
Abstract
Objective
The prevalence of children needing palliative or end-of-life care is increasing. However, no comprehensive tool exists to assess the experiences of such care. We describe the development and testing of VOICES-Children (VOICES-C): the first questionnaire to assess care experiences of palliative and end-of-life services for children aged 0 to 18 years in the last 3 months of life.
Methods
VOICES-Children was developed in 3 phases: (1) a literature review of care quality domains, parent interviews, healthcare professional (HCP) focus-groups/interviews, data integration, and prototype development; (2) prototype testing through HCP and parent interviews; and (3) completion of VOICES-C. In phase 1, 24 parents were interviewed, 38 HCPs (critical care nurses, physicians, palliative care staff, and specialist palliative care service staff) participated in focus groups, and 3 took part in an interview. Participants were recruited from 2 neonatal intensive care units, 2 pediatric intensive care units, 1 cardiac intensive care unit, and a children's specialist palliative care service. In phase 2, 10 HCPs and 14 parents were interviewed.
Results
Data integration identified 19 meta-themes, including the importance of space, and the timing and amount of information. Testing demonstrated that VOICES-C captured parent experiences effectively. The final questionnaire comprised 83 questions about home care, the pediatric setting, and experiences of the last 2 days of life.
Conclusions
VOICES-Children uses literature, experience data, and parental insights to produce a robust questionnaire of pediatric end-of-life care experience, administered postbereavement, that can be applied across healthcare settings. By assessing quality, services can be improved and inequities in delivery reduced.
Introduction
In 2023, around 12,280 children in the European Union died before their first birthday. 1 A child's death is often the “ultimate loss” 2 and parents experience long-lasting grief, poorer quality of life, and increased risk of psychological ill health. 3 Pediatric end-of-life care aims to achieve optimal quality of life for children and their families, including bereavement care. 4 However, inequalities exist in access to and experiences of children's end-of-life care, with best practice lagging behind that of the adult population.5,6
While core principles are shared between adult and pediatric palliative care, children's care is a distinct specialty. The patterns of dying and death in the neonatal period and childhood differ from those in later life. Some pediatric diseases are rare, creating complexities in diagnosis and treatment, and pediatric palliative care can last years.7–9 A child's physical, emotional, cognitive, social, cultural and spiritual development, and communicative ability can affect their interaction with services.7,8,10 Parents and family members are responsible for decision-making, for the child's personal and medical care, and for communicating with healthcare professionals (HCPs).7,9,11
Despite the increasing prevalence of children requiring palliative or end-of-life care, 12 and the need to evaluate that care, 13 no comprehensive questionnaire exists to assess end-of-life care quality and experience for children and families. One review identified eleven tools measuring aspects of children's end-of-life care (eg, specifically the pediatric intensive care unit [PICU]), although none that could be applied universally. 14 A comprehensive pediatric questionnaire is needed to evaluate end-of-life care for children with life-limiting conditions in the last days of their lives and bereaved carers’ experiences. 15 This would enable consistent and uniform data to be collected across settings and populations. 16
We report on the development of VOICES-Children (VOICES-C), a questionnaire of care experiences in the last 3 months of life of children aged 0 to 18 years. VOICES-C builds on the VOICES-Short Form (VOICES-SF) questionnaire,17,18 which has been used globally,19–29 has compared care-settings, 30 determined factors associated with achieving the deceased's preferred place of death, 31 and assessed the impact of social deprivation on experience. 32 Our study assesses the acceptability of VOICES-C and its content validity and sensitivity to parent and professional experience.
Methods and Results
VOICES-Children Development
Psychometric testing is inappropriate as VOICES-C is not a psychometric scale. 17 Instead, principles of good questionnaire design and testing were followed (Figure 1). For clarity of presentation, the methods and results are presented together for each phase of the study.
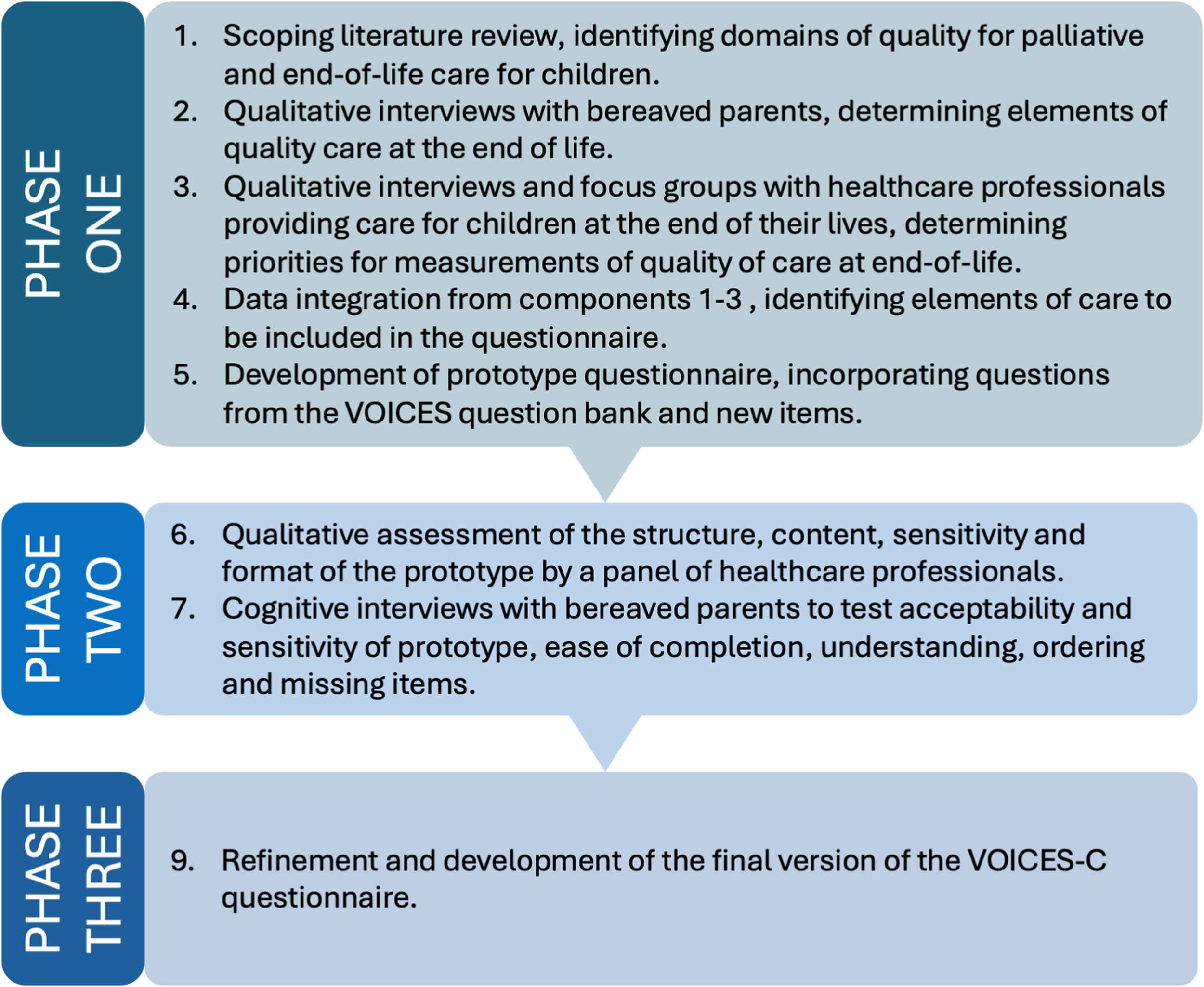
Summary of the developmental phases of VOICES-Children (VOICES-C).
Phase 1: Development
Design
Concept elicitation was used to develop VOICES-C, involving a literature review, interviews with bereaved parents, and focus groups/interviews with HCPs in which creative tools (such as the use of images) were used with open-ended questions to ensure experiences were shared in their own words, resulting in a participant-centered questionnaire. 33
Scoping Literature Review
Approach
The aim of the scoping review was to identify and synthesize evidence on quality domains in pediatric end-of-life and palliative care.
34
“Child” was defined as anyone aged <18 years, and all types of care were considered, including homes, hospitals and specialist palliative care services. AMED, CINAHL, MEDLINE, PsycINFO, and PsychARTICLES databases were searched from their inception to December 2018. Search terms included: (palliative OR end-of-life OR ‘end of life’ OR terminal), children (pediatric OR paediatric OR adolescent OR child*), and quality of care (perception* OR view* OR experience* OR need* OR satisfaction OR Quality of care). focused on bereaved parents’ views explored the essential elements of quality palliative care for children and young people focused on end-of-life or palliative care employed qualitative, quantitative, or mixed methods with open-ended questions.
Studies were excluded if they:
focused on HCPs’ accounts did not focus on end-of-life care involved case reports or nonempirical studies.
Data were extracted, tabulated, and assessed for quality. 35 Caldwell et al's 36 framework was used, and an inductive thematic analysis was applied. 37
Findings
A total of 12,788 records were retrieved (4962 papers after duplicate removal). Titles and abstracts were screened using the eligibility criteria, resulting in 42 potentially eligible papers. After reading full papers, 20 met the eligibility criteria and were included (Supplementary file1). The domains identified were:
the importance of compassionate interpersonal interaction with HCPs the provision of multidisciplinary care to the child and family practical issues (eg, access to care services).
Parents and HCP Interviews and Focus Groups
The aim of the parent and HCP interviews and focus groups was to determine elements of quality care and priorities for measurement to inform the prototype VOICES-C questionnaire.
Recruitment (Parents)
Parents whose child died between 2014 and 2015 were identified by clinical teams at 2 neonatal intensive care units (NICUs), 2 PICUs, 1 cardiac intensive care unit (CICU), and a children's specialist palliative care service. Significant dates were avoided, for example, the child's birthday; 104 parents were approached (39 from PICU, 39 from NICU, 16 from the palliative care service, 10 from CICU); 26 parents (25% response rate) registered their interest, and 24 parents of 20 children participated, including 17 mothers and 7 fathers. Children had a range of diagnoses, including congenital cardiac conditions and preterm birth with brain damage.
Recruitment (HCPs)
Purposive sampling was used to identify HCPs who supported children at the end-of-life and their families. Healthcare professionals were identified from the same organizations above. Four profession-specific focus groups were held (critical care nurses, critical care physicians, palliative care HCPs, specialist palliative care staff). Three interviews with palliative care staff were conducted. Forty-one HCPs participated (14 doctors; 24 nurses; 3 allied health professionals).
Methods
Parent telephone interviews were conducted in the period 2016 to 2017 by experienced practitioner researchers. Healthcare professional focus groups and telephone interviews were conducted in-person from 2016 to 2017 by an experienced facilitator. Topic guides were used, informed by the literature review. Interviews and focus groups were recorded and transcribed, and data were analyzed thematically. 37 KH and A-SD coded the transcripts independently and inductively, generating a coding list and preliminary themes, comparing and grouping codes, and agreeing themes and subthemes. RA evaluated codes, themes, and subthemes.
Results
Eight themes were identified in parent interviews (Table 1): time and space to say “goodbye”; legacies; availability of a key person; treating the child with humanity and individuality; recognition of parental expertise; the competence of and trust in HCPs; managing information and communication; symptom management. Fourteen themes were identified from the HCP focus groups and interviews (Table 2), relating to care coordination and delivery, effective communication and decision-making, and sustaining effective relationships.
Themes and Data Relating to Quality of Care From Bereaved Parents and Parents Caring for a Child With Life-Limiting Disease.

To protect the anonymity of participants, participant's names are replaced with their participant number.
Qualitative Themes From HCPs Working With Children With Life-Limiting Disease.

Data Integration
Data from the review, interviews, and focus groups were integrated (A-SD, KH) using a triangulation method
38
(Supplementary File 2). This involved:
coding and comparing findings across data sources creating a “convergence coding matrix,” where data were interrogated for convergence, complementarity, dissonance, and silence across sources developing meta-themes across data sources.
The meta-themes and codes (Table 3) formed the prototype questions and response items.
Meta-Themes.

VOICES-Children Prototype Development
Several decisions were made regarding the prototype, informed by experiences of creating VOICES and VOICES-SF:
Questions would focus on the last 3 months of life. Separate questionnaires would be developed for male and female children who had died. Items would combine closed questions and free-text comments. VOICES-C would be organized by care setting, with sections on the last 2 days of life and care around the time of death. Questions, where relevant, would be repeated by care setting. VOICES-Children would include demographic and disease-specific questions.
Elements of quality of children's end-of-life care were initially mapped against the VOICES-SF or the VOICES question bank. Several items were relevant for VOICES-C, for example, how long the child had been ill before they died. Some items were adapted to reflect children's services or specific needs. New items were generated using, where possible, similar wording to VOICES, informed by the meta-themes. Some items were adapted to align with the language parents used and the meanings underlying the concepts, informed by data integration findings. For example, the VOICES question regarding being “treated with dignity and respect” was changed to being “looked after in a caring way,” reflecting the parent's wish for their child to receive personal, loving care.
The VOICES-C prototype consisted of 75 questions, distributed across domains including: care at home; urgent out-of-hours care; care in NICU or PICU. Demographic questions included age, sex, ethnicity, and religion. Filter questions guided parents to appropriate sections depending on where their child had received care.
Phase 2: VOICES-Children Prototype Testing
The prototype was tested through interviews with HCPs and bereaved parents, through which content validity and sensitivity were established.
Healthcare Professional Testing
Method
Healthcare professionals with at least 2 years’ experience of working with children approaching the end-of-life were identified from 1 PICU, 1 NICU, and 2 children's specialist palliative care services. Professionals were contacted through work-based email and invited to participate. Participants were given a copy of the prototype. While navigating through the questionnaire, they:
assessed its structure, wording, comprehensiveness, and relevance to practice suggested revisions to problematic items or terms highlighted gaps or missing concepts/questions.
Interviews were audio-recorded, and notes made by prototype items. Data were analyzed using framework analysis,
39
which categorized problems and recommended amendments. Analytic categories were:
comprehension (question structure, syntax, question content) response options other issues not covered above.
Ten HCPs were interviewed by RA and JD from 2021 to 2022: 7 nurses, 1 family counselor, 1 neonatal consultant, and 1 clinical psychologist. Clinical experience ranged from 5 to 22 years. Interviews were conducted by telephone (n = 5), in person (n = 4), and via email (n = 1).
Results
Overall feedback was positive. Participants considered the questionnaire long but could not identify items for removal. Table 4 summarizes substantive recommendations.
Comments and Recommended Changes to the Questionnaire.

Parent Cognitive Interviews
Method
Parents were identified through a national charity supporting children's palliative care and clinical teams at 4 healthcare settings in the south of England: a NICU, a PICU, a pediatric ward in a specialist children's hospital, and a children's specialist palliative care service. Parents were eligible if their child had died 1 to 5 years before the study started (March-May, 2020). Significant dates were avoided during recruitment. Parents expressed their interest in participating by sending a reply slip or a scanned email attachment to the researcher, or by emailing, phoning, or texting the researcher directly. Health professional support was available to parents if they became distressed.
During interviews, parents were provided with the prototype and asked to “think aloud” their thoughts and feelings about questions and response items. This assessed the appropriateness, suitability, sensitivity, and inclusivity of items. Four telephone interviews were conducted and 10 via video call. Interviews were recorded and transcribed, with transcript content merged into one document containing responses to questions as they appeared in the questionnaire. KH, A-SD, and LW reviewed the document and findings and agreed that changes were discussed.
Results
Fourteen parents of thirteen children were interviewed individually from 2021 to 2022. The age of children at the time of death ranged from 14 h to 18 years (average 6.7 years). Eight children were boys and 5 were girls. Deaths occurred in the home, specialist palliative care, NICU, PICU, and Pediatric Ward. Twelve mothers and 2 fathers were interviewed. Responses were positive, and families welcomed the opportunity to share experiences. Table 5 summarizes participants’ recommendations. No parent had to complete all sections, and the routing was largely appropriate. All parents reported that their experiences were represented but wanted to share more about their child. The final sections were important but emotionally difficult, and parents recommended text to alert them to emotionally challenging sections.
Exemplar Comments and Recommended Changes to the Questionnaire.

Phase 3: Finalizing VOICES-C
The final version of VOICES-C was created after final amendments to the prototype. VOICES-Children comprises 83 questions, including questions about the help the deceased received, the respondent's perceptions about specific aspects of care, and their satisfaction with the quality of care overall and from specific services. It is structured around care provided at home and in the pediatric setting, and asks questions about the experiences of the last 2 days of life. It includes questions about siblings and sociodemographic information.
Discussion
This article describes the development and validation of the world's first questionnaire that can be applied across healthcare settings to assess the quality and experience of end-of-life care for children, from the perspective of parents. While the adult version of the questionnaire, VOICES-SF, has been widely adopted,19,20,31 it was unsuitable for assessing pediatric care. VOICES-Children will enable systematic, methodologically robust evaluations of children's end-of-life care from the family perspective and, for the first time, allows such care to be compared to that provided to adults. Research indicates that the evidence underpinning the design and delivery of children's end-of-life care is not as robust as in other care settings. 40 Furthermore, there is greater inequity in access to pediatric palliative services due to the relatively limited development of specialist care. 41 The application of VOICES-C will improve our understanding of precisely how children's palliative and end-of-life care lags behind adult care.5,6 In adult services, the use of Patient-Reported Outcome Measures, Patient-Reported Experience Measures, and other tools is well established to capture experience and drive improvement. In pediatric care, this work is more fragmented and inconsistent. 42 Children's experiences of end-of-life care remain invisible in national datasets, limiting our ability to compare care across the lifecourse, identify and address inequities, and drive-up standards. This represents a significant gap in evidence, equity, and accountability. Embedding the assessment of children's palliative and end-of-life care in policy and practice is essential in ensuring that everyone receives high-quality end-of-life care, regardless of age. 42
End-of-life care experiences vary across healthcare systems and cultures, and VOICES-C therefore includes domains that are relevant across diverse settings, avoiding terminology tied to a single healthcare context. VOICES-C represents a standardized approach for global comparative research in pediatric end-of-life care, promoting the international sharing of knowledge and best practices, and helping to improve care standards worldwide. However, for this to happen, wider testing of VOICES-C is recommended across different demographics, cultural contexts, and causes of death, given the selective nature of participants in the development of the questionnaire.
VOICES-Children's development highlights the importance of parental expertise and involvement, trust and communication, and the need for emotionally attuned care that celebrates a child's uniqueness, physical and emotional closeness, bereavement support and legacy-making, and the presence of a designated keyworker to hold responsibility and provide continuity. While effective symptom management is essential, these interactional aspects of care were of the highest concern. During testing, these items prompted divergent views between parents and HCPs. Parents found items on whether the child was looked after “in a caring way” and “trust” in HCPs to be meaningful and reflective of their experiences. However, most HCPs were concerned that these terms were too subjective and were thus open to inconsistent interpretation. They were also concerned that describing care as “caring” implied a judgment on their professionalism given that everything they did constituted “care.” Healthcare professionals considered “trust” to be complex, contentious and difficult to quantify. Parents thought “trust” reflected their need for safety, partnership, control and assurance that nothing would be done without their agreement. This highlights a mismatch in priorities: for parents, trust and emotional experience are central to assessing care; for professionals, the emphasis may lie in delivering clinical standards and actions. This reinforces the importance of acknowledging the language and priorities of families when evaluating care quality, even if this introduces emotional or relational nuances that might be challenging for HCPs.
Our data revealed that VOICES-SF items of “dignity” and “respect” were unlikely to resonate with bereaved parents, where looking after the child “in a caring way” was more important. This may reflect the conceptual differences in how care quality is understood between adult and pediatric contexts. In adult care, “dignity” and “respect” are tied to autonomy, independence, and privacy. 43 In contrast, children's care is understood by parents in relational terms, grounded in emotional warmth, attachment, attentiveness, and the child being known and comforted. An important message for researchers, clinicians, and policymakers is that the language parents prefer is not rooted in policy or institutional terminology. It is personal, reflecting the experience of entrusting their child's well-being to others at times of great vulnerability.
Parents expressed a desire to tell the story of their child. VOICES-Children responds to this by incorporating open-ended free-text questions and inviting parents to tell their child's story. Many parents felt that participating helped to preserve their child's legacy and was an opportunity for their child's final months to shape care for others. This reminds us that parents wish to be involved in shaping children's services. 44
VOICES-Short Form was developed to evaluate care provided in the last 3 months of life for any adult who dies. This was founded on the human right to a dignified death, regardless of the cause or whether the death was expected. Although many children only access care in the final days or hours of life, they are part of the population receiving end-of-life care. If we fail to include their experiences, we overlook a critical aspect of service delivery. All children who die and their families are entitled to excellent end-of-life care. This means ensuring that “all staff are prepared to care,” 45 including where a child dies suddenly and unexpectedly. End-of-life care is a universal responsibility across the health and social care workforce. Meeting this responsibility requires assurance that first responders, emergency departments, and critical care settings are equipped to provide good end-of-life and bereavement care, even when there is little notice that a child might die. Exploration of the use of VOICES-C in this context is warranted.
Study Limitations
While the questionnaire was developed using robust methods, certain limitations are acknowledged. Every attempt was made to ensure VOICES-C was developed with a representative group of parents and HCPs. However, there is a potential that not all parents' or healthcare experiences were included. For example, mothers were disproportionately represented during cognitive testing. It is acknowledged that service availability and configuration vary nationally and internationally. Wider testing of VOICES-C is warranted via national and international surveys reflecting different settings and experiences.
Conclusion
Our study has, for the first time, developed a robust questionnaire for assessing the quality of pediatric end-of-life care that can be used across healthcare settings. 14 Given the increasing number of children requiring palliative or end-of-life care, 12 the need for such a questionnaire has never been greater. The development of VOICES-C demonstrates that experience data are profoundly important to understanding care quality. Parental insights are essential in how we define, design, and evaluate care. We must embed routine, systematic assessment of experience into practice to address inequities in pediatric end-of-life care and deliver our promise for excellence. 46
Supplemental Material
sj-docx-1-pal-10.1177_08258597261449531 - Supplemental material for Development and Testing of VOICES-C: A Questionnaire for Assessing the Quality and Experiences of End-of-Life Care for Children and Their Families
Supplemental material, sj-docx-1-pal-10.1177_08258597261449531 for Development and Testing of VOICES-C: A Questionnaire for Assessing the Quality and Experiences of End-of-Life Care for Children and Their Families by Katherine Hunt, David Wright, Rawnaq Almahadeen, Jitske Dijkstra, Richard Wagland, Duncan Randall, Seilin Uhm, Alison Richardson and Anne-Sophie Darlington in Journal of Palliative Care
Supplemental Material
sj-docx-2-pal-10.1177_08258597261449531 - Supplemental material for Development and Testing of VOICES-C: A Questionnaire for Assessing the Quality and Experiences of End-of-Life Care for Children and Their Families
Supplemental material, sj-docx-2-pal-10.1177_08258597261449531 for Development and Testing of VOICES-C: A Questionnaire for Assessing the Quality and Experiences of End-of-Life Care for Children and Their Families by Katherine Hunt, David Wright, Rawnaq Almahadeen, Jitske Dijkstra, Richard Wagland, Duncan Randall, Seilin Uhm, Alison Richardson and Anne-Sophie Darlington in Journal of Palliative Care
Footnotes
Acknowledgments
The authors would like to express our gratitude to all parents and HCPs who gave generously of their time to support the development and user-testing of VOICES-C. The authors also thank Louise Worswick for her contribution to part of the data collection and analysis.
ORCID iDs
Ethics Statement
Ethical and research governance approval was granted by the University of Southampton (ERGO 47198; 67290), the UK Integrated Research Application System (IRAS 15/SC/0492), the children's specialist palliative care service ethics committee and hospital R&D departments. Participants gave informed consent to participate in the study before taking part. Consent for publication was obtained directly from the participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the University of Southampton Annual Adventures in Research scheme, (2015). Alison Richardson is funded by National Institute for Health and Care Research (NIHR) Applied Research Collaboration Wessex. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data relating to this research project are available from the corresponding author (K.J.Hunt@soton.ac.uk) upon reasonable request. The data are not publicly available due to privacy or ethical restrictions. Some interview data will be redacted where they contain information that could compromise participant anonymity.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.