
Abstract
Elementary public schools remain the most common venues for addressing children’s severe conduct problems. Nevertheless, very few longitudinal studies have examined association between receiving psychoeducational services for conduct problems in school and subsequent conduct problem severity. This study explored if psychoeducational service reception contributed to reduce conduct problems in a sample of 434 elementary school-aged boys and girls presenting a high level of conduct problems. The study used a repeated measures design at 12-month intervals, for 4 years. Information regarding the severity of children’s conduct problems and services was provided by parents and teachers. Latent Growth Modeling was used to identify a mean trajectory of conduct problems. Results revealed that psychoeducational services were associated with a decrease in conduct problems over time, but this association was only observed in boys. There was no association between service reception at study inception and the trajectory of conduct problems among girls. These results suggests that psychoeducational services are well suited to the difficulties of boys with conduct problems; however, they may call for a review of the services offered to girls in schools, both in terms of the detection of conduct problems in young girls, and in terms of their treatment options.
Keywords
Conduct problems (CP) refer to a variety of antisocial or externalizing behaviors, including peer aggression and bullying, rule breaking, as well as defiance and opposition to authority (American Psychiatric Association, 2013). Boys and girls who show high levels of CP in childhood are at elevated risk of maintaining a high level of CP overtime and experiencing a chain of negative events that may extend into adolescence and adulthood (Bevilacqua et al., 2018). It is, thus, important to intervene in childhood to reduce CP and their related consequences.
Public schools remain the most common venues for addressing children’s CP (Costello et al., 2014; Georgiades et al., 2019) and at the elementary level, CP are a common reason for which teachers seek support from school professionals (Briesch et al., 2013). Though the support services vary in their designation and may differ from one province or territory to another (Tremblay & Belley, 2017), they are commonly offered under special or psychoeducational services and implemented by mental health professionals (e.g., school psychologists, school counselors) following an individualized service plan. 1 These services, which include formal assessments of behavioral difficulties and/or psycho-social and educational needs, aim to help children attain learning-related and socialization goals, and to assist children in a variety of different ways, including with their behavioral adjustment (e.g., behavioral intervention and support, psychological services, and coaching in order to assist teachers with behavioral management in class; Gaudreau et al., 2020).
Considering the negative life consequences that are associated with severe CP in childhood and the central role psychoeducational services may play for children who present CP, it is important to know if these services offered at elementary schools help minimize CP over time. A review of the literature revealed however, that very few longitudinal studies have been conducted among school-aged children with CP to examine the effects of psychoeducational services on the evolution of CP, and those that have not produced encouraging results (e.g., Lane et al., 2005; Mattison & Spitznagel, 2001; Siperstein et al., 2011). 2 These studies failed to find any significant improvement in CP over time following reception of “special educational” services. However, the relatively small sample sizes of these studies (Ns all less than 86) and the absence of a comparison group (e.g., children with significant CP but who do not receive services) limits our capacity to compare progress of children with CP at baseline. Two large community-based studies compared children receiving “special educational” services for a variety of needs (not uniquely for CP), to those not receiving services on the evolution of CP or externalizing problems (Dempsey et al., 2016; Morgan et al., 2010) and found either a negative or no predictive effect of services on later problems. However, these results would need to be replicated among a more homogeneous group with CP. In addition, the comparison groups in these studies were children who were not receiving services, regardless of the presence of CP.
It is well documented that the greater the level of a child’s CP, the more likely it is that a child will receive psychoeducational services at school (Burnett-Zeigler & Lyons, 2012; Little & McLennan, 2010). Children with CP who do not receive psychoeducational services at one time point would still have a high chance of receiving services in the future (Kulkarni & Sullivan, 2019). Thus, a study aimed at longitudinally examining the effect of psychoeducational services on a sample of children with CP would need to control for service reception over time.
None of the previously described studies examined the differences between boys and girls with CP receiving psychoeducational services. More boys with CP than girls receive these services in schools (Anderson et al., 2015; Forness et al., 2012; Smeets & Roeleveld, 2016), which may be only partly related to the increased prevalence of CP in boys (Ghandour et al., 2019). Indeed, studies have shown that at similar levels of CP, fewer girls are referred for school services (Costello et al., 2014; Coutinho et al., 2002). Further, in the diverse clientele receiving psychoeducational services, studies have shown that girls receive services over a shorter period of time (Holt et al., 2007; Verlaan et al., 2018) and less intense treatment than boys (e.g., Burnett-Zeigler & Lyons, 2012;). Thus, it is important to know if the association between psychoeducational service reception and CP is the same for boys and girls.
The Current Study
In a sample of elementary school-aged children presenting with CP, the present longitudinal study aimed to investigate the effect of psychoeducational services for CP at study inception on the evolution of CP severity over 4 years (five measurement time points), while also controlling for psychoeducational service reception at later time points. The study also examined differences between boys and girls in these associations. This study contributes to our understanding of the links between CP and psychoeducational services by limiting the sample to children with CP, including a roughly equal proportion of boys and girls, and children both receiving and not receiving services at study inception. Given the correlational and longitudinal nature of our research design, data were analyzed using latent growth models, which allowed the observation of the effect of a predictor on the evolution of a dependent variable over time.
Method
Participants
Participants were selected in 155 public schools from eight school boards in Quebec. The sample included 434 students with CP aged 6.3 to 9.9 years (mean age of 8.4 years) at the time of recruitment (Time 1). Among these children, 339 received psychoeducational services for CP (i.e., CP was the primary reason for referral), and 95 did not.
The selection of
Measures
Conduct Problems
The DSM-Oriented scale for CP (Achenbach & Rescorla, 2001) was used at study inception and at each of the four follow-up time points. The scale is comprised of 17 items (Child Behavior Checklist; parent report; α = .90) and 13 items (Teacher Report Form; α = .92), which are rated on a three point Likert scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true). Examples of items included “Cruelty, bullying, or meanness to others,” and “Breaks rules at home, school, or elsewhere.” While not being a diagnostic instrument, these scales are accompanied with norms and clinical cutoffs (T scores between 65 and 69 correspond to borderline clinical range, while those over 70 are over the clinical cutoff). Since CP in children are known to be context-specific (De Los Reyes et al., 2019), we retained the highest T score between the parent and the teacher at every assessment in order to tap the full amplitude of the child’s CP. This multi-informant approach has been identified as providing an optimal balance between sensitivity and specificity in the assessment of CP compared to the use of a single informant score or of a parent-teacher mean score (Lapalme et al., 2020).
Psychoeducational Services
At study inception, the reception of psychoeducational services for CP was determined using official school board records. The reception of these services according to school board lists was confirmed by 94% of parents whose children participated in the study. The non-reception of psychoeducational services was determined if children did not appear on official records and parents reported no reception of psychoeducational services for CP since school entry. At each of the four follow-up time points, it was both parents and teachers who gave information on psychoeducational service reception. A child was considered to be receiving services if either parents or teachers reported that the child had received services for CP at school.
Control Variables
Age of the child at baseline and annual family income were used as covariates in the analysis.
Procedure
All procedures of the current study were approved by the University Research Ethics Board. After receiving signed consent from parents, graduate-level students administered questionnaires to parents at their home and obtained parental consent to contact the child’s teacher. Teacher reports were completed by telephone. The initial assessment (Time 1) was followed by an assessment every 12 months over a 4-year period (Time 2 to Time 5).
As expected, some children who did not receive psychoeducational services at Time 1 did receive services at later time points (specifically, 19.1% at Time 2, 30.4% at Time 3, 29.0% at Time 4, and 37.8% at Time 5). Conversely, some children who received services at Time 1 did not continue in services at later time points (specifically, 17.7% at Time 2, 17.9% at Time 3, 23.2% at Time 4, and 23.8% at Time 5). Of those 339 students receiving services at T1, 148 continued receiving services throughout the five assessment time points (43.7%). Among the 95 students who did not receive services at T1, 41 (43.2%) never received services.
Data Analytic Strategy
Latent Growth Modeling (LGM) was used to identify the developmental trajectory of CP. LGM is a fixed and random coefficient modeling technique that estimates change over time in some outcome (e.g., CP) by using time-specific measures to estimate an underlying growth trajectory. The fixed effects represent the mean of the trajectory pooling of all the individuals within the sample, and the random effects represent the variance of the individual trajectories around these group means. The management of missing data using full information maximum likelihood (FIML), the possibility of including time varying covariates and the ability of LGM to parse out the variances in both intra and inter individual manners in order to evaluate individual change as a function of time (Voelkle, 2007) were the factors that guided us to select LGM as the ideal data analytic technique.
Over five measurement time points, 5.9% of responses were missing; however, we used the FIML method since the data were missing at random as confirmed by Little’s test (Chi-square = 66.76, df = 59, p = .228). All models were estimated using Mplus 8.8 (Muthén & Muthén, 1998-2022). As suggested in the literature (Hu & Bentler, 1999; Marsh et al., 2005), an adequate to excellent model fit may be indicated by values respectively greater than 0.90 and 0.95 on the comparative fit index (CFI), and Tucker-Lewis index (TLI) and by values lower than 0.08 and 0.05 on the mean square error of approximation (RMSEA). A non-significant Chi-square test is another indicator of good model fit; however, the Chi-square test is sensitive to large sample sizes (Kline, 2015).
The analyses were carried out in three steps. First, the base model was estimated using LGM to describe the longitudinal trajectory of CP through the five measurement timepoints. This analysis identified two latent factors, the intercept and the slope. This first step was carried out on the entire sample as well as among boys and girls using the multi-group technique. Both linear and a quadratic models were tested and compared in order to retain the trajectory shape that best fit the data. The inclusion of a quadratic term did not significantly improve model fit for CP. A conditional model was then estimated by adding covariates to the base model (Figure 1). The covariates included use of psychoeducational services, the age of the child at study inception and family socio-economic status. This model was tested on the overall sample as well as among boys and girls separately, again via the multi-group model. Finally, comparison of coefficients analysis was performed across groups to verify whether the effect of the psychoeducational services on the CP trajectory was the same in boys and girls. This analysis was carried out within the multi-group model via the model test function of MPlus.
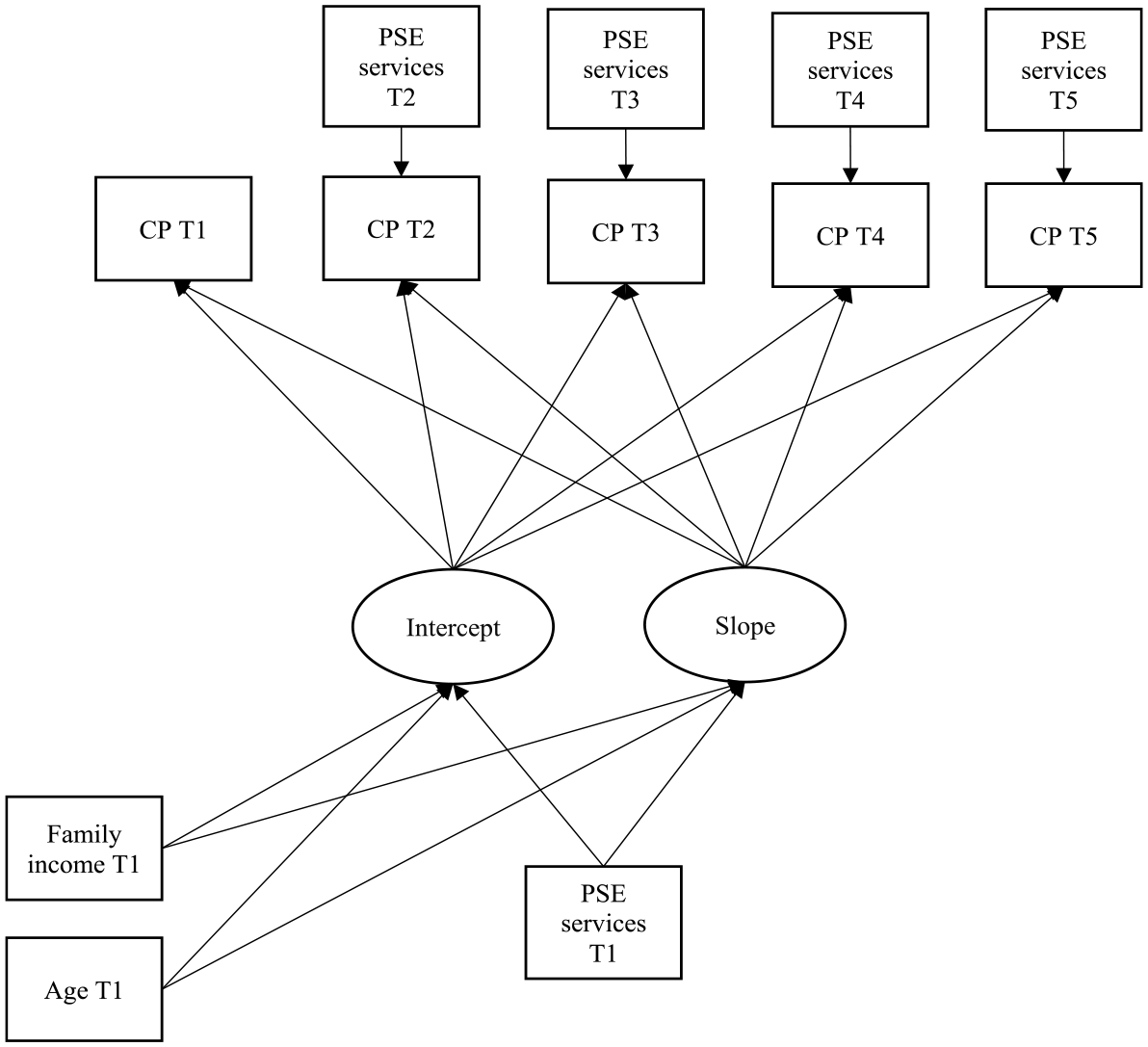
Conditional model.
Results
Descriptive statistics and correlations are shown in Table 1. Mean CP scores for both boys and girls are in the clinical range at Time 1, and progressively decline into the borderline clinical range. CP scores were equivalent between boys and girls for Times 1 through 4 but were higher in girls in Time 5. As indicated by high correlations between scores at different measurement time points, individuals seemed to retain their relative position across the years. The stability at the aggregate (group) level does not imply, however, that there was no change at the individual level. Individual rates of stability (or change) were examined next by growth curve analysis.
Descriptives and Correlations.
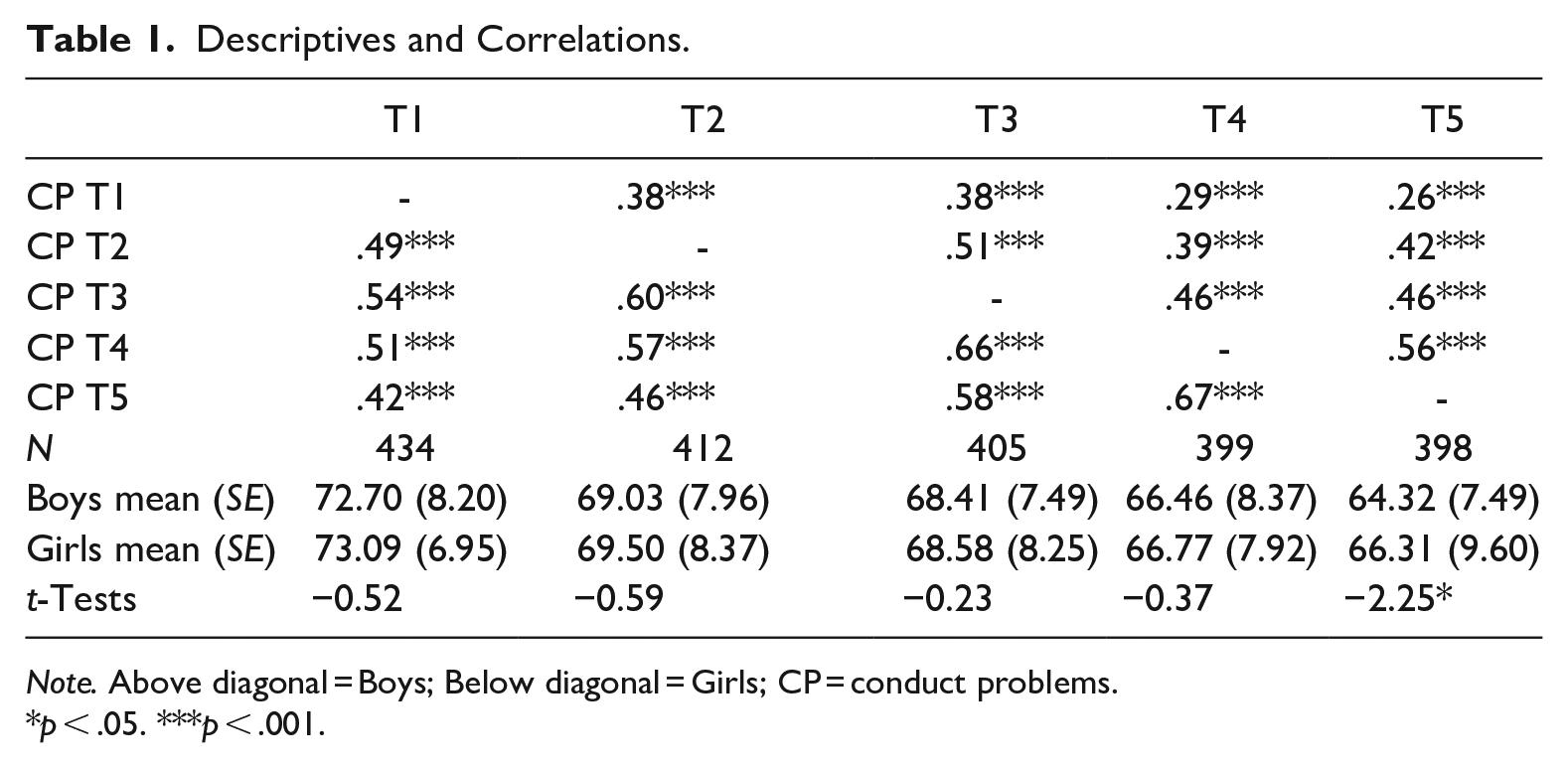
Note. Above diagonal = Boys; Below diagonal = Girls; CP = conduct problems.
p < .05. ***p < .001.
Base models presented good model fit (Table 2). These models indicated that CP significantly declined over time. The conditional models including the covariates are shown in Table 3, and have good model fit. These models showed that, at study inception, the reception of psychoeducational services at school was positively associated with CP severity; children who received services presented higher levels of CP than those who did not, and this was found among both boys and girls equally. The reception of psychoeducational services at times 3, 4, and 5 was also positively associated with CP severity cross-sectionally, which indicates that those children receiving services are those with higher levels of CP. 3 However, these correlations were stronger among boys than among girls at times 3 and 4. In addition, the reception of psychoeducational services at study inception was associated with a decrease in CP over time (slope); however, this effect was only present among boys. No association between the reception of psychoeducational services and the evolution of CP was found for girls.
Base Models.
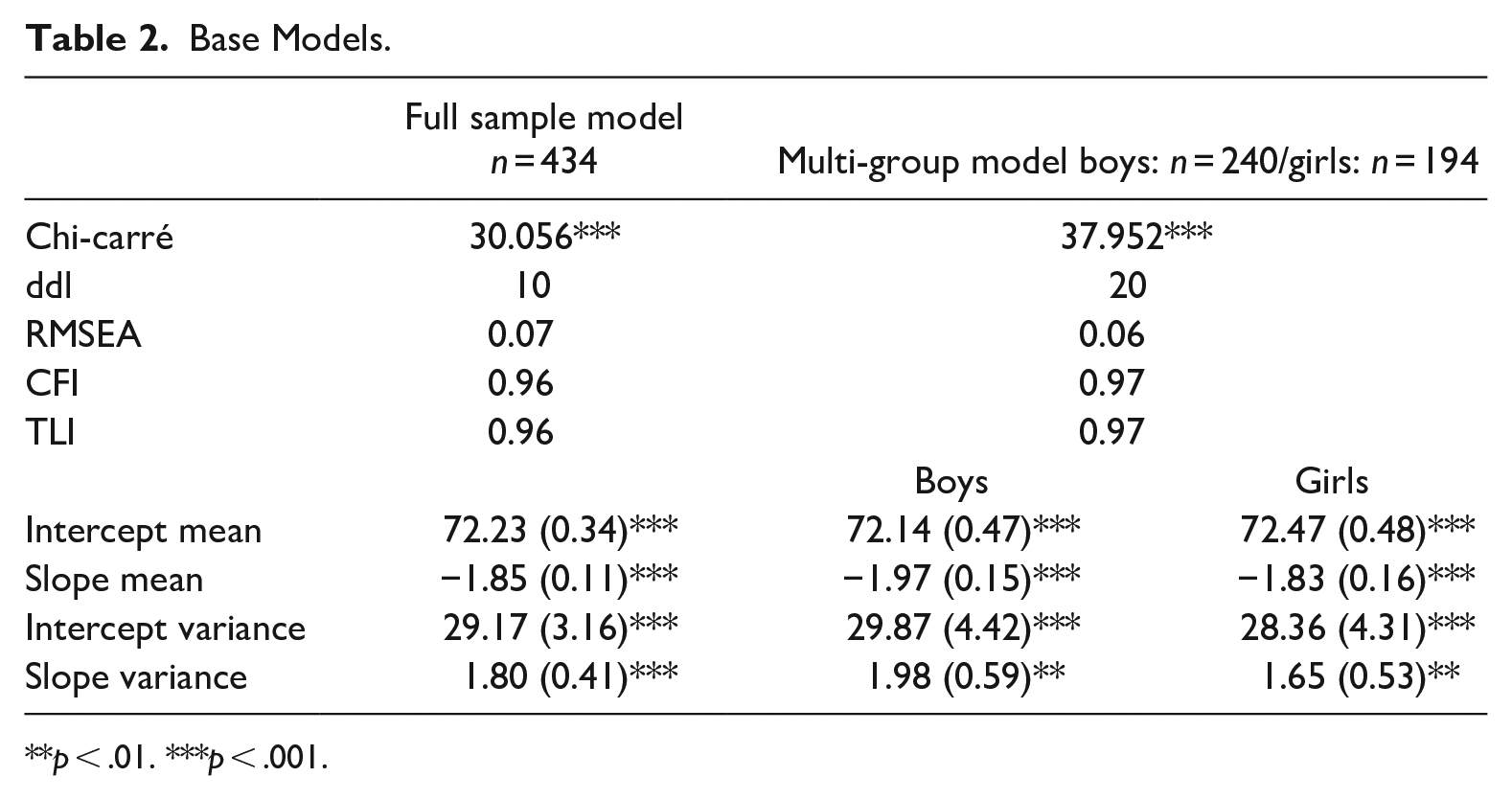
p < .01. ***p < .001.
Conditional Models.
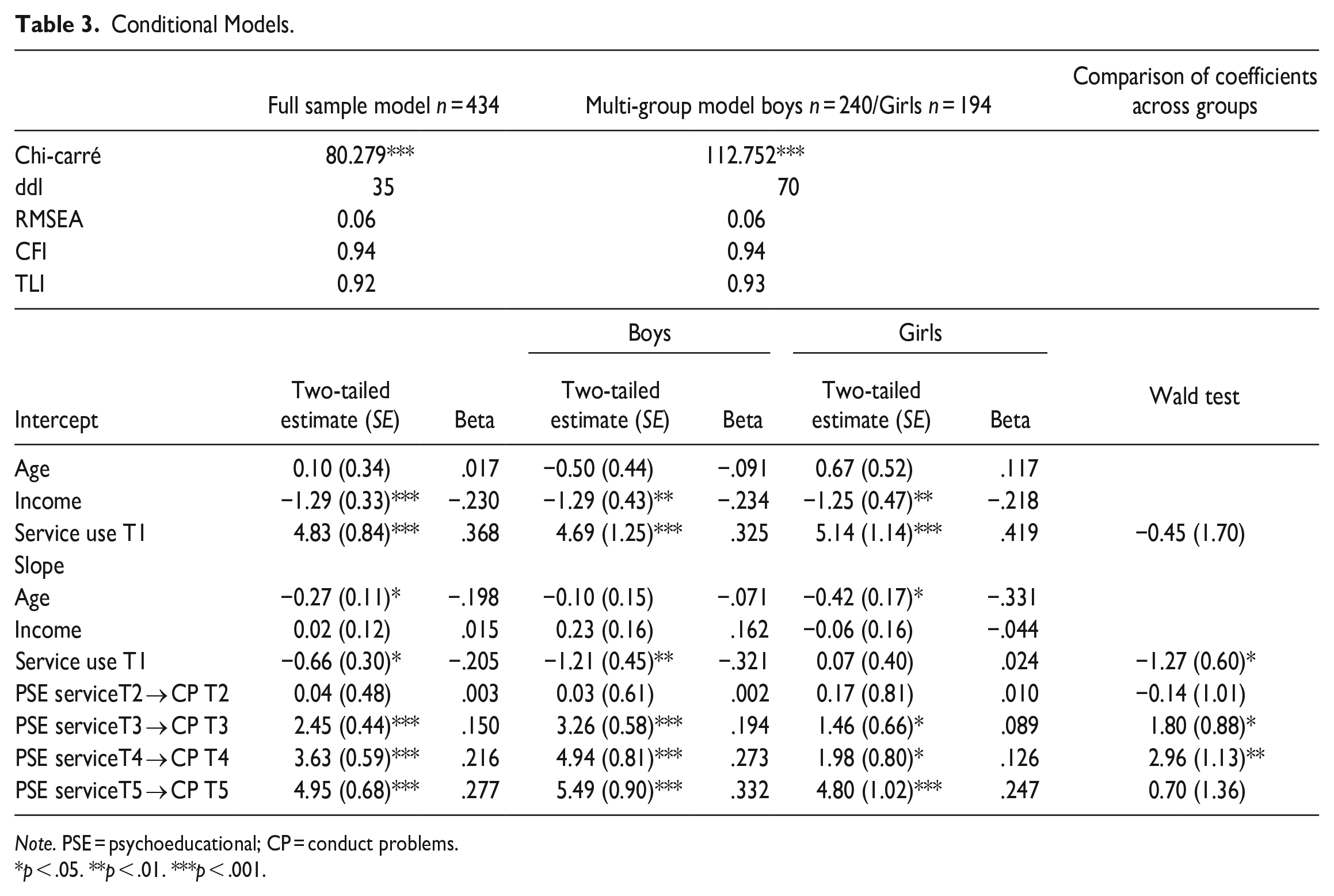
Note. PSE = psychoeducational; CP = conduct problems.
p < .05. **p < .01. ***p < .001.
Discussion
Given the important role schools play in addressing children’s CP (Costello et al., 2014; Georgiades et al., 2019), it is important to know if these services are effective in reducing the severity of CP. Our study identified three main results.
First, the study confirmed that reception of psychoeducational services at elementary school was associated with CP severity. This was observable at both study inception, where psychoeducational service reception was associated with higher level of CP, and at subsequent time points, where psychoeducational services continued to be offered in schools to children with higher CP. These results suggest, on the one hand, that children are appropriately identified at elementary schools for referral to psychoeducational services for CP. On the other hand, as noted by Siperstein et al. (2011), these results also suggest that children who receive psychoeducational services represent the most impaired of all students with CP. Indeed, in our sample, those receiving psychoeducational services had a higher level of CP than those who did not receive these services, even though both groups had a level of CP that fell over the borderline clinical range.
These results, which are consistent with the literature, could reflect both a lack of school resources or poorer screening of CP in girls. Indeed, a second finding showed that although the association between the severity of CP and the reception of services is observable in both boys and girls, this association appears less strong for girls. First, when we selected participants for this study, we observed that girls were over-represented among children with CP not receiving psychoeducational services at school (58% girls vs. 42% boys). The higher proportion of girls compared to boys who were identified via the screening of children who did not receive psychoeducational services is consistent with findings from other research suggesting that girls receive fewer services for their CP than boys (Costello et al., 2014). Next, the association between CP severity and psychoeducational service reception over time was stronger among boys than among girls. This may be another indication CP in boys are better identified for services than CP in girls.
Third, psychoeducational services were associated with a more rapid decline of CP over time among boys. In fact, the mean CP score for the boys in the study moved from the clinical range at Time 1 to just below the borderline cutoff at Time 5. This encouraging result is in contrast with results of previous studies (Dempsey et al., 2016; Lane et al., 2005; Mattison & Spitznagel, 2001; Morgan et al., 2010; Siperstein et al., 2011) which found no improvement in CP after reception of school services. The fact that our design employed a homogeneous group of children with significant CP who received or not psychoeducational services, might account for the fact that we were able to observe an association among boys, when other studies did not. However, this study failed to observe the same association among girls. Although the mean score for girls also declined, their decline was not associated with service reception, and they remained in the borderline clinical range. This may suggest that services are insufficient in terms of intensity or breadth of intervention in order to meet the needs of girls with severe CP. Indeed, several studies have supported the idea that interventions that lead to positive results in children with CP are intensive, target multiple domains and extend over a long period of time (Hoagwood et al., 2007; Powell et al., 2011). However, psychoeducational services in schools (i.e., not specific treatment programs) rarely incorporate several domains of a child’s life (such as the family). Given the lack of association between service reception and decreases in CP severity over time for girls with early and severe CP, one hypothesis could be that these clinical features may be even more important for the treatment of girls than boys.
Another explanation could be that services do not address appropriate targets for intervention among girls. This explanation is supported by our results, which showed that the association between the reception of school services and the severity of CP over time was less strong among girls. Services may target only a subset of symptoms of CP, possibly neglecting those presentations more typically manifested among girls with severe CP, for example indirect aggression (Boutin et al., 2021). Further, school services for CP may neglect traits underlying severe CP, such as callous-unemotional traits, which have been shown to be more highly resistant to intervention (Levine et al., 2022) and which are less consistent with feminine gender stereotypes. In addition, girls with CP may have more comorbidities than boys with CP (e.g., depression, Costello et al., 2003). However, these difficulties (indirect aggression and depression) are typically more difficult to detect in school settings.
Study Strengths and Limitations
The current study has several strengths including the longitudinal nature of the study design, the homogeneity of the sample composed only of students with CP in childhood, the presence of children who received or did not receive psychoeducation services at study entry, and the large number of girls with CP referred for these services. The interpretation of the findings should take into account some methodological limitations. First, given that our sample comes mostly from schools located in disadvantaged neighborhoods, and that CP is disproportionally identified in children from low socio-economic backgrounds (Shaw & Shelleby, 2014), our results describing the association between service reception and later CP may not be generalizable to children with CP from more advantaged backgrounds. Second, the study followed children with CP over a period of 4 years of elementary school. As such, it is impossible to know if these services may have delayed effects during the transition to secondary school. Third, although the longitudinal design allows for temporal ordering of events, causal conclusions cannot be drawn based on the design, which is correlational.
Our goal in this study was to evaluate whether the reception of psychoeducational services at school was related to the developmental trajectory of CP, not to evaluate any specific intervention. In other words, once a child is identified and receives psychoeducational assistance at school, are these services associated with a reduction in CP severity? However, psychoeducational services offered in schools are typically highly variable as they are offered following a detailed individualized plan. Therefore, they are difficult to record and for parents and teachers to recount accurately (e.g., the frequency or duration of each meeting). Given this limitation, we do not have specific information on the content of the services or their frequency. In addition, as previously discussed, there was variability in the reception of services over the 4 years of the study. Thus, a more fine-grained analysis of the types of services that may or may not be helpful, especially for girls, would be beneficial in adapting services for youth with CP.
Relevance to the Practice of School Psychology
Overall, results suggest that psychoeducational services in elementary schools are associated with reductions in CP severity among boys. This suggests that these services are well suited to the problems of boys with CP. However, our results may call for a review of the services offered to girls in schools, both in terms of the detection of CP in young girls, and in terms of their treatment options. In addition, giving increased attention to those symptom presentations that may be more prevalent or representative of the behavioral repertoire of girls than boys with CP (e.g., depressive symptoms or indirect aggression), or which differ more from gender-based expectations for girls (e.g., callous-unemotional traits) may be relevant. Further, since several children who did not receive psychoeducational services at study inception did go on to receive services at later time points, a more systematic detection of CP among schoolchildren may be relevant in order to detect difficulties earlier, offer treatment, and prevent negative consequences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (82694), and by the Social Sciences and Humanities Research Council (435-2012-0803).