
Abstract
School disruption (SD) places students at risk of early school departure and other negative psychological outcomes. Based on the data derived from a sample of Ontario children and youth, this study aims to identify risk factors associated with SD among 1,241 school-aged students. A logistic regression model revealed that substance use, family functioning, Attention Deficit/Hyperactivity Disorder and experiencing bullying, significantly predicted SD. Substance use and family functioning resulted in the largest contributions to SD when holding other variables constant. This study provides supporting evidence of risk factors predicting SD and suggests that mental health and school personnel should consider family functioning and substance use in particular, when creating interventions to decrease premature school termination.
Introduction
School disruption (SD), conceptualized as interruptions of “learning conditions, teaching environment or relationships in school” (Veiga, 2011, p. 469), creates many complications for children and youth (hereafter referred to as children). Children acquire skills necessary for long-term success related to academic, social, and civic skills when actively involved in school. Disruptions in academic trajectories, may result in excessive absenteeism which has been linked to lower academic performance, involvement with the juvenile system, and permanent school dropout (Finning et al., 2019). Moreover, Canada has one of the highest school-absence rates in the world since one in four teenagers avoid attending regularly (Alphonso, 2018).
There have been several efforts in understanding students’ engagement in school. However, the current literature is limited due to conceptual and measurement issues surrounding SD. One of the major challenges in studying this construct is the variety of narrow definitions that have been used to discuss student engagement (Li, 2011). As a result, existing measurement instruments have a specific focus on either behavioral, emotional, or cognitive dimensions of the phenomenon (Veiga, 2011; Wang & Holcombe, 2010). Furthermore, outcomes in several SD studies have focused exclusively on academic consequences (Li, 2011), disregarding the multidimensional nature of SD and the overall impact on children’s development (Li, 2011; Veiga, 2011).
Grounded in relational developmental systems framework (Lerner et al., 2015), it is necessary to study SD from multiple perspectives. According to this framework, children’s development is shaped by associations among environmental factors, interpersonal relationships, and opportunities in a variety of contexts. These elements are moderated by the child’s “physical, psychological, cognitive, social, and emotional processes” as they foster or undermine learning (Darling-Hammond et al., 2020, p. 97). Within this framework, the current study aims to investigate social, psychiatric, and individual risk factors on SD.
Social Characteristics
Complex family factors have been associated with SD. Disengaged students experience family dysfunction more so than engaged peers (Carless, 2014). Children with conflictual family relationships tend to have compromised peer relationships as well (Auerbach et al., 2014), placing them at greater risk of engaging in or experiencing bullying and victimization (Ward et al., 2018). Bullying contributes to poor socio-emotional adjustment, academic underachievement, higher rates of substance use, increased aggression, internalizing problems (IP); marked by symptoms of guilt, worry and social withdrawal (Rooney et al., 2013) and externalizing problems (EP); marked by aggression, non-compliance, and behavioral disruption (Rooney et al., 2013; Shetgiri, 2013). Such environments increase rates of problematic relationships among students and school personnel, thereby contributing to school refusal (Carroll, 2011).
Psychiatric Characteristics
Among psychiatric characteristics that may be related to SD are IP, EP, Attention Deficit/Hyperactivity Disorder (ADHD) and substance use. IP such as depression, are among the most common mental health (MH) problems in childhood (Pedersen et al., 2019). Students experiencing depression are more likely to avoid challenges and engage in more ineffective learning strategies than non-depressed counterparts (Quiroga et al., 2013). Similarly, students with EP such as aggression have been found to have higher rates of SD (Vaughn et al., 2011). Moreover, students with ADHD typically exhibit a variety of behaviors characterized by attentional problems, distractibility, impulsivity and hyperactivity that negatively impact classroom and academic performance (Dupaul & Jimerson, 2014). Previous literature has highlighted associations between SD and substance use. For example, disengaged students were found to be nearly three times more likely to have an alcohol/cannabis use disorder or nicotine dependence when compared to non-disengaged students (Vaughn et al., 2011).
Individual Characteristics
The expression of school refusal changes as children develop. Often, refusal becomes absenteeism as children enter secondary school. SD has been found in both males and females (Munkhaugen et al., 2017) with research suggesting that males in middle school show greater decreases in school bonding compared to females (Zaharakis et al., 2018).
Present Study
The extant SD literature is limited due to conceptual and measurement issues. Despite evidence supporting the relationship between SD and particular risk factors, a multidimensional research perspective is needed to better understand this construct (Li, 2011). A thorough exploration of SD can contribute to identifying factors alleviating these behaviors while providing clues about implementation of effective intervention programs boosting healthy development and school attendance. To our knowledge, this is the largest study to utilize a new, standardized instrument examining risk factors associated with SD across various domains. Based on the extant literature, it was predicted that (1) exhibiting IP, EP, ADHD, substance use, poor family functioning, and experiencing victimization would exert varying degrees of impact of SD and; (2) SD was expected to increase with age.
Method
Participants
This study consisted of 1,241 students from 4 to 18 years of age (M = 11.08, SD = 3.44) who were assessed as part of standard of care, when seeking services from 10 mental health agencies in Ontario, Canada. All agency referrals were made through family physicians, pediatricians, parents, school personnel or other allied professionals. In the total sample, there were 802 males and 439 females. In Table 1, the general distribution of the variables is illustrated by SD. Of the 1,241 children who participated, 796 exhibited SD. The median score for IP and EP was greater for children exhibiting SD compared to non-disrupted counterparts.
Sample Characteristics by SD and Non-SD.
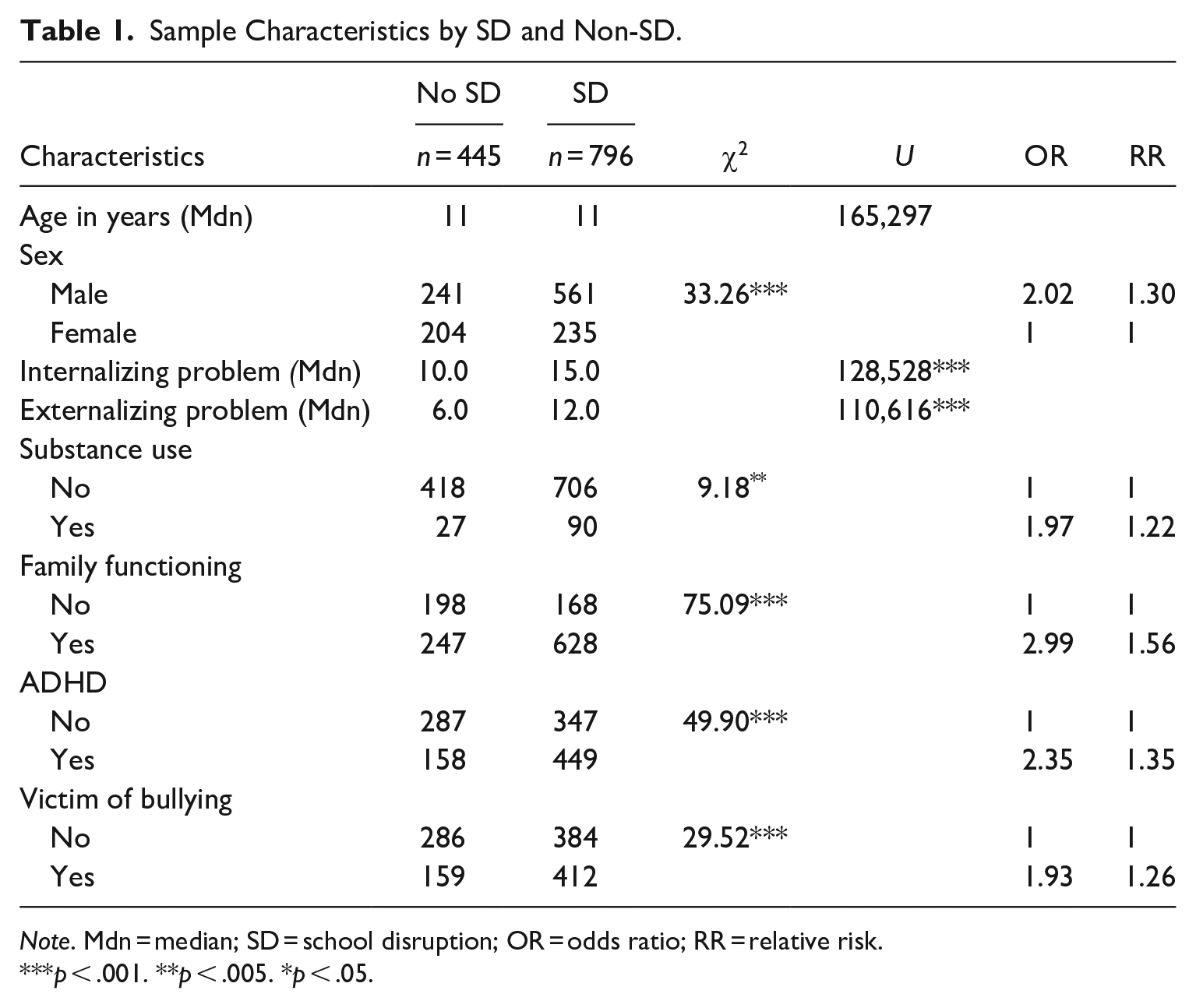
Note. Mdn = median; SD = school disruption; OR = odds ratio; RR = relative risk.
p < .001. **p < .005. *p < .05.
Independent and Dependent Measures
Comprised of approximately 400 clinical elements, the interRAI ChYMH (Stewart, Theall et al., 2015) gathers information covering medical, psychological, social and environmental issues impacting child functioning. This clinician-rated instrument has been validated in a variety of care settings and uses items with a 3-day look back period although some items use a 7-day, 90-day or lifetime estimate depending on the issue. A limited number of self-report items are also included (see Hirdes et al., 2020). Similar to other studies, standardized measures and items reflecting the construct of interest within the interRAI ChYMH were utilized (e.g., Stewart, Thornley et al., 2020).
The interRAI ChYMH is part of an integrated health information assessment system exhibiting strong reliability and validity (Lau et al., 2018, 2019, 2021; Li et al., 2021; Phillips et al., 2012; Stewart & Hamza, 2017; Stewart & Hirdes, 2015; Stewart, Celebre et al., 2020; Stewart, Babcock et al., 2020; Stewart, Klassen & Hamza, 2016; Stewart, Morris et al., 2020; Stewart, Poss et al., 2019). It can also be used for program evaluation, outcome measurement, resource allocation and case-mix systems (Fries et al., 2019). The dependent measure, Risk for School Disruption Scale (RSD; Stewart, Klassen & Hamza, 2016, Stewart, Klassen & Tohvner, 2016), was created using six items. These items included: an increase in lateness or absenteeism, poor productivity or disruptiveness at school, expressed intent to quit school, conflict with staff, expression of strong, persistent dissatisfaction with school, and refusal to attend school/currently removed from school. The scale is scored from 0 to 8 with higher scores indicative of an increased risk of SD. Previous validation research has indicated that the SD scale to have adequate internal consistency (0.77), and was positively correlated with a variety scales related to school-related issues including the Child Behavior Checklist (Achenbach & Rescorla, 2001), the Basic Child and Family Phone interview (Cunningham et al., 2009) as well as the Beck-Youth Inventory (Beck et al., 2001). Similar to the previous study, the scale was categorized into the following values: 0 = SD (score of 0) and 1 = no SD (scores between 1 and 8) based on a cut-point of 1+ identifying children and youth at risk of SD and in need for early intervention (Stewart, Klassen & Tohvner, 2016).
Independent measures for this study included: IP, EP, substance use, family functioning, ADHD, victim of bullying, sex, and age were also obtained from the interRAI ChYMH.
Internalizing problems
The Internalizing Scale (IS) assessed the frequency and severity of symptoms of IP within the past 3 days. The frequency of each behavior was assessed using a 4-point scale (0 = not present to 4 = exhibited daily in last 3 days, three or more episodes or continuously), ranging from 0 to 52. This scale exhibited strong psychometric properties with higher scores indicative of greater IP (Lau et al., 2019).
Externalizing problems
Similarly, the Externalizing Scale (ES) assessed the frequency and severity of EP within the past 3 days. The frequency of each behavior was assessed using a 4-point scale (0 = not present to 4 = exhibited daily in last 3 days, three or more episodes or continuously), ranging from 0 to 32. This scale exhibited strong psychometric properties with higher scores indicative of greater EP (Lau et al., 2021).
Substance use
Substance use was defined as consumption of alcohol to the point of intoxication, or use of inhalants, hallucinogens, cocaine or crack, stimulants, opiates, or cannabis over the last year. Intentional misuse of prescription or over-the-counter medication in the last 90 days was also included in the composite variable. Items were endorsed as yes or no with respect to engagement in substance use.
Family functioning
The family functioning scale incorporates six items including: strong and supportive relationship with family (inverse scored), family is persistently hostile or critical of child, family members report feeling overwhelmed by child’s condition, parent/primary caregiver was unable/unwilling to continue caring, parent/primary caregiver or sibling(s) had current developmental, MH or substance use issues. Scores range from 0 to 6 with higher scores indicative of weaker family functioning. For this study, the scale was categorized into the following values: 0 = no family functioning problems (score of 0) and 1 = presence of family functioning problems (scores between 1 and 6).
ADHD
The presence or absence of a diagnosis of ADHD was based on DSM-IV diagnoses obtained from psychiatrists and psychologists documented within the ChYMH.
Victim of bullying
Bullying victimization was defined as a “child subjected to repeated acts of teasing or harassment, rumors spreading about him or her, physical assault, theft of money of items, intimidation, and/or racial slurs or negative comments about his or her religion, sexual orientation, disability, body type or socioeconomic status” (Stewart, Hirdes et al., 2015; Stewart, Theall et al., 2016). This was assessed with the following options: 0 = Never, 1 = More than 1 year ago, 2 = 31 days to 1 year ago, 3 = 8 to 30 days ago, 4 = 4 to 7 days ago, and 5 = In last 3 days. Similar to other studies, children received a score of 0 for those responding never to the item and 1, if scores ranged from 1 to 5 (e.g., Baiden et al., 2017).
Demographic variables
Males were coded as 0 and females coded as 1.
Procedure
Data were collected between November 2013 and February 2015 using the interRAI Child and Youth Mental Health (ChYMH) and the Adolescent Supplement assessment system (Stewart, Hirdes et al., 2015). Each assessor, who had at least 2 years of clinical experience working with children, received a 2-day training program focused on the administration of the instrument. Assessors ranged in discipline and included psychologists, nurses, psychiatrists, child and youth workers, speech and language therapists, resource teachers, and social workers. Through a semi-structured interview, either in person or over the telephone, information from a variety of sources (e.g., family members, clinical observations) were entered into a de-identified, web-based software system that was password protected and encrypted, providing each case a randomly assigned study-specific participant number. Approval for the secondary analysis was granted through the university’s ethics board.
Data Analysis
Statistical analyses were performed using SPSS software, version 22 (SPSS, Chicago, IL, USA). Bivariate analyses of chi-square and Mann-Whitney tests were conducted to identify the relationship between SD and several risk factors. All assumptions related to sample size, multicollinearity and linearity of the logit were conducted to assess data suitability for use with multivariate analyses. A binary logistic regression was then performed to examine the probability of SD given the factors previously highlighted. For all analyses, the statistical significance level was 0.05 and adjusted odds ratios were considered statistically significant if associated confidence intervals did not include a value of 1.0.
Results
Bivariate Results
For categorical variables, chi-square tests were conducted to examine group differences between children with and without SD. For continuous data, Mann-Whitney tests were used to examine the group differences because age, IP and EP were not normally distributed, violating the assumption of the independent t-test (Field, 2009). Table 1 displays the results with p, U, and chi-square values.
A significant association between sex and SD was found (χ2 = 33.26, df = 1, p < .001) such that the proportion of male participants with SD (69.5%) was greater than females (53.5%). Family functioning was significantly associated with SD (χ2 = 75.09, df = 1, p < .001). Among participants with family functioning problems, 71.8% experienced SD in contrast to the 45.9% without family functioning problems experiencing SD. There was also a significant relationship between bullying and SD (χ2 = 29.52, df = 1, p < .001). Among victims of bullying, approximately three quarters (72.2%) experienced SD.
Mann-Whitney tests for IP (U = 128,528, z = −8.03, p < .001) and EP (U = 1,10616, z = −10.99, p < .001) resulted in significant relationships with SD. Children with greater IP and EP scores were more likely to experience SD. In addition, there were significant relationships between substance use (χ2 = 9.18, df = 1, p < .005), ADHD (χ2 = 49.90 df = 1, p < .001) and SD. Students utilizing substances were more likely to experience SD than non-users. Students with ADHD were more likely to experience SD (74%) than students without (54.7%). Results did not indicate a significant relationship between age and SD.
Multivariate Results
Despite several variables being significantly associated with SD at the bivariate level, those results did not control for the effect of other predictors. Sex, substance use, family functioning, ADHD, IP, and EP maintained their significance once all variables in the multivariate model were adjusted for. Age was not included, as it was not associated with SD at the bivariate level. Table 2 indicates that students were more likely to experience SD when they were male, had problems with family functioning, were victims of bullying, experienced substance use, were diagnosed with ADHD and exhibited IP and EP. With all other variables held constant, the strongest predictors of SD were substance use, odds ratio of 2.13 (CI = 1.31–3.46, p < .005) and family functioning, with an odds ratio of 1.85 (CI = 1.39–2.45, p < .001).
Logistic Regression Analysis Predicting SD.
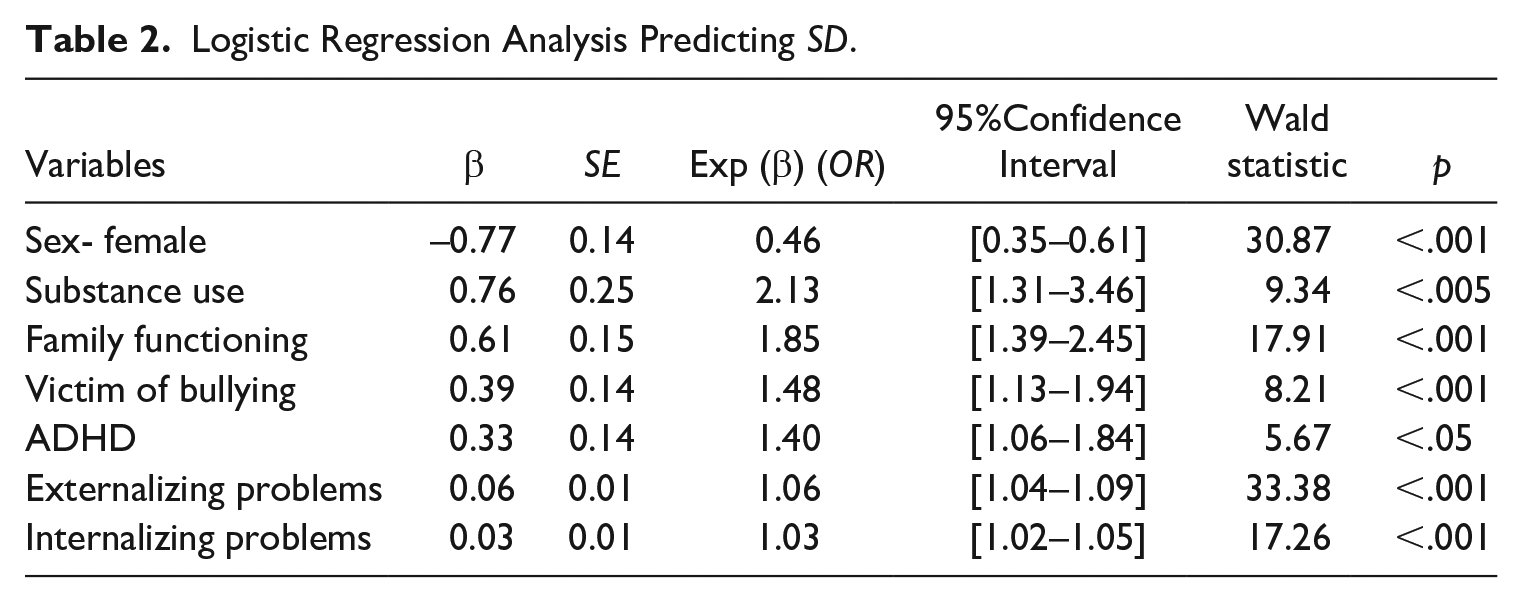
Students diagnosed with ADHD were 1.40 times more likely to experience SD (CI = 1.06–1.84, p < .005) than those not diagnosed. Similarly, those experiencing bullying were 1.48 times more likely to experience SD than non-victims of bullying (CI = 1.13–1.94, p < .05). Females were 54% less likely to experience SD than males (CI = 0.35–0.61, p < .001). EP (CI = 1.04–1.09, p < .001) and IP (CI = 1.02–1.05, p < .001) were also found to be significantly related to SD. Together, all predictors made a significant contribution to the model χ2(7) = 228.05, p < .001 and the model was able to correctly classify 71.5% of those experiencing SD versus those who did not.
Discussion
The results indicated that sex, family functioning, victim of bullying, ADHD, substance use, IP/EP were significant predictors of SD, whereas age was not. Additionally, family functioning and substance use had the largest impact on SD when holding the other variables constant.
Social Characteristics
This study extends prior work by evaluating family functioning as opposed to family structure. In recent years, the concept of family functioning has gained some notoriety. However, most study outcomes focus on well-being as opposed to academic outcomes (Lin et al., 2019). In this study, students with family difficulties were 85% more likely than those without to experience SD. Results confirm findings from Stubbs and Maynard (2017) suggesting family cohesion is an important factor in school engagement. Similarly, victims of bullying were 48% more likely than non-victims to experience SD. Bullying victimization has been associated with low perceptions of safety and subsequently, unsafe school environments increase children’s school refusal behaviors (Egger et al., 2003).
Psychiatric Characteristics
Results indicated that IP/EP, substance use and ADHD were associated with SD. IP made a significant contribution to the prediction of SD but the effect was small, which is consistent with studies reporting a limited effect of depression on dropout (Fergusson & Woodward, 2002). The current study found that with each unit increase of reported EP, experiencing SD increased by 6%. This finding is consistent with previous literature and supports that SD is part of a cumulative process of conduct-related problems leading to early school departure (Sweeten et al., 2009).
Students with ADHD were 40% more likely to experience SD than their non-ADHD peers. ADHD impairs executive functioning and self-regulation (Loe & Feldman, 2007). High rates of off-task behavior and attention seeking impacts academic success (Vile Junod et al., 2006). Adolescents with ADHD, compared to peers without this diagnosis, have an increased likelihood of academic difficulties thereby influencing future school disengagement (Birchwood & Daley, 2012).
Substance users were 113% more likely to experience SD than non-using peers. Early substance use has been associated with a decreased likelihood of successful developmental milestones during adolescence and reduced probability of high school graduation (McCluskey et al., 2002). Several explanations may shed light on this research finding. For example, drug use in early adolescence impairs cognitive development, memory, attention and overall functioning, leading to poor school performance. Initiation of substance use increases the risk of other negative outcomes (e.g., teen pregnancy), which may indirectly contribute to non-attendance and later premature school leaving (Mrug et al., 2010). Once disengaged from school, adolescents seek affiliations with deviant peers thereby exacerbating the likelihood of sustained substance use and increased deviancy (Kliewer & Murrelle, 2007).
Individual Characteristics
Previous studies have found that being male increases the probability of truancy (Van der Aa et al., 2009), and the likelihood of a history of SD (Vaughn et al., 2011), resulting in increased probability of school dropout. Former findings were echoed by the current study given that females were 54% less likely to experience school disruption, compared to males. Contrary to the literature, age in this study was not a significant predictor of SD, challenging research suggesting truancy increases with age (Smith et al., 2010). Such an inconsistency could be attributed to how SD is defined across studies. Truancy is only one of the components of SD and does not completely reflect the disruption process. Unlike other studies, this study included a variety of constructs associated with SD such as relations with staff as well as student interest and commitment to school. In addition, many studies investigating truancy patterns have included only adolescent samples (age 12–18 years) (Vaughn et al., 2013). The current study included all clinically-referred school-aged children (4–18 years) which could have influenced findings. Furthermore, our findings suggest that SD should warrant attention across all age groups, as it is not a phenomenon only impacting adolescents.
Limitations
Gender was not included in the current study. It is possible that those struggling with gender related issues are at highest risk due to exposure to bullying and victimization and increased risk of suicide and self-harm. Future studies should incorporate sex and gender to comment on their respective implications on SD.
Information surrounding substance use is typically reserved for children who are 12 years or older when using the ChYMH. In the event the clinician suspects younger children are engaging in more mature behaviors (e.g., illicit drug use), clinicians would gather this information. This practice may be subjective as it relies on the clinician’s judgment. To minimize subjectivity from one source, the ChYMH adopts a multi-informant style to result in a more accurate assessment of the potential risk of SD and its associated features. Additionally, severity of SD was not considered. Research is currently underway to examine risk levels longitudinally.
Relevance to the Practice of School Psychology
Based on our findings, family functioning, substance use problems, ADHD and bullying were associated with SD. Given the lack of standardized screening in relation to risk factors associated with SD, it is important to utilize an integrated assessment system identifying these issues as early as possible to facilitate prompt identification and intervention, before school issues become chronic in nature. This is particularly relevant for school psychologists given that preventative strategies could be implemented utilizing psychological services and care planning protocols (Stewart, Theall et al., 2015) to support vulnerable students, especially those exhibiting the highest number of risk factors.
Targeting students who exhibit risk factors associated with early school departure could be identified at an earlier stage in their school career, thereby leading to a reduction in early school termination, improved school graduation rates, and ultimately a decrease in underemployment. Moreover, anti-bullying school programs can further assist in a reduction of exclusion, peer ridicule, and traumatizing peer-to-peer experiences, thereby enhancing the likelihood that high-risk, vulnerable children will remain engaged in school, enhancing the likelihood of successful transition into promising career paths. Additional benefits could result in fewer students in conflict with the law, reduced unemployment rates, and improvements in quality of life (Finning et al., 2019). Cultivating opportunities for students with symptoms related to ADHD to obtain the tools necessary to help organize themselves, reflect and adapt to their environments will also aid in student success. Fostering executive functioning skills at an early age could enhance self-direction, foster more appropriate decision-making and reduce the likelihood of SD (Darling-Hammond et al., 2020). Improved executive functioning skills may also improve sound decision-making during the adolescent years as temptation and exposure to substances become more prevalent (Wright et al., 2013).
To foster a supportive environment and ensure student success, building strong relationships with caregivers to promote positive academic outcomes for their students is paramount. Parental involvement, and parental wellness, has been connected to academic achievement for children from kindergarten through to high school. Extended learning opportunities for caregivers (e.g., parenting programs) can foster positive academic outcomes in their children. A multi-systemic approach that enlists supports from several service sectors to meet the student needs can strengthen academic outcomes (Darling-Hammond et al., 2020), reducing the likelihood of SD thereby promoting a healthier community.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.