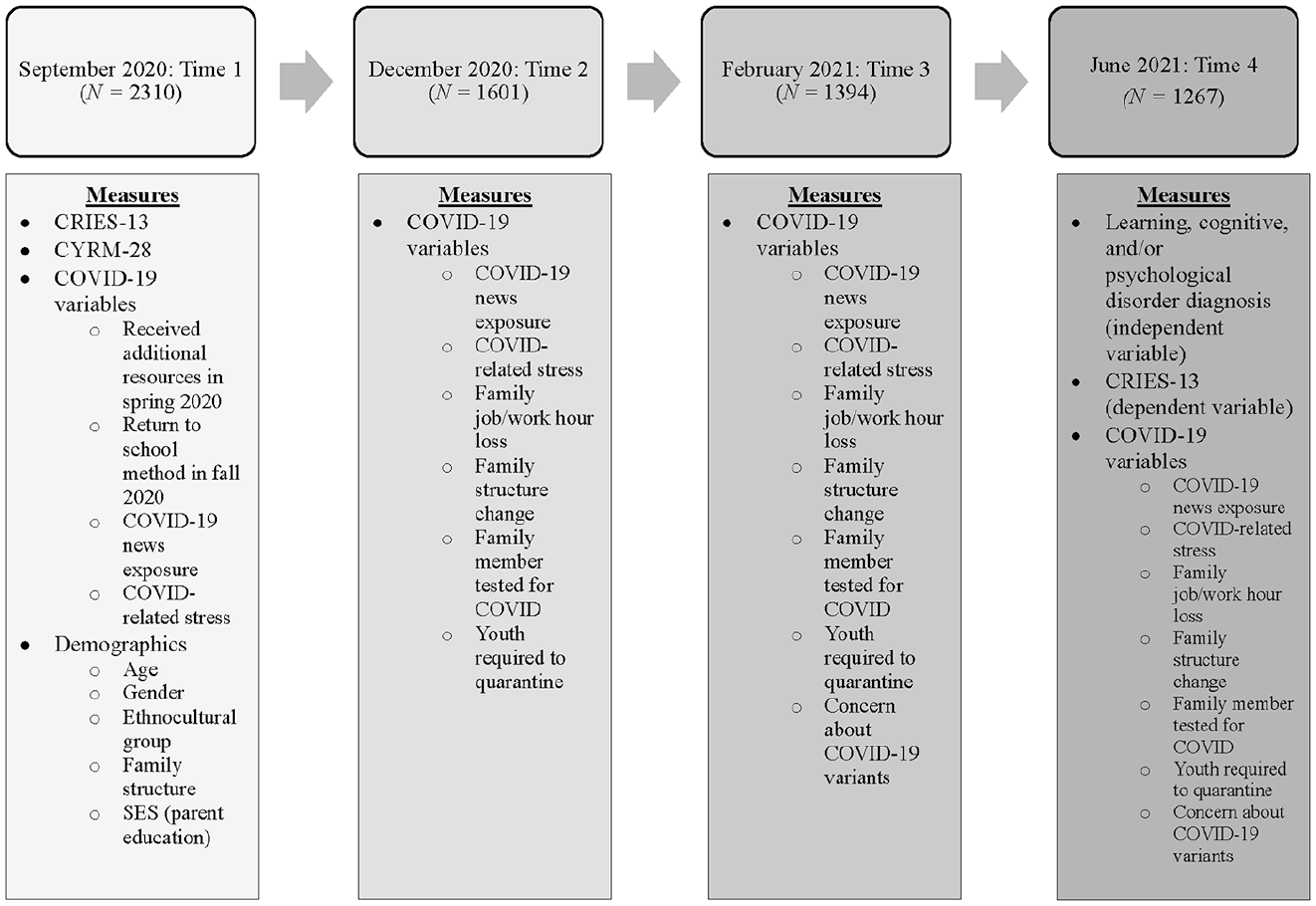
Study timeline and included variables.
In total, we received consent for 5386 youth to participate in the study (5,277 forms from parents/guardians and 109 from youth aged 18; ~3.5% consent rate across all four boards). At T1, 2,310 youth completed the survey (42.9% assent rate). Retention rates were: 69.3% at T2 (n = 1601); 60.3% at T3 (n = 1,394); and 54.8% at T4 (n = 1,267). For the present paper, youth were included in our sample if they had (1) completed surveys at both T1 and T4 (as our key dependent and independent variables were measured at these timepoints) and (2) provided data on the diagnosis question at T4 (as this was our key independent variable; n = 1,227). Youth who completed both T1 and T4 surveys were significantly older, and more likely to be a cisgender girl, to live in a dual-caregiver household, and to have returned to school in an online or blended format than youth with T1 data only. There were no differences in socioeconomic status (SES) or ethnocultural group between those who completed both T1 and T4 or only T1.
Measures
Learning, Cognitive, and/or Psychological Disorder Diagnosis
Two questions were asked at T4 to assess any diagnosis among participants. First, youth were asked if,
Youth Trauma Symptomology
Youth trauma symptomology was assessed using the Child Revised Impact of Events Scale (CRIES-13; CORC Child Outcomes Research Consortium, n.d.; Giannopoulou et al., 2006; Perrin et al., 2005). This 13-item measure is designed to assess how youth are dealing with current stressful life events. In this study, students were given the following prompt: “Below is a list of comments made by people after a stressful life event. Please select each item showing how frequently these comments were true for you during the past seven days about COVID-19.” Items on the CRIES-13 tap intrusion, avoidance, and arousal symptoms. This scale has evidence of reliability and factor structure in a sample of early and mid-adolescents from Bosnia (Smith et al., 2003) and in an adolescent sample who survived a cruise ship disaster (Yule et al., 1994), and has criterion validity evidence in an emergency department sample of children and youth (Perrin et al., 2005). Participants rate each item on a Likert scale with four anchors (0 = not at all, 1 = rarely, 3 = sometimes, 5 = often). Scale scores are created by summing across items. Total scale scores range from 0 to 65 (αT1 = 0.90; αT4 = 0.92), with higher scores indicating greater trauma symptomology. We used CRIES-13 data from T1 and T4 in this paper (Figure 1).
Peer and Family Support
Peer and family support were assessed using the Child and Youth Resiliency Measure (CYRM)—Youth Version, a 28-item scale that measures the availability of resources known to promote resilience (Liebenberg et al., 2012). The CYMR has reliability and validity evidence for youth aged 11 to 19 years, and is appropriate for use across multiple contexts and cultures (e.g., Höltge et al., 2021; Jefferies et al., 2019). Participants rate each item using a five-point Likert scale (1 = not at all to 5 = a lot), and total and sub-scale scores are created by summing across items. Higher scores indicate that more of the particular resource (e.g., peer support) is available to the youth. As the current study investigates the availability of social support, two sub-scales were used from the larger measure: (1) peer support (e.g., I feel supported by my friends; αT1 = 0.86; 2 items; score range 2–10) and (2) psychological caregiving (e.g., my family stays by me in difficult times; αT1 = 0.83; 5 items, score range 5–25; referred to in this paper as family support). We used CYRM data from T1 in this paper (Figure 1).
COVID-19 Variables
We also collected several time-varying COVID-19 specific variables (Figure 1). At T1, we asked if youth had received any additional resources since schools closed in March 2020 (learning support, mental health support, support from a teacher, principal or guidance counselor; 0 = no, 1 = yes), and their return to school method in fall 2020 (0 = in-person, 1 = online/blended). At all timepoints, we assessed youth exposure to COVID-19 news on social media using a single item (1 = never to 5 = daily), and their COVID-related stress using an 11-item scale created to assess the pandemic’s impact on youth stress (1 = not at all to 4 = extremely; αT1 = 0.82; Craig et al., 2023). At T2, T3, and T4, we asked if their family had experienced job/work hour loss (0 = no, 1 = yes); family structure change (e.g., parents are now separated/divorced; 0 = no, 1 = yes); whether a family member had been tested for COVID-19 since the prior timepoint (0 = no, 1 = yes); and if the youth was required to quarantine since the prior timepoint (0 = no, 1 = yes). At T3 and T4, we used a single item to assess if the youth was concerned about emerging COVID-19 variants (1 = not at all to 4 = extremely).
If a COVID-19 variable that was collected at multiple timepoints had consistent associations with T4 CRIES-13 scores (Figure 1), we combined these data across timepoints to reduce the number of variables for analysis. This resulted in the creation of the following composite variables: T1 to T4 COVID-related news exposure (indicating average across timepoints); T1 to T4 COVID related stress (indicating average across timepoints); T2 to T4 family job/work hour loss (1 = yes, any; 0 = no, none, across timepoints), T2 to T4 family structure change (1 = yes, any; 0 = no, none, across timepoints); T2 to T4 having a family member tested for COVID-19 (1 = yes, any; 0 = no, none, across timepoints), and T2 to T4 youth having to quarantine (1 = yes, any; 0 = no, none, across timepoints).
Demographics
At T1, we collected age, gender (write-in response), ethnocultural group, family structure (two caregivers in the home; 0 = yes, 1 = no), and SES (assessed by the highest level of education obtained by the youth’s parent figure(s); 6 levels; Table 1). Due to sample size constraints and recognizing Canada’s history of colonization and systemic racism, we created a combined ethnocultural variable for analysis (0 = White only, 1 = Ethnocultural group; Table 1).
Demographic, COVID-19, Moderator, and Outcome Variables.
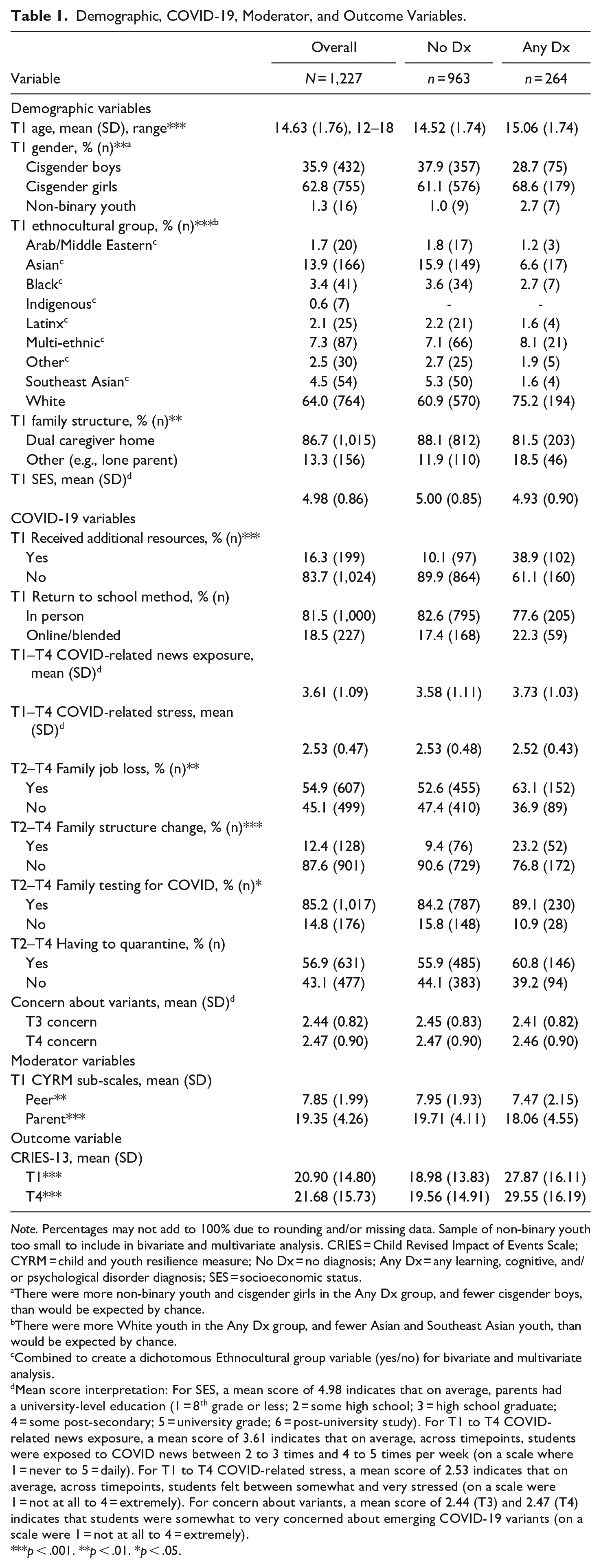
Note. Percentages may not add to 100% due to rounding and/or missing data. Sample of non-binary youth too small to include in bivariate and multivariate analysis. CRIES = Child Revised Impact of Events Scale; CYRM = child and youth resilience measure; No Dx = no diagnosis; Any Dx = any learning, cognitive, and/or psychological disorder diagnosis; SES = socioeconomic status.
There were more non-binary youth and cisgender girls in the Any Dx group, and fewer cisgender boys, than would be expected by chance.
There were more White youth in the Any Dx group, and fewer Asian and Southeast Asian youth, than would be expected by chance.
Combined to create a dichotomous Ethnocultural group variable (yes/no) for bivariate and multivariate analysis.
Mean score interpretation: For SES, a mean score of 4.98 indicates that on average, parents had a university-level education (1 = 8th grade or less; 2 = some high school; 3 = high school graduate; 4 = some post-secondary; 5 = university grade; 6 = post-university study). For T1 to T4 COVID-related news exposure, a mean score of 3.61 indicates that on average, across timepoints, students were exposed to COVID news between 2 to 3 times and 4 to 5 times per week (on a scale where 1 = never to 5 = daily). For T1 to T4 COVID-related stress, a mean score of 2.53 indicates that on average, across timepoints, students felt between somewhat and very stressed (on a scale were 1 = not at all to 4 = extremely). For concern about variants, a mean score of 2.44 (T3) and 2.47 (T4) indicates that students were somewhat to very concerned about emerging COVID-19 variants (on a scale were 1 = not at all to 4 = extremely).
p < .001. **p < .01. *p < .05.
Data Analysis
We used descriptive and bivariate statistics (chi-square, independent samples t-tests, one-way ANOVA) to explore sample characteristics, as well as potential confounders of the diagnosis-CRIES relationship at the p < .10 level. In these analyses, we found that T4 CRIES-13 scores significantly varied by age; gender (cisgender girls); SES; receiving additional resources at T1; T1 return to school method (online/blended/did not return); T1 to T4 COVID-19 news exposure; T1 to T4 COVID-related stress scores; T2 to T4 family job loss; T2 to T4 family structure change; T2 to T4 COVID-19 testing (having a family member test for COVID); T2 to T4 having to quarantine; and T3 and T4 COVID-19 variant concern. We thus initially controlled for all these variables in multivariate analysis, and then used backwards selection to determine the final list of covariates (Table 2).
Multivariate Regression Model Predicting T4 CRIES-13 scores, with Moderation by CYRM Peer and Family support Sub-Scales.
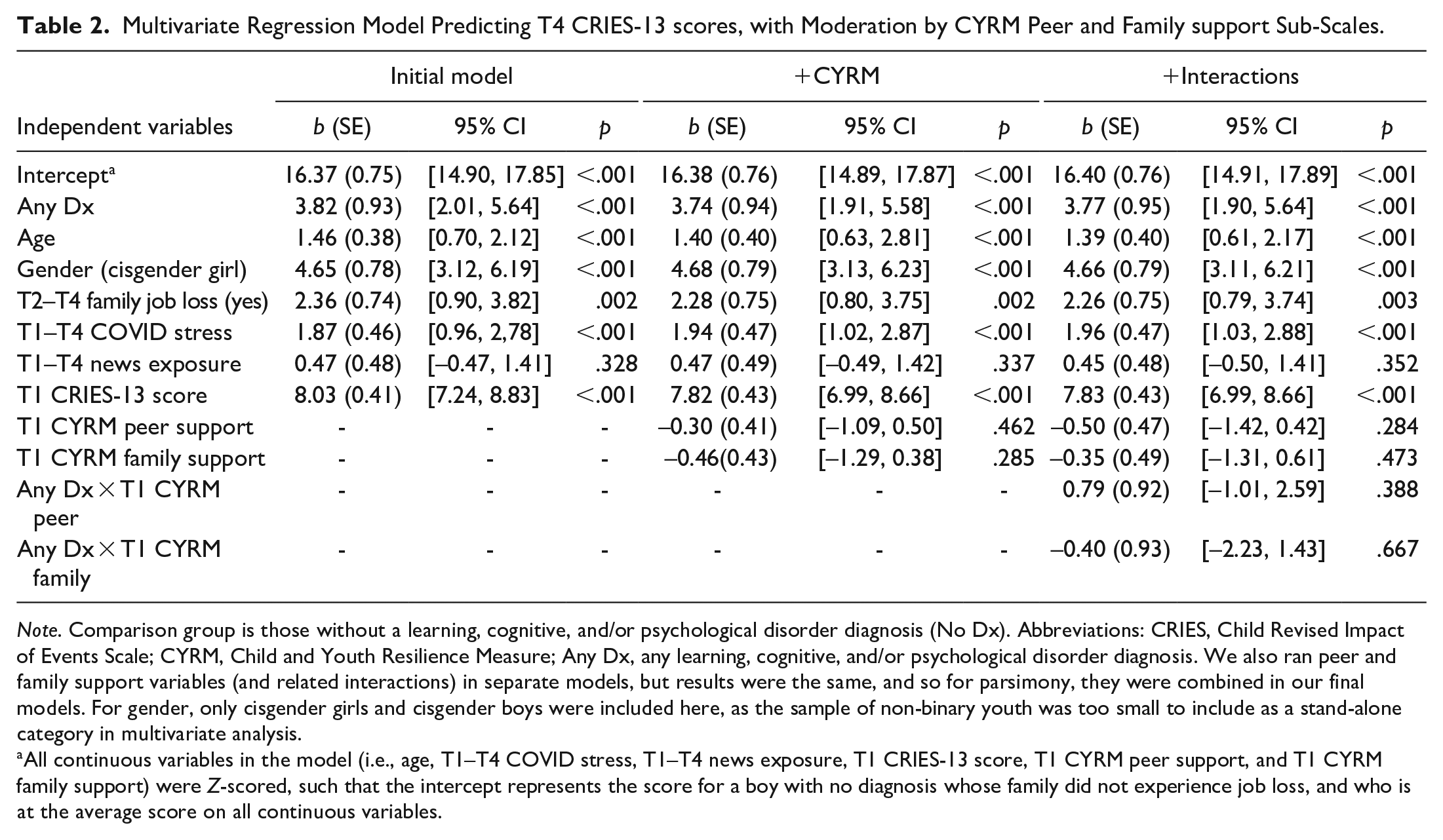
Note. Comparison group is those without a learning, cognitive, and/or psychological disorder diagnosis (No Dx). Abbreviations: CRIES, Child Revised Impact of Events Scale; CYRM, Child and Youth Resilience Measure; Any Dx, any learning, cognitive, and/or psychological disorder diagnosis. We also ran peer and family support variables (and related interactions) in separate models, but results were the same, and so for parsimony, they were combined in our final models. For gender, only cisgender girls and cisgender boys were included here, as the sample of non-binary youth was too small to include as a stand-alone category in multivariate analysis.
All continuous variables in the model (i.e., age, T1–T4 COVID stress, T1–T4 news exposure, T1 CRIES-13 score, T1 CYRM peer support, and T1 CYRM family support) were Z-scored, such that the intercept represents the score for a boy with no diagnosis whose family did not experience job loss, and who is at the average score on all continuous variables.
We used multivariate linear regression to explore longitudinal associations between CRIES-13 scores at T4 and any diagnosis. All analysis were conducted using SPSS V26, and all continuous variables were Z-scored (i.e., mean-centered) prior to multivariate analysis. We also conducted supplemental analyses to explore associations between T4 CRIES-13 scores and when a diagnosis was received (i.e., before and/or since COVID-19; see Supplemental Material). We used the PROCESS macro (Hayes, 2018) to explore potential interaction effects. Imputation of missing values was used for participants with incomplete responses to CYRM and CRIES-13 items at a given survey occasion, but only in cases where data were partially completed at the relevant survey timepoint. Missing data on item-level variables for these participants were imputed with the numerical mean of the assessment scale, so as to not skew the summed scale scores. For all analyses except assessment of potential confounders, we used a cut-off of p < .05.
Positionality
We are all White scholars trained within the Western scientific tradition. KR was an undergraduate honours student in Psychology at the time of study completion, who also worked as an Advanced Care Paramedic. Her work as a paramedic meant she was exposed to individuals suffering with mental illness and this exposure typically occurred during times of mental health crisis. These experiences impart an obligation to support individuals with mental illness, but also catastrophize what living with mental illness may look like, a bias KR attended to throughout the research process through reflection and team meetings. Both KDS and DEC are faculty members in psychology, and provided support and supervision to KR. As adults, we are also all outsiders to the experiences of youth with and without learning, cognitive, and/or psychological diagnoses during the pandemic.
Results
Sample Descriptives and Bivariate Comparisons
The overall sample was predominantly White (Table 1), with a mean age (SD) of 14.63 (1.76) years. Most youth identified as cisgender girls (62.8%), with a small portion identifying as non-binary (1.3%; Table 1). Full sample demographics are presented in Table 1.
When comparing the two diagnosis groups (No Dx vs. Any Dx), there were no significant differences by SES; however, the Any Dx group was significantly more likely to be older, to identify as non-binary or a cisgender girl, to identify as White, and to live in a non-dual caregiver household, as compared to the No Dx group. In terms of COVID-19 specific variables, youth in the Any Dx group reported significantly more receipt of support resources since schools closed in March 2020, as well as higher levels of family job loss, family structure change, and family testing for COVID-19 across all waves, as compared to the No Dx group. For comparisons on these variables for groups created based on timing of when a diagnosis was received (i.e., before and/or since COVID), see Supplemental Table S1.
In analyses exploring bivariate associations between T4 CRIES-13 scores and diagnosis status, as expected, we found that youth in the Any Dx group had significantly higher CRIES-13 scores than youth in the No Dx group at T4 (Table 1). Youth in the Any Dx group also had significantly lower CYRM scores in both the peer and family support domains at T1 (Table 1).
Multivariate Analysis
As predicted, in a multivariate model exploring if T4 CRIES-13 scores were predicted by diagnosis status, we found that being in the Any Dx group was associated with significantly higher T4 CRIES-13 scores, as compared to being in the No Dx group, and over and above scores at T1 (Table 2, Column 1). In this model, we also found that age was a significant covariate, such that a one standard deviation increase in age was related to a 1.46 point increase in CRIES-13 scores at T4 (Table 2). CRIES-13 scores at T4 were also significantly higher for cisgender girls, for those who reported family job loss between T2 and T4, for those who reported higher COVID-19 related stress from T1 to T4, and for those with higher CRIES-13 scores at T1 (Table 2).
We then assessed potential moderation of this main effect by peer and family social support. First, we added CYRM family and peer social support sub-scales to our model. For both peer and family social support, we did not find a significant main effect (Table 2, Column 2). Second, we explored interactions between the two CYRM sub-scales (peer, family) and the Any Dx group (Table 2, Column 3). None of these interactions were significant. As such, in this study, having a learning, cognitive, and/or psychological diagnosis was associated with a significant increase in trauma symptomology from September 2020 to June 2021 as compared to youth with no diagnosis, but this relationship was not buffered by peer or family social support.
In supplemental exploratory analysis based on diagnosis timing, we found that youth who had received a diagnosis prior to COVID-19 only, or who had received a diagnosis both prior to and since COVID-19, reported significantly higher CRIES-13 scores at T4 (Supplemental Table S2). There was not a significant association between receiving a diagnosis since COVID-19 and CRIES-13 scores at T4 (Supplemental Table S2). As in our main analyses, we also did not find any effect moderation by social support in these supplemental models (Supplemental Table S2).
Discussion
This study investigated if having a self-reported learning, cognitive, and/or psychological disorder diagnosis influenced trauma symptomology in adolescents in the context of the first full academic year of the pandemic, and if social support moderated this potential effect. In our large, longitudinal sample of youth from Western Canada, we found that participants with a self-reported diagnosis had significantly elevated trauma symptomology in June 2021, as compared to those with no diagnosis and controlling for trauma symptomology at the beginning of the 2020/2021 school year and other COVID-related stressors. Exploratory analyses suggest this finding was driven by youth who had a diagnosis prior to COVID-19. However, we also found that neither peer nor family social support moderated against this risk for increased trauma symptomology.
Our first hypothesis was confirmed. This finding aligns with the limited prior literature showing that mental health-related diagnosis may have placed adolescents at a higher risk of stress-related psychological problems during the pandemic (Findik et al., 2022; Zhang et al., 2021). Our findings are also consistent with research conducted in adults, in that individuals with pre-existing mental health conditions were found to have an increased risk for mental health complications during the pandemic (Buneviciene et al., 2021; Miller et al., 2021; Neelam et al., 2021). Our study adds to this literature by demonstrating that the increased risk for poor outcomes is not limited to a specific diagnosis, and using longitudinal data.
Our second hypotheses were not supported. The lack of moderation by peer and family support was initially surprising given that previous research quite consistently indicates that social support is a protective factor for adolescents (Dumont & Provost, 1999; Magson et al., 2020). However, considering peer support, another study conducted during the pandemic found that emotional support from peers did not buffer against PTSD symptoms in young adults, which the authors speculate may be because peers were experiencing similar struggles, leaving them with less ability to attend to the emotional needs of their friends (Liu et al., 2020). If peers are unable to attend to the emotional needs of their friends, this may then interfere with the ability of peer support to remain protective for youth in this context. We speculate this may have been captured in our sample, given that peer support data were collected in September 2020, 6 months after the start of the pandemic. In addition, another study looking at the moderating effects of social support for adults working remotely during the pandemic found that social support did not moderate the association between negative home–work interaction and loneliness (Slavković et al., 2022). The authors of this study suggested that the lack of moderation may be explained by the inability to transfer the social connectedness of the physical workplace into a remote work setting (Slavković et al., 2022). Similarly, for the youth in our sample, the pandemic may have changed the nature of peer social support when received primarily through technology-mediated interactions, such that technology was not able to fully supplement the loss of in-person interactions between peers. Finally, since the CYRM measures were created to assess social support in a “typical” (i.e., in-person, non-pandemic) setting, it is possible that this measure was unable to capture the complexity of peer social support during the pandemic.
In terms of the lack of moderation by family support, it is possible that the stress and strain experienced during the pandemic interfered with this resource (Fegert et al., 2020). Specifically, the Any Dx group experienced significantly higher levels of family job loss during the pandemic, as compared to the No Dx group. Experiencing job loss during a time of economic uncertainty threatens to negatively impact caregiver wellbeing, and their subsequent ability to provide support, and may have contributed to the lack of moderation in this sample. Also, we found that youth in the Any Dx group were significantly more likely to experience a family structure change during the pandemic (specifically that extended family and siblings moved into their home during the 2020/21 school year; data not shown). These family structure changes may have led to disruptions in parent-child relationships, contributing to the lack of moderation and overall lower family support reported by this group. Considering social support more broadly, in our prior work with these data, we found that Asian youth who more strongly derived support from educational, spiritual, and cultural resources had higher COVID-19 stress than Asian youth who depended less on these resources for support, which we feel highlights the contextual nature of social support, such that the circumstances of the pandemic may have altered the meaning or effect of these usually protective variables (Exner-Cortens et al., 2022).
Limitations
A key limitation is our measurement of learning, cognitive, and/or psychological disorder diagnosis in this sample. First, although we asked whether this diagnosis was received from a psychologist or other medical professional, our data are ultimately self-report and thus may over- or underestimate actual diagnoses in this sample. We were unable to verify (e.g., using health records) the self-reported diagnosis provided by our participants. For any diagnosis made prior to COVID-19, there may also be recall bias. Second, as we were limited in the number of questions we could ask on each survey, we were only able to add two single items to our T4 survey to assess diagnosis, meaning we cannot differentiate between the well-being of youth with learning, cognitive, or psychological disorder diagnoses. We also recognize that the number of actual disorders by type in our sample is unknown. Given the emerging nature of research during the pandemic, we also only added these two items at T4. Although we acknowledge that the use of a retrospective, self-report, single item measure to assess such diagnoses has limitations, given the lack of longitudinal research on trauma symptomology during the pandemic, and the even smaller amount of work looking at person-centered questions within longitudinal data, we still believe our data are an important addition to the literature. We strongly encourage future longitudinal research by investigators who are able to disentangle the differential effects of different diagnoses on mental health and well-being outcomes in the post-pandemic period.
In terms of sample representativeness, we note that we had an ~3.5% consent rate across all four boards, which is not unusual in school-based research, especially during a time of heightened stress like the pandemic. However, this is a limitation of our sampling strategy. Retention across the four waves of data in this study was likely also impacted by the pandemic context, both in terms of the other stressors youth and families were facing (which may have impeded their desire or ability to complete surveys), and as we could not do in-person follow-up due to pandemic restrictions.
Another key limitation is that we did not have pre-pandemic data for comparison. Although we were able to look longitudinally over the course of the 2020/2021 school year, without pre-pandemic data, we are unable to say with certainty the role the pandemic played in our findings. What we are able to conclude is that youth who were at risk for poor mental health outcomes before the pandemic were especially vulnerable during the pandemic, and that these youth likely need dedicated formal and informal supports. This sample only included youth attending school in four urban districts in two large Western Canadian cities, and thus we are missing important perspectives of suburban and rural youth. Although the pandemic disrupted all youths’ access to resources, larger urban centers typically had greater availability of supports for youth, and so exploring the well-being and resource needs of rural youth during and post pandemic is a critical task for future research (Brausch et al., 2023).
Finally, as we were interested in assessing if the participant’s perception of social support, measured at the same time as the initial assessment of trauma symptoms (i.e., T1), moderated trauma symptoms 1 year later, we only explored moderation by CYRM scores at T1 in these analyses. However, as described above, we recognize that social support (and more broadly, youth resilience) is a dynamic and contextual experience, which can fluctuate over time (Exner-Cortens et al., 2022; Ungar & Theron, 2020). Thus, we may have found different results if we had explored moderation by social support at different timepoints.
Relevance to the Practice of School Psychology
This study aimed to identify youth who were at elevated risk for trauma symptomology during the first full academic year of the COVID-19 pandemic. We found that youth with an existing learning, cognitive, and/or psychological disorder diagnosis were at significantly higher risk for trauma symptomatology across this year, and that this risk was not buffered by peer or family social support. Thus, school psychologists should be aware that these youth may be especially vulnerable to poor mental health outcomes in the post-pandemic period, and were also disproportionately at risk for other factors that can contribute to worsening mental health (e.g., family economic uncertainty).
Together, our findings highlight that youth with a learning, cognitive, and/or psychological disorder diagnoses, and the families and communities they reside in, need school mental health supports at the micro and macro levels in the post-pandemic period. At the micro level, schools can adopt and implement trauma-informed approaches, as well as ensure linkage to mental health supports both within and outside of the school setting (e.g., to school psychologists and school social workers). For example, Chafouleas et al. (2016) present a trauma-informed mental health service delivery framework that can be used to guide these efforts within schools. At the macro level, ongoing post-pandemic policy supports at the school level and beyond for youth, families, and communities remain critical, including reliable and rapid access to culturally-responsive school mental health services. In addition, school psychologists and other school mental health providers can join advocacy efforts for a national mental health strategy for children and youth in Canada (Vaillancourt et al., 2021). In sum, to promote post-pandemic well-being in this vulnerable subgroup of youth, access to holistic mental health supports, and continued advocacy, is needed.
Supplemental Material
sj-docx-1-cjs-10.1177_08295735251336409 – Supplemental material for Trauma Symptomology During COVID-19 Among Youth with a Learning, Cognitive or Psychological Disorder Diagnosis: Exploring Moderation by Social Support
Supplemental material, sj-docx-1-cjs-10.1177_08295735251336409 for Trauma Symptomology During COVID-19 Among Youth with a Learning, Cognitive or Psychological Disorder Diagnosis: Exploring Moderation by Social Support by Keri Rempel, Kelly Dean Schwartz and Deinera Exner-Cortens in Canadian Journal of School Psychology
Footnotes
Acknowledgements
Thank you to the participating school divisions, youth, and families, and to Mitch Rath and Jodi Gibson, for their support of this project.
Data Availability
Please contact the second author (Dr. Schwartz) for questions about data availability.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a Canadian Institutes of Health Research (CIHR) Operating Grant: COVID-19 MS & Substance Use – Matching Access to Service with Needs (Dr. Schwartz) and by the Canada Research Chairs program (Dr. Exner-Cortens).
Ethical Approval
This research was approved by the University of Calgary Conjoint Faculties Research Ethics Board (CFREB) and the participating school divisions. All youth under age 18 required written parent/guardian consent, and also provided their own assent prior to participation.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.